Introduction
Radiation therapy is a less invasive treatment for
brain and neck diseases, such as head and neck cancers and
arteriovenous malformations (1–4).
Although some studies reported the efficacy of stereotactic
radiation therapy for either newly diagnosed glioma or recurrent
glioma, especially for lesions that are unamenable to resection,
such as lesions of eloquent areas of the brain, strong
recommendation of stereotactic radiation therapy for glioma has not
yet been established (5–7). Necrosis, cavernous malformation, and
radiation-induced tumor formation are major side effects observed
in the latter stages of radiation therapy; these side effects
sometimes distress the patients (8–10).
Mostly, radiation necrosis occurs about 3–36 months after radiation
therapy (11–13), and radiation-induced cavernous
malformation (RICM) caused by radiation injury is reported to occur
after a rather longer period of 1–26 years after radiation therapy
(9–11). Due to the long latency period of RICM
after radiation therapy, RICMs occurring in glioma patients have
been scarcely reported (9,10,14).
Here, we present three cases of long surviving
glioma patients with symptomatic hemorrhage from RICM, resulting
from radiation necrosis that occurred more than 4 years after the
last irradiation episode. The lesions were pathologically proven in
2 cases and clinically suggested by magnetic resonance imaging
(MRI) in 1 case. Thus, it is important to consider late
complications of radiation therapy when administered to low grade
glioma patients, since they could potentially survive for a long
period.
Case report
Case 1
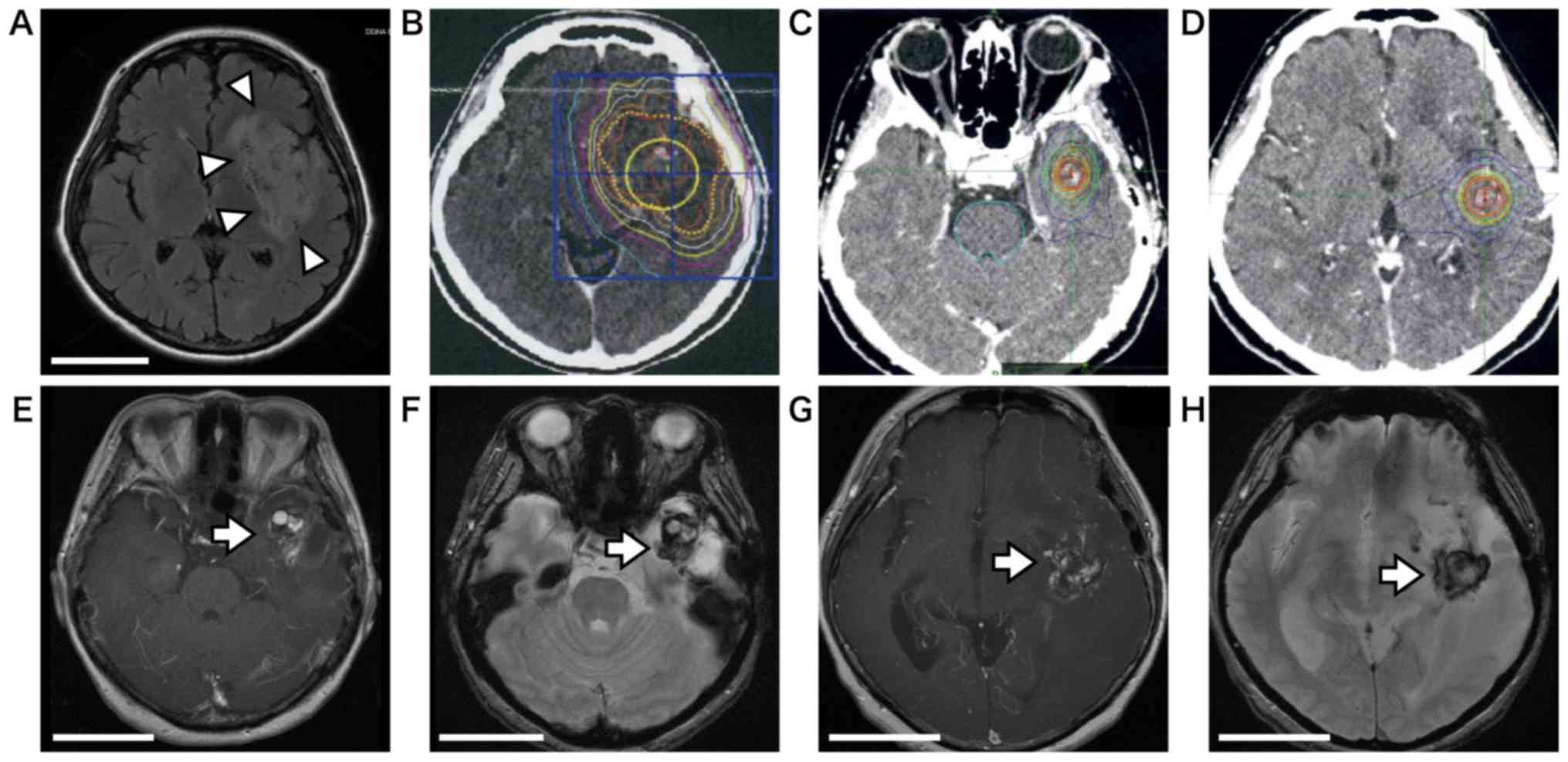
At age 50 years, the female patient had a left
insular tumor, which invaded the frontal and temporal lobes
(Fig. 1A). The histopathological
diagnosis of the biopsy specimen was oligoastrocytoma. Using a
CyberKnife, the patient was initially administered 35 Gy/5 fr
(Fig. 1B). At age 55 years, each
lesion appeared in the temporal and insular cortex on
contrast-enhanced MRI; the patient was re-treated with additional
30 Gy/3 fr (Fig. 1C and D), followed
by temozolomide and interferon β chemotherapy for 4 years.
At age 59 years, she presented with gradual
development of speech disturbance and was referred to our hospital.
An MRI scan revealed an enlargement of the temporal mass with
heterogeneous enhancement on contrast-enhanced T1 weighted image
(T1-CE) (Fig. 1E) and low intensity
rim on T2* with strong perifocal edema (Fig. 1F). The lesion (lesion 1) was totally
resected; histopathological examination of the lesion revealed
cavernous malformation and radiation necrosis without tumor
recurrence. The patient was closely observed without further
chemotherapy.
Two years later, another MRI scan revealed a
gradually increasing enhanced insular mass with minor hemorrhage
and perifocal edema (Fig. 1G and H).
RICM with radiation necrosis was suspected because of similarities
in MRI findings to the previous ones. Since aphasia and right
hemiparesis gradually worsened even after corticosteroid treatment,
the lesion (lesion 2) was partially removed and the
histopathological diagnosis was again radiation necrosis without
tumor recurrence. A ventriculoperitoneal shunt was placed for
concurrent communicating hydrocephalus. Perifocal edema gradually
decreased; she could now perform daily activities at home without
much support.
Case 2
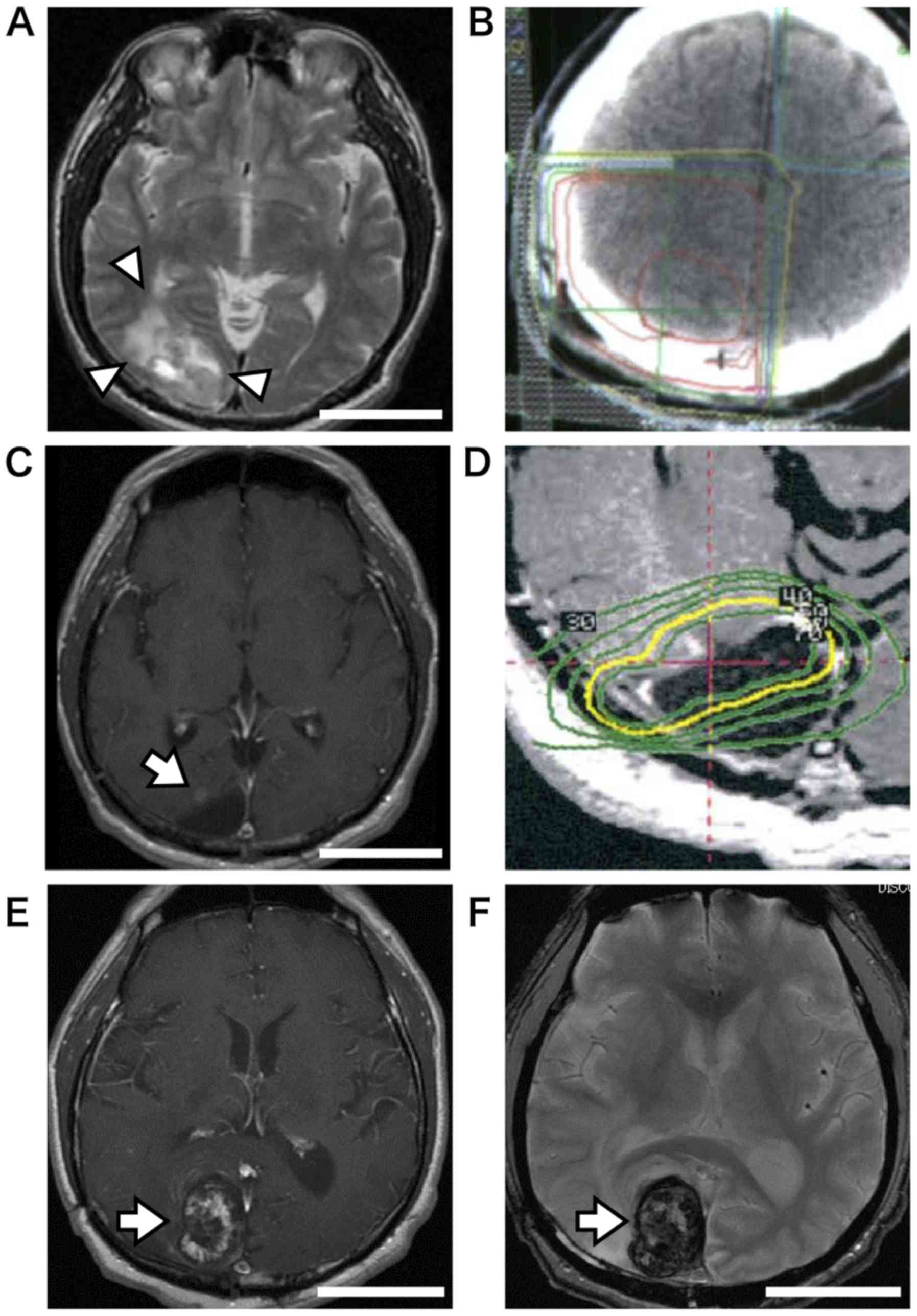
At age 52 years, this male patient had a right
occipital tumor (Fig. 2A). After
total resection of the tumor, a histopathological examination
revealed an anaplastic ependymoma. The patient was treated with 60
Gy of postoperative external irradiation (Fig. 2B). One year later, a small enhanced
nodule on the tumor resection surface was noticed on MRI (Fig. 2C) and 20 Gy of γ-knife radiation was
administered (Fig. 2D). Without
additional treatment in 12 years, no enhanced lesion was
observed.
At age 67 years, the patient presented with
intermittent visual hallucinations in the left visual field. An MRI
scan revealed a heterogeneous enhanced mass lesion (Fig. 2E) that enlarged gradually. The lesion
was comprised of hemorrhages that consisted of low signals on T2*
on MRI images (Fig. 2F). After total
resection of the lesion (lesion 3), a histopathological examination
revealed radiation necrosis with cavernous malformation-like areas.
The postoperative course was uneventful and visual hallucination
completely disappeared.
Case 3
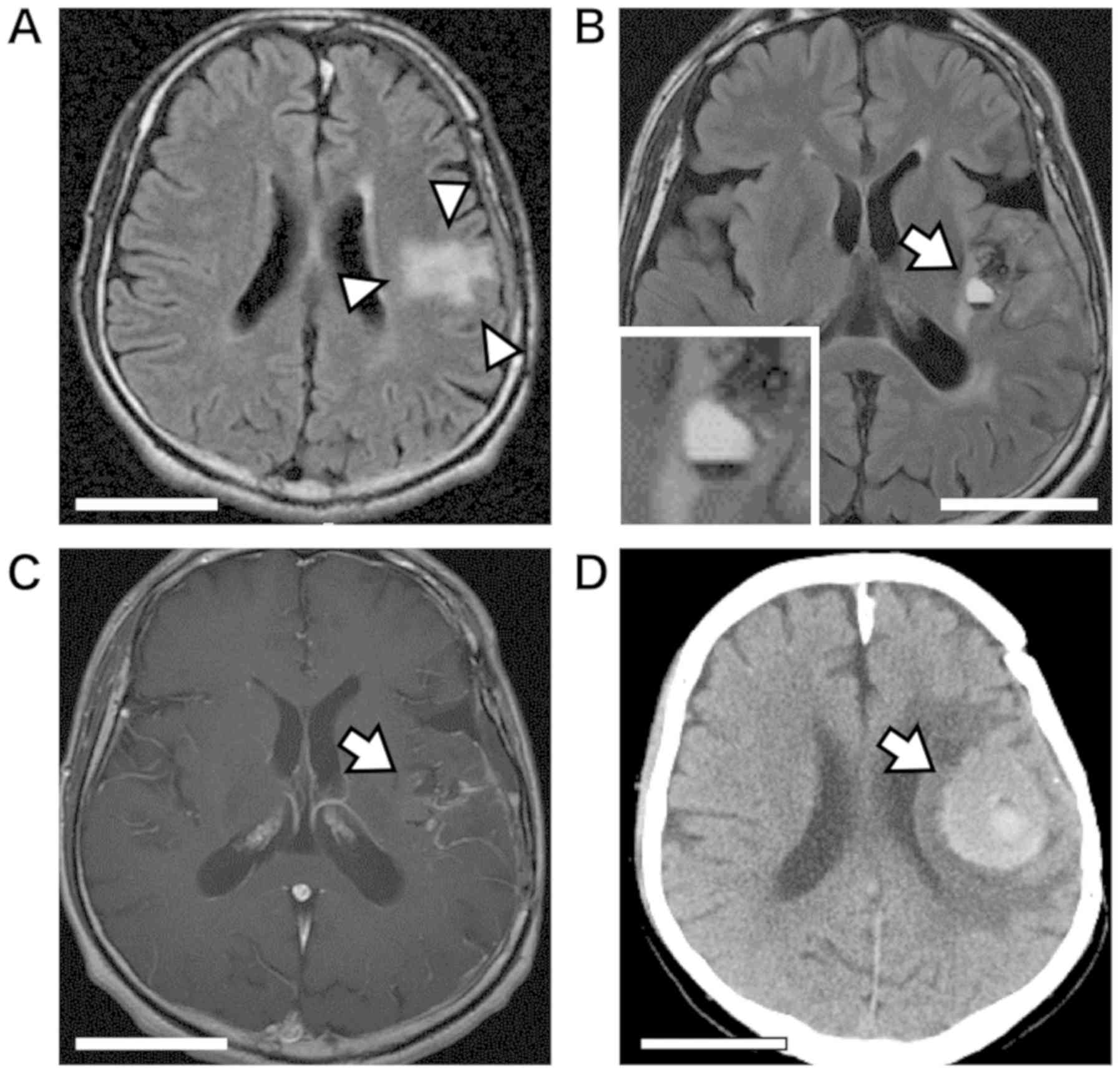
At age 39 years, this male patient was diagnosed of
left insular anaplastic astrocytoma with an oligodendroglial
component by open biopsy in the previous hospital. The patient was
treated with intraoperative irradiation (dose unknown) and 56 Gy of
conventional external irradiation, followed by administration of
four doses of nimustine hydrochloride. After finishing the initial
treatment, the patient was referred to our hospital. An MRI scan
revealed a T2 high lesion with no obvious enhancement after more
than 10 years (Fig. 3A).
At age 50 years, another MRI scan revealed a cystic
lesion (lesion 4) with mild enhancement in the insula (Fig. 3B and C). A biopsy was performed in
suspicion of tumor recurrence, but a histopathological examination
revealed only gliosis with no tumor recurrence. The patient did not
receive further treatment but was assessed with MRI during
follow-up. Two years later, the patient suffered a sudden onset of
severe right hemiparesis and motor aphasia. Computed tomography
(CT) scans revealed subcortical hemorrhage right on the primary
motor cortex, adjacent to the tumor location (Fig. 3D). Two years later, the right
hemiparesis suddenly worsened again; a CT scan revealed a
hemorrhage recurrence in almost the same area of the previous
hemorrhage. Although hematoma was stereotactically aspirated, the
patient experienced severe right hemiparesis and mild aphasia.
Histological findings. Histopathological examination
was performed on each surgically resected or biopsied specimen
fixed with 10% formalin for 24 h at room temperature.
Paraffin-embedded sections cut by 4 µm thickness were performed
hematoxylin and eosin (H&E) and following immunohistological
staining. For immunohistological examination, after
deparaffinization, antigen activation was performed at 95°C for 40
min at pH 9.0 using TE buffer. The commercially available primary
antibodies, CD31 (monoclonal mouse; Dako, Agilent Technologies
Inc.; clone: JC70A, code no. M0823; dilution, 1:30) and VEGF
(vascular endothelial growth factor) (polyclonal rabbit; GeneTex
Inc.; GTX102643 dilution, 1:100), were used at room temperature for
30 min. Subsequently, ChemMate Envision kit/HRP (Dako, Agilent
Technologies Inc.) for CD31 immunostaining and Histofine Simple
Stain MAX-PO (Multi) (Nichirei Bioscience Inc.) for VEGF
immunostaining were used as the secondary antibody at room
temperature for 30 min. Finally, sections were reacted with
3,3-Diaminobenzidine (DAB) as a chromogen at room temperature.
Slides were observed under a light microscope.
Radiation necrosis was histologically diagnosed in
all cases, except in case 3 which was diagnosed as gliosis.
Microscopically, coagulative necrosis, hyalinized blood vessels,
and telangiectasia, which is suggestive of radiation vasculopathy,
were observed in most of the cases (Fig.
4A). Tumor recurrence was not observed in all cases. In the
totally resected lesions (lesions 1 and 3), the core of radiation
necrosis consisted of RICM, which is a cavernous hemangioma-like
component with thin-walled vessels (Fig.
4B and C: lesion 1, Fig. 4D and
E: lesion 3). There were hemorrhages that permeated surrounding
stroma of cavernous hemangioma-like lesions (Fig. 4F). A reactive increase in astrocyte
number was observed in the perinecrotic or stromal hemorrhage area
(Fig. 4G). Immunoreactivity for
vascular endothelial growth factors (VEGF) was observed in the
cytoplasm of the astrocytes in the perinecrotic hemorrhage area
(Fig. 4H and I).
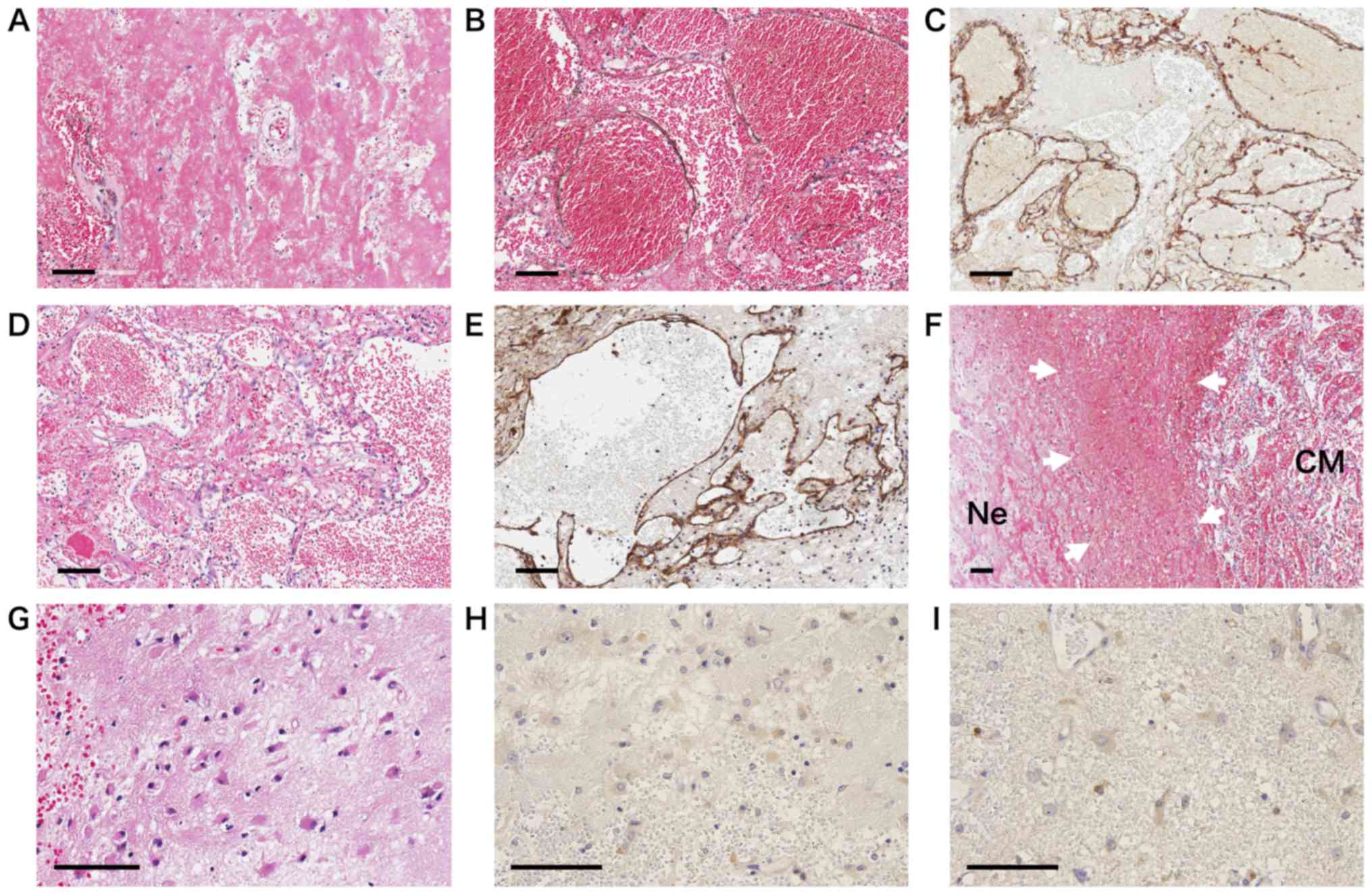 | Figure 4.H&E staining and
immunohistochemistry of the surgical specimen. Bar=100 μm. (A)
Typical necrosis and hyalin exudation of the necrotic core of
lesion 1 (H&E, magnification, ×200). (B-E) Cavernous
malformation-like areas consist of thin and vulnerable vessels with
telangiectasia and permeating hemorrhage of lesion 1 (H&E, B
and CD31, C) and lesion 3 (H&E, D and CD31, E) (magnification,
×200). (F) Permeative hemorrhage areas (white arrows) are seen
between the cavernous hemangioma-like lesion (CM) and necrotic area
(Ne) of lesion 1 (H&E magnification, ×100). (G) Peri-permeating
hemorrhage areas in which large astrocytes are mixed with
microhemorrhage (VEGF magnification, ×400). (H and I) Astrocytes
are immunoreactive to VEGF. This immunoreactivity for VEGF is
observed in peri-lesional interstitial hemorrhage areas of lesion 1
(magnification, ×400). |
Discussion
Radiation necrosis is one of the major side effects
of radiation therapy that usually occurs several months to years
after radiation. The total incidence of radiation necrosis is
estimated at 3–24% (1,15). The important risk factors of
radiation necrosis are irradiation doses to brain tissue greater
than 60 Gy, a fraction size greater than 1.8–2.0 Gy, and subsequent
administration of chemotherapy (1,8,12,16). On
the other hand, in most reported cases, RICM is observed at a
frequency of about 6.7–41.2% in children with brain tumors long
after radiation therapy (8–10). RICMs were observed in the cases with
fractionated radiation therapy with doses greater than 20 Gy or 30
Gy (9,10,17). The
higher the dosage, the shorter the latency (9). However, RICM in adult patients with
glioma has been scarcely reported (9,14).
The clinical characteristics of the patients are
summarized in Table I. The
histological diagnosis was oligoastrocytoma in 2 cases and
anaplastic ependymoma in 1 case. The age at diagnosis ranged
between 39 and 52 years (average, 47 years). The interval between
the last irradiation and the occurrence of symptoms was 45–173
months (average, 107 months). Annual incidence of hemorrhage from
RICM is reported to be about 4%; approximately 40% of RICM patients
are estimated to suffer from symptomatic hemorrhages (14,18). The
clinical courses and imaging findings of the presented cases of
RICM with delayed radiation necrosis have the following
characteristics. The ability of patients to perform daily
activities deteriorated because of acute or chronic hemorrhages.
Three lesions showed chronic enlargement of hematoma with
uncontrollable perifocal edema. Although most radiation necrosis
are responsive to steroid administration (2,12,13), the
perifocal edema of RICMs in the presented cases of radiation
necrosis was steroid resistant and needed surgical interventions
(case 1 and 3). Total resection of cavernous malformation,
including necrotic tissues, appeared to be effective for improving
neurological symptoms, such as seizure control.
 | Table I.Summary of clinical characteristics of
cases. |
Table I.
Summary of clinical characteristics of
cases.
| Characteristics | Case 1 | Case 2 | Case 3 |
|---|
| Lesion | Lesion 1 and 2 | Lesion 3 | Lesion 4 |
| Age at diagnosis | 50 | 52 | 39 |
| Sex | Female | Male | Male |
| Histology | Oligoastrocytoma | Anaplastic
ependymoma | Oligoastrocytoma |
| Location | Left temporal and
insular | Right occipital | Left frontal |
| First
irradiation | CyberKnife (35
Gy) | Conventional RT (60
Gy) | Intraoperative RT +
Conventional RT (56 Gy) |
| Additional
irradiation | CyberKnife (30
Gy) | γ-Knife (20 Gy) | – |
| Last
irradiation~symptom onset (month) | 45 and 69 | 173 | 142 |
| Clinical
presentation | Chronic | Chronic | Acute |
| Worsening of epilepsy
control | Yes | Yes | No |
| Outcome | MD | GR | SD |
It is important for appropriate treatments to
distinguish tumor recurrence from RICM with radiation necrosis. The
MRI study of delayed radiation necrosis with RICM showed chronic
enlargement of heterogeneously enhanced lesions with perifocal
edema and repeated hemorrhages with low intensity rim on T2*
(8). The presence of hypointense rim
T2*, which resembles the appearance of ‘sporadic’
(non-radiation-induced) cavernous malformations, could be helpful
in differentiating RICM with delayed radiation necrosis from tumor
recurrence. In fact, no tumor recurrence was found in any of the
surgically-obtained specimens in this study.
Radiation-induced endothelial and glial damage may
lead to microvasculopathy and telangiectasia, resulting in vascular
insufficiency and infarction. This eventually culminates in gray
and/or white matter necrosis (1–3). This
hypoxia causes the upregulation of VEGF via the activation of
hypoxia inducible factor-1α. The expression of VEGF produces leaky
and fragile angiogenesis and subsequent perilesional edema in
radiation necrosis (1).
Immunoreactivity for VEGF is observed in the cytoplasm of
astrocytes in the perinecrotic area. Upregulated production of VEGF
may promote angiogenesis of vulnerable vessels, which then causes
chronic or acute hemorrhages and strong perilesional edema.
Stereotactic radiotherapy could be an option for the
treatment of unresectable gliomas, even as an initial treatment
(5–7,19).
However, cases 1 and 2 received obvious overdose of radiation by an
additional stereotactic radiotherapy and presented with repeated
hemorrhages, medically uncontrollable symptomatic epilepsy, and
cerebral edema. Although tumor did not recur, presented cases
experienced disorders that affected their abilities to perform
daily activities. Therefore, overdose radiation should be avoided
in low grade glioma patients, who could potentially survive for a
long period.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in the published article.
Author's contributions
TO analyzed and interpreted data, and significantly
contributed to the writing of the manuscript. TY, SK, TS, HN
treated and operated on patients. SB performed the histological
examination and diagnosis of the brain lesions. All authors were
involved in the writing of the manuscript from the draft stage. All
authors have read and approved the final revision.
Ethics approval and consent to
participate
Each patient involved in this study provided written
informed consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
RICM
|
radiation-induced cavernous
malformation
|
|
FLAIR
|
fluid attenuated inversion
recovery
|
|
MRI
|
magnetic resonance imaging
|
|
CT
|
computed tomography
|
|
VEGF
|
vascular endothelial growth factor
|
|
HIF-1α
|
hypoxia inducible factor-1α
|
References
|
1
|
Miyatake S, Nonoguchi N, Furuse M,
Yoritsune E, Miyata T, Kawabata S and Kuroiwa T: Pathophysiology,
diagnosis, and treatment of radiation necrosis in the brain. Neurol
Med Chir (Tokyo). 55:50–59. 2015. View Article : Google Scholar
|
|
2
|
Cheng KM, Chan CM, Fu YT, Ho LC, Cheung FC
and Law CK: Acute hemorrhage in late radiation necrosis of the
temporal lobe: Report of five cases and review of the literature. J
Neurooncol. 51:143–150. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nonoguchi N, Miyatake S, Fukumoto M,
Furuse M, Hiramatsu R, Kawabata S, Kuroiwa T, Tsuji M, Fukumoto M
and Ono K: The distribution of vascular endothelial growth
factor-producing cells in clinical radiation necrosis of the brain:
Pathological consideration of their potential roles. J Neurooncol.
105:423–431. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Motegi H, Kuroda S, Ishii N, Aoyama H,
Terae S, Shirato H and Iwasaki Y: De novo formation of cavernoma
after radiosurgery for adult cerebral arteriovenous
malformation-case report. Neurol Med Chir (Tokyo). 48:397–400.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Tanaka S, Shin M, Mukasa A, Hanakita S,
Saito K, Koga T and Saito N: Stereotactic radiosurgery for
intracranial gliomas. Neurosurg Clin N Am. 24:605–612. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ogura K, Mizowaki T, Arakawa Y, Sakanaka
K, Miyamoto S and Hiraoka M: Efficacy of salvage stereotactic
radiotherapy for recurrent glioma: Impact of tumor morphology and
method of target delineation on local control. Cancer Med.
2:942–949. 2013. View
Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ryken TC, Parney I, Buatti J, Kalkanis SN
and Olson JJ: The role of radiotherapy in the management of
patients with diffuse low grade glioma: A systematic review and
evidence based clinical practice guideline. J Neurooncol.
125:551–583. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kanda T, Wakabayashi Y, Zeng F, Ueno Y,
Sofue K, Maeda T, Nogami M and Murakami T: Imaging findings in
radiation therapy complications of the central nervous system. Jpn
J Radiol. 36:519–527. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Furuse M, Miyatake SI and Kuroiwa T:
Cavernous malformation after radiation therapy for astrocytoma in
adult patients: Report of 2 cases. Acta Neurochir (Wien).
147:1097–1101. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Jain R, Robertson PL, Gandhi D, Gujar SK,
Muraszko KM and Gebarski S: Radiation-induced cavernomas of the
brain. AJNR Am J Neuroradiol. 26:1158–1162. 2005.PubMed/NCBI
|
|
11
|
Lee JK, Chelvarajah R, King A and David
KM: Rare presentations of delayed radiation injury: A lobar
hematoma and a cystic space-occupying lesion appearing more than 15
years after cranial radiotherapy: Report of two cases.
Neurosurgery. 54:1010–1013. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Shah R, Vattoth S, Jacob R, Manzil FF,
O'Malley JP, Borghei P, Patel BN and Cure JK: Radiation necrosis in
the brain: Imaging features and differentiation from tumor
recurrence. Radiographics. 32:1343–1359. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rahmathulla G, Marko NF and Weil RJ:
Cerebral radiation necrosis: A review of the pathobiology,
diagnosis and management considerations. J Clin Neurosci.
20:485–502. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Cutsforth-Gregory JK, Lanzino G, Link MJ,
Brown RD Jr and Flemming KD: Characterization of radiation-induced
cavernous malformations and comparison with a nonradiation
cavernous malformation cohort. J Neurosurg. 122:1214–1222. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kawano H, Sato K, Hosotani K, Kubota T,
Goya T, Arikawa S and Wakisaka S: Repeating hemorrhage with a long
duration after radiotherapy for glioma: Radiological and
histological observations. Brain Tumor Pathol. 13:85–92. 1996.
|
|
16
|
Yoshii Y: Pathological review of late
cerebral radionecrosis. Brain Tumor Pathol. 25:51–58. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Winkler EA, Rutledge C, Ward M, Tihan T,
Sneed PK, Barbaro N, Garcia P, McDermott M and Chang EF:
Radiation-induced cavernous malformation as a late sequelae of
stereotactic radio surgery for epilepsy. Cureus. 11:e23082018.
|
|
18
|
Singla A, Brace O'Neill JE, Smith E and
Scott RM: Cavernous malformations of the brain after treatment for
acute lymphocytic leukemia: Presentation and long-term follow-up. J
Neurosurg Pediatr. 11:127–132. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hoffman LM, Plimpton SR, Foreman NK,
Stence NV, Hankinson TC, Handler MH, Hemenway MS, Vibhakar R and
Liu AK: Fractionated stereotactic radiosurgery for recurrent
ependymoma in children. J Neurooncol. 116:107–111. 2014. View Article : Google Scholar : PubMed/NCBI
|