Introduction
Colloid carcinoma (CC), also known as mucinous
non-cystic adenocarcinoma, is a distinctive type of invasive
adenocarcinoma of the pancreas at the extreme well-differentiated
end of the spectrum of pancreatic neoplasia (1). Pancreatic CC is a rare subtype that
constitutes only 1–3% of invasive pancreatic adenocarcinomas
(2). It is predominantly located in
the head of the pancreas and almost always arises in association
with intra-ductal papillary mucinous neoplasm (IPMN), especially
the intestinal sub-type of IPMN. In addition, certain CCs involve
the pancreatic tail and may originate from mucinous cystic
neoplasms (MCN) (2,3). According to previous studies, CC is
considered to exhibit a particularly indolent behavior with 5-year
survival rates of 57–72% after resection, which is significantly
better than for the more commonly found pancreatic ductal carcinoma
(4,5).
At present, only small cases studies of CC of the
pancreas on MRI and contrast-enhanced CT have been reported
(6–12). However, due to the absence of the
typical features on MRI and contrast-enhanced CT, it is always hard
to distinguish CC from other pancreatic tumors, such as IPMN and
MCN. To our knowledge, there have been no published reports about
CC appearance on 18F-FDG PET/CT imaging. In this study
we present 18F-FDG PET/CT findings in five cases with
pancreatic CC as well as a correlation with their characteristics
on MRI and contrast-enhanced CT.
Materials and methods
Patients
From January 2013 to August 2016, a total of five
patients with histologically proven pancreatic CC, which underwent
an 18F-FDG PET/CT examination in our department, were
identified and enrolled in this retrospective study. Additional
imaging consisted of contrast-enhanced CT (n=1), MRI of the
pancreas (n=1) or both modalities (n=3). The interval between FDG
PET/CT and MRI or CT scans ranged from two to seven days. The
institutional review board approved this study, and informed
patient consent was obtained from all individual participants.
18F-FDG PET/CT scan
18F-FDG PET/CT scan was performed on a
Discovery VCT 64 system (GE Healthcare, Milwaukee, WI, USA) with
15.7 cm axial field view. Patients were required to fast for at
least 6 h before imaging, and serum glucose levels were kept less
than 7.4 mmol/l. Image was obtained approximately 60 min after
intravenous administration of 3.7–5.6 MBq of FDG per kilogram of
body weight. 6 or 7 bed positions from the base of skull to
mid-thighs were imaged. PET images were acquired for 2.5 min per
bed position. CT was performed on the same scanner without
intravenous contrast administration. CT images were acquired with
140 kV, 200 mAs (adjusted by auto mA), and a gantry rotation speed
of 0.8 sec. All CT scans were obtained using 3.75-mm-thick axial
slices. Moreover, four out of five patients underwent an additional
delayed (abdominal) PET/CT examination with an interval of ~90 min
after the first scan.
Visual and semi-quantitative analysis
of PET images
PET/CT results were retrospectively analyzed and
interpreted by two experienced nuclear medicine physicians who were
blinded to the patients' clinical data, previous radiological
findings and pathology reports. Visual analysis grades of the
pancreatic lesions were defined as follows by comparing the FDG
uptake levels of the tumor to the surrounding normal tissue
(13): grade 0 (no uptake), grade 1
(equivocal uptake), grade 2 (mildly increased and non-discrete
uptake), grade 3 (mildly increased and discrete uptake), and grade
4 (definitely increased uptake). A result of grades 2–4 was
considered to be positive, and a grade of 0 or 1 was considered to
be negative. In case of discrepancy regarding the PET/CT findings,
a consensus was reached after mutual discussion between the
interpreting physicians. Areas of focally increased accumulation
known to represent physiological 18F-FDG uptakes, such
as brown fat, were excluded from the analysis.
For semi-quantitative analysis, maximum standard
uptake value (SUVmax) and tumor-to-normal pancreatic
tissue ratio (TNR) were analyzed. SUVmax was calculated
as decay-corrected maximum activity concentration in the lesion
divided by administered activity divided by body weight in
kilograms. SUVmax of the normal pancreas was acquired as
an average SUVmax of five regions of interest (ROIs)
drawn on different segments of the normal pancreas. Each ROI was
measured as a circle with a diameter of 1.5 cm. TNR was defined as
SUVmax of the tumor divided by SUVmax of the
normal pancreas tissue. In the case of a false-negative result on
FDG PET, an ROI was placed over the area corresponding to the tumor
displayed on CT and/or MRI.
MRI and contrast-enhanced CT
examinations
MRI was performed using 1.5 Tesla MR unit (Magnetom
Avanto, Siemens Medical Solutions, Germany). The conventional MR
protocol used in this study included a transverse
respiratory-triggered T2-weighted fat-suppressed turbo spin-echo
sequence (TR/TE=2000/70 ms; section thickness: 5 mm; intersection
gap: 2 mm; 320×224 matrix), and a transverse breath-hold
three-dimensional T1-weighted, fat-suppressed spoiled
gradient-recalled-echo sequence (TR/TE=209/4.8 ms; section
thickness: 5 mm; intersection gap: 2 mm; 256×192 matrix).
Multiphasic images consisting of arterial (35–45 sec), portal
(70–80 sec), and delayed (120 sec) phases were acquired after the
administration of 30 ml of contrast medium (gadopentetate
dimeglumine, Magnevist; Bayer Healthcare, Berlin, Germany).
Diffusion-weighted imaging (DWI) was acquired with two b values (0
and 500 sec/mm2).
Triple-phase CT imaging was performed using Light
Speed VCT (GE Healthcare, Milwaukee, WI, USA). A section thickness
of 3 mm with a reconstruction interval of 3 mm, a field of view of
300–370 mm, a gantry rotation time of 0.5 sec, a tube current of
150–200 mA, and a peak voltage of 120 kVp were used. The detector
collimation was 0.625 mm and the table speed was 46.8 mm per
rotation, respectively. For contrast imaging, a fixed dose of 1.5
ml of iopromide per kilogram of body weight was administered at a
rate of 2–3 ml/sec. The scanning time was delayed for the arterial
and the portal venous phase for 35–45 and 70–80 sec following
intravenous contrast administration, respectively.
MRI and contrast-enhanced CT
analysis
The investigators analyzed MRI and/or CT features of
the pancreatic tumors as follows: Lesion location; lesion size,
measured as the longest diameter on the axial scan; contour and
margin of the lesion; attenuation or signal intensity
characteristics; enhancement features on dynamic images; presence
and degree of ductal dilatation (main pancreatic duct ≥2 mm);
calcification; and presence of other associated findings, such as
adjacent organ invasion, lymph node involvement and distant
metastases.
Pathological examination
All five patients underwent surgical resection of
the intrapancreatic lesions for histopathologic confirmation within
two weeks following FDG PET/CT imaging. Histopathology was reviewed
by two experienced pathologists.
Statistical analysis
SPSS 18.0 software for Windows (SPSS Inc, Chicago)
was used for statistical analysis. Data were expressed as mean ±
SD. The paired Student t test was used to compare the difference
between SUVmax of early and delayed stages. The 95%
confidence level was chosen to determine the significance between
groups, with P<0.05 indicating a significant difference.
Results
Patient characteristics
As shown in Table I,
the five identified patients consisted of three males and two
females with an average age of 66±9 years (range 53–75 years). At
the time of initial diagnosis, two patients presented with
abdominal pain and distension, one patient presented with jaundice,
fever and abdominal distention, and the remaining two lesions were
incidentally found on imaging. CA 19-9 levels were normal in three
patients and elevated in two patients, which were 1,540.0 and
3,108.0 U/ml (normal range <37 U/ml), respectively.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
|
|
|
|
|
|
|
|
| 18F-FDG
PET/CT |
|
|
|
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|---|
|
|
|
|
| Tumor |
SUVmax |
|
|
|
|
|
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|---|
| Case no. | Sex | Age (year) | CA 19-9 levels
(ng/ml) | Location | Maximum diameter
(cm) | Contour | Margin | Early | 1.5 h delay | Normal pancreatic
tissues | TNR | Retention
index | CT | MRI | AJCC stage |
|---|
| 1 | F | 53 | 1540.0 | Head | 6.7 | Iobulated | Relatively
well-defined | 3.0 | 3.2 | 1.3 | 2.3 | 6.7% | √ | √ | Ib |
| 2 | M | 75 | – | Body | 3.5 | Round | Indiscrete | 3.5 | 2.9 | 1.3 | 2.7 | – | – | √ | Ib |
| 3 | F | 68 | 3108.0 | Head and neck | 2.7 | Lobulated | Indiscrete | 5.3 | 5.8 | 1.7 | 3.1 | 9.4% | √ | – | IIb |
| 4 | M | 63 | – | Head | 5.0 | Lobulated | Indiscrete | 4.9 | 6.7 | 1.3 | 3.8 | 36.7% | √ | √ | IIa |
| 5 | M | 72 | – | Head | 5.4 | Lobulated | Well-defined | 8.6 | – | 4.0 | 2.2 | – | √ | √ | IIa |
All five patients underwent surgical resection of
the tumors, which was performed as pancreaticoduodenectomy in four
patients, and distal pancreatectomy in one patient. Moreover, one
patient with CC in the head and neck of the pancreas underwent an
additional dissection of the hepatoduodenal ligament lymph nodes
because of invasion of Glisson's sheath. Three lesions were located
in the pancreatic head, one in the head and neck, and one in the
body. The mean maximum diameter of the tumors on axial imaging was
4.7±1.6 cm (range 2.7–6.7 cm).
18F-FDG PET/CT
findings
On visual analysis, the FDG uptake of tumor slightly
higher than that of the surrounding pancreatic parenchyma was
observed in case 1 (Fig. 1) and case
2 (Fig. 2), moderately higher in case
3 (Fig. 3) and 4 (Fig. 4), and considerably higher in case 5
(Fig. 5). Although the
SUVmax of the CC lesion was 8.6 in case 5, the remaining
pancreatic parenchyma SUVmax was 4.0, which corresponded
to inflammation in histopathology. For five lesions, the mean of
early SUVmax was 5.1±2.2, with a variability of
SUVmax ranging from 3.0 to 8.6, and the average of TNR
was 2.8±0.7, with the range from 2.2 to 3.8.
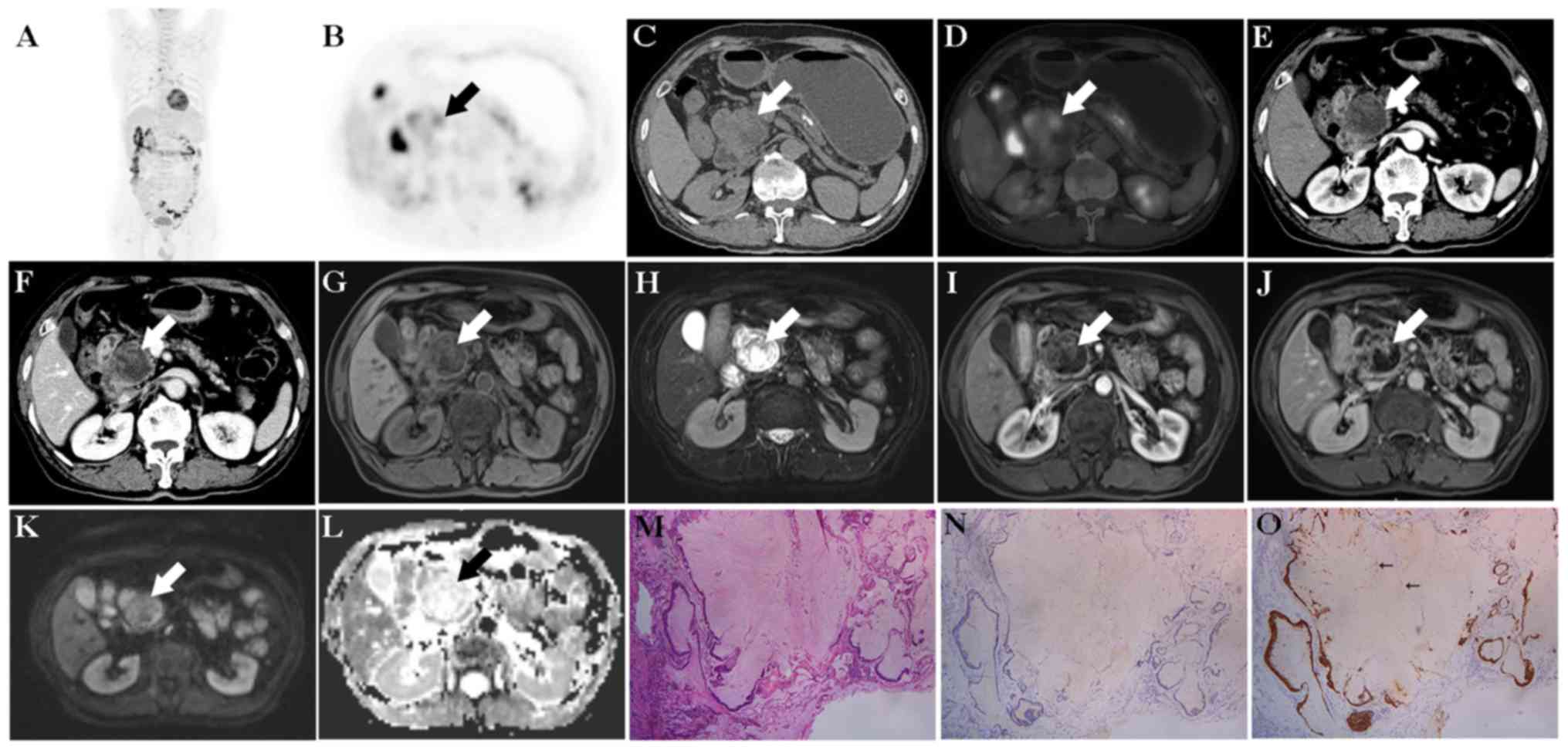
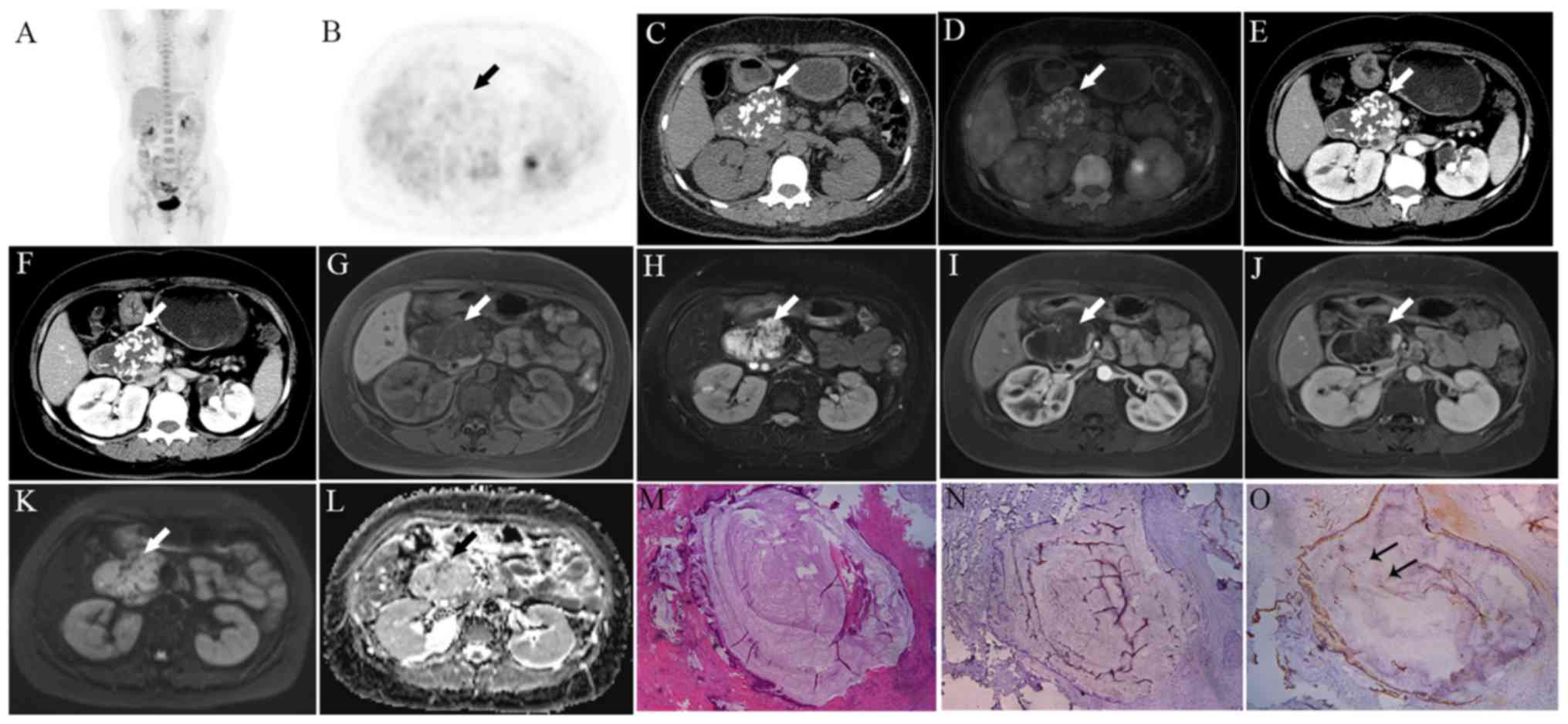 | Figure 1.(Case 1). PET/CT showed the pancreatic
lesion (arrow) with mild FDG uptake and without metastases [A,
maximum intense projection (MIP); B, PET; C, CT; D, fused]. The
SUVmax of the early and 1.5 h-delayed stages was 3.0 and
3.2, respectively, and the retention index was 6.7%.
Contrast-enhanced CT showed a lesion of the pancreatic head (arrow)
was mainly composed of cystic components and scattered
calcification, and the capsule wall of the lesion was slightly
enhanced (E, arterial stage; F, portal venous phase). Moreover,
there was an apparent atrophy of the pancreatic body and tail and a
dilation of pancreatic duct. MRI displayed the lesion (arrow) with
low signal on T1WI (G) and high signal on T2WI (H). The septations
were observed in the lesion, and were strongly enhanced (I,
arterial stage; J, delayed phase). The lesion (arrow) showed also a
high signal on DWI (K) and ADC (L) map. The lesion communicated
with the main pancreatic. Mucinous cystic neoplasms (MCN) or
intra-ductal papillary mucinous neoplasm (IPMN) was suspected based
on contrast-enhanced CT and MRI. However, the pathological
examination showed colloid carcinoma (CC) (M, H&E,
magnification ×100) with negative MUC1 (N, magnification ×100) and
positive MUC2 (O, magnification ×100, arrows). |
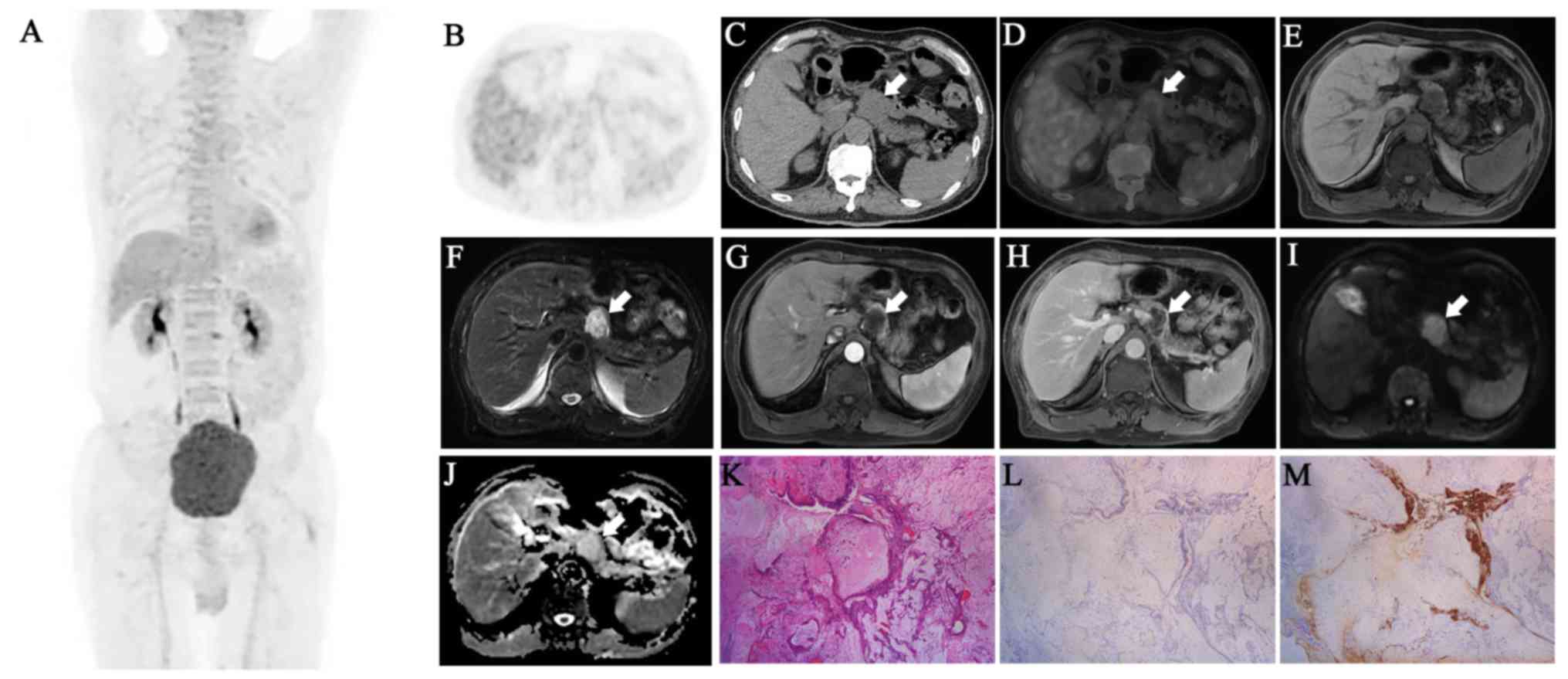 | Figure 2.(Case 2). PET/CT showed a lesion
(arrow) with mild FDG uptake with a SUVmax of 3.5, and
no distant metastases (A, MIP; B, PET; C, CT; D, fused). On the 1.5
h-delayed stage, SUVmax decreased to 2.9. MRI showed the
pancreatic lesion (arrow) with low signal on T1WI (E), and high
signal on T2WI (F). The lesion (arrow) was mildly enhanced on the
enhanced arterial phase (G), and was further filled with contrast
agent in the delayed phase (H) with additional peripheral
enhancement. The lesion (arrow) showed also a high signal on DWI
(I) and ADC (J) map. Therefore, a solid pseudo papillary tumor
(SPT) was suspected based on imaging findings, but pathology
confirmed a colloid carcinoma (CC) (K, H&E, magnification ×100)
with negative MUC1 (L, magnification ×100) and positive MUC2 (M,
magnification ×100, arrows). |
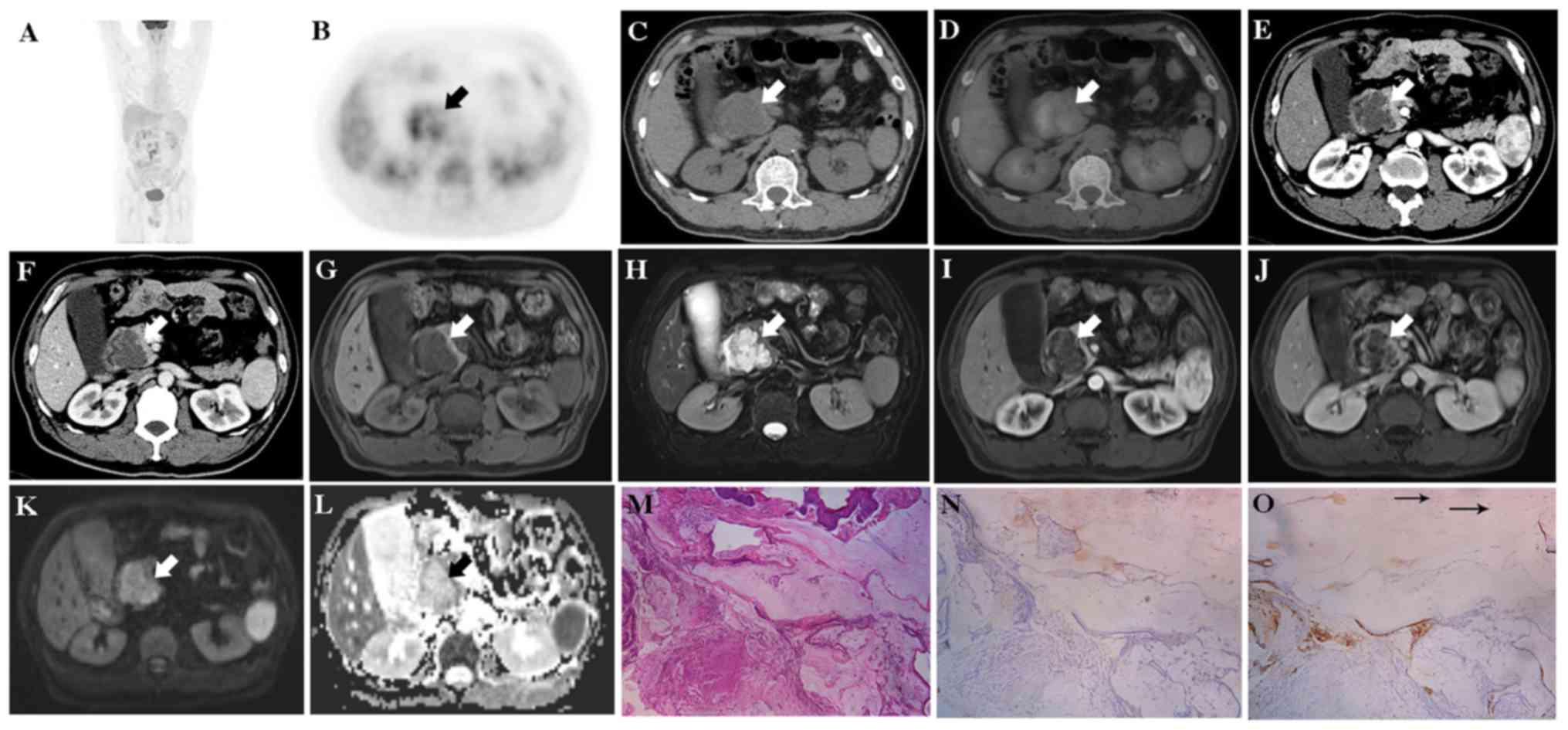
 | Figure 3.(Case 3). PET/CT [A, MIP; B and E,
PET; C and F, CT; D and G, fused) displayed the significantly
enlarged pancreatic duct (B-D) arrow] and the lesion of pancreatic
head and neck (E-G), arrow) with moderate uptake of FDG, and
SUVmax of the early and 1.5 h-delayed lesion was 5.3 and
5.8, respectively, and the retention index was 9.4%. No local
invasion and distant metastases were observed on PET/CT imaging.
Contrast-enhanced CT displayed the enlarged pancreatic duct (H,
arrow) and a multi-cystic lesion (I and J, arrow) communicating
with the pancreatic duct. The capsule wall and septations of the
mass were mildly enhanced. Moreover, dilated intra-hepatic and
extra-hepatic bile ducts and an enlarged gallbladder were observed.
Thus, intra-ductal papillary mucinous neoplasm (IPMN) was firstly
considered by the radiologists. The pathology confirmed colloid
carcinoma (CC) (K, H&E, magnification ×100) with negative MUC1
(L, magnification ×100) and positive MUC2 (M, magnification ×100,
arrows) and additional involvement of three metastatic lymph nodes
in the Glisson's sheath. |
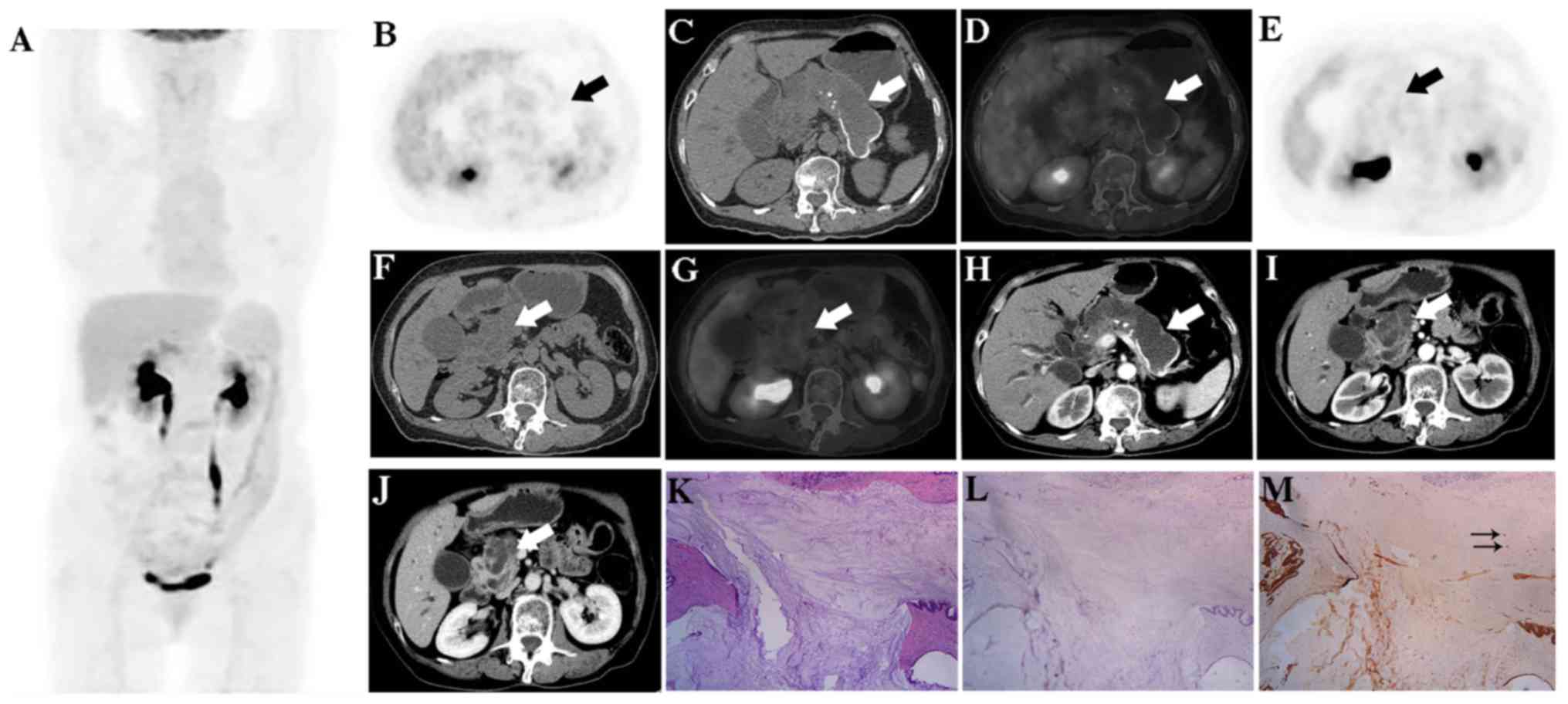
 | Figure 4.(Case 4). PET/CT (A, MIP; B, PET; C,
CT; D, fused) displayed a strong uptake of FDG by the pancreatic
lesion (arrow), and the SUVmax of early and 1.5
h-delayed stages were 4.9 and 6.7, respectively, and the retention
index was 36.7%. CT showed a slightly enhancing lesion (arrow) on
the arterial phase (E) that was further filled with the contrast
agent on the portal vein phases (F). MRI displayed a lesion (arrow)
with low signal on T1WI (G) and high signal on T2WI (H), and a
similar enhancement pattern to CT (I, arterial stage; J, delayed
phase). The lesion (arrow) showed also a high signal on DWI (K) and
ADC (L) map. Moreover, the boundary between and the lesion and the
duodenal descending segment was detectable on imaging. Intra-ductal
papillary mucinous neoplasm (IPMN) was considered by the
radiologists, but pathology diagnosed a colloid carcinoma (CC) (M,
H&E, magnification ×100) which was negative for MUC1 (N,
magnification ×100) and positive for MUC2 (O, magnification ×100,
arrows). |
 | Figure 5.(Case 5). PET/CT (A, MIP; B, PET; C,
CT; D, fused) displayed that the lesion of the pancreatic head
(arrow) had a strong FDG uptake and the SUVmax was 8.6.
The pancreatic body and tail showed apparent atrophy and
calcification as well as diffuse FDG accumulation with a
SUVmax of 4.0. FDG accumulated also in the adjacent
duodenum and the SUVmax was 12.9. Moreover, a
non-specific inflammation in mediastinal and bilateral hilar lymph
nodes was observed (A). CT showed a solid-cystic mass (arrow) in
the pancreatic head, and the solid parts were progressively
enhancing (E, arterial stage; F. portal venous phase). MRI
displayed the lesion (arrow) with heterogeneous signal, with
iso-intense or low signal on T1WI (G), and high signal on T2WI (H)
and additional dilation of pancreatic duct. The lesion (arrow) was
heterogeneously enhancing (I, arterial stage; J, delayed phase) and
showed a high signal on DWI (K) and on the ADC (L) map. Therefore,
mucinous cystic neoplasms (MCN) was initially considered, but the
pathological exam confirmed the presence of CC in the pancreatic
head (M, H&E, magnification ×100) with negative MUC1 (N,
magnification ×100) and positive MUC2 (O, magnification ×100,
arrows) as well as the pancreatitis of the body and tail. |
Four patients underwent both early and 1.5 h-delayed
PET/CT examinations. The mean SUVmax of the early and
delayed stages were 4.2±1.1 (range, 3.0–5.3), and 4.7±1.9 (range,
2.9–6.7), respectively, and there was no significant difference
between SUVmax of the early and delayed stages
(P>0.05). The SUVmax increased in three cases, and
decreased in one case. The retention index in the three cases with
increasing SUVmax was 6.7, 9.4 and 36.7%, respectively,
and the average was 17.6±16.6%.
MRI and contrast-enhanced CT
findings
Four patients received MRI scans (cases 1, 2, 4 and
5). CCs showed heterogeneously hypo-intense signals on T1-weighted
images and heterogeneously hyper-intense signals on T2-weighted
images which were brighter than the spleen. Additionally, there was
spot-like and streak-like hypo-attenuation observed within the
tumors on T2-weighted images. On gadolinium-enhanced MR images, the
solid portions or septations of the lesions were progressively
enhancing, which could be described as sponge-like enhancement
pattern. The tumors of patients 1 and 2 showed additional
peripheral enhancement. Pancreatic upstream ductal dilation was
found in three cases, including cases 1, 3 and 5, and two lesions
were communicating with the pancreatic duct (cases 1 and 3).
Four patients underwent additional abdominal
contrast-enhanced CT examination (cases 1, 3, 4 and 5). CCs showed
predominantly a cystic component with septations on CT images. The
solid portions and septations of tumor showed a slight
hyper-attenuation or iso-attenuation on pre-contrast CT, weak
enhancement during the arterial phase on contrast-enhanced CT and
increasing enhancement in the portal venous phase. All four lesions
showed internal sponge-like enhancement pattern, which was less
visible on CT than on MRI. Moreover, calcifications in different
patterns were observed in three cases with CCs (cases 1, 3 and 5):
One case with coarse calcification in the lesion (case 1), one case
with punctate and eggshell calcification in the enlarged pancreatic
duct (case 3) and one case with coarse calcification in the
non-lesion part of the pancreas with pancreatitis (case 5).
Pathological findings
All five cases were histologically confirmed CCs
which were negative for MUC1 expression and positive for MUC2. Case
1 and case 2 did not show any lymph node metastasis or invasion of
adjacent organs. The Glisson's sheath was invaded by CC in case 3
where three positive lymph nodes were found. The remaining two
cases of CC (cases 4 and 5) were located in the pancreatic head and
invaded the duodenum. Moreover, based on the American Joint
Committee on Cancer (AJCC) TNM staging system (7th edition)
(14), two cases were staged as Ib,
one case as stage IIa and two cases as stage IIb (Table I).
Discussion
CC of the pancreas was first described in a case
report by Muir in 1952 (15). Owing
to the ambiguity in the classification and lack of awareness of
this entity, many CCs of the pancreas have been categorized as
ordinary ductal adenocarcinoma, or misdiagnosed as IPMN, MCN or
signet-ring cell adenocarcinoma (2).
In a pathological study of 17 patients diagnosed with pancreatic CC
in 2001, Adsay et al (4)
considered it as a rare mucous-producing tumor that should be
distinguished from other pancreatic neoplasms. According to the
Armed Forces Institute of Pathology (AFIP) definition in 2007, the
colloid component of CC should comprise at least 80% of the
neoplasm (1).
Compared with pancreatic ductal adenocarcinoma, CC
usually shows an indolent clinical behavior with a slower growing
pattern and better prognosis (16).
The different clinical behavior may be in part related to two
characteristic features of this tumor: a) altered tumor-cell
polarity found in microscopic examination where the stromal cell
surface demonstrates secretory properties instead of a ductal cell
surface, and b) the type of mucin secreted by the tumor cells
(17). Both MUC1 and MUC2 seem to
have important roles in pancreatic neoplasia. MUC1 appears to be a
marker of an aggressive phenotype and may facilitate vascular
spread of tumor cells. MUC2 is commonly expressed in tumors with an
indolent course, such as some IPMNs and specifically in CCs
involving different organs (16,17). It
has been postulated that the secretion of MUC2 into the stroma
provokes the formation of a gelatinous layer of mucin around the
tumor cells that would limit their metastatic spread (17,18).
It has been reported that CCs yield a 5-year
survival rate ranging from 57–72% in resectable cases (4,5).
Therefore, it is paramount to identify patients eligible for
surgical treatment using radiological staging. CCs on CT usually
appear as masses with round or lobular margins and usually have
clear boundaries. The exception is that some tumors may have
ill-defined boundaries towards the duodenum that indicates invasion
to the duodenum (10), such as cases
4 and 5 in this study. CCs predominantly present with cystic
components with septations, which show hyper-attenuation or
iso-attenuation on pre-contrast CT, weak enhancement during the
arterial phase on contrast-enhanced CT, and increasing enhancement
in the portal venous phase. In our series, four of five cases have
the similar appearance. Additionally, calcification was also
observed in CCs, and the most likely explanation for the
calcification in CCs is the presence of thick mucin, which has the
tendency to build up calcium salt deposits (19,20).
There is limited information on the morphological
appearance of pancreatic CC on MR imaging. Yoon et al
(12) described the appearance of CC
on MRI as a mass with lobulated contours and indiscrete margins
that exhibited a hyper-intense salt-and-pepper-like appearance on
T2-weighted imaging with peripheral and internal sponge-like or
mesh-like progressive delayed contrast enhancement. These findings
were confirmed by our study. Moreover, Yoon et al (12) suggested that the distinction of CC
from IPMN could be made with greater confidence based on the
absence of pancreatic ductal communication or downstream ductal
dilation in MRCP. However, in our study, three cases of CCs
presented with with upstream pancreatic ductal dilation and two
lesions even communicated with the pancreatic duct. CCs usually
arise from IPMN, thus the communication between the tumors and the
pancreatic duct is possible and reasonable (2,3). In
addition, none of the CCs in our study showed intra-ductal
papillary components or bulging of the papilla of Vater into the
duodenal lumen, which are common findings in IPMN (21). We found that CCs displayed
hyper-intense on both DWI and ADC map, which reflects the low
cellularity and fluid-rich environment of CC and results in greater
freedom of motion of water molecules (22).
Combined morphological and metabolic imaging, FDG
PET/CT has proven to be a valuable diagnostic tool in pancreatic
cancer which may provide, apart from improved staging for lymph
nodes and distal metastasis, additional prognostic information
depending on the SUVmax of the primary tumor (13,23,24). To
our knowledge, this study is the first and largest series of CCs
imaged by FDG PET/CT. All CCs except one case showed a mild to
moderate FDG uptake judged by visual interpretation. However, in
the single case with elevated FDG uptake, histopathological
evaluation of the surgical specimen revealed pancreatitis, which
may most likely be the reason of the increased FDG uptake. While
the limited number of cases did not allow any further statistical
analysis, AJCC stage I tumors showed SUVmax of 3.0 and
3.5 respectively, while more advanced tumors which showed local
invasion into the duodenum or lymph node metastases on
histopathology presented with higher SUVmax ranging from
4.9 to 8.6. These findings are in congruence with a recent
meta-analysis that showed a prognostic value for SUVmax
for pancreatic tumors (24). Finally,
no distant metastases were observed on 18F-FDG PET/CT
imaging in all five cases, which reflects that the less aggressive
growth pattern of CC with better prognosis compared to ductal
adenocarcinoma. While FDG-PET/CT provided additional information
regarding locoregional and distal metastases as well as on the FDG
uptake of the primary, dual-time-point PET/CT scan showed only
relatively small changes in SUVmax between the early and
delayed stages. Therefore, the value of dual-time-point imaging of
PET/CT in the assessment of CC remains to be elucidated.
In conclusion, CC of the pancreas do not have
typical features on CT and MRI and are therefore hard to
distinguish from other pancreatic tumors such as IPMN and MCN.
18F-FDG PET/CT did not show tumor characteristics which
were unique to CC, but provided important information on potential
locoregional and distant metastases as well as on metabolic tumor
activity which may improve further patient management. The presence
of CC should be considered when a pancreatic tumor presents with a
predominantly cystic pattern with septations and sponge-like
enhancement, calcifications, upstream pancreatic ductal dilation,
the presence of the ‘salt-and-pepper sign’ on T2-weighted MRI, mild
to moderate FDG uptake and the absence of distant metastases.
Acknowledgements
Not applicable.
Funding
This study was supported in part by the National
Science Foundation for Scholars of China (grant no. 81571703) and
funding sponsored by Shanghai Pujiang Program (grant no.
2015PJD006).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
HS and LJ conceived and designed the study. LJ, QT,
HN, CMP and GZ collected and analyzed the imaging and pathology
data. LJ, QT and CMP wrote the paper. CMP also edited the
paper.
Ethics approval and consent to
participate
This retrospective study was approved by the ethics
committee of Zhongshan hospital. Informed consent to participate
was obtained from the patients.
Consent for publication
The patients of our study provided written informed
consent for the publication of any associated data and accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Hruban R, Pitman M and Klimstra D: AFIP
Atlas of Tumor Pathology. Tumors of the Pancreas. 4th Series,
Fascicle 6. Washington; American Registry of Pathology, American
Registry of Pathology and Armed Forces Institute of Pathology,
Washington, DC; 2007
|
|
2
|
Liszka L, Zielinska-Pajak E, Pajak J and
Gołka D: Colloid carcinoma of the pancreas: Review of selected
pathological and clinical aspects. Pathology. 40:655–663. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Seidel G, Zahurak M, Iacobuzio-Donahue C,
Sohn TA, Adsay NV, Yeo CJ, Lillemoe KD, Cameron JL, Hruban RH and
Wilentz RE: Almost all infiltrating colloid carcinomas of the
pancreas and periampullary region arise from in situ papillary
neoplasms: A study of 39 cases. Am J Surg Pathol. 26:56–63. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Adsay NV, Pierson C, Sarkar F, Abrams J,
Weaver D, Conlon KC, Brennan MF and Klimstra DS: Colloid (mucinous
noncystic) carcinoma of the pancreas. Am J Surg Pathol. 25:26–42.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
D'Angelica M, Brennan MF, Suriawinata AA,
Klimstra D and Conlon KC: Intraductal papillary mucinous neoplasms
of the pancreas: An analysis of clinicopathologic features and
outcome. Ann Surg. 239:400–408. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Escalon JG, Gerst S, Porembka M, Allen PJ
and Do RK: Imaging comparison of tubular and colloid pancreatic
adenocarcinoma arising from intraductal papillary mucinous neoplasm
on multidetector CT. Clin Imaging. 40:1195–1199. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Gao Y, Zhu YY and Yuan Z: Colloid
(mucinous non-cystic) carcinoma of the pancreas: A case report.
Oncol Lett. 10:3195–3198. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Jung JY, Song MH, Park YS, Jo YJ, Kim SH,
Jun DW, Kim DH and Lee WM: A case of mucinous noncystic carcinoma
of the pancreas. Korean J Gastroenterol. 51:204–208. 2008.(In
Korean). PubMed/NCBI
|
|
9
|
Plerhoples TA, Ahdoot M, DiMaio MA, Pai
RK, Park WG and Poultsides GA: Colloid carcinoma of the pancreas.
Dig Dis Sci. 56:1295–1298. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ren FY, Shao CW, Zuo CJ and Lu JP: CT
features of colloid carcinomas of the pancreas. Chin Med J (Engl).
123:1329–1332. 2010.PubMed/NCBI
|
|
11
|
Rubio-Perez I, Martin-Perez E,
Sanchez-Urdazpal L, Corbaton P and Larrañaga E: Colloid carcinoma
of the pancreas: A distinct pancreatic neoplasm with good
prognosis. Report of a case. JOP. 13:219–221. 2012.
|
|
12
|
Yoon MA, Lee JM, Kim SH, Lee JY, Han JK,
Choi BI, Choi JY, Park SH and Lee MW: MRI features of pancreatic
colloid carcinoma. AJR Am J Roentgenol. 193:W308–W313. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Jiang L, Tan H, Panje CM, Yu H, Xiu Y and
Shi H: Role of 18F-FDG PET/CT imaging in intrahepatic
cholangiocarcinoma. Clin Nucl Med. 41:1–7. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Edge SB, Byrd DR, Compton CC, Fritz AG,
Greene FL and Trotti A: AJCC Cancer Staging Manual. 7th edition.
Springer; New York, NY; 2010
|
|
15
|
Muir EG: Colloid carcinoma of the
pancreas. Br J Surg. 40:1771952. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Nakata K, Ohuchida K, Aishima S, Sadakari
Y, Kayashima T, Miyasaka Y, Nagai E, Mizumoto K, Tanaka M,
Tsuneyoshi M and Oda Y: Invasive carcinoma derived from
intestinal-type intraductal papillary mucinous neoplasm is
associated with minimal invasion, colloid carcinoma, and less
invasive behavior, leading to a better prognosis. Pancreas.
40:581–587. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Adsay NV, Merati K, Nassar H, Shia J,
Sarkar F, Pierson CR, Cheng JD, Visscher DW, Hruban RH and Klimstra
DS: Pathogenesis of colloid (pure mucinous) carcinoma of exocrine
organs: Coupling of gel-forming mucin (MUC2) production with
altered cell polarity and abnormal cell-stroma interaction may be
the key factor in the morphogenesis and indolent behavior of
colloid carcinoma in the breast and pancreas. Am J Surg Pathol.
27:571–578. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Levi E, Klimstra DS, Andea A, Basturk O
and Adsay NV: MUC1 and MUC2 in pancreatic neoplasia. J Clin Pathol.
57:456–462. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kalaitzakis E, Braden B, Trivedi P,
Sharifi Y and Chapman R: Intraductal papillary mucinous neoplasm in
chronic calcifying pancreatitis: Egg or hen? World J Gastroenterol.
15:1273–1275. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zapiach M, Yadav D, Smyrk TC, Fletcher JG,
Pearson RK, Clain JE, Farnell MB and Chari ST: Calcifying
obstructive pancreatitis: a study of intraductal papillary mucinous
neoplasm associated with pancreatic calcification. Clin
Gastroenterol Hepatol. 2:57–63. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Song SJ, Lee JM, Kim YJ, Kim SH, Lee JY,
Han JK and Choi BI: Differentiation of intraductal papillary
mucinous neoplasms from other pancreatic cystic masses: Comparison
of multirow-detector CT and MR imaging using ROC analysis. J Magn
Reson Imaging. 26:86–93. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wang Y, Miller FH, Chen ZE, Merrick L,
Mortele KJ, Hoff FL, Hammond NA, Yaghmai V and Nikolaidis P:
Diffusion-weighted MR imaging of solid and cystic lesions of the
pancreas. Radiographics. 31:E47–E64. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Jha P and Bijan B: PET/CT for pancreatic
malignancy: Potential and pitfalls. J Nucl Med Technol. 43:92–97.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wang Z, Chen JQ, Liu JL, Qin XG and Huang
Y: FDG-PET in diagnosis, staging and prognosis of pancreatic
carcinoma: A meta-analysis. World J Gastroenterol. 19:4808–4817.
2013. View Article : Google Scholar : PubMed/NCBI
|














