Introduction
Despite improved screening methods for the detection
of potentially curable hepatocellular carcinoma (HCC), asymptomatic
HCC is only sporadically diagnosed in patients (1). As a result, HCC is most commonly
diagnosed in the advanced or terminal stage with the presence of
intra- or extra-hepatic metastases (1). Therefore, HCC is one of the most lethal
cancer types, with the third highest mortality rate of all cancer
types worldwide, following lung cancer and gastric cancer (2). HCC has many risk factors, including
hepatitis B virus (HBV) and hepatitis C virus (HCV), both of which
cause acute and chronic infections that can lead to cirrhotic
pathological processes, which are thought to be the underlying
causes for HCC (1,3). Accumulating evidence suggests that HBV
infection is associated with approximately 80% of HCC cases in
China (3,4), with this association continuing to
increase in recent years (5).
Surgical tumor resection is considered to be an effective treatment
for early stage HCC, providing a good outcome in the majority of
cases (6). Unfortunately, due to the
suboptimal diagnostic methods available to detect individuals with
a high risk of developing HCC, most patients are presented to
clinicians with advanced stage HCC, at which point a variety of
treatment options are less effective, including surgical resection,
liver transplantation and locoregional procedures including
radiofrequency ablation (7).
In the last decade, several studies have identified
that there are many serum biomarkers that have the potential to
assist the early diagnosis of HCC (1,8,9). α-fetoprotein (AFP) levels were
detectable in the blood of many patients with advanced HCC
(10,11). However, high AFP levels were
unreliably detected in patients with early stage HCC. The
diagnostic value of AFP is further complicated by the fact that it
cannot provide significant discrimination between malignant and
non-malignant liver disorders (1).
Furthermore, an absence of AFP in certain patients with HCC was
also identified (12). Therefore,
exclusively using AFP as a diagnostic biomarker for the early
detection of HCC is hindered by the aforementioned limitations.
If properly validated, biomarkers circulating in the
plasma or serum could serve as the criterion standard for
non-invasive liver cancer diagnostics. Several other serum
biomarkers have been identified and their potential as candidates
for detection of early stage HCC has been thoroughly evaluated in
recent years (1,8,9). For
example, AFP-L3 and des-gamma-carboxy prothrombin (DCP) have
reportedly been useful in HCC screening (13). AFP-L3 is a glycoform of AFP, used for
the early detection of HCC (14).
AFP-L3 is exclusively derived from cancer cells (9,15) and has
a higher specificity for HCC compared with AFP (14). However, AFP-L3 is not typically
detected when AFP levels are <20 ng/ml (8) and it has a low sensitivity for early
stage HCC diagnosis (16,17). DCP is an abnormal prothrombin molecule
that is increased in HCC, with a diagnostic sensitivity that may be
greater compared with AFP (8).
However, the detection of DCP alone exhibited a low sensitivity in
the diagnosis of early stage HCC (18). It has previously been demonstrated
that the sensitivity for diagnosing HCC could be substantially
increased if both AFP and DCP levels were examined together
(18–20). However, this approach appears to be
less sensitive in detecting HCC when patients have AFP levels
<20 ng/ml (8). Therefore, there is
an urgent need to identify novel and reliable biomarkers that can
either replace or be used in combination with AFP for the detection
of preclinical HCC.
As a key member of the aldo-keto reductase
superfamily, aldo-keto reductase family 1 member B10 (AKR1B10)
modulates cell growth and survival by regulating lipid synthesis
(21,22) and eliminating carbonyl compounds
(23–28). These are key steps involved in the
proliferation and development of tumors through the regulation of
the retinoic acid signaling pathway (29,30).
AKR1B10 is overexpressed in several types of tumor tissue (23), including HCC tissue (31,32).
AKR1B10 is mainly expressed in the cytoplasm and can be secreted
through a lysosome-mediated non-classical pathway and regulated by
lysosome exocytosis signaling (33).
As an independent risk factor, AKR1B10 can exert its regulatory
role in the initiation and development of HCC, suggesting it is
involved in the molecular signaling pathways that lead to the
development of HCC. However, to the best of our knowledge, this
role of AKR1B10 is not well understood (34–36). The
expression of AKR1B10 in patients with HCC is negatively associated
with the degree of tumor differentiation; enhanced expression of
AKR1B10 was identified in well-differentiated, low-grade HCC
tissues and downregulated expression of AKR1B10 was identified in
poorly differentiated, high-grade HCC tissues (32,37).
Patients with low AKR1B10 expression appear to be associated with a
poorer prognosis compared with those with positive expression
following surgical resection of HCC tumors (31,37,38).
Although several studies have investigated serum AKR1B10 in
patients with HCC, to the best of our knowledge, the pattern of
AKR1B10 expression in patients with early stage HCC is unclear.
In the current study, an attempt was made to
characterize expression profiles of serum AKR1B10 and AFP in
patients with HCC. Serum AKR1B10 levels were first measured in
patients with different types of hepatic diseases using sandwich
ELISA. Next, the diagnostic performance of AKR1B10 in patients with
HCC was determined. Finally, AKR1B10 and AFP levels were assessed
and evaluated to determine if these biomarkers provide optimal
sensitivity and specificity for the detection of early stage
HCC.
Materials and methods
Patients
The current study enrolled a total of 84 patients
with HBV/HCV-related HCC (69 males and 15 females), 74 patients
with HBV/HCV-associated liver cirrhosis (42 males and 32 females)
and 29 patients with chronic hepatitis B/C (14 males and 15
females). These patients were admitted to Shengjing Hospital of
China Medical University (Shenyang, China) from September 2012 to
October 2014. Eligible patients were confirmed to have a history of
either hepatitis B surface antigen-/HBV DNA-positive or hepatitis C
antibody-/HCV RNA-positive for at least 6 months. An additional 30
healthy subjects (14 males and 16 females) who underwent a routine
health check at the same hospital during the same period of time
were chosen as controls. The characteristics of all participants
are summarized in Table I. The
diagnostic criteria employed were based on the guidelines for the
prevention and treatment for chronic HBV (2010 version) (39) and diagnosis, management and treatment
of HCC (V2011) (1). The study
protocols were reviewed and approved by the Intuitional Review
Board and the Ethics Committee of Shengjing Hospital of China
Medical University. Written informed consent was obtained from all
participants prior to the start of the study. The identity of each
participant, whose serum samples and medical records were obtained,
was coded and later decoded after data analysis was completed.
 | Table I.Characteristics of all
participants. |
Table I.
Characteristics of all
participants.
|
Characteristics | HCC (n=84) | Liver cirrhosis
(n=74) | Chronic hepatitis
(n=29) | Healthy control
(n=30) |
|---|
| Age, years, mean
(range) | 57 (33–78) | 55 (31–75) | 36 (23–57) | 32 (28–40) |
| Sex, n |
|
|
|
|
|
Male | 69 | 42 | 14 | 14 |
|
Female | 15 | 32 | 15 | 16 |
| Etiology, n |
|
|
|
|
| HBV
infection | 71 | 41 | 17 | 0 |
| HCV
infection | 13 | 33 | 12 | 0 |
| ALT, U/l, mean ±
SD | 65.80±61.09 | 75.80±101.80 | 57.48±59.68 |
26.23±6.48a,b |
| AST, U/l, mean ±
SD | 98.70±86.37 | 92.04±119.67 |
49.21±39.07a,b |
25.37±9.13a,b |
| Albumin, g/l, mean
± SD | 32.82±6.03 | 33.52±6.79 |
41.04±4.56a,b |
39.81±3.75a,b |
| TBil, µmol/l, mean
± SD | 59.19±90.31 | 47.23±74.16 |
14.38±5.35a,b |
11.50±3.96a,b |
| PT INR | 1.15±0.18 | 1.16±0.27 |
0.98±0.09a,b |
0.93±0.09a,b |
Laboratory investigations
Blood samples collected from the patients and
controls were tested by the Clinical Laboratory of Shengjing
Hospital of China Medical University. An array of biochemical
parameters and hepatic enzymes were specifically measured and
analyzed, including alanine aminotransferase, aspartate
aminotransferase, albumin, total bilirubin, prothrombin time
international normalized ratio and AFP.
Sandwich ELISA
Serum AKR1B10 was detected by sandwich ELISA using
the AKR1B10 ELISA kit (CSB-ELOO1540HU; Wuhan Institute of
Biological Products Co., Ltd., Wuhan, Hubei, China). First, 96-well
plates were coated with the purified antibody as the solid phase
and the sample (100 µl/well) was added in triplicate. Plates were
incubated at 37°C for 2 h and then incubated at 37°C for a further
1 h with 1:100 diluted biotin-labelled human AKR1B10 antibody (100
µl/well). After 3 washes (2 min each) with washing buffer (200
µl/well), plates were incubated at 37°C for 1 h with 100 µl/well of
streptavidin-HRP conjugates, then washed 5 times (2 min each) with
200 µl/well of washing buffer. 3,3′,5,5′-Tetramethylbenzdine (90
µl) was added to the wells and incubated at 37°C for 15 min.
Reactions were stopped with 50 µl/well of stop solution. Using a
plate reader, A450 values were read within 5 min.
Standard reagents were used for establishing a standard curve from
which serum AKR1B10 concentration was calculated.
Statistical analysis
Analyses were performed using SPSS Statistics 17.0
(SPSS, Inc., Chicago, IL, USA). One-way analysis of variance
(ANOVA), Fisher's exact test, Mann-Whitney U test and Z test were
used for statistical inference, when appropriate. If a significant
difference was identified by one-way ANOVA, a post hoc Fisher's
least significant difference test was used to determine the
difference within the groups. P<0.05 was considered to indicate
a statistically significant difference. Receiver operating
characteristic (ROC) analyses compared the diagnostic performance
of experimental parameters with a non-parametric method and the
optimal cutoff value was screened and proposed. Data were presented
as mean ± standard deviation.
Results
Patient characteristics
A total of 187 patients and 30 healthy controls were
enrolled and their demographic and biochemical characteristics are
summarized in Table I. Among them, 84
patients (44.9%) were confirmed to have HCC, 74 patients (39.5%)
were confirmed to have liver cirrhosis and 29 patients (15.5%) were
confirmed to have chronic hepatitis. There was a male predominance
in HCC patients. Compared with the controls, there were significant
differences in many demographic and biochemical characteristics
among the groups. These differences were consistent with clinical
practice after age and sex were factored into data analysis, and
follow the general pathophysiological courses of development of
liver diseases, including HCC, cirrhosis and chronic hepatitis.
Serum AKR1B10 and AFP levels in
patients with various liver disorders
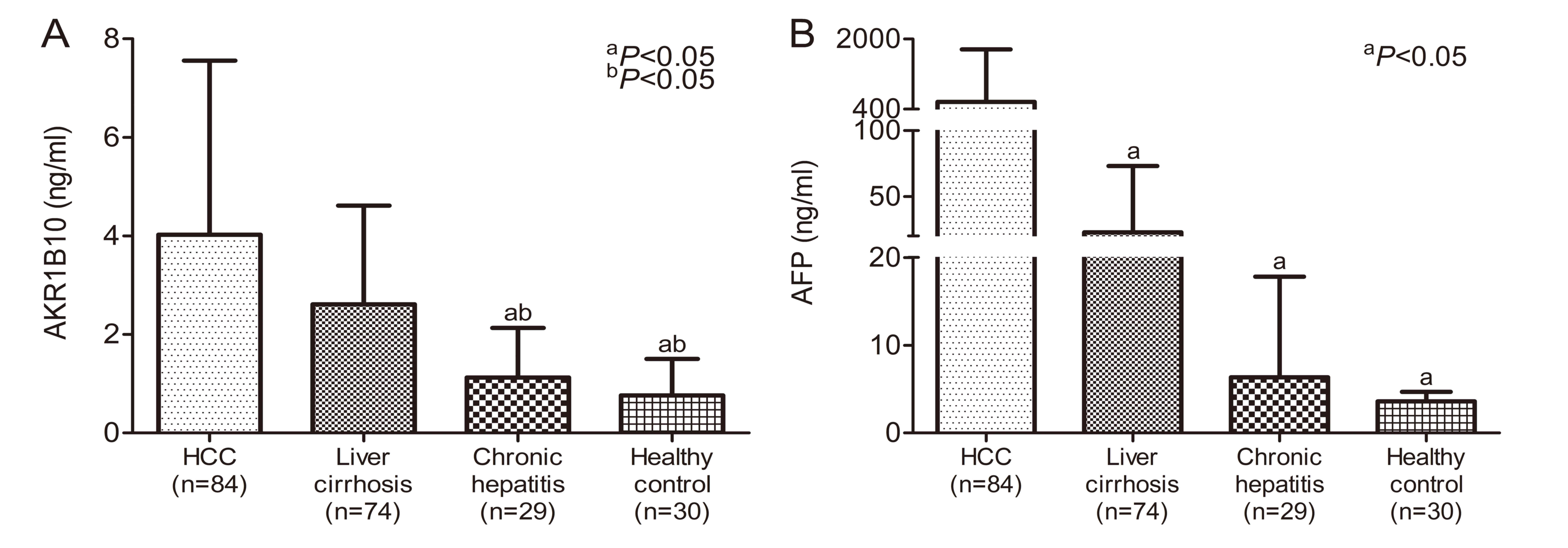
AKR1B10 levels in the serum samples obtained from
the subjects in the different groups were compared using one-way
ANOVA and the results are presented in Fig. 1A. The mean serum AKR1B10 level was
significantly higher in patients with HCC (4.02±3.53 ng/ml, n=84)
compared with patients with liver cirrhosis (2.61±2.0 ng/ml, n=74),
chronic hepatitis (1.12±1.01 ng/ml, n=29) or the controls
(0.76±0.74 ng/ml, n=30; P<0.05). Furthermore, a significant
difference in serum AKR1B10 expressions was evident between the
patients with liver cirrhosis and those with chronic hepatitis
(P<0.05), but not between patients with chronic hepatitis and
the controls (P=0.584). This indicates that the production of
AKR1B10 was enhanced when hepatocytes were undergoing cirrhosis.
Additionally, a significant increase in AFP levels was identified
in patients with HCC (566.82±1,196.90 ng/ml, n=84), liver cirrhosis
(22.88±50.29 ng/ml, n=74) and chronic hepatitis (6.35±11.47 ng/ml,
n=29) when compared to the controls (3.59±1.08 ng/ml, n=30), as
demonstrated in Fig. 1B
(P<0.05).
Regardless of the etiology of the infection, no
significant differences were identified in AKR1B10 expression when
comparing patients with HBV and HCV-related HCC (P=0.614), liver
cirrhosis (P=0.384) or chronic hepatitis (P=0.452; Table II), this suggests that release of
AKR1B10 from the damaged hepatocytes is independent of the history
of the viral infection. However, for patients with HBV infection,
HCC had a significantly higher AKR1B10 expression compared with the
liver cirrhosis and chronic hepatitis groups (P<0.05;
Table II). However no significant
difference was revealed in AKR1B10 expression between the liver
cirrhosis and chronic hepatitis groups (P=0.094). For patients with
HCV infection, the HCC and liver cirrhosis groups exhibited a
significant increase in AKR1B10 expression compared with the
chronic hepatitis group (P<0.05). However no significant
difference was identified in the expression levels between the HCC
and liver cirrhosis groups (P=0.358).
| Table II.Association of AKR1B10 expression
with viral etiology of liver disorders. |
Table II.
Association of AKR1B10 expression
with viral etiology of liver disorders.
|
| AKR1B10
(ng/ml) |
|---|
|
|
|
|---|
|
Characteristics | HCC (n=84) | Liver cirrhosis
(n=74) | Chronic hepatitis
(n=29) |
|---|
| HBV infection | 4.17±3.69
(n=71) | 2.52±2.21
(n=41)a | 1.04±1.04
(n=17)a |
| HCV infection | 3.27±2.56
(n=13) | 2.72±1.74
(n=33) | 1.24±1.00
(n=12)a,b |
| P-value | 0.614 | 0.384 | 0.452 |
Association of serum AKR1B10 and AFP
levels in patients with different stages of HCC
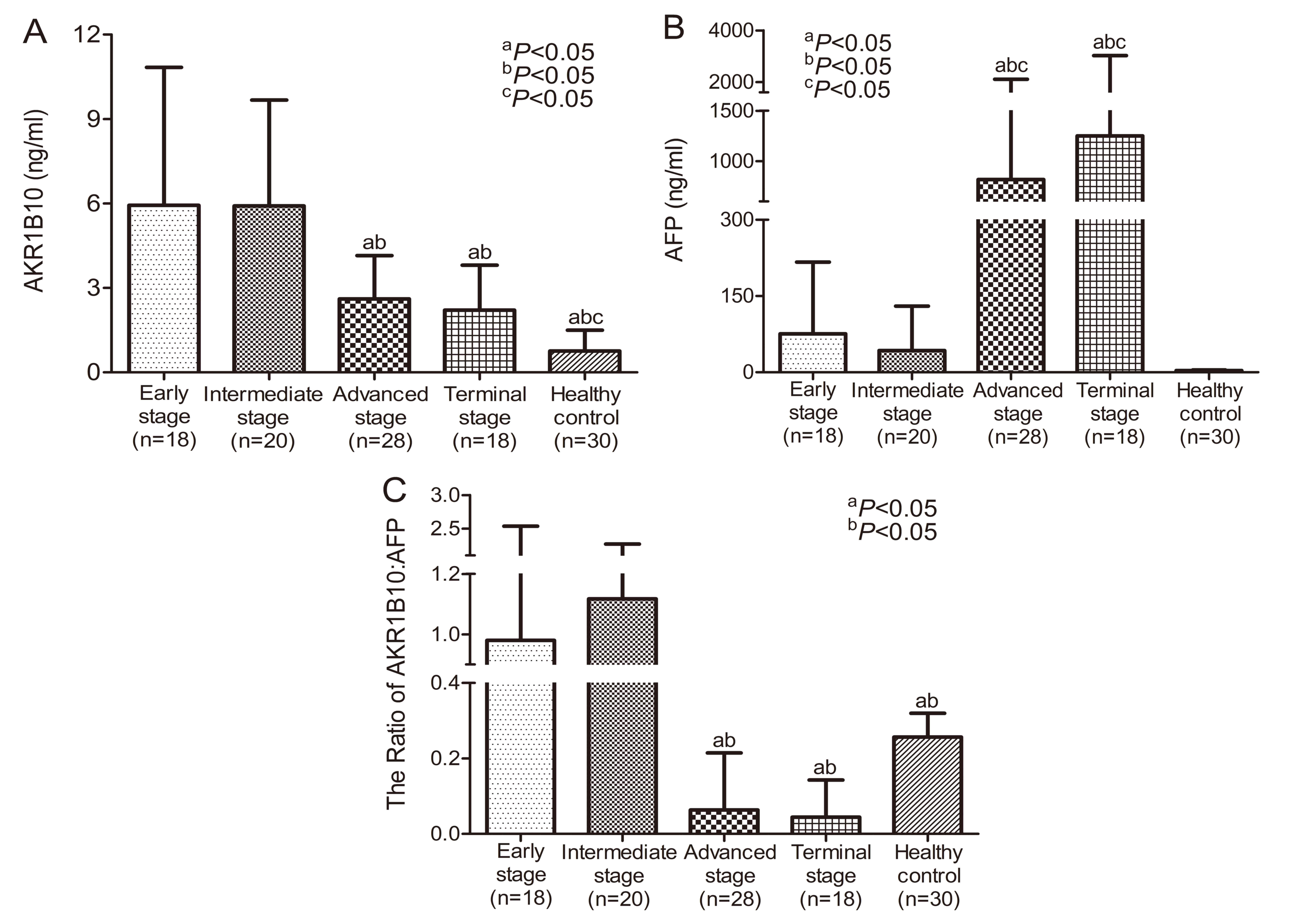
The current study assessed the association of
AKR1B10 and AFP levels in patients with HCC in relation to the
stage of liver cancer, based on the Barcelona Clinic Liver Cancer
(BCLC) staging classification (40).
Patients with tumors that were in early, intermediate, advanced and
terminal stages were selected for further subgroup analysis. As
indicated in Fig. 2, significant
differences were identified between serum AKR1B10 and AFP levels at
different stages. The highest AKR1B10 levels were identified in HCC
patients in early and intermediate stages but they declined to a
constant level in advanced and terminal stages (Fig. 2A). By contrast, the highest levels of
AFP were detected in the advanced and terminal stages compared with
the early and intermediate stages of HCC (Fig. 2B). The ratio of AKR1B10 to AFP was
significantly higher in the early and intermediate stages compared
with the advanced and terminal stages of HCC (Fig. 2C). The current results indicate that
there are variations in the expression of AKR1B10 and AFP
throughout the development of HCC. There is a clear increase in
AKR1B10 levels but not AFP levels in early stage HCC. This suggests
that AKR1B10 may be a primary factor involved in the development of
HCC and could therefore be considered as a biomarker for the
detection of early stage HCC. Conversely, serum AFP levels were
only significantly higher when HCC was in the advanced or terminal
stage.
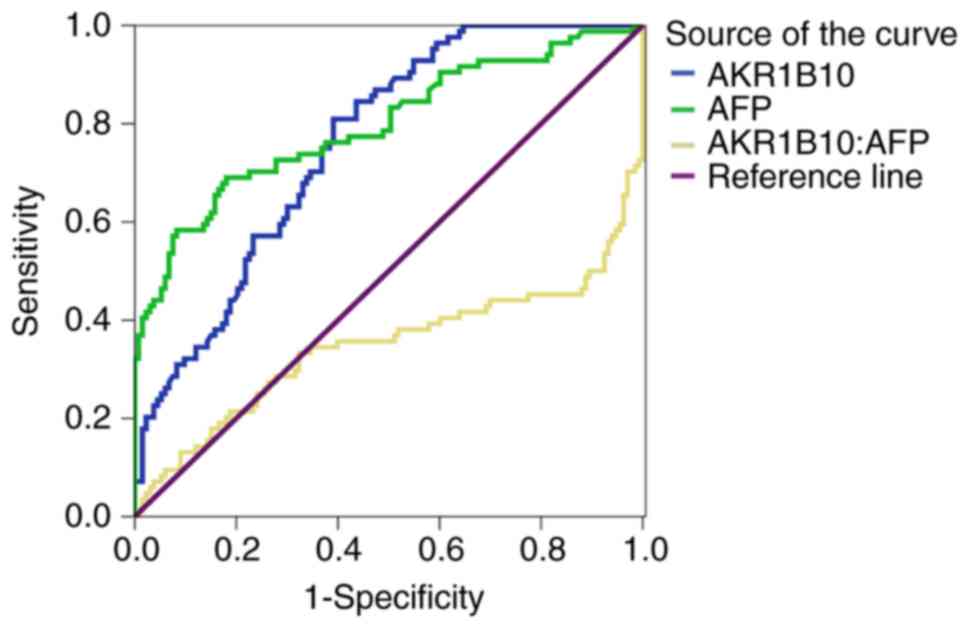
Comparison of the sensitivity and
specificity of serum AKR1B10 and AFP for the diagnosis of HCC
The sensitivity and specificity of serum AKR1B10 and
AFP for diagnosing HCC were determined by generating an ROC curve
(Fig. 3). When a cutoff value of 1.51
ng/ml was used, the sensitivity and specificity of serum AKR1B10
for diagnosing HCC were 81.0 and 60.9%, respectively. Accordingly,
the sensitivity and specificity for HCC were 69.0 and 82.0%,
respectively, if a cutoff value of 11.71 ng/ml of serum AFP was
used. It appeared that a high specificity for HCC diagnosis could
only be achieved when a high level of serum AFP was used. In
addition, among patients with HCC with ARK1B10 >1.51 ng/ml, only
26 patients exhibited concentrations of AFP <11.71 ng/ml, which
is the relative diagnostic threshold of AFP with the highest
sensitivity and specificity. This finding further revealed that
there was a marked expression of ARK1B10 before AFP becomes more
clinical relevant. Furthermore, diagnostic performance of AKR1B10
and AFP for HCC was further assessed and compared (Table III). With 95% confidence interval,
the area under curve (AUC) for AKR1B10 [AUC=0.759 (0.697–0.821)]
and AFP [AUC=0.796 (0.732–0.860)] was similar. No statistically
significant difference in the performance for HCC diagnosis was
identified between AFP and AKR1B10 (Z=0.805, P=0.390).
| Table III.Comparison of the AUC for serum
AKR1B10 and AFP for HCC diagnosis. |
Table III.
Comparison of the AUC for serum
AKR1B10 and AFP for HCC diagnosis.
| Item | AUC | SE | 95% CI | Z-value | P-value |
|---|
| AKR1B10 | 0.759 | 0.032 | 0.697–0.821 |
|
|
| AFP | 0.796 | 0.033 | 0.732–0.860 |
|
|
| AFP-AKR1B10 | 0.037 | 0.046 |
| 0.805 | 0.390 |
Complementary diagnostic performance
of AKR1B10 with AFP for HCC
The current findings suggest that ARK1B10 is a
potential serum biomarker for early detection of HCC. The current
study further explored whether concurrent measurement of ARK1B10
with AFP could increase the sensitivity of HCC diagnosis. As
expected, a sensitivity of 92.86% (78/84) for HCC diagnosis was
achieved when a combination of AKR1B10 and AFP proteins were
measured. In addition, the specificity and positive predictive
value for diagnosing HCC were 52.63% (70/133) and 55.32% (78/141),
respectively, with a negative predictive value as high as 92.11%
(70/76) (Table IV). Compared with a
single biomarker, the combined measurement of AKR1B10 and AFP
levels markedly increased the sensitivity and negative predictive
value for HCC diagnosis. Taken together, these findings demonstrate
there is promise for developing a novel diagnostic approach to
detect early stage HCC.
| Table IV.Diagnostic performance of serum
AKR1B10 in combination with AFP in patients with HCC. |
Table IV.
Diagnostic performance of serum
AKR1B10 in combination with AFP in patients with HCC.
| AKR1B10/AFP | HCC | Non-HCC | Total |
|---|
| AKR1B10 >1.5
ng/ml | 78 | 63 | 141 |
| ± AFP >11.71
ng/ml |
| Negative for
both | 6 | 70 | 76 |
| Total | 84 | 133 | 217 |
Discussion
HCC is notorious for its subtle onset and rapid
progression (1). The vast majority of
patients with HCC are already in advanced stage complicated with
multiple intra- and extra-hepatic metastases when a diagnosis is
confirmed (1). A reliable method
allowing diagnosis of asymptomatic HCC is of paramount importance
to reduce mortality and improve prognosis of patients with HCC
(41). The current study assessed the
diagnostic performance of AKR1B10 in diagnosing Chinese patients
with HCC who had previously contracted either HBV or HCV infection.
The current results indicated that patients with HCC have a
significantly higher level of serum AKR1B10 compared with patients
with hepatic cirrhosis and chronic hepatitis. Compared with
advanced and terminal stage HCC, a significant increase in the
concentration of AKR1B10 was detected in patients with early stage
HCC, while AFP levels were below the threshold for HCC
diagnosis.
HCCs are not homogeneous and certain HCCs may have
normal or only mildly elevated levels of AFP compared with healthy
individuals. The highest sensitivity and specificity of AFP for
diagnosis of HCC (60–80% and 70–90%, respectively) was achieved at
a cut of value of 16 nm/ml (42), but
AFP was not expressed in approximately 30–40% of patients with HCC,
which makes this diagnostic approach less reliable (12). In the current study, in 31% (26/84) of
patients with HCC, enhanced AKR1B10 expression was highly
associated with HCC, while the concentration of AFP was still below
its threshold for HCC diagnosis. This suggests that the
concentration of AKR1B10 associates well with the development of
HCC and thus could be a potential biomarker for early HCC
detection.
For the high-risk population, it is recommended that
serum AFP level measurement and liver ultrasonography be performed
every 6 months as a screening method (43). However, the role of such an approach
is devalued by the relatively low sensitivity and specificity of
AFP as a reliable biomarker for identifying early stage HCC. The
current study identified that 62% of patients with HCC (52/84) had
serum AFP levels of <200 ng/ml, and 200 ng/ml is considered to
be the diagnostic value of HCC in clinical practice. Furthermore,
by setting the ROC curve with a cutoff value of 11.095 ng/ml, the
sensitivity and specificity of AFP for diagnosing HCC were 77.1 and
81.2%, respectively, which is consistent with previously published
results (19). Unfortunately, AFP
levels below the diagnostic threshold of 20 ng/ml were only
sporadically observed in patients with HCC.
It is known that AKR1B10 expression is upregulated
in HCC tissues (31,32,37).
However, to the best of our knowledge, its biological significance
in molecular and pathological processes in HCC is poorly
understood. So far, data from only a handful of studies suggest
that serum AKR1B10 could be a convenient and potential biomarker
for diagnosing HCC. The current findings indicate that serum
AKR1B10 levels in patients with HCC were significantly higher
compared with patients with non-cancerous hepatic disease,
including liver cirrhosis and chronic hepatitis and further
analysis demonstrated a strong association between AKR1B10 and HCC,
as also reported by a previous study (31). Notably, with an AKR1B10 cutoff value
of 1.51 ng/ml determined by an ROC curve in the current study, the
sensitivity and specificity of AKR1B10 reach a level where
diagnosis of HBV/HCV-related HCC could be achieved.
When the association of AKR1B10 levels with BCLC
staging was considered, the current study identified a significant
increase in serum AKR1B10 in patients with early and intermediate
stage HCC compared with patients with advanced and terminal stage
HCC. This unique pattern of expression is the opposite of that
identified for AFP levels, which were the highest in the terminal
stage. These findings strongly suggest there is a close association
between the expression of ARK1B10 and early development of HCC.
Although the upregulation of AKR1B10 expression is also observed in
patients with HBV or HCV infections as well as hepatic fibrosis
(34), it appears that elevation of
AKR1B10, which has significant clinical implications, occurs as
soon as hepatocytes begin to undergo cirrhosis, with the final
pathohistological changes leading to liver cancer. As identified in
the current study, both HBV and HCV increase serum AKR1B10, which
was more pronounced in HCC and liver cirrhosis. Therefore, a robust
expression of ARK1B10 during the early stage of HCC increases its
candidacy as a potential biomarker compared with AFP, in the early
detection of HCC. Furthermore, the current data support the notion
that, with a concurrent evaluation of multiple potential
biomarkers, which is still a focus of ongoing research, the rate of
detection of early stage HCC could be improved, as reported
previously (44). By combining
AKR1B10 with AFP, there could be a notable improvement in the
diagnostic performance and screening of HCC.
A limitation of the current study is the relatively
small number of subjects. In addition, whether the association
between serum AKR1B10 levels and tissue AKR1B10 expression in
patients with HCC was linearly dependent or not was not
investigated. In this regard, a prospective large sample analysis
of the association between serum AKR1B10 levels and HCC tissues
expression should be performed in multicenter studies. Furthermore,
AKR1B10 expression was not exclusively revealed in malignant
tumors; a low to moderate expression was also observed in the
normal human tissues or non-neoplastic conditions. Therefore,
further studies are required to characterize the specific role of
AKR1B10 in liver cancer screening.
In conclusion, levels of AKR1B10 are significantly
elevated in patients with HCC in a stage-dependent manner and could
serve as a prospective serum biomarker for diagnosing
HBV/HCV-related early HCC. The unique expression of AKR1B10 in
early stage HCC makes it a stronger candidate biomarker compared
with others for early detection of HCC. Furthermore, evaluating
combined AKR1B10 and AFP levels has some promising clinical
implications, since a high diagnostic accuracy for HCC by
concurrently examining these two biomarkers appears to be
achievable.
Acknowledgements
Not applicable.
Funding
The present study was funded by the National Science
and Technology Major Project (grant nos. 2017ZX10201201,
2017ZX10202202 and 2017ZX10202203), the China National Science and
Technology Key Project for Infectious Diseases Control for the
consecutive 12th Five-Year Plan Period (grant no.
2012ZX10002003-003-010), the Liaoning Provincial Science and
Technology Key Project for Translational Medicine (grant no.
2016509), the Liaoning Provincial Science and Technology Key
Project for Translational Medicine (grant no. 2014225020), the
Science and Technology Project of Liaoning Province (grant no.
2013225021) and the Outstanding Scientific Fund of Shengjing
Hospital (grant no. 201102).
Availability of data and materials
All data generated or analyzed during the present
study were included in this published study.
Authors' contributions
CH and LG gathered samples, analyzed and interpreted
the patient data, and wrote the manuscript. HB and XD made
contributions to conception, design and acquisition of funding. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study protocols were approved by the Ethics
Committee of Shengjing Hospital of China Medical University
(approval no. 2016PS105J) and written informed consent was obtained
from all participants.
Patient consent for publication
Written informed consent for publication was
obtained from all participants.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ministry of Health of the People's
Republic of China: Diagnosis, management, and treatment of
hepatocellular carcinoma (V2011). J Clini Hepatol. 11:1141–1159.
2011.(In Chinese).
|
|
2
|
Global Burden of Disease Cancer C, .
Fitzmaurice C, Dicker D, Pain A, Hamavid H, Moradi-Lakeh M,
MacIntyre MF, Allen C, Hansen G, Woodbrook R, et al: The global
burden of cancer 2013. JAMA Oncol. 1:505–527. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
El-Serag HB: Hepatocellular carcinoma. N
Engl J Med. 365:1118–1127. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
McGlynn KA, Petrick JL and London WT:
Global epidemiology of hepatocellular carcinoma: An emphasis on
demographic and regional variability. Clin Liver Dis. 19:223–238.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yang X, Gao JY, Wang J and Cheng J: The
impact of anti-HBV treatment on the occurrence and recurrence of
hepatocellular carcinoma: Focus on Asian studies. Discov Med.
19:89–99. 2015.PubMed/NCBI
|
|
6
|
Forner A, Llovet JM and Bruix J:
Hepatocellular carcinoma. Lancet. 379:1245–1255. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bruix J and Sherman M; Practice Guidelines
Committee, American Association for the Study of Liver Diseases, .
Management of hepatocellular carcinoma. Hepatology. 42:1208–1236.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tsuchiya N, Sawada Y, Endo I, Saito K,
Uemura Y and Nakatsura T: Biomarkers for the early diagnosis of
hepatocellular carcinoma. World J Gastroenterol. 21:10573–10583.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Spangenberg HC, Thimme R and Blum HE:
Serum markers of hepatocellular carcinoma. Semin Liver Dis.
26:385–390. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Aghoram R, Cai P and Dickinson JA:
Alpha-foetoprotein and/or liver ultrasonography for screening of
hepatocellular carcinoma in patients with chronic hepatitis B.
Cochrane Database Syst Rev. CD002799:2012.
|
|
11
|
Chun S, Rhie SY, Ki CS, Kim JE and Park
HD: Evaluation of alpha-fetoprotein as a screening marker for
hepatocellular carcinoma in hepatitis prevalent areas. Ann Hepatol.
14:882–888. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Giannini EG, Marenco S, Borgonovo G,
Savarino V, Farinati F, Del Poggio P, Rapaccini GL, Anna Di Nolfo
M, Benvegnù L, Zoli M, et al: Alpha-fetoprotein has no prognostic
role in small hepatocellular carcinoma identified during
surveillance in compensated cirrhosis. Hepatology. 56:1371–1379.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Dai M, Chen X, Liu X, Peng Z, Meng J and
Dai S: Diagnostic value of the combination of Golgi Protein 73 and
alpha-fetoprotein in hepatocellular carcinoma: A meta-analysis.
PLoS One. 10:e01400672015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Li D, Mallory T and Satomura S: AFP-L3: A
new generation of tumor marker for hepatocellular carcinoma. Clin
Chim Acta. 313:15–19. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sato Y, Nakata K, Kato Y, Shima M, Ishii
N, Koji T, Taketa K, Endo Y and Nagataki S: Early recognition of
hepatocellular carcinoma based on altered profiles of
alpha-fetoprotein. N Engl J Med. 328:1802–1806. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Marrero JA, Feng Z, Wang Y, Nguyen MH,
Befeler AS, Roberts LR, Reddy KR, Harnois D, Llovet JM, Normolle D,
et al: Alpha-fetoprotein, des-gamma carboxyprothrombin, and
lectin-bound alpha-fetoprotein in early hepatocellular carcinoma.
Gastroenterology. 137:110–118. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sterling RK, Jeffers L, Gordon F, Venook
AP, Reddy KR, Satomura S, Kanke F, Schwartz ME and Sherman M:
Utility of Lens culinaris agglutinin-reactive fraction of
alpha-fetoprotein and des-gamma-carboxy prothrombin, alone or in
combination, as biomarkers for hepatocellular carcinoma. Clin
Gastroenterol Hepatol. 7:104–113. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lok AS, Sterling RK, Everhart JE, Wright
EC, Hoefs JC, Di Bisceglie AM, Morgan TR, Kim HY, Lee WM, Bonkovsky
HL and Dienstag JL; HALT-C Trial Group, . Des-gamma-carboxy
prothrombin and alpha-fetoprotein as biomarkers for the early
detection of hepatocellular carcinoma. Gastroenterology.
138:493–502. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ertle JM, Heider D, Wichert M, Keller B,
Kueper R, Hilgard P, Gerken G and Schlaak JF: A combination of
α-fetoprotein and des-U-carboxy prothrombin is superior in
detection of hepatocellular carcinoma. Digestion. 87:121–131. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Pote N, Cauchy F, Albuquerque M, Voitot H,
Belghiti J, Castera L, Puy H, Bedossa P and Paradis V: Performance
of PIVKA-II for early hepatocellular carcinoma diagnosis and
prediction of microvascular invasion. J Hepatol. 62:848–854. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ma J, Yan R, Zu X, Cheng JM, Rao K, Liao
DF and Cao D: Aldo-keto reductase family 1 B10 affects fatty acid
synthesis by regulating the stability of acetyl-CoA
carboxylase-alpha in breast cancer cells. J Biol Chem.
283:3418–3423. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wang C, Yan R, Luo D, Watabe K, Liao DF
and Cao D: Aldo-keto reductase family 1 member B10 promotes cell
survival by regulating lipid synthesis and eliminating carbonyls. J
Biol Chem. 284:26742–26748. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Cao D, Fan ST and Chung SS: Identification
and characterization of a novel human aldose reductase-like gene. J
Biol Chem. 273:11429–11435. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Conklin D, Prough R and Bhatanagar A:
Aldehyde metabolism in the cardiovascular system. Mol Biosyst.
3:136–150. 2007. View
Article : Google Scholar : PubMed/NCBI
|
|
25
|
Spite M, Baba SP, Ahmed Y, Barski OA,
Nijhawan K, Petrash JM, Bhatnagar A and Srivastava S: Substrate
specificity and catalytic efficiency of aldo-keto reductases with
phospholipid aldehydes. Biochem J. 405:95–105. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Yan R, Zu X, Ma J, Liu Z, Adeyanju M and
Cao D: Aldo-keto reductase family 1 B10 gene silencing results in
growth inhibition of colorectal cancer cells: Implication for
cancer intervention. Int J Cancer. 121:2301–2306. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Martin HJ and Maser E: Role of human
aldo-keto-reductase AKR1B10 in the protection against toxic
aldehydes. Chem Biol Interact. 178:145–150. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhong L, Liu Z, Yan R, Johnson S, Zhao Y,
Fang X and Cao D: Aldo-keto reductase family 1 B10 protein
detoxifies dietary and lipid-derived alpha, beta-unsaturated
carbonyls at physiological levels. Biochem Biophys Res Commun.
387:245–250. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Crosas B, Hyndman DJ, Gallego O, Martras
S, Parés X, Flynn TG and Farrés J: Human aldose reductase and human
small intestine aldose reductase are efficient retinal reductases:
Consequences for retinoid metabolism. Biochem J. 373:973–979. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Gallego O, Belyaeva OV, Porte S, Ruiz FX,
Stetsenko AV, Shabrova EV, Kostereva NV, Farrés J, Parés X and
Kedishvili NY: Comparative functional analysis of human
medium-chain dehydrogenases, short-chain dehydrogenases/reductases
and aldo-keto reductases with retinoids. Biochem J. 399:101–109.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Matkowskyj KA, Bai H, Liao J, Zhang W, Li
H, Rao S, Omary R and Yang GY: Aldoketoreductase family 1B10
(AKR1B10) as a biomarker to distinguish hepatocellular carcinoma
from benign liver lesions. Hum Pathol. 45:834–843. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Heringlake S, Hofdmann M, Fiebeler A,
Manns MP, Schmiegel W and Tannapfel A: Identification and
expression analysis of the aldo-ketoreductase1-B10 gene in primary
malignant liver tumours. J Hepatol. 52:220–227. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Luo DX, Huang MC, Ma J, Gao Z, Liao DF and
Cao D: Aldo-keto reductase family 1, member B10 is secreted through
a lysosome-mediated non-classical pathway. Biochem J. 438:71–80.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Sato S, Genda T, Hirano K, Tsuzura H,
Narita Y, Kanemitsu Y, Kikuchi T, Iijima K, Wada R and Ichida T:
Up-regulated aldo-keto reductase family 1 member B10 in chronic
hepatitis C: Association with serum alpha-fetoprotein and
hepatocellular carcinoma. Liver Int. 32:1382–1390. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Mori M, Genda T, Ichida T, Murata A, Kamei
M, Tsuzura H, Sato S, Narita Y, Kanemitsu Y, Ishikawa S, et al:
Aldo-keto reductase family 1 member B10 is associated with
hepatitis B virus-related hepatocellular carcinoma risk. Hepatol
Res. 47:E85–E93. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Murata A, Genda T, Ichida T, Amano N, Sato
S, Tsuzura H, Sato S, Narita Y, Kanemitsu Y, Shimada Y, et al:
Pretreatment AKR1B10 expression predicts the risk of hepatocellular
carcinoma development after hepatitis C virus eradication. World J
Gastroenterol. 22:7569–7578. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Schmitz KJ, Sotiropoulos GC, Baba HA,
Schmid KW, Müller D, Paul A, Auer T, Gamerith G and Loeffler-Ragg
J: AKR1B10 expression is associated with less aggressive
hepatocellular carcinoma: A clinicopathological study of 168 cases.
Liver Int. 31:810–816. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Ha SY, Song DH, Lee JJ, Lee HW, Cho SY and
Park CK: High expression of aldo-keto reductase 1B10 is an
independent predictor of favorable prognosis in patients with
hepatocellular carcinoma. Gut Liver. 8:648–654. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Chinese Society of Hepatology and Chinese
Society of Infectious Diseases, Chinese Medical Association: The
guideline of prevention and treatment for chronic hepatitis B (2010
version). Zhonghua Gan Zang Bing Za Zhi. 19:13–24. 2011.(In
Chinese). PubMed/NCBI
|
|
40
|
Llovet JM, Brú C and Bruix J: Prognosis of
hepatocellular carcinoma: The BCLC staging classification. Semin
Liver Dis. 19:329–338. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Bruix J and Sherman M; American
Association for the Study of Liver Diseases, . Management of
hepatocellular carcinoma: An update. Hepatology. 53:1020–1022.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Trevisani F, D'Intino PE, Morselli-Labate
AM, Mazzella G, Accogli E, Caraceni P, Domenicali M, De Notariis S,
Roda E and Bernardi M: Serum alpha-fetoprotein for diagnosis of
hepatocellular carcinoma in patients with chronic liver disease:
Influence of HBsAg and anti-HCV status. J Hepatol. 34:570–575.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Bellissimo F, Pinzone MR, Cacopardo B and
Nunnari G: Diagnostic and therapeutic management of hepatocellular
carcinoma. World J Gastroenterol. 21:12003–12021. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Chaiteerakij R, Zhang X, Addissie BD,
Mohamed EA, Harmsen WS, Theobald PJ, Peters BE, Balsanek JG, Ward
MM, Giama NH, et al: Combinations of biomarkers and Milan criteria
for predicting hepatocellular carcinoma recurrence after liver
transplantation. Liver Transpl. 21:599–606. 2015. View Article : Google Scholar : PubMed/NCBI
|