Introduction
Astrocytic glioma represents the most prevalent form
of malignant tumor to occur in the primary central nervous system
(CNS) of adults (1). The 5-year
survival rate in glioma patients remains lower than that for other
cancers in the United States of America (2). Despite the progress that has been made
in conventional therapies including neurosurgery, radiotherapy and
chemotherapy, the prognosis of patients with glioma remains poor
(3,4).
Due to this markedly poor prognosis and lack of effective
therapeutic options, a greater understanding of the molecular
properties of glioma to develop effective diagnostic and
therapeutic strategies is urgently required.
The matrix metalloproteinase (MMP) family is a group
of zinc-dependent endopeptidases that share similar structure and
serve as main regulators in the process of tumorigenesis (5). Previous studies have indicated MMPs are
important in a number of physiological processes, including in the
degradation of basal epithelial membranes and various extracellular
matrix (ECM) components, in apoptosis, angiogenesis and
inflammation, and also in cell growth, migration and
differentiation (5). Research has
also demonstrated that the degradation of the ECM served a crucial
role in the process of glioma cell invasion into surrounding brain
tissue (6). Furthermore, MMP-13 was
indicated to be associated with the World Health Organization (WHO)
grade and as a potential prognostic marker in glioma (7). In addition, numerous other MMP family
members, including MMP-14, MMP-19 and MMP-28 have been confirmed to
be correlated with the WHO grade and have prognostic value in
glioma (8,9). Aberrant expression of the MMP family
members has been closely associated with the pathological process
of glioma, and therefore MMPs have potential as diagnostic
molecular biomarkers in human glioma.
Matrix metalloproteinase-26 (MMP-26) belongs to a
large ECM protease family (10,11).
MMP-26 is a human-specific protease that was first cloned from a
human endometrial tumor cDNA library in 2000 (10,11). The
lack of a hinge region distinguished it from other MMPs (12). MMP-26 has the capacity to effectively
degrade various components of the ECM, including fibronectin,
gelatins, vitronectin and fibrinogen (13). In particular, published research has
demonstrated that MMP-26 served a critical role in the invasion and
angiogenesis of glioma cells (14).
However, the clinical and prognostic significance of MMP-26 in
glioma need to be investigated further.
In the present study, the expression of MMP-26 in
human astrocytic glioma specimens was detected, to investigate its
role and significance in the progression of glioma.
Materials and methods
Clinical data and tissue samples
Clinical paraffin-embedded astrocytic glioma tissue
samples were obtained from 120 patients who had received tumor
excision surgery between January 2000 and December 2008. All the
slides were re-evaluated according to the 2007 WHO classification
of tumors of the central nervous system criteria (4th edition) by
two pathologists, with differences resolved by careful discussion.
None of the patients had received anti-cancer treatments prior to
operation. Overall survival (OS) was based on patient operative
time as a starting point, to patient fatality, loss at follow-up or
the last follow-up. The follow-up information was updated every
three months and a follow-up of at least five years was performed.
The complete follow-up information was obtained in the current
research. The Sun Yat-Sen University Cancer Center ethics committee
reviewed and approved the current study and each patient signed
written informed consent at the Cancer Center of Sun Yat-Sen
University.
Immunohistochemical staining
Immunohistochemistry staining was performed on 5 µm
sections of the paraffin-embedded astrocytic glioma tissue samples
using an SPlink Detection kits (cat. no. SP-9000; ZSGB-Bio,
Beijing, China) based on the protocols of the manufacturer. In
brief, the sections were first transferred to adhesive slides and
dried at 60°C for at least 30 min. Xylene was then used to
deparaffinize the sections and rehydrate them with a decreasing
alcohol gradient and double-distilled water. The heat-induced
antigen retrieval was performed in citrate buffer by boiling for 10
min. Subsequently, the sections were treated with 3% hydrogen
peroxide (H2O2) to remove endogenous
peroxides. Then, the sections were incubated with MMP-26 antibody
(cat. no. ab81285; dilution 1:50; Abcam, Cambridge, MA, USA). Human
colorectal cancer tissues were used as a positive control.
Phosphate buffer solution replaced MMP-26 antibody, which served as
a negative control.
Evaluation of MMP-26 staining
The immunohistochemical staining results were
analyzed according to a previously described method (15). The percentage of MMP-26-positive cells
was scored as 0 for <5%, 1 for 5-<25%, 2 for 25–50% and 3 for
>50% cell staining. The intensity of staining was scored as 0
for no staining, 1 for pallide-flavens, 2 for yellow and 3 for
brown staining. The MMP-26 immunohistochemical score was defined by
multiplying the positive cells percentage and staining intensity
scores. Samples were then divided into two groups according to the
score: Scores ≤4 defined a low MMP-26 expression group while scores
>4 defined a high MMP-26 expression group. The
immunohistochemical scoring was conducted by two independent
pathologists blinded to the information on the patient's clinical
characteristics.
Statistical analysis
The data were analyzed using SPSS software (version
22.0; IBM Corp., Armonk, NY, USA). The χ2 test was used
to analyze associations between MMP-26 expression and
clinicopathological features. The Kaplan-Meier method was used to
estimate survival from survival curves, and the log-rank test was
used to calculate the difference between survival curves.
Statistical significance was defined at P<0.05.
Results
Study population
Table I presents the
clinicopathological features of the 120 patients investigated in
the current study. Among them, 90 patients (75.0%) succumbed to
mortality before the end of the follow-up period. The patient's
median age was 42 (range, 2–75) years. A total of 89 patients
(74.2%) had received total tumor resection. Among the patients, 40
cases (33.3%) were classified as grade II, 31 cases (25.9%) as
grade III and 49 cases (40.8%) as grade IV, based on the WHO
grading standards. The median follow-up period was 51.8 (range,
2.0–156.0) months.
 | Table I.Clinical characteristics of the 120
glioma patients. |
Table I.
Clinical characteristics of the 120
glioma patients.
| Characteristic | Number (%) |
|---|
| Age (years) |
|
|
Median | 42 |
|
Range | 2–75 |
| Sex |
|
| Male | 70
(58.3) |
|
Female | 50
(41.7) |
| WHO grade |
|
| II | 40
(33.3) |
| III | 31
(25.9) |
| IV | 49
(40.8) |
| KPS |
|
| ≥70 | 113 (94.2) |
|
<70 | 7
(5.8) |
| Extent of
resection |
|
|
Total | 89
(74.2) |
|
Subtotal | 31
(25.8) |
| Location |
|
|
Supratentorial | 111 (92.5) |
|
Infratentorial | 9
(7.5) |
| Mortality |
|
| No | 30
(25.0) |
| Yes | 90
(75.0) |
Immunohistochemical
characteristics
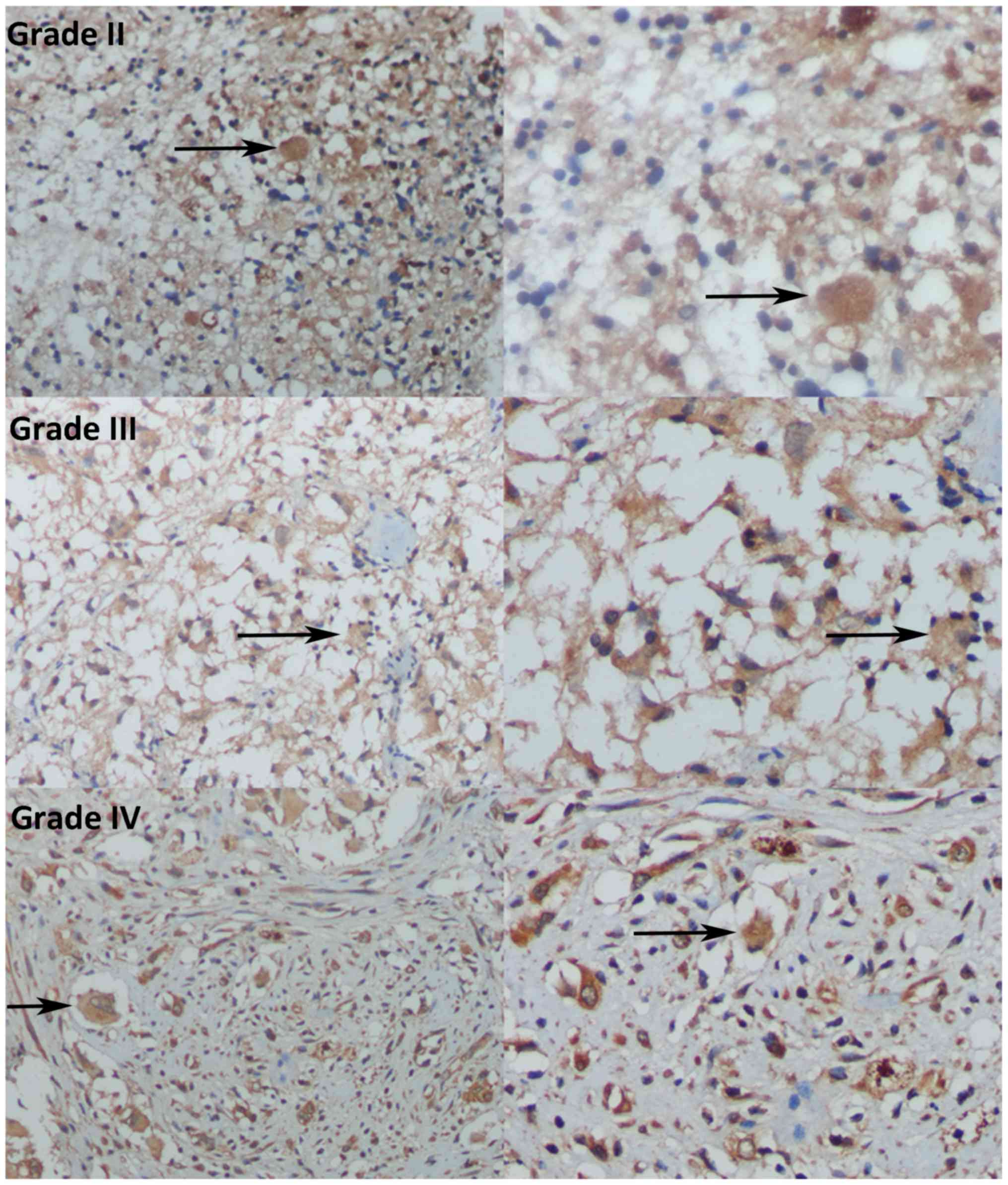
In the immunohistochemistry analysis, low MMP-26
protein expression was determined in 89 of the 120 (74.2%)
paraffin-embedded astrocytic glioma tissues, and high MMP-26
protein expression was detected in the remaining cases (31 of 120,
25.8%). Immunoreactivity of MMP-26 was mainly detected in the
cytoplasm (Fig. 1).
Associations between MMP-26 expression
and clinical characteristics
The associations between MMP-26 expression and the
clinical features of the patients with astrocytic glioma are
presented in Table II. The results
demonstrated that MMP-26 expression was significantly related to
tumor WHO grade (P=0.006), but did not reveal significant
differences associated with patient age, sex distribution,
Karnofsky performance status score, extent of resection or tumor
location in the astrocytic glioma patients (P>0.05).
| Table II.Associations of MMP-26 expression with
the clinicopathological features of glioma patients. |
Table II.
Associations of MMP-26 expression with
the clinicopathological features of glioma patients.
|
| MMP-26
expression |
|
|
|---|
|
|
|
|
|
|---|
| Variable | Low | High | P-value | χ2
value |
|---|
| All cases | 89 | 31 |
|
|
| Sex |
|
|
|
|
| Male | 51 | 19 |
|
|
|
Female | 38 | 12 | 0.698 | 0.150 |
| Age (years) |
|
|
|
|
| ≥40 | 45 | 13 |
|
|
|
<40 | 44 | 18 | 0.408 | 0.685 |
| KPS |
|
|
|
|
| ≥70 | 83 | 30 |
|
|
|
<70 | 6 | 1 | 0.784 | 0.582 |
| Extent of
resection |
|
|
|
|
|
Total | 66 | 23 |
|
|
|
Subtotal | 23 | 8 | 0.997 | <0.001 |
| Location |
|
|
|
|
|
Supratentorial | 82 | 29 |
|
|
|
Infratentorial | 7 | 2 | 0.794 | 0.068 |
| WHO grade |
|
|
|
|
| II | 35 | 5 |
|
|
|
III | 25 | 6 |
|
|
| IV | 29 | 20 | 0.006a | 10.132 |
Prognostic value of MMP-26 expression
in astrocytic glioma
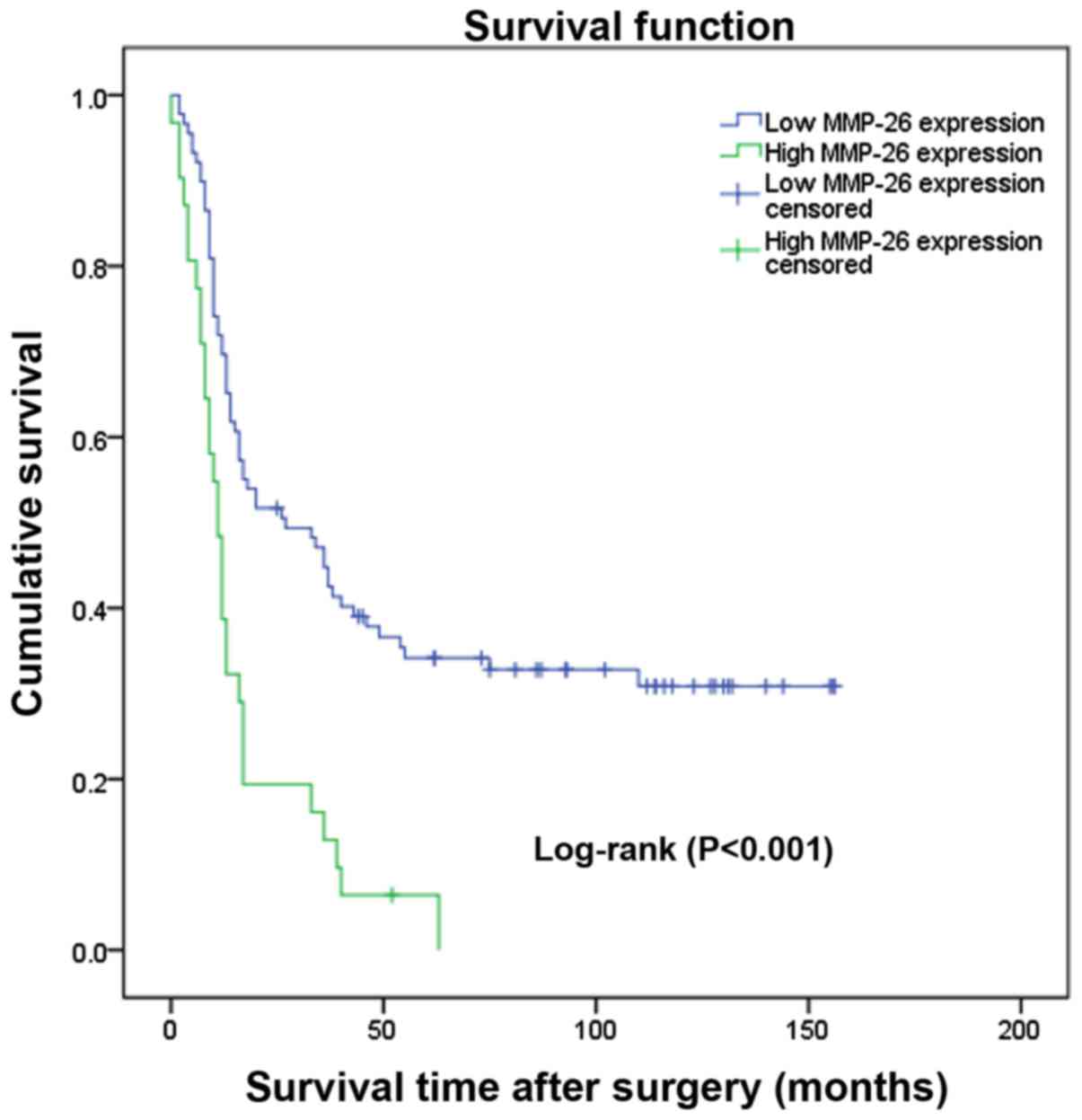
The prognostic value of MMP-26 expression was
analyzed by comparing OS according to MMP-26 expression levels. The
data demonstrated that the difference in the OS rate between the
high and low expression groups was statistically significant
(Fig. 2; P<0.001) according to the
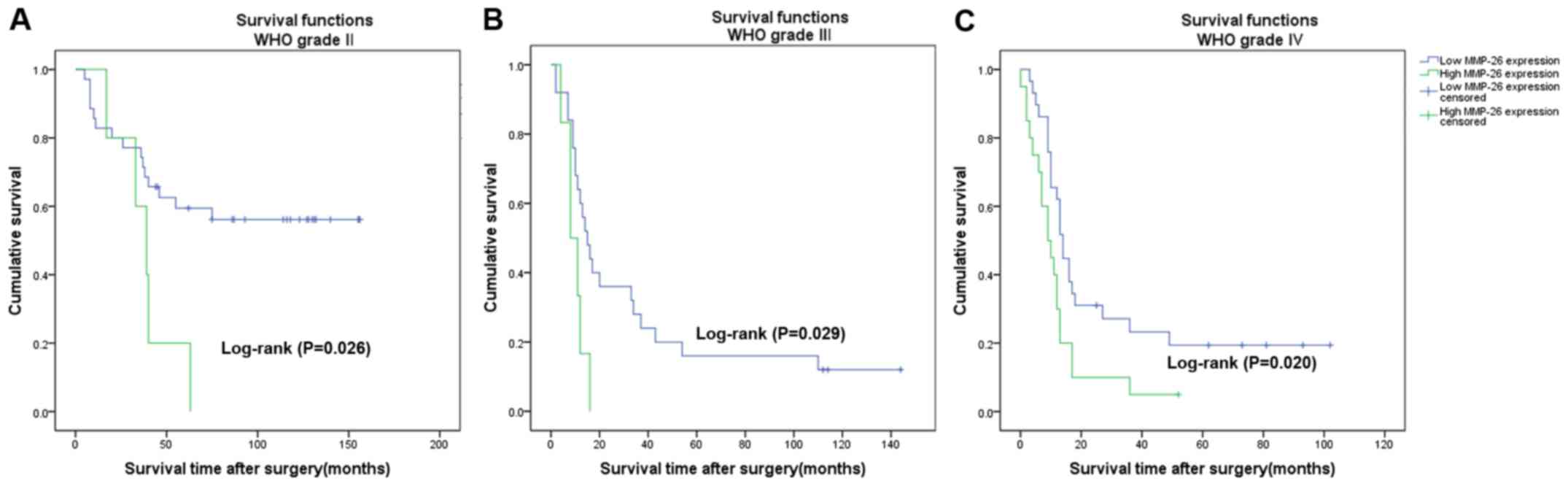
Kaplan-Meier survival analysis. Separate analysis of the difference
of the OS rate between the MMP-26 expression groups according to
WHO grade also revealed a statistically significant difference
(Fig. 3; P<0.05). Univariate and
multivariate survival analyses adjusting for all of the available
clinicopathological parameters of patients are presented in
Table III. The analyses of the
univariate and multivariate Cox regression indicated that age, WHO
grade and MMP-26 expression were independent factors for evaluating
the prognosis of patients with astrocytic glioma (Table III; P<0.05).
| Table III.Univariate and Multivariate Cox
regression analyses of patient survival. |
Table III.
Univariate and Multivariate Cox
regression analyses of patient survival.
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Variable | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Sex (male vs.
female) | 0.709 | 0.464–1.085 | 0.113 | 0.821 | 0.277–1.438 | 0.383 |
| Age (≥40 years vs.
<40 years) | 2.506 | 1.623–3.871 |
<0.001a | 2.170 | 0.467–3.909 | 0.001a |
| KPS (≥70 vs.
<70) | 0.162 | 0.787–4.181 | 0.162 | 0.950 | 0.023–2.751 | 0.909 |
| Extent of resection
(total vs. subtotal) | 1.389 | 0.884–2.182 | 0.154 | 1.552 | 0.345–3.320 | 0.071 |
| Tumor location
(supratentorial vs. infratentorial) | 0.295 | 0.093–0.935 | 0.038 | 0.697 | 0.991–12.140 | 0.557 |
| WHO grade
(T2/T3/T4) | 1.828 | 1.424–2.346 |
<0.001a | 1.573 | 1.565–6.090 | 0.001a |
| MMP-26 (low vs.
high) | 2.600 | 1.657–4.080 |
<0.001a | 1.865 | 0.352–2.360 | 0.009a |
Discussion
Primary CNS tumors represented 1.38% of all
malignant tumors and accounted for 2.60% of all malignant
tumor-associated mortalities in the United States in 2015 (2). Astrocytic glioma, which is the most
prevalent and lethal form of primary tumor of the CNS, has a highly
unfavorable prognosis. Statistics indicate that the median OS time
of patients with glioblastoma (GBM) is no more than fifteen months,
and that the 5-year survival rate is less than 10% (3). Despite the possibility for early
detection and advancements in various therapeutic methods, glioma
continues to pose a serious health threat to human health (16). It is well known that the prognosis of
glioma has a strong relationship with local recurrence and
progression. With the development of molecular biology, it is
important to identify sensitive biomarkers that can not only
identify early local recurrence and progression, but which also
have the versatility to be used as suitable targets for
therapy.
In the present study, research was conducted on
MMP-26 expression in astrocytic glioma and its clinical
significance. MMP-26 expression was evaluated in 120 cases of
paraffin-embedded astrocytic glioma tissue samples, and its
correlation with the clinicopathological parameters of patients was
assessed. According to the results, it was identified that high
MMP-26 expression was more likely to occur in advanced grade
astrocytic glioma, and furthermore, it was confirmed that MMP-26
expression was correlated with WHO grade. However, no significant
relationships with other clinicopathological parameters were
identified. Previous studies have indicated the possible
participation of MMP-26 in tumor invasion and metastasis (17–19). Hu
et al identified that the expression of MMP-26 was
correlated with cancer invasion and metastasis and served an
important role in tumor progression in colorectal cancer (15). Yamamoto et al confirmed that
MMP-26 expression was significantly correlated with cancer
invasion, metastasis and recurrence in esophageal squamous cell
carcinoma (20). The present data
also implied that MMP-26 may serve a vital role in glioma
progression. Thus, MMP-26 may play a similar role in the invasion
and progression of glioma to that observed in many other
cancers.
In addition, the present results demonstrated that
high MMP-26 expression in glioma was independently associated with
poor rates of OS in patients following tumor resection.
Kaplan-Meier analysis indicated that patients with high MMP-26
expression tended to have a lower OS rate compared with in patients
with low MMP-26 expression, suggesting that high MMP-26 expression
levels indicated poor prognosis in astrocytic glioma patients. In
addition, univariate and multivariate analyses adjusting all of the
available clinicopathological parameters of patients, demonstrated
that MMP-26 was an independent factor associated with the OS time
of the astrocytic glioma patients, in addition to the generally
established clinical predictors of age and WHO grade. Thus, MMP-26
may be regarded as a possible biomarker for predicting the OS time
of astrocytic glioma patients, and also as an independent
prognostic index for patients with astrocytic glioma. As the number
of the patients we have enrolled is small and we have only detected
the MMP-26 protein expression by immunohistochemistry, further
studies referring to the MMP-26 expression in mRNA and gene level
should be conducted to confirm the prognostic significance of
MMP-26 expression in astrocytic glioma. At present, the mechanism
of MMP-26 in enhancing tumor invasion and predicting the OS of
glioma patients is not clear. A previous study demonstrated that
MMP-26 served a key role in the invasion process of glioma cells by
impacting on ECM components in vitro (14). Additionally, MMP-26 has been reported
to promote glioma cell invasion into the tissues surrounding the
tumor (14). Furthermore, proMMP-9
could be activated by MMP-26, which is dependent upon cleavage of
the Ala93-Met94 site in the proenzyme (20,21). TIMP4
may also play an important role in the interactions with MMP-26 to
promote the cancer carcinogenesis and progression (22–24).
However, the underlying mechanisms should be clarified in greater
detail.
In conclusion, the present study confirmed that
MMP-26 expression was significantly associated with WHO grade, and
that MMP-26 was an independent predictor of OS in glioma patients.
The current findings indicated that MMP-26 may serve as a novel
indicator for the diagnosis and in evaluating the prognosis of
patients with glioma. Since the number of the patients we studied
is small and we have only detected the MMP-26 protein expression by
immunohistochemistry, further studies should be taken to confirm
the prognostic significance of MMP-26 expression in glioma.
Acknowledgements
Not applicable.
Funding
This study was supported by the Science and
Technology Planning Project of Guangdong Province, China (grant
nos. Z012B031800382 and 2014A020212098) and National Natural
Science Foundation of China (grant no. 81401908).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request
Authors' contributions
YGM and XYC were involved in conception and design
of the study; YGM provided administrative support; JGG, CCG and ZQH
were involved in provision of study materials and patients; JGG and
CCG were involved in collection and assembly of data; data analysis
and interpretation, and manuscript writing were performed by JGG,
XYC and ZQH. All authors approved the final version of the
manuscript.
Ethics approval and consent to
participate
The Sun Yat-Sen University Cancer Center ethics
committee reviewed and approved the current study and each patient
signed written informed consent at the Cancer Center of Sun Yat-Sen
University.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflicts of interests.
References
|
1
|
Ostrom QT, Gittleman H, Fulop J, Liu M,
Blanda R, Kromer C, Wolinsky Y, Kruchko C and Barnholtz-Sloan JS:
CBTRUS statistical report: Primary brain and central nervous system
tumors diagnosed in the united states in 2008–2012. Neuro Oncol.
17(Suppl 4): iv1–iv62. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2015. CA Cancer J Clin. 65:5–29. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Stupp R, Hegi ME, Mason WP, van den Bent
MJ, Taphoorn MJ, Janzer RC, Ludwin SK, Allgeier A, Fisher B,
Belanger K, et al: Effects of radiotherapy with concomitant and
adjuvant temozolomide versus radiotherapy alone on survival in
glioblastoma in a randomised phase III study: 5-year analysis of
the EORTC-NCIC trial. Lancet Oncol. 10:459–466. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Stupp R, Mason WP, van den Bent MJ, Weller
M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA, Marosi C, Bogdahn
U, et al: Radiotherapy plus concomitant and adjuvant temozolomide
for glioblastoma. N Engl J Med. 352:987–996. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Malemud CJ: Matrix metalloproteinases
(MMPs) in health and disease: An overview. Front Biosci.
11:1696–1701. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
6
|
Liu L, Wu J, Ying Z, Chen B, Han A, Liang
Y, Song L, Yuan J, Li J and Li M: Astrocyte elevated gene-1
upregulates matrix metalloproteinase-9 and induces human glioma
invasion. Cancer Res. 70:3750–3759. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wang J, Li Y, Li C, Yu K and Wang Q:
Increased expression of matrix metalloproteinase-13 in glioma is
associated with poor overall survival of patients. Med Oncol.
29:2432–2437. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wang L, Yuan J, Tu Y, Mao X, He S, Fu G,
Zong J and Zhang Y: Co-expression of MMP-14 and MMP-19 predicts
poor survival in human glioma. Clin Transl Oncol. 15:139–145. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wang X, Zhang K, Chen X, Zhao C and Sun Z:
Epilysin is overexpressed in glioblastoma and related to clinical
outcome of patients. Med Oncol. 32:3632015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Park HI, Ni J, Gerkema FE, Liu D,
Belozerov VE and Sang QX: Identification and characterization of
human endometase (matrix metalloproteinase-26) from endometrial
tumor. J Biol Chem. 275:20540–20544. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Uria JA and López-Otin C: Matrilysin-2, a
new matrix metalloproteinase expressed in human tumors and showing
the minimal domain organization required for secretion, latency,
and activity. Cancer Res. 60:4745–4751. 2000.PubMed/NCBI
|
|
12
|
de Coignac AB, Elson G, Delneste Y,
Magistrelli G, Jeannin P, Aubry JP, Berthier O, Schmitt D, Bonnefoy
JY and Gauchat JF: Cloning of MMP-26. A novel matrilysin-like
proteinase. Eur J Biochem. 267:3323–3329. 2000.
|
|
13
|
Marchenko GN, Ratnikov BI, Rozanov DV,
Godzik A, Deryugina EI and Strongin AY: Characterization of matrix
metalloproteinase-26, a novel metalloproteinase widely expressed in
cancer cells of epithelial origin. Biochem J. 356:705–718. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Deng Y, Li W and Li Y, Yang H, Xu H, Liang
S, Zhang L and Li Y: Expression of Matrix Metalloproteinase-26
promotes human glioma U251 cell invasion in vitro and in vivo.
Oncol Rep. 23:69–78. 2010.PubMed/NCBI
|
|
15
|
Hu Q, Yan C, Xu C, Yan H, Qing L, Pu Y, He
Z and Li X: Matrilysin-2 expression in colorectal cancer is
associated with overall survival of patients. Tumour Biol.
35:3569–3574. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chang SM, Butowski NA, Sneed PK and Garner
IV: Standard treatment and experimental targeted drug therapy for
recurrent glioblastoma multiforme. Neurosurg Focus.
20:E42006.PubMed/NCBI
|
|
17
|
Bister V, Skoog T, Virolainen S, Kiviluoto
T, Puolakkainen P and Saarialho-Kere U: Increased expression of
matrix metalloproteinases-21 and −26 and TIMP-4 in pancreatic
adenocarcinoma. Mod Pathol. 20:1128–1140. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Li L, Mei TH, Zhou XD and Zhang XG:
Expression and clinical significance of matrix metalloproteinase
(MMP)-26 protein in non-small cell lung cancer. Ai Zhengr.
28:60–63. 2009.
|
|
19
|
Yang H, Wang Y, Li Y, Zhang L, Deng Y, Qi
D, Li Y and Li W: Roles of matrix metalloproteinase-26 in the
growth, invasion and angiogenesis of breast cancer. Oncol Lett.
4:832–836. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yamamoto H, Vinitketkumnuen A, Adachi Y,
Taniguchi H, Hirata T, Miyamoto N, Nosho K, Imsumran A, Fujita M,
Hosokawa M, et al: Association of matrilysin-2 (MMP-26) expression
with tumor progression and activation of MMP-9 in esophageal
squamous cell carcinoma. Carcinogenesis. 25:2353–2360. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zhao YG, Xiao AZ, Newcomer RG, Park HI,
Kang T, Chung LW, Swanson MG, Zhau HE, Kurhanewicz J and Sang QX:
Activation of pro-gelatinase B by endometase/matrilysin-2 promotes
invasion of human prostate cancer cells. J Biol Chem.
278:15056–15064. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhang J, Cao YJ, Zhao YG, Sang QX and Duan
EK: Expression of matrix metalloproteinase-26 and tissue inhibitor
of metalloproteinase-4 in human normal cytotrophoblast cells and a
choriocarcinoma cell line, JEG-3. Mol Hum Reprod. 8:659–666. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zhao YQ, Wang QY, Zhai M, Xu J, Chen XQ,
Liu WL, Zhang M, Song SJ, Wang JM, Meng FY and Shan YD: A
multi-center clinical trial of recombinant human thrombopoietin in
chronic refractory idiopathic thrombocytopenic purpura. Zhonghua
Nei Ke Za Zhi. 43:608–610. 2004.(In Chinese). PubMed/NCBI
|
|
24
|
Lee S, Desai KK, Iczkowski KA, Newcomer
RG, Wu KJ, Zhao YG, Tan WW, Roycik MD and Sang QX: Coordinated peak
expression of MMP-26 and TIMP-4 in preinvasive human prostate
tumor. Cell Res. 16:750–758. 2006. View Article : Google Scholar : PubMed/NCBI
|