Introduction
According to a large-scale survey of 36 types of
cancer spanning 185 countries in 2018, lung cancer ranks first in
the global cancer incidence (11.6%) and mortality rates (18.4%)
(1). In China, lung cancer also
accounts for the highest cancer-related morbidity and mortality
(2). Among all pathological types of
lung cancer, non-small cell lung cancer (NSCLC) accounts for ~80%
of cases, making it the most common histological type, with a
5-year survival rate of only 15%. Patients with lung cancer are
usually diagnosed at an advanced stage (3). However, with the widespread application
of low-dose helical computed tomography (CT) in clinical practice,
early- or intermediate-stage NSCLC is being diagnosed in an
increasing number of asymptomatic patients (4). For patients with early- or
intermediate-stage lung cancer, surgery is the first and most
effective treatment method, as well as the only method that can
cure NSCLC. However, the influence of different surgical methods on
the prognosis of patients is still controversial (5–7).
The concept of precision medicine (8) has facilitated the development of
medical methodology specific to the patient. In contrast to the
original ‘one size fits all’ approach, medical professionals can
adjust the treatment according to subtle differences in patients to
maximize the outcome. Based on this, the latest (8th) edition of
the Tumor-Node-Metastasis (TNM) staging system can more accurately
predict the prognosis of lung cancer patients (9). However, it is necessary to combine
variables such as age, sex, degree of tumor differentiation and
treatment to further predict the survival rate of patients with
lung cancer, as predicting the prognosis of patients exclusively by
TNM stage of NSCLC is insufficient.
Nomograms are based on multifactor regression
analyses and integrate multiple predictive indexes with visual
graphics, which makes the results of the prediction model readable
and the prognosis of patients easy to evaluate (10). Despite a number of nomograms based on
large samples for predicting the prognosis of patients with lung
cancer, limited studies have been performed on stage II or III
NSCLC. Therefore, the present study aimed to construct a nomogram
based on early (11,12) and advanced (13) lung cancer using large-scale data
obtained from the Surveillance, Epidemiology and End Results (SEER)
database containing information on the clinical characteristics and
patient survival.
Materials and methods
Data collection
Data were extracted from the SEER database
(https://seer.cancer.gov) by SEER*Stat Software
(version 8.3.5; http://seer.cancer.gov/data-software/), and the
Incidence SEER 18 Regs Custom Data (with additional treatment
fields), Nov 2017 Sub (1973–2015 varying), were selected for
analysis. Data were limited to patients diagnosed with stage II and
III lung cancer between January 1, 2010 to November 31, 2015. The
retrieval formula based on the inclusion criteria displayed in the
software was {Site and Morphology. CS Schema v0204+}=‘Lung’ AND
{Stage-American Joint Committee on Cancer (AJCC). Derived AJCC
Stage Group, 7th ed. (2010+)}
=‘II’,‘IIA’,‘IIA1’,‘IIA2’,‘IIB’,‘IIC’,‘III’,‘IIIA’,‘IIIB’,‘IIIC’,‘IIIC1’,‘IIIC2’
AND {Race, Sex, Year Dx, Registry, County, Year of
diagnosis}=‘2010’,‘2011’,‘2012’,‘2013’,‘2014’,‘2015’. The clinical
information of the patients included patient ID, age at diagnosis,
diagnostic confirmation, race (Caucasian, African-American or
other), sex, marital status at diagnosis, histologic type, grade,
primary site and laterality, AJCC stage, T stage, N stage, surgery
at primary site, scope of regional lymph node surgery, radiation
therapy, chemotherapy, survival months, vital status, first
malignant primary indicator and sequence number.
Once the preliminary data were obtained, patients
were excluded based on the following exclusion criteria: i)
Clinical information of the patient was missing; ii) diagnostic
confirmation was not consistent with positive histology, such as
only clinical diagnosis or direct visualization without microscopic
confirmation; iii) patient was <18 years; iv) survival time was
<1 month; v) the meaning of the patient's relevant code was
unclear or had other meaning that could not be included in the
study; for example, in a surgical procedure, 00 refers to no
surgery, 21 refers to wedge resection, 22 refers to segmental
resection, and 31 refers to lobectomy, and patients with additional
codes, such as 41–49, were excluded; vi) the data point applied to
a small number of patients; for example, only 23 patients underwent
pneumonectomy and were thus excluded; vii) the patient had more
than one primary tumor.
The data were divided into two groups based on
patient age (≤60 and >60 years). In addition, regarding marital
status, patients who were widowed, divorced, unmarried or domestic
partners and single (unmarried) were all considered unmarried. In
terms of pathological types, only four pathological tissue types
were included: Adenocarcinoma (ADC), squamous cell carcinoma (SCC),
large cell carcinoma (LCC) and adenosquamous carcinoma (ASC).
Regarding radiotherapy, patients were divided into two groups: Yes
and no, where beam radiation, radioactive implants, and
radioisotopes were all considered as ‘yes’. The remaining clinical
information was determined via the specific meaning of the code and
the specific output of the software.
Statistical analysis
The random allocation method was used to divide the
data into a training set and a validation set at a 7:3 ratio.
Median survival time with 95% confidence intervals (CIs) for the
two groups was determined using the Kaplan-Meier method. In the
training cohort, unadjusted univariate Cox regression analysis was
used for all variables included in the study. P<0.05 was
considered to indicate a statistically significant difference.
Factors with statistical significance according to the results of
the unadjusted univariate Cox regression analysis were included in
the multivariate Cox regression analysis to identify independent
risk factors. These independent risk factors were used to construct
a nomogram using R software version 3.5.1 (64 bit; http://www.r-project.org) using the rms (14) and survival packages (https://www.rdocumentation.org/packages/survival/versions/2.42-3).
The nomogram used 3- and 5-year overall survival (OS) as end
points. Harrell's concordance indexes (C-indexes) (15) and calibration curves were used to
verify the predicted effect of the nomogram. The training set was
used for internal validation, and the validation set was used for
external validation. Bootstraps of 1,000 resamples were used for
analysis. In addition, to validate the ability of the nomogram to
discriminate patients with different TNM stages, patients in the
validation set were assigned into four groups according to the
quartiles of their prognostic scores. The Kaplan-Meier method was
used to estimate overall survival rate in the four groups, and the
differences were evaluated using the log-rank test with a threshold
of P<0.05.
Results
Patient clinicopathological
characteristics
According to the inclusion and exclusion criteria,
15,344 patients with stage II and III NSCLC were included in the
study. Among them, 3,261 patients had stage IIA, 2,865 had stage
IIB, 6,851 had stage IIIA and 2,367 had stage IIIB NSCLC. The mean
age was 68.41 (range, 15–101 years) years. The patients were
divided into two random groups at a ratio of 7:3 to form the
training and validation sets, comprising 10,744 and 4,600 patients,
respectively. The median survival was 22.00 months and the 3- and
5-year survival rates were 0.638 and 0.512 for the training set.
The median survival was 23.50 months and the 3- and 5-year survival
rates were 0.666 and 0.551 for the validation set. The clinical
characteristics and survival information of the two sets are
presented in Tables I and II.
 | Table I.Clinical characteristics of the
training set. |
Table I.
Clinical characteristics of the
training set.
|
|
| OS, months | OS, % |
|
|---|
|
|
|
|
|
|
|---|
| Characteristic | No. of
patients | Median | 95% CI | 3-year | 5-year | Log-rank
P-value |
|---|
| Age |
|
|
|
|
|
|
|
≤60 | 2,360 | 34 | 30.61–37.39 | 48.5±1.2 | 39.4±1.4 | <0.001 |
|
>60 | 8,384 | 21 | 21.13–21.87 | 35.8±0.6 | 25.4±0.7 |
|
| Sex |
|
|
|
|
|
|
|
Male | 5,929 | 19 | 18.06–19.94 | 34.1±0.7 | 25.9±0.8 | <0.001 |
|
Female | 4,815 | 29 | 27.22–30.78 | 43.3±0.9 | 31.7±1.0 |
|
| Marital status |
|
|
|
|
|
|
|
Married | 5,896 | 25 | 23.67–26.33 | 34.1±0.7 | 25.3±0.9 | <0.001 |
|
Unmarried | 4,848 | 21 | 19.83–22.16 | 36.1±0.8 | 25.0±1.0 |
|
| Race |
|
|
|
|
|
|
|
Caucasian | 8,623 | 25 | 23.67–26.33 | 37.7±0.6 | 28.2±0.7 | <0.001 |
|
African-American | 1,274 | 21 | 19.83–22.17 | 39.7±1.6 | 27.1±2.0 |
|
|
Other | 847 | 23 | 22.15–23.87 | 46.2±2.1 | 34.3±2.4 |
|
| Histology |
|
|
|
|
|
|
|
ADC | 5,552 | 32 | 30.17–33.83 | 46.1±0.8 | 33.9±1.0 | <0.001 |
|
SCC | 4,784 | 16 | 15.12–16.87 | 29.6±0.8 | 22.2±0.9 |
|
|
LCC | 270 | 22 | 17.86–26.14 | 37.0±3.5 | 26.8±4.2 |
|
|
ASC | 138 | 17 | 13.13–20.87 | 78.4±3.6 | 61.2±4.3 |
|
| Grade |
|
|
|
|
|
|
| I | 765 | 31 | 26.10–35.89 | 46.4±2.2 | 30.2±2.9 | <0.001 |
| II | 4,379 | 26 | 24.43–27.56 | 41.6±0.9 | 31.1±1.0 |
|
|
III | 5,441 | 20 | 18.96–21.04 | 35.3±0.8 | 26.2±0.9 |
|
| IV | 159 | 17 | 12.84–21.16 | 34.7±4.3 | 29.8±4.6 |
|
| AJCC (7th) T stage
(45) |
|
|
|
|
|
|
| T1 | 1,324 | 32 | 27.81–36.20 | 47.1±1.6 | 34.2±2.1 | <0.001 |
| T2 | 3,996 | 27 | 25.24–28.76 | 42.0±0.9 | 31.0±1.1 |
|
| T3 | 3,419 | 23 | 21.53–24.47 | 38.5±1.0 | 29.3±1.1 |
|
| T4 | 2,005 | 14 | 12.90–15.10 | 26.3±1.2 | 17.9±1.3 |
|
| AJCC (7th) N stage
(45) |
|
|
|
|
|
|
| N0 | 3,362 | 29 | 26.56–31.44 | 45.3±1.0 | 34.2±1.2 | <0.001 |
| N1 | 2,293 | 35 | 31.84–38.16 | 48.6±1.3 | 36.9±1.5 |
|
| N2 | 4,323 | 18 | 17.03–18.97 | 31.1±0.8 | 21.9±0.9 |
|
| N3 | 766 | 13 | 11.91–14.08 | 22.0±1.8 | 13.8±2.0 |
|
| Primary site |
|
|
|
|
|
|
| Main
bronchus | 302 | 12 | 9.78–14.21 | 33.9±0.9 | 25.4±1.0 | <0.001 |
| Upper
lobe | 6,650 | 24 | 22.86–25.13 | 39.4±0.7 | 30.2±0.8 |
|
| Middle
lobe | 460 | 28 | 23.24–32.76 | 43.6±2.8 | 31.9±3.4 |
|
| Lower
lobe | 3,332 | 23 | 21.49–24.51 | 37.9±1.0 | 26.6±1.2 |
|
| Laterality |
|
|
|
|
|
|
|
Left | 4,448 | 23 | 21.64–24.37 | 38.9±0.9 | 29.4±1.0 | 0.346 |
|
Right | 6,296 | 23 | 21.85–24.15 | 38.5±0.7 | 27.9±0.8 |
|
| Surgery |
|
|
|
|
|
|
|
None | 5,757 | 13 | 12.49–13.51 | 20.2±0.7 | 12.2±0.7 | <0.001 |
| Wedge
resection | 351 | 30 | 24.78–35.22 | 45.9±3.2 | 35.6±3.7 |
|
|
Segmental resection | 114 | 41 | 28.39–53.61 | 52.5±5.9 | 37.6±7.2 |
|
|
Lobectomy | 4,522 | 56 | 51.17–60.83 | 60.4±0.9 | 47.9±1.1 |
|
| Lymph node
dissection |
|
|
|
|
|
|
|
None | 5,652 | 13 | 12.49–13.51 | 20.2±0.7 | 12.2±0.7 | <0.001 |
|
1–3 | 651 | 40 | 33.07–46.93 | 45.9±3.2 | 35.6±3.7 |
|
| ≥4 | 4,441 | 53 | 48.87–23.87 | 60.4±0.9 | 47.9±1.1 |
|
| Radiation |
|
|
|
|
|
|
| No | 5,152 | 19 | 18.17–19.83 | 33.9±0.9 | 25.4±1.0 | <0.001 |
|
Yes | 5,592 | 29 | 27.12–30.88 | 45.1±0.8 | 35.5±0.9 |
|
| Chemotherapy |
|
|
|
|
|
|
| No | 4,185 | 18 | 16.81–19.19 | 33.9±0.9 | 25.4±1.0 | <0.001 |
|
Yes | 6,559 | 27 | 25.73–28.27 | 41.6±0.7 | 30.5±0.9 |
|
| Table II.Clinical characteristics of the
validation set. |
Table II.
Clinical characteristics of the
validation set.
|
|
| OS, months | OS, % |
|
|---|
|
|
|
|
|
|
|---|
| Characteristic | No. of
patients | Median | 95% CI | 3-year | 5-year | Log-rank
P-value |
|---|
| Age |
|
|
|
|
|
|
|
≤60 | 1,041 | 30 | 24.54–34.54 | 45.7±1.8 | 34.6±2.1 | <0.001 |
|
>60 | 3,559 | 21 | 19.68–22.31 | 34.6±1.0 | 23.7±1.1 |
|
| Sex |
|
|
|
|
|
|
|
Male | 2,507 | 20 | 18.77–21.22 | 31.7±1.1 | 22.3±1.2 | <0.001 |
|
Female | 2,093 | 28 | 25.31–30.69 | 43.9±1.3 | 31.3±1.6 |
|
| Marital status |
|
|
|
|
|
|
|
Married | 2,519 | 26 | 24.01–27.98 | 41.8±1.2 | 30.0±1.3 | <0.001 |
|
Unmarried | 2,081 | 20 | 18.44–21.55 | 31.5±1.2 | 21.5±1.4 |
|
| Race |
|
|
|
|
|
|
|
Caucasian | 3,713 | 22 | 20.68–23.32 | 36.8±0.9 | 26.1±1.1 | 0.035 |
|
African-American | 547 | 22 | 19.31–24.68 | 35.2±2.5 | 26.3±2.7 |
|
|
Other | 340 | 31 | 25.94–36.05 | 44.2±3.4 | 25.4±3.9 |
|
| Histology |
|
|
|
|
|
|
|
ADC | 2,420 | 31 | 28.66–33.33 | 41.8±1.2 | 30.0±1.3 | <0.001 |
|
SCC | 2,026 | 16 | 14.69–17.30 | 28.1±1.2 | 19.1±1.3 |
|
|
LCC | 103 | 30 | 18.56–41.43 | 43.9±5.8 | 33.4±6.1 |
|
|
ASC | 31 | 15 | 7.23–22.77 | 31.5±1.2 | 21.5±1.4 |
|
| Grade |
|
|
|
|
|
|
| I | 370 | 41 | 30.81–51.18 | 52.0±3.1 | 40.1±3.9 | <0.001 |
| II | 1,837 | 26 | 23.79–28.20 | 40.7±1.4 | 27.4±1.6 |
|
|
III | 2,334 | 19 | 17.62–20.37 | 32.2±1.2 | 23.0±1.2 |
|
| IV | 59 | 20 | 9.21–30.78 | 37.2±7.1 | 30.1±7.4 |
|
| AJCC (7th) T stage
(45) |
|
|
|
|
|
|
| T1 | 601 | 37 | 28.94–45.05 | 50.9±2.4 | 35.1±3.0 | <0.001 |
| T2 | 1,718 | 25 | 22.64–27.35 | 39.6±1.4 | 27.3±1.6 |
|
| T3 | 1,444 | 23 | 21.08–24.91 | 36.5±1.5 | 26.0±1.7 |
|
| T4 | 837 | 13 | 11.45–14.54 | 23.4±1.8 | 16.0±1.9 |
|
| AJCC (7th) N stage
(45) |
|
|
|
|
|
|
| N0 | 1,433 | 30 | 26.09–33.90 | 45.6±1.6 | 35.4±1.9 | <0.001 |
| N1 | 990 | 34 | 29.35–38.46 | 48.7±1.9 | 32.3±2.3 |
|
| N2 | 1,848 | 18 | 16.68–19.32 | 27.9±1.2 | 18.6±1.3 |
|
| N3 | 329 | 13 | 10.62–15.37 | 19.7±2.8 | 4.5±3.5 |
|
| Primary site |
|
|
|
|
|
|
| Main
bronchus | 118 | 14 | 9.43–18.57 | 18.1±4.4 | 12.1±5.7 | <0.001 |
| Upper
lobe | 2,869 | 22 | 20.46–23.53 | 37.0±1.1 | 25.4±1.2 |
|
| Middle
lobe | 181 | 22 | 17.03–26.96 | 36.2±4.3 | 32.2±4.7 |
|
| Lower
lobe | 1,432 | 25 | 22.55–27.48 | 39.2±1.6 | 28.6±1.8 |
|
| Laterality |
|
|
|
|
|
|
|
Left | 1,913 | 23 | 20.98–25.01 | 37.7±1.3 | 26.2±1.5 | 0.932 |
|
Right | 2,687 | 23 | 21.48–24.51 | 36.8±1.1 | 26.4±1.2 |
|
| Surgery |
|
|
|
|
|
|
|
None | 2,433 | 13 | 12.23–13.77 | 17.9±1.0 | 9.4±1.0 | <0.001 |
| Wedge
resection | 163 | 35 | 26.19–43.80 | 47.8±5.0 | 30.7±6.5 |
|
|
Segmental resection | 45 | 31 | 24.01–37.98 | 46.9±9.1 | 37.5±9.4 |
|
|
Lobectomy | 1,959 | 50 | 44.69–55.03 | 60.0±1.3 | 45.3±1.6 |
|
| Lymph node
dissection |
|
|
|
|
|
|
|
None | 2,398 | 13 | 12.20–13.79 | 18.3±1.0 | 10.1±1.0 | <0.001 |
|
1–3 | 306 | 35 | 29.49–40.51 | 46.5±3.4 | 29.2±4.2 |
|
| ≥4 | 1,896 | 50 | 44.13–55.87 | 59.5±1.4 | 45.4±1.7 |
|
| Radiation |
|
|
|
|
|
|
| No | 2,176 | 19 | 17.75–20.25 | 28.6±1.2 | 19.3±1.2 | <0.001 |
|
Yes | 2,424 | 30 | 27.34–32.65 | 44.9±1.2 | 32.7±1.4 |
|
| Chemotherapy |
|
|
|
|
|
|
| No | 1,812 | 18 | 16.04–19.96 | 33.9±1.3 | 24.9±1.5 | <0.001 |
|
Yes | 2,788 | 25 | 23.32–26.67 | 39.3±1.1 | 27.3±1.3 |
|
Cox regression analysis
The following factors were included in the
univariate Cox regression analysis: Age (≤60 vs. >60), race
(Caucasian vs. African-American vs. other), sex (male vs. female),
marital status (married vs. unmarried), histological type (ADC vs.
SCC vs. LCC vs. ADC), grade (well differentiated, grade I vs.
moderately differentiated, grade II vs. poorly differentiated,
grade III vs. undifferentiated or anaplastic, grade IV), primary
site (main bronchus vs. upper lobe vs. middle lobe vs. lower lobe),
latency (left vs. right), T stage (T1 vs. T2 vs. T3 vs. T4), N
stage (N0 vs. N1 vs. N2 vs. N3), surgery at primary site (none vs.
wedge resection vs. segmental resection vs. lobectomy), scope of
regional lymph node surgery (none vs. 1–3 regional lymph nodes
removed vs. ≥4 regional lymph nodes removed), radiation therapy
(yes vs. no) and chemotherapy (yes vs. no). The results of the
univariate Cox regression analysis indicated no significant
difference regarding laterality (P=0.353). The remaining prognostic
factors with P<0.05 were included in the multivariate Cox
regression analysis. The results demonstrated that all included
factors, with the exception of the primary site, were independent
prognostic factors and were thus included in the construction of
the nomogram (Table III).
| Table III.Results of the univariate and
multivariate Cox regression analysis. |
Table III.
Results of the univariate and
multivariate Cox regression analysis.
|
| Univariate
analysis |
| Multivariate
analysis |
|
|---|
|
|
|
|
|
|
|---|
| Characteristic | Hazard ratio | 95% CI | P-value | Hazard ratio | 95% CI | P-value |
|---|
| Age |
|
|
|
|
|
|
|
≤60 | Reference |
|
| Reference |
|
|
|
>60 | 1.479 | 1.383–1.581 | <0.001 | 1.293 | 1.208–1.205 | <0.001 |
| Sex |
|
|
|
|
|
|
|
Male | Reference |
|
| Reference |
|
|
|
Female | 0.762 | 0.723–0.804 | <0.001 | 0.770 | 0.728–0.813 | <0.001 |
| Marital status |
|
|
|
|
|
|
|
Married | Reference |
|
| Reference |
|
|
|
Unmarried | 1.167 | 1.108–1.229 | <0.001 | 1.103 | 1.043–1.165 | <0.001 |
| Race |
|
|
|
|
|
|
|
Caucasian | Reference |
|
| Reference |
|
|
|
African-American | 0.987 | 0.911–1.069 | 0.745 | 0.893 | 0.822–0.968 | 0.007 |
|
Other | 0.804 | 0.725–0.890 | <0.001 | 0.825 | 0.744–0.914 | <0.001 |
| Histology |
|
|
|
|
|
|
|
ADC | Reference |
|
| Reference |
|
|
|
SCC | 1.651 | 1.566–1.741 | <0.001 | 1.210 | 1.143–1.281 | <0.001 |
|
LCC | 1.261 | 1.068–1.488 | 0.006 | 1.367 | 1.157–1.614 | <0.001 |
|
ASC | 1.369 | 1.090–1.720 | 0.007 | 1.031 | 0.796–1.336 | 0.816 |
| Grade |
|
|
|
|
|
|
| I | Reference |
|
| Reference |
|
|
| II | 1.159 | 1.036–1.297 | 0.010 | 1.140 | 1.016–1.280 | 0.025 |
|
III | 1.423 | 1.274–1.589 | <0.001 | 1.290 | 1.152–1.445 | <0.001 |
| IV | 1.490 | 1.184–1.874 | 0.001 | 1.387 | 1.073–1.792 | 0.013 |
| AJCC (7th) T stage
(45) |
|
|
|
|
|
|
| T1 | Reference |
|
| Reference |
|
|
| T2 | 1.170 | 1.069–1.281 | 0.001 | 1.094 | 0.997–1.199 | 0.056 |
| T3 | 1.333 | 1.216–1.461 | <0.001 | 1.275 | 1.158–1.405 | <0.001 |
| T4 | 1.900 | 1.725–2.092 | <0.001 | 1.387 | 1.247–1.530 | <0.001 |
| AJCC (7th) N stage
(45) |
|
|
|
|
|
|
| N0 | Reference |
|
| Reference |
|
|
| N1 | 0.864 | 0.799–0.935 | <0.001 | 1.248 | 1.147–1.358 | <0.001 |
| N2 | 1.442 | 1.354–1.535 | <0.001 | 1.478 | 1.379–1.584 | <0.001 |
| N3 | 1.915 | 1.733–2.116 | <0.001 | 1.501 | 1.349–1.668 | <0.001 |
| Primary site |
|
|
|
|
|
|
| Main
bronchus | Reference |
|
| Reference |
|
|
| Upper
lobe | 0.559 | 0.488–0.641 | <0.001 | 0.887 | 0.773–1.019 | 0.092 |
| Middle
lobe | 0.499 | 0.414–0.602 | <0.001 | 0.893 | 0.739–1.079 | 0.244 |
| Lower
lobe | 0.582 | 0.505–0.669 | <0.001 | 1.022 | 0.885–1.180 | 0.762 |
| Laterality |
|
|
|
|
|
|
|
Left | Reference |
|
| NS |
|
|
|
Right | 1.025 | 0.973–1.081 | 0.353 | NS |
|
|
| Surgery |
|
|
|
|
|
|
|
None | Reference |
|
| Reference |
|
|
| Wedge
resection | 0.446 | 0.381–0.522 | <0.001 | 0.488 | 0.409–0.582 | <0.001 |
|
Segmental resection | 0.392 | 0.292–0.526 | <0.001 | 0.453 | 0.330–0.622 | <0.001 |
|
Lobectomy | 0.300 | 0.283–0.318 | <0.001 | 0.389 | 0.334–0.452 | <0.001 |
| Lymph node
dissection |
|
|
|
|
|
|
|
None | Reference |
|
| Reference |
|
|
|
1–3 | 0.395 | 0.350–0.447 | <0.001 | 0.815 | 0.697–0.953 | 0.010 |
| ≥4 | 0.312 | 0.294–0.331 | <0.001 | 0.742 | 0.641–0.857 | <0.001 |
| Radiation |
|
|
|
|
|
|
| No | Reference |
|
| Reference |
|
|
|
Yes | 0.751 | 0.712–0.791 | <0.001 | 0.756 | 0.710–0.805 | <0.001 |
| Chemotherapy |
|
|
|
|
|
|
| No | Reference |
|
| Reference |
|
|
|
Yes | 0.706 | 0.670–0.744 | <0.001 | 0.632 | 0.596–0.670 | <0.001 |
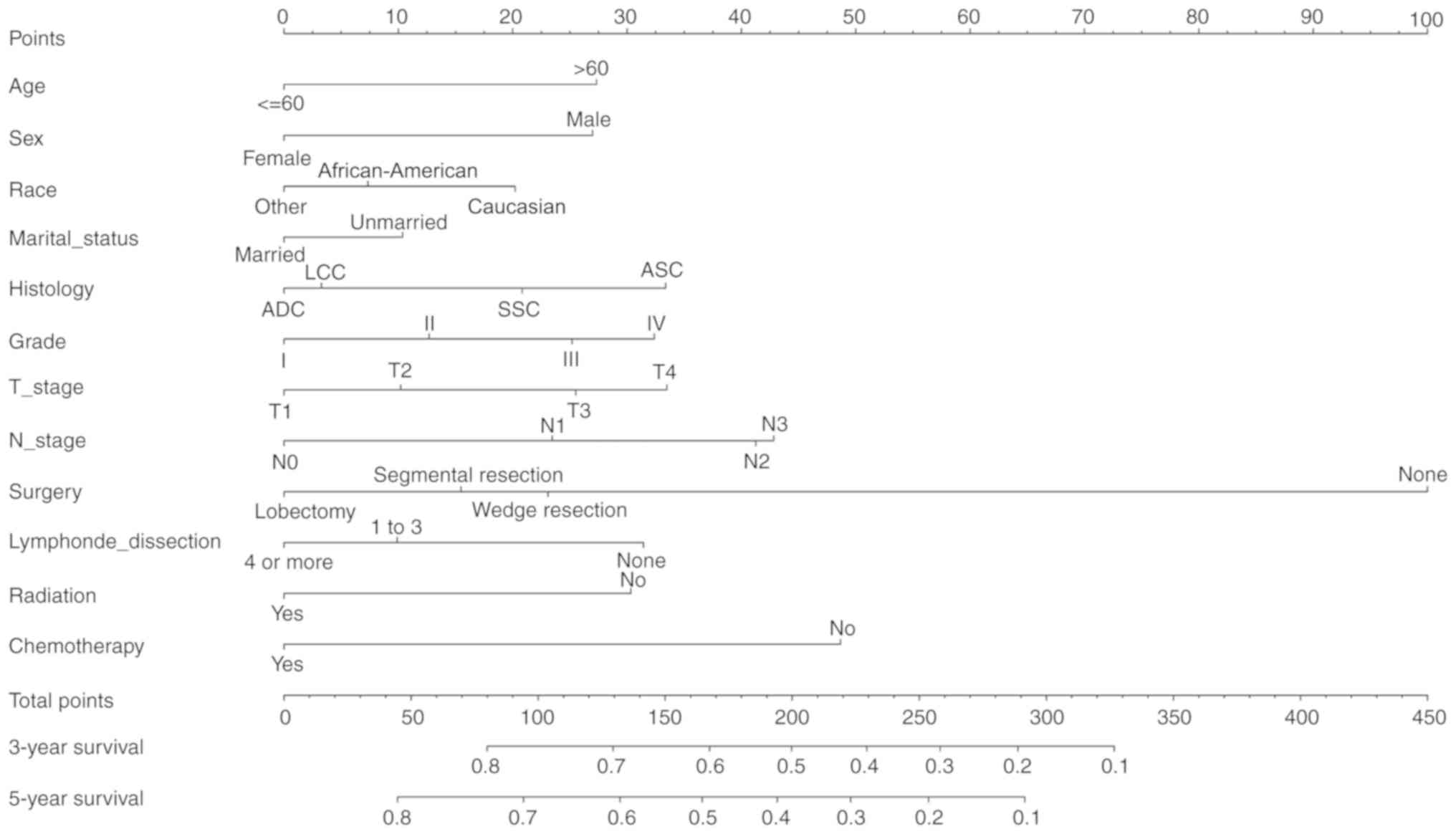
Construction and validation of the
nomogram
The nomogram comprised 12 prognostic factors: Age,
sex, race, marital status, histological type, grade, T stage, N
stage, surgery type, extent of lymph node dissection, radiation
therapy and chemotherapy. Surgery, especially lobectomy, exhibited
the strongest impact on prognosis among all factors; chemotherapy
also served an important role (Fig.
1). Marriage had a relatively small effect on prognosis. The
effects of other factors on prognosis were moderate. A total score
was calculated by adding up the scores of each factor according to
the different characteristics. The 3- and 5-year survival rates
were estimated by drawing a straight line from the total score on
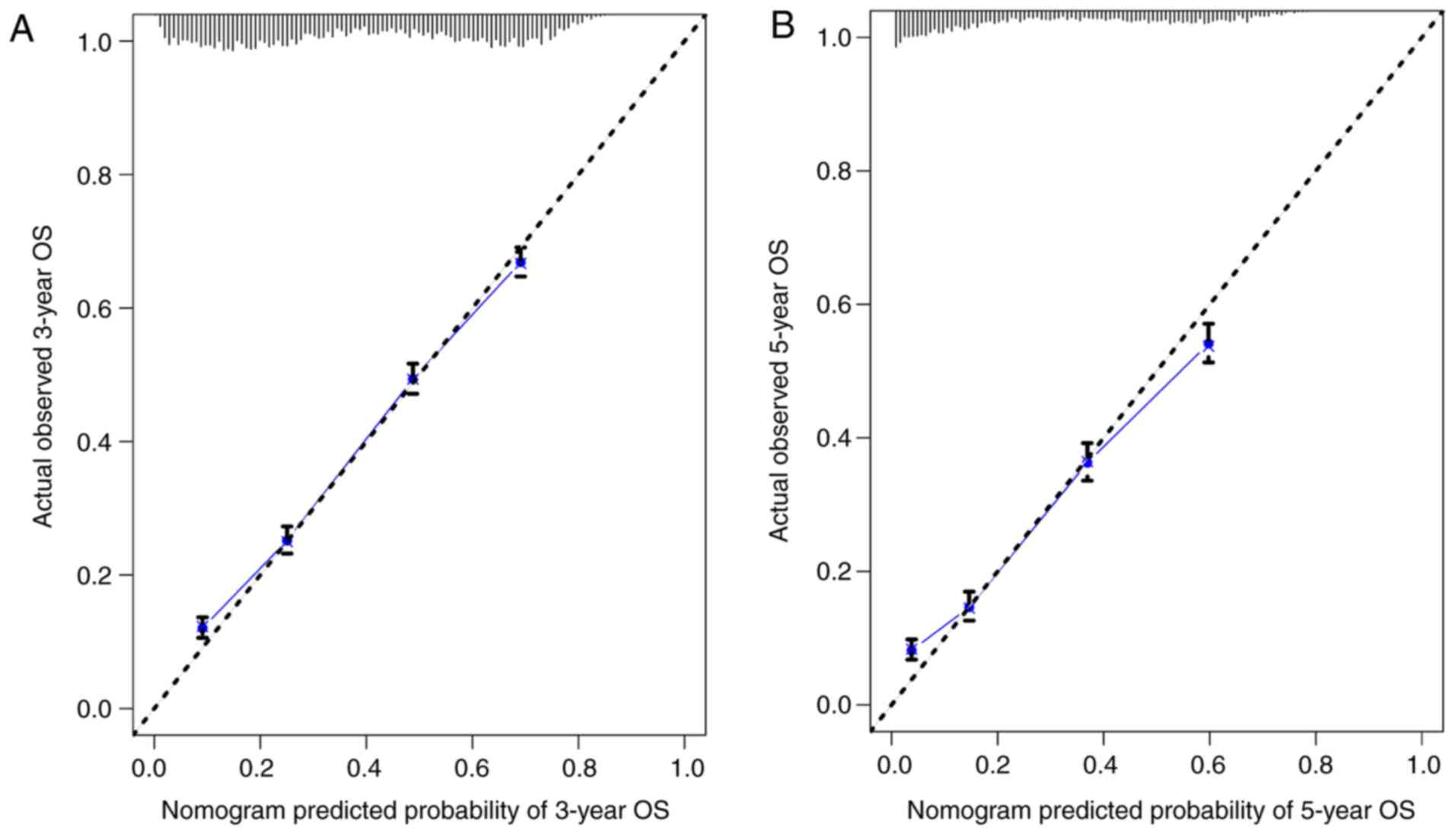
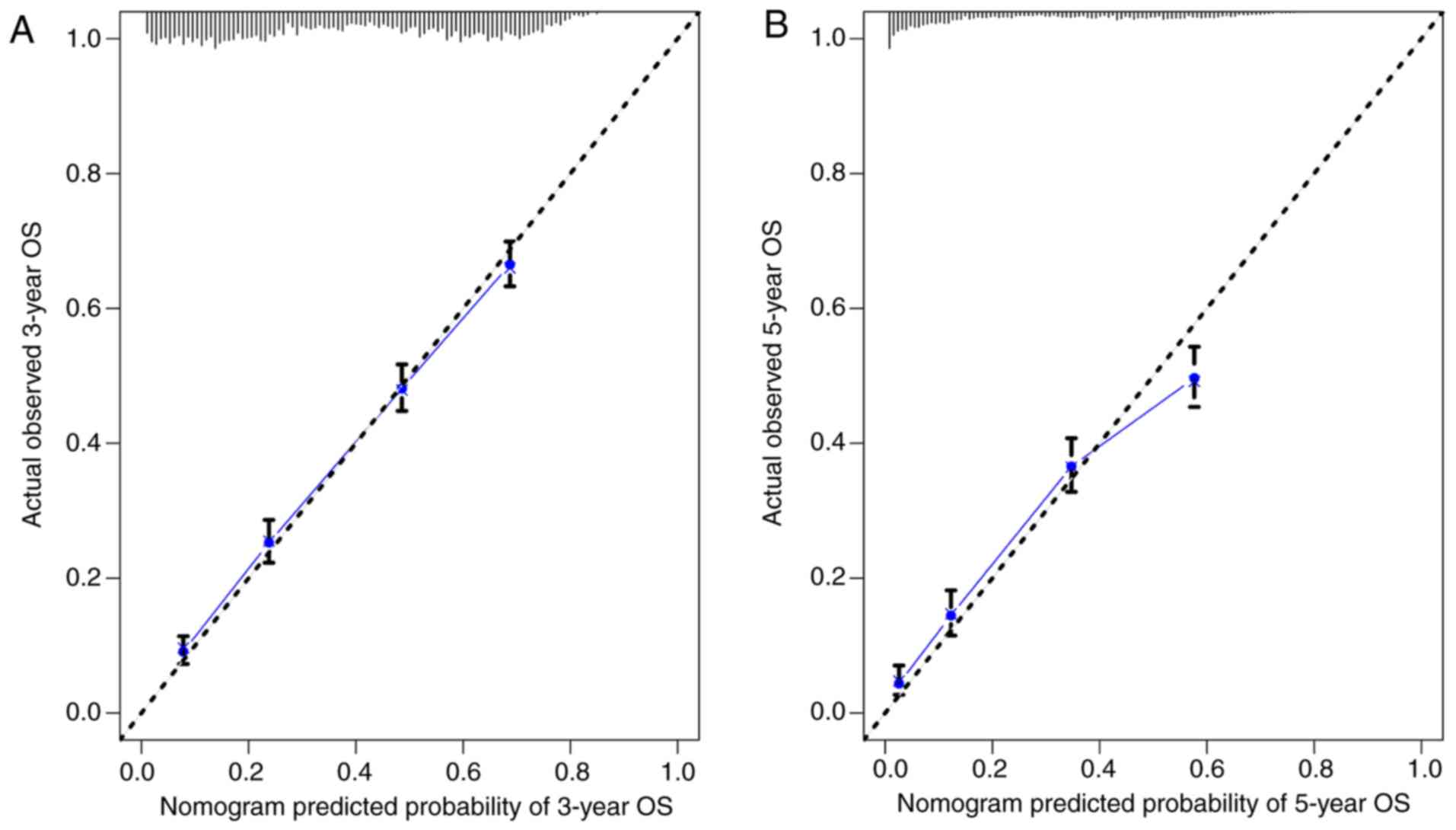
the nomogram. The C-index calculated by the bootstrap self-sampling
method was 0.719 (95% CI, 0.718–0.719) in the training set and
0.721 (95% CI, 0.720–0.722) in the validation set, indicating good
predictability of the nomogram. In addition, the calibration curve
was similar to the standard curve in predicting the 3- and 5-year
survival rates of patients from the training set and validation
set, indicating good predictive ability of the nomogram (Figs. 2 and 3).
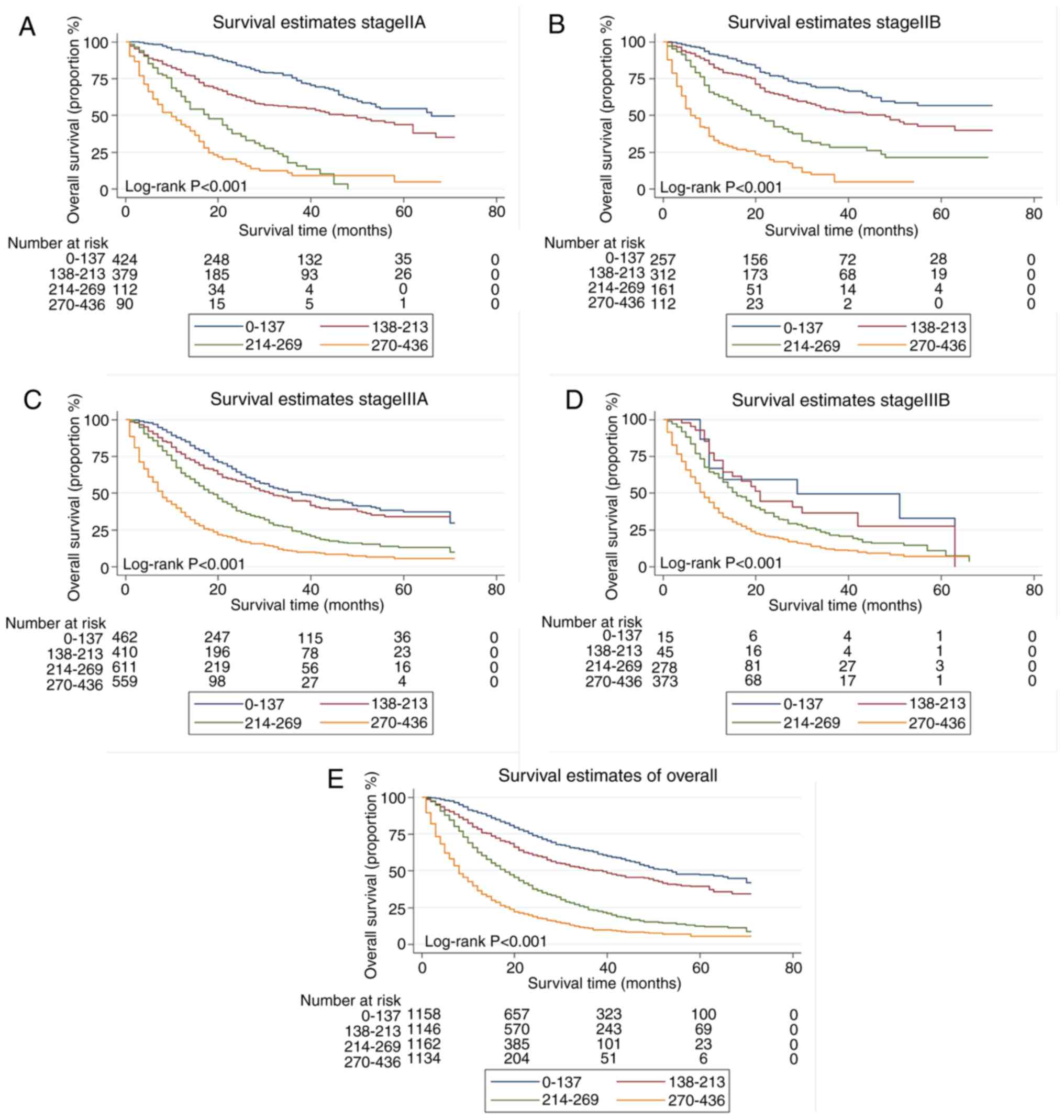
Risk stratification
The total score for each patient in the training set
was calculated, and the scores divided into quartiles (0–137,
138–213, 214–269 and 270–436) to represent different outcomes. A
statistically significant difference in survival was identified
among patients with stage IIA, IIB, IIIA and IIIB NSCLC when the
quartiles of scores were applied to divide the patients in the
validation set (all P<0.001; Fig.
4).
Discussion
To the best of our knowledge, this is the first
large-scale clinical retrospective study that used the SEER
database to construct a nomogram to predict survival rates for
patients with stage II and III NSCLC. In this study, a total of
15,344 patients were included following rigorous screening, and 12
risk factors that significantly affected prognosis were determined
by the Cox regression method. A nomogram was constructed based on
these 12 risk factors. The C-index and the graphical calibration
method were used for internal validation, which suggested that the
nomogram exhibited a good predictive ability. The nomogram
demonstrated that the survival of patients with NSCLC was affected
by multiple factors, especially the treatment strategy. The
nomogram also accurately predicted the prognosis of different risk
groups, including patients with stage IIA, IIB, IIIA and IIIB
NSCLC. Compared with traditional TNM staging, the model established
in the present study combined more clinical information to
determine the prognosis of patients more accurately and guide the
treatment strategy.
Demographic factors of the patients in the present
study, such as age, sex and race, had a moderate influence on
prognosis, and marital status only had a minor effect. In elderly
patients with NSCLC, the aging of organs coupled with a decrease in
immune function leads to a high possibility of tumor recurrence.
Elderly patients with NSCLC exhibit low tolerance to surgery,
radiotherapy and chemotherapy, and therefore, their compliance to
anticancer treatment may be poor. Additionally, elderly patients
may often suffer from other conditions, and thus their survival
rate is reduced (16). Through
follow-up of 14,578 postoperative patients with NSCLC between
January 2009 and January 2014 in multiple centers, Dziedzic et
al (17) demonstrated that the
risk of tumor recurrence and metastasis increased with age. In a
retrospective study involving 33,919 patients with lung cancer from
Taiwan, China, Wang et al (18) reported that age >65 years was an
independent risk factor for prognosis. Thus, age is associated with
the prognosis of patients with lung cancer.
A recent large-scale epidemiological survey revealed
that the incidence and mortality rates of female patients with lung
cancer are increasing (1). Chang
et al (19) retrospectively
analyzed 2,770 patients with stage I and II NSCLC and demonstrated
that the 5-year survival rate of female patients with lung ADC was
higher compared with that of male patients, whereas no significant
differences were observed in the 5-year survival rate of patients
with non-adenocarcinoma. However, another study has reported the
opposite result, i.e. that sex is not a risk factor for patients
with NSCLC (17). Although the
mechanism by which sex affects the prognosis of patients with lung
cancer requires further study, male and female patients exhibit
distinctive clinical and biological characteristics, such as the
likelihood of ADC. In addition, mutations in the epidermal growth
factor receptor gene are often identified in female patients
(17). Results for non-smoking
patients with lung ADC also indicated that female patients may more
likely benefit from targeted therapy compared with male patients
(20).
In terms of marital status, Merrill et al
(21) used a sample of 779,978 male
and 1,032,868 female patients from the SEER database and reached
the opposite conclusion from that of the present study; marriage
was beneficial for only non-fatal cancers such as breast,
colorectal and kidney cancer, but did not improve the 5-year
survival rate for patients with lung or liver cancer. However,
another study that used the SEER database reported that among
patients with NSCLC, married individuals exhibited higher overall
and tumor-specific survival rates compared with unmarried
individuals (22). A multicenter
trial (23) has demonstrated that
married patients with cancer experience less psychological distress
and receive better social support compared with unmarried patients,
which may explain why marriage improved the prognosis of patients
with lung cancer. Race is also strongly associated with the
prognosis of lung cancer, although this association remains
controversial. An epidemiological survey of 38 states in the United
States that included 80% of the population revealed that
African-American patients exhibited lower survival rates compared
with Caucasian patients (24).
Another retrospective analysis, spanning 10 years in the United
States, suggested that racial differences in lung cancer mortality
were due to differences in access to health care and provision of
the recommended treatment (25). In
a retrospective study from Florida, the authors noted that Asian
patients had higher survival rates compared with Caucasian and
African-American patients following adjustment for certain
confounding factors, such as economic status (26). In addition, the results of the
present study suggested that other populations, including Asians,
exhibited the best prognosis.
In the present study, the results of the traditional
TNM staging of lung cancer were the same as those of NSCLC.
Prognosis became progressively worse with increasing T/N stages,
and the histopathological type and degree of tumor differentiation
also determined the prognosis of patients with lung cancer.
Regarding differentiation, poorly differentiated tumors have a
stronger ability to invade and metastasize and are highly
malignant; the results of the present study also demonstrated that
a low degree of tumor differentiation in patients with NSCLC was
associated with a low survival rate. There are different views
regarding the ability of TNM stage to reflect accurately the
prognosis of patients. For example, three retrospective studies
from Asia and Europe suggested that patients with different AJCC
stages had no statistical difference in prognosis, therefore it was
not advisable to rely solely on AJCC stages to determine prognosis,
as there are numerous remaining factors affecting the survival of
patients with NSCLC (27–29). A previous study confirmed that gene
mutation is one of the possible reasons for the difference in
prognosis between lung SCC and ADC (30). However, in further studies on NSCLC,
more attention should be paid to the pathological types and
differentiation degree. For example, the AJCC has advocated that
researchers focus on the influence of different pathological types
on prognosis in esophageal cancer (31).
For patients with NSCLC, appropriate treatment such
as surgery or drug therapy should be selected based on the clinical
situation of the patients, in order to obtain the optimal
prognosis.. In theory, cancer can be cured if drugs that completely
eradicate cancer cells were discovered; currently, the ability of
drugs to cure cancer is limited to several types of malignant
tumors. For the majority of malignant tumors, finding a cure is
more likely in the early stages of disease, when the tumor has not
spread and can be surgically removed. The present study
demonstrated that patients with >4 groups lymph node metastasis,
lobectomy in combination with lymph node dissection was associated
with the best prognosis. Speicher et al (32) have reported that surgical lobectomy
significantly prolonged long-term survival in a follow-up study of
39,403 patients with lung cancer. A meta-analysis by Zhang et
al (33) also revealed that
lobectomy resulted in better prognosis compared with segmental lung
resection in patients with stage I NSCLC, and that age and tumor
size should not be considered limiting factors for lobectomy. In
addition, the latest National Comprehensive Cancer Network
guidelines recommend lobectomy as the first-choice treatment for
patients with stage II and III NSCLC with good lung reserve
function that can tolerate surgery (34). For NSCLC, lymph node metastasis,
especially mediastinal lymph node metastasis, is an independent
risk factor for poor prognosis (35). Lymph node dissection has also been
demonstrated to significantly improve prognosis (36). In 1996, the International Association
for the Study of Lung Cancer presented the concept of systematic
lymph node dissection (SLD), with lobectomy combined with SLD
identified as the standard surgical method for NSCLC (37). In 2006, the guidelines of the
European Society of Thoracic Surgeons defined the scope of SLD as
the resection of at least six groups of lymph nodes, including
>3 ipsilateral mediastinal and subcarinal lymph nodes. The
complete dissection of mediastinal lymph nodes and surrounding
adipose tissue is required (38).
According to the standards of the Japan Lung Cancer Society, Adachi
et al (39) defined lymph
node dissection as: i) The removal of at ≥3 hilar and
intrapulmonary lymph nodes; ii) the resection of ≥3 mediastinal
lymph nodes; or iii) the removal of ≥6 lymph nodes. Similarly, the
results of the present study demonstrated that the dissection of ≥4
groups of lymph nodes significantly improved patient survival.
With the emergence of targeted therapy and
immunotherapy, the survival advantage of patients receiving
conventional platinum-based adjuvant chemotherapy as the standard
treatment is moderate, especially for patients with stage II or III
NSCLC (40). However, a large
retrospective study has also reported that postoperative adjuvant
chemotherapy is essential for improving the prognosis of patients
(41). Radiotherapy is also a
standard treatment for NSCLC. A large-scale retrospective analysis
using the SEER database concluded that preoperative radiotherapy
can significantly improve the survival rate of patients with
IIIA/N2 NSCLC (42). However,
radiotherapy results in numerous side effects, such as skin ulcers
or severe reactions including radiological pneumonia (43). Increasing the dose of radiation
appears to improve the prognosis of patients who only receive
radiation therapy, but decrease survival in patients who receive a
combination of radiotherapy and chemotherapy (44). Therefore, the selection of anticancer
treatment strategy for patients should be combined with their
clinicopathological data.
The present study had several limitations. First,
due to the limited information available in the SEER database,
smoking history, radiotherapy dose, specific chemotherapy regimen,
surgical methods (open or endoscopic surgery) and additional
clinical information could not be obtained, which may have affected
the results. Second, the T/N staging was based on the 7th edition
of the AJCC staging system. Although the 7th edition TN stage and
tumor size were available, the tumor invasion degree information
was not included, and thus the AJCC staging results could not be
converted to the 8th edition. For example, a 600 mm T3 lung cancer
record from the SEER database should be classified as T4 according
to the 8th edition of AJCC staging if it extends to the diaphragm.
Finally, the patients with NSCLC in the SEER database were all from
the United States, and although patients of different races were
included, the cohort may not be representative of patients
worldwide.
In conclusion, a nomogram combining substantial
demographic, pathological and treatment data to predict OS for
patients with stage II and III NSCLC was established and validated
using a population-based study from the SEER database.
Well-designed trials are needed to improve this nomogram.
Acknowledgments
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
YL and XW conceived of and designed the study,
acquired and analyzed the data and wrote the manuscript. PZ, GY, XF
and CH revised the manuscript and analyzed the data. All authors
read and approved the manuscript and agree to be accountable for
all aspects of the research in ensuring that the accuracy or
integrity of any part of the work are appropriately investigated
and resolved.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Liu S, Chen Q, Guo L, Cao X, Sun X, Chen W
and He J: Incidence and mortality of lung cancer in China,
2008–2012. Chin J Cancer Res. 30:580–587. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Barlesi F, Mazieres J, Merlio JP,
Debieuvre D, Mosser J, Lena H, Ouafik L, Besse B, Rouquette I,
Westeel V, et al: Routine molecular profiling of patients with
advanced non-small-cell lung cancer: Results of a 1-year nationwide
programme of the French cooperative thoracic intergroup (IFCT).
Lancet. 387:1415–1426. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
National Lung Screening Trial Research
Team, ; Church TR, Black WC, Aberle DR, Berg CD, Clingan KL, Duan
F, Fagerstrom RM, Gareen IF, Gierada DS, et al: Results of initial
low-dose computed tomographic screening for lung cancer. N Engl J
Med. 368:1980–1991. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gorenstein LA and Sonett JR: The surgical
management of stage I and stage II lung cancer. Surg Oncol Clin N
Am. 20:701–720. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Filosso PL, Rena O, Donati G, Casadio C,
Ruffini E, Papalia E, Oliaro A and Maggi G: Bronchial carcinoid
tumors: Surgical management and long-term outcome. J Thorac
Cardiovasc Surg. 123:303–309. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Li Q, Xiao W, Xie T, He J, Han Y and Zhu
J: Surgical treatment for lung cancer in the elderly. Zhongguo Fei
Ai Za Zhi. 10:34–36. 2007.(In Chinese). PubMed/NCBI
|
|
8
|
König IR, Fuchs O, Hansen G, von Mutius E
and Kopp MV: What is precision medicine? Eur Respir J.
50:17003912017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Rami-Porta R, Bolejack V, Crowley J, Ball
D, Kim J, Lyons G, Rice T, Suzuki K, Thomas CF Jr, Travis WD, et
al: The IASLC lung cancer staging project: Proposals for the
revisions of the T descriptors in the forthcoming eighth edition of
the TNM classification for lung cancer. J Thorac Oncol.
10:990–1003. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Balachandran VP, Gonen M, Smith JJ and
DeMatteo RP: Nomograms in oncology: More than meets the eye. Lancet
Oncol. 16:e173–e180. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yang H, Li X, Shi J, Fu H, Yang H, Liang
Z, Xiong H and Wang H: A nomogram to predict prognosis in patients
undergoing sublobar resection for stage IA non-small-cell lung
cancer. Cancer Manag Res. 10:6611–6626. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zhou H, Zhang Y, Qiu Z, Chen G, Hong S,
Chen X, Zhang Z, Huang Y and Zhang L: Nomogram to predict
cause-specific mortality in patients with surgically resected stage
I non-small-cell lung cancer: A competing risk analysis. Clin Lung
Cancer. 19:e195–e203. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Deng J, Ren Z, Wen J, Wang B, Hou X, Xue Z
and Chu X: Construction of a nomogram predicting the overall
survival of patients with distantly metastatic non-small-cell lung
cancer. Cancer Manag Res. 10:6143–6156. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Frank E and Harrel J; (homepage on the
Internet), : Rms: Regression Modeling Strategies. R Package Version
3.4–0. http://CRAN.Rproject.org/packagermsFebruary
19–2019
|
|
15
|
Heagerty PJ and Zheng Y: Survival model
predictive accuracy and ROC curves. Biometrics. 61:92–105. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Socinski MA, Evans T, Gettinger S, Hensing
TA, VanDam Sequist L, Ireland B and Stinchcombe TE: Treatment of
stage IV non-small cell lung cancer: Diagnosis and management of
lung cancer, 3rd ed: American College of Chest Physicians
evidence-based clinical practice guidelines. Chest. 143 (5
Suppl):e341S–e368S. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dziedzic DA, Rudzinski P, Langfort R and
Orlowski T; Polish Lung Cancer Study Group (PLCSG), : Risk factors
for local and distant recurrence after surgical treatment in
patients with non-small-cell lung cancer. Clin Lung Cancer.
17:e157–e167. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wang BY, Huang JY, Cheng CY, Lin CH, Ko J
and Liaw YP: Lung cancer and prognosis in Taiwan: A
population-based cancer registry. J Thorac Oncol. 8:1128–1135.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chang JW, Asamura H, Kawachi R and
Watanabe S: Gender difference in survival of resected non-small
cell lung cancer: Histology-related phenomenon? J Thorac Cardiovasc
Surg. 137:807–812. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Rosell R, Moran T, Queralt C, Porta R,
Cardenal F, Camps C, Majem M, Lopez-Vivanco G, Isla D and Provencio
M: Screening for epidermal growth factor receptor mutations in lung
cancer. N Engl J Med. 361:958–967. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Merrill RM and Johnson E: Benefits of
marriage on relative and conditional relative cancer survival
differ between males and females in the USA. J Cancer Surviv.
11:578–589. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wu Y, Ai Z and Xu G: Marital status and
survival in patients with non-small cell lung cancer: An analysis
of 70006 patients in the SEER database. Oncotarget.
8:103518–103534. 2017.PubMed/NCBI
|
|
23
|
Varlotto JM, Voland R, McKie K, Flickinger
JC, DeCamp MM, Maddox D, Rava P, Fitzgerald TJ, Graeber G, Rassaei
N, et al: Population-based differences in the outcome and
presentation of lung cancer patients based upon racial, histologic,
and economic factors in all lung patients and those with metastatic
disease. Cancer Med. 7:1211–1220. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Richards TB, Henley SJ, Puckett MC, Weir
HK, Huang B, Tucker TC and Allemani C: Lung cancer survival in the
United States by race and stage (2001–2009): Findings from the
CONCORD-2 study. Cancer. 123 (Suppl 24):S5079–S5099. 2017.
View Article : Google Scholar
|
|
25
|
Williams CD, Salama JK, Moghanaki D, Karas
TZ and Kelley MJ: Impact of race on treatment and survival among
U.S. veterans with early-stage lung cancer. J Thorac Oncol.
11:1672–1681. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Tannenbaum SL, Koru-Sengul T, Zhao W, Miao
F and Byrne MM: Survival disparities in non-small cell lung cancer
by race, ethnicity, and socioeconomic status. Cancer J. 20:237–245.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Asamura H, Goya T, Koshiishi Y, Sohara Y,
Eguchi K, Mori M, Nakanishi Y, Tsuchiya R, Shimokata K, Inoue H, et
al: A Japanese lung cancer registry study: Prognosis of 13,010
resected lung cancers. J Thorac Oncol. 3:46–52. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Cho BC, DE Pas T, Kalofonos H, Wang Q,
Ramlau R, Cheng Y, Vitiello F, Laisaar T, Vallières E, Kubisa B, et
al: Prognostic factors in early-stage NSCLC: Analysis of the
placebo group in the MAGRIT study. Anticancer Res. 39:1403–1409.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Li H, Sun Z, Yang F, Sui X, Liu T and Wang
J: Primary tumour resection in non-small-cell lung cancer patients
with ipsilateral pleural dissemination (M1a): A population-based
study. Eur J Cardiothorac Surg. 55:1121–1129. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Meng F, Zhang L, Ren Y and Ma Q: The
genomic alterations of lung adenocarcinoma and lung squamous cell
carcinoma can explain the differences of their overall survival
rates. J Cell Physiol. 234:10918–10925. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Rice TW, Gress DM, Patil DT, Hofstetter
WL, Kelsen DP and Blackstone EH: Cancer of the esophagus and
esophagogastric junction-major changes in the American joint
committee on cancer eighth edition cancer staging manual. CA Cancer
J Clin. 67:304–317. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Speicher PJ, Gu L, Gulack BC, Wang X,
D'Amico TA, Hartwig MG and Berry MF: Sublobar resection for
clinical stage IA non-small-cell lung cancer in the United States.
Clin Lung Cancer. 17:47–55. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Zhang Y, Sun Y, Wang R, Ye T, Zhang Y and
Chen H: Meta-analysis of lobectomy, segmentectomy, and wedge
resection for stage I non-small cell lung cancer. J Surg Oncol.
111:334–340. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
NCCN Guidelines Insights (homepage on the
Internet), . Non-Small Cell Lung Cancer, Version 3. 2019,
https://.nccn.org/patientsFebruary
19–2019
|
|
35
|
Rami-Porta R, Asamura H, Travis WD and
Rusch VW: Lung cancer-major changes in the American joint committee
on cancer eighth edition cancer staging manual. CA Cancer J Clin.
67:138–155. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Hughes MJ, Chowdhry MF, Woolley SM and
Walker WS: In patients undergoing lung resection for non-small cell
lung cancer, is lymph node dissection or sampling superior?
Interact Cardiovasc Thorac Surg. 13:311–315. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Sugi K, Nawata K, Fujita N, Ueda K, Tanaka
T, Matsuoka T, Kaneda Y and Esato K: Systematic lymph node
dissection for clinically diagnosed peripheral non-small-cell lung
cancer less than 2 cm in diameter. World J Surg. 22:290–295. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Lardinois D, De Leyn P, Van Schil P, Porta
RR, Waller D, Passlick B, Zielinski M, Lerut T and Weder W: ESTS
guidelines for intraoperative lymph node staging in non-small cell
lung cancer. Eur J Cardiothorac Surg. 30:787–792. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Adachi H, Sakamaki K, Nishii T, Yamamoto
T, Nagashima T, Ishikawa Y, Ando K, Yamanaka K, Watanabe K,
Kumakiri Y, et al: Lobe-specific lymph node dissection as a
standard procedure in surgery for non-small cell lung cancer: A
propensity score matching study. J Thorac Oncol. 12:85–93. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Nagasaka M and Gadgeel SM: Role of
chemotherapy and targeted therapy in early-stage non-small cell
lung cancer. Expert Rev Anticancer Ther. 18:63–70. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Salazar MC, Rosen JE, Wang Z, Arnold BN,
Thomas DC, Herbst RS, Kim AW, Detterbeck FC, Blasberg JD and Boffa
DJ: Association of delayed adjuvant chemotherapy with survival
after lung cancer surgery. JAMA Oncol. 3:610–619. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Chen D, Wang H, Song X, Yue J and Yu J:
Preoperative radiation may improve the outcomes of resectable
IIIA/N2 non-small-cell lung cancer patients: A propensity score
matching-based analysis from surveillance, epidemiology, and end
results database. Cancer Med. 7:4354–4360. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Benveniste MF, Gomez D, Carter BW,
Betancourt Cuellar SL, Shroff GS, Benveniste APA, Odisio EG and
Marom EM: Recognizing radiation therapy-related complications in
the chest. Radiographics. 39:344–366. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Bradley J and Hu C: Learning from trials
on radiation dose in non-small cell lung cancer. Int J Radiat Oncol
Biol Phys. 96:748–750. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Edge SB, Byrd DR, Compton CC, Fritz AG,
Greene FL and Trotti A: AJCC Cancer Staging Manual7th edition.
Springer; New York, NY: 2009
|