Introduction
Cervical cancer is one of the main causes of cancer
death in women (1), most of which is
caused by human papillomavirus (HPV) infection (2). Approximately 86% of women who die from
cervical cancer are in developing countries (3,4).
According to the clinical stage standard issued by FIGO, cervical
cancer was staged based on the depth of tumor invasion and the
degree of invasion to surrounding tissues (5). Patients with cervical cancer with FIGO
stage I–II were divided into early cervical cancer (6). Although these were not mentioned in
FIGO stage, lymph node metastasis has a very close relationship
with the prognosis of cervical cancer and is the most important in
cervical cancers (7).
Clinically, various imaging methods are used to
detect lymph node metastasis in cancer, including magnetic
resonance imaging (MRI) and computed tomography (CT) (8). CT imaging is very common in various
clinical diagnoses. Its clinical value in tumor diagnosis and
differential diagnosis cannot be ignored, and it has non-invasive
advantages (9,10). MRI has no radiation effect on human
body. It can complete local and whole body scanning, which is more
advanced and safe. Compared with CT, it also provides more
anatomical details for diagnosis and the image contains more
abundant texture information than CT images. Therefore, it is
challenging to compare the advantages and disadvantages of MRI and
CT. This needs to be analyzed on a case-by-case basis (11,12). In
this study, we compared the diagnostic value and clinical
significance of MRI and CT in detecting lymph node metastasis of
early cervical cancer.
Patients and methods
Collection of baseline data
In this study, we selected 160 patients with lymph
node metastasis of cervical cancer from April 2015 to April 2019,
including 122 patients with squamous cell carcinoma, 18 patients
with adenosquamous carcinoma, 10 patients with endometrioid
adenocarcinoma and 10 patients with clear cell carcinoma. The age
of patients ranged from 28 to 64 years, with an average age of
35.59±4.02 years. FIGO stage included 17 cases in stage Ia, 47
cases in stage Ib, 43 cases in stage IIa and 53 cases in stage
IIb.
Inclusion criteria: i) The patient was diagnosed as
cervical cancer by pathology after treatment in Jining No. 1
People's Hospital (Jining, China); ii) FIGO stage was stage I and
II in patients. iii) Patients underwent plain scan to increase
examination before operation (the scanning range included at least
inferior diaphragm to pubic symphysis). iv) The patient had no
other treatment before surgery. v) Patients selected radical
hysterectomy bilateral salpingo-oophorectomy and pelvic
lymphadenectomy, radical hysterectomy pelvic lymphadenectomy
para-aortic lymphadenectomy. vi) Patients and their families signed
informed consent forms in advance. The study was approved by the
Ethics Committee of Jining No. 1 Hospital.
Exclusion criteria: i) Patients who received only
plain scan or only pelvic plain scan and enhanced scan before
operation. ii) The stage of FIGO was stage III or above and the
postoperative pathology was cervical intraepithelial neoplasia.
iii) Scan did not conform to the standard, patient examination
preparation was not perfect or contrast agent injection factors did
not conform to the diagnostic criteria. iv) The treatment method
was radiotherapy, chemotherapy or other treatment methods. v) The
patient received other preoperative treatment.
Examination methods
i) Main reagents and instruments: Siemens Verio 3.0T
superconducting magnetic resonance was from Siemens. Gd-DTPA, a
bolus contrast agent, 18F-deoxyglucose
(18FDG), a CT imaging agent, were from Accdon. CT
scanners were from Royal Philips Electronics. Sixty-four slice CT
was from Siemens.
ii) CT examination methods: The patient should
avoid, or consume only liquid food with little residue the day
before the examination to ensure the formation of unformed feces.
The enema was cleaned with warm water before examination for 1–2 h.
Patients drank 600–800 ml warm boiled water to fill the bladder
30–60 min before examination to increase the contrast with the
uterus. Retention enema was performed ~5 min before CT scan: In
order to fully dilate the rectum, the patient was placed in the
left lateral position, taking the tolerance dose as the degree, and
injected ~400 ml warm water through the anus with the intestinal
irrigator bag to increase the contrast between the large intestine
and the uterus. Training the patient's breathing before
examination: It is required to hold the breath after inhaling
calmly during examination, and to breathe calmly if the breath
cannot be held. Before the examination, the technical operator
explained to the patient the matters needing attention and checked
whether the patient had any foreign matters affecting diagnosis,
such as metal. The most commonly used volume of continuous scanning
method was adopted: The tube voltage was 120 kV, the tube current
was 300 mA, the slice thickness was 5 mm, the interlayer spacing
was 5 mm and the reconstruction thickness was 1 mm. The patient was
placed in a supine position with both hands on the top of the head.
The scanning range included at least inferior diaphragm to pubic
symphysis. After conventional axial plain CT scan, the body
position remained unchanged. Professional nurses injected 100 ml of
nonionic contrast agent through superficial vein of the elbow with
high pressure injector at an injection rate of 2.5–3.0 ml/sec.
Arterial phased scan was performed ~30 sec later, mainly scanning
the liver. Portal phase enhanced scan was performed ~65–75 sec,
including whole abdomen or chest and abdomen and pelvic.
Equilibrium phase can be added to scan when it was necessary
according to lesion display and diagnostic needs.
iii) MRI examination methods: The examinee did not
eat for 48 h, and drank a proper amount of water to fill the
bladder before 9 a.m. on the examination day. Then scan of 4.0
mm/layer was performed. The examination sequences were as follows:
sagittal SET1WI, TR/TE 364/15 msec; sagittal TSE T2WI, TR/TE
2890/108 msec; sagittal fat suppression T2W(ISTIR), TR/TE3840/103
msec, TI 115 msec; oblique transverse T2WI of scanning diameter
line and perpendicular to uterine axis, TR/TE 4890/84 msec; Gd-DTPA
T1WI transverse, TR/TE 397/15 msec; The sagittal scan parameters of
T1WI were the same as those of plain scan.
The CT and MRI images were read by two radiologists
with more than 10 years experience and no knowledge of the surgical
and pathological results. The CT staging and MRI staging of
cervical cancer were carried out according to the reading
results.
Judgement of criterion
i) Image analysis of MRI diagnostic stage (Table I). ii) Image analysis of CT diagnosis
of SC stage (Table II).
 | Table I.Features of MRI of early cervical
cancer in different stages. |
Table I.
Features of MRI of early cervical
cancer in different stages.
| Grouping | Features |
|---|
| Stage Ia | No evidence of mass
lesion. |
| Stage Ib | Tumor pierced
cervical low signal intensity ring. |
| Stage IIa | The tumor pierced the
upper vagina but did not touch the parametrium. |
| Stage IIb | The matrix of the
cervix was destroyed and the parametrium tissues were invaded. |
| Table II.Features of CT of early cervical
cancer in different stages. |
Table II.
Features of CT of early cervical
cancer in different stages.
| Grouping | Features |
|---|
| Stage Ia | No metastatic lymph
nodes. |
| Stage Ib | Metastatic lymph
nodes appeared, but were not obvious. |
| Stage IIa | Metastatic lymph
nodes appeared but did not invade the parametrium. |
| Stage IIb | Metastatic lymph
nodes began to invade the parametrium. |
Statistical methods
Data analysis was completed by SPSS 18.0. The
counting data were expressed as [n(%)]. The χ2 test was
used for univariate analysis and comparison of the diagnostic
accuracy of SC at each stage. The difference was statistically
significant at P<0.05.
Results
Baseline data
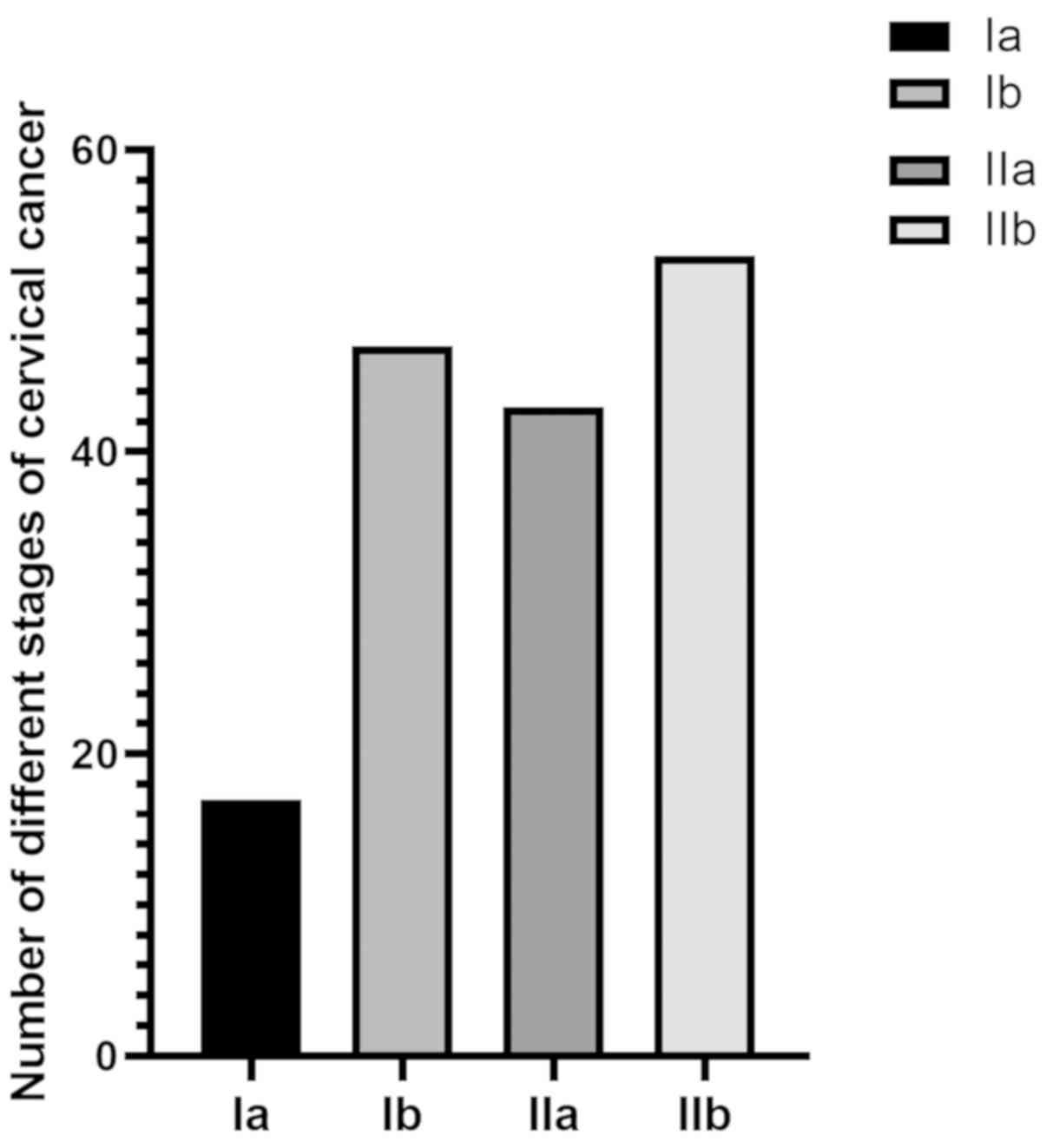
The basic conditions of 160 patients were
investigated, such as age, obesity, smoking and drinking habits,
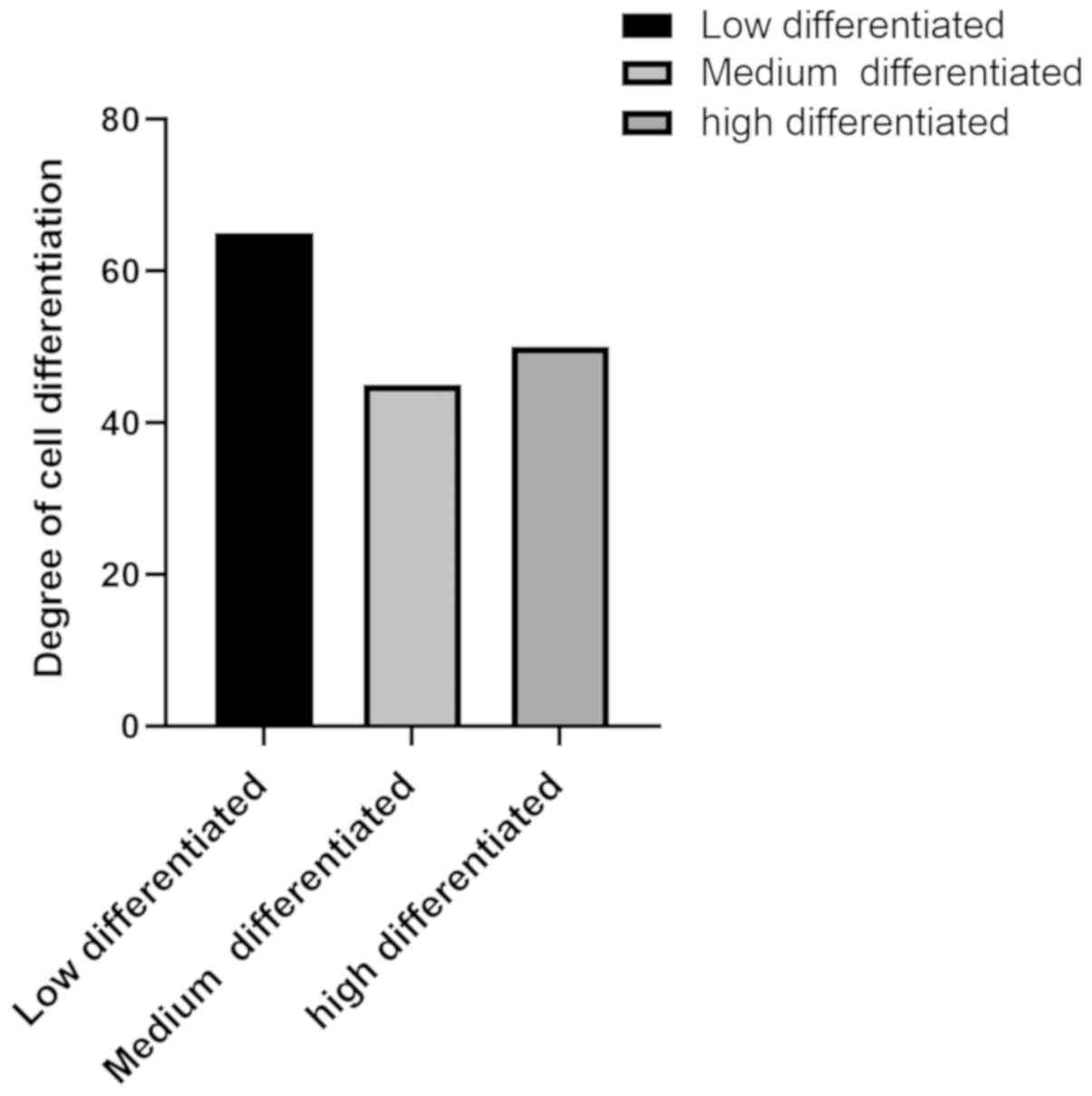
histological classification, clinical stage (Fig. 1 and Table III). Degree of differentiation and
lymph node metastasis of cervical cancer are shown in (Fig. 2).
| Table III.Baseline clinical data of 160 SC
patients. |
Table III.
Baseline clinical data of 160 SC
patients.
| Factors | [n(%)] |
|---|
| Age (years) |
|
| ≤50 | 105 (65.63) |
|
>50 | 55 (34.37) |
| Smoking |
|
| Yes | 81 (50.63) |
| No | 79 (49.67) |
| Drinking |
|
| Yes | 78 (48.75) |
| No | 82 (51.25) |
| Obesity |
|
| Yes | 80 (50.00) |
| No | 80 (50.00) |
| Histological
classification of cervical cancer |
|
| Squamous
cell carcinoma | 122 (76.25) |
|
Adenosquamous carcinoma | 18 (11.25) |
|
Endometrioid
adenocarcinoma | 10 (6.25) |
| Clear
cell carcinoma | 10 (6.25) |
| Clinical stage of
cervical cancer |
|
| Stage
Ia | 17 (10.63) |
| Stage
Ib | 47 (29.37) |
| Stage
IIa | 43 (26.87) |
| Stage
IIb | 53 (33.13) |
| Differentiation
degree |
|
| Poorly
differentiated | 65 (40.63) |
| Middle
differentiated | 45 (28.12) |
| Well
differentiated | 50 (31.25) |
| Lymph node
metastasis |
|
| Yes | 96 (60.00) |
| No | 64 (40.00) |
Diagnostic efficiency of MRI and CT in
lymph node metastasis of early cervical cancer in different
stages
i) Diagnostic efficacy of MRI and CT
in lymph node metastasis of early cervical cancer in stage I
The sensitivity, specificity and diagnostic
accordance rate of MRI in the diagnosis of early cervical cancer in
stage I were 75.00%, 72.92 and 77.50%, respectively. The
sensitivity, specificity and diagnostic accordance rate of CT in
the diagnosis of early cervical cancer in stage I were 62.50, 56.25
and 58.75%, respectively. Comparing data of the two groups, the
sensitivity, specificity and diagnostic accordance rates of MRI in
the diagnosis of early cervical cancer in stage I were
significantly higher than those of CT (P<0.05) (Tables IV–VI).
| Table IV.Diagnostic efficacy of MRI in lymph
node metastasis of early cervical cancer in stage I. |
Table IV.
Diagnostic efficacy of MRI in lymph
node metastasis of early cervical cancer in stage I.
|
| Pathological
diagnostic results |
|
|---|
|
|
|
|
|---|
| Grouping | Stage Ia-Ib | Stage non-Ia-Ib | Total |
|---|
| Ia-Ib phase by MRI
diagnosis | 54 | 26 | 80 |
| Non-Ia-Ib phase by
MRI diagnosis | 10 | 70 | 80 |
| Total | 64 | 96 | 160 |
| Table VI.Comparison of diagnostic efficiency
of MRI and CT in lymphatic metastasis of early cervical cancer in
stage I. |
Table VI.
Comparison of diagnostic efficiency
of MRI and CT in lymphatic metastasis of early cervical cancer in
stage I.
| Factors | MRI | CT | χ2
value | P-value |
|---|
| Sensitivity | 75.00% (54/64) | 62.50% (40/64) | 7.850 | 0.005 |
| Specificity | 72.92% (70/96) | 56.25% (54/96) | 5.829 | 0.016 |
| Diagnostic
accordance rate | 77.50%
(124/160) | 58.75%
(94/160) | 12.950 | <0.001 |
ii) Diagnostic efficacy of MRI and CT
in lymphatic metastasis of early cervical cancer in stage II
The sensitivity, specificity and diagnostic
accordance rate of MRI in the diagnosis of lymphatic metastasis of
early cervical cancer in stage II were 79.17, 78.13 and 78.75%,
respectively. The sensitivity, specificity and diagnostic
accordance rate of CT in the diagnosis of lymphatic metastasis of
early cervical cancer in stage II were 62.50, 68.75 and 60.00%,
respectively. Comparing the data of the two groups, the
sensitivity, specificity and diagnostic accordance rate of MRI in
the diagnosis of lymphatic metastasis of early cervical cancer in
stage II were significantly higher than those of CT in the
diagnosis of lymphatic metastasis of early cervical cancer in stage
II (P<0.05). However, there was no obvious difference in
specificity (P>0.05) (Tables
VII–IX).
| Table VII.Diagnostic efficacy of MRI in
lymphatic metastasis of early cervical cancer in stage II. |
Table VII.
Diagnostic efficacy of MRI in
lymphatic metastasis of early cervical cancer in stage II.
|
| Pathological
diagnostic results |
|
|---|
|
|
|
|
|---|
| Grouping | Stage IIa-IIb | Stage
non-IIa-IIb | Total |
|---|
| IIa-IIb phase by
MRI diagnosis | 76 | 14 | 70 |
| Non-IIa-IIb phase
by MRI diagnosis | 20 | 50 | 90 |
| Total | 96 | 64 | 160 |
| Table IX.Comparison of diagnostic efficiency
of MRI and CT in lymphatic metastasis of early cervical cancer in
stage II. |
Table IX.
Comparison of diagnostic efficiency
of MRI and CT in lymphatic metastasis of early cervical cancer in
stage II.
| Factors | MRI | CT | χ2
value | P-value |
|---|
| Sensitivity | 79.17% (76/96) | 62.50% (60/96) | 6.454 | 0.011 |
| Specificity | 78.13% (50/64) | 68.75% (44/64) | 1.442 | 0.230 |
| Diagnostic
accordance rate | 78.75%
(126/160) | 58.75%
(94/160) | 14.890 | <0.001 |
Comparison of diagnostic efficiency
between MRI combined with CT and MRI or CT alone in lymphatic
metastasis of early cervical cancer in different stage
The sensitivity, specificity and diagnostic
accordance rate of MRI combined with CT in the diagnosis of early
cervical cancer in stage I were 78.13, 87.50 and 83.75%,
respectively, which were significantly higher than the sensitivity
and diagnostic accordance rate of MRI or CT alone (P<0.05).
However, the sensitivity, specificity and diagnostic accordance
rate of MRI combined with CT in the diagnosis of early cervical
cancer in stage II were 91.66, 82.81 and 88.13%, respectively.
There was no obvious difference in specificity (P>0.05), the
specificity and diagnostic accordance rate were significantly
higher than that of MRI or CT alone (P<0.05) (Tables X–XII).
| Table X.Diagnostic efficacy of MRI combined
with CT in lymphatic metastasis of early cervical cancer in stage
I. |
Table X.
Diagnostic efficacy of MRI combined
with CT in lymphatic metastasis of early cervical cancer in stage
I.
|
| Pathological
diagnostic results |
|
|---|
|
|
|
|
|---|
| Grouping | Stage Ia-Ib | Stage
non-Ia-Ib | Total |
|---|
| Ia-Ib phase by
combined diagnosis | 50 | 12 | 62 |
| Non-Ia-Ib phase by
combined diagnosis | 14 | 84 | 98 |
| Total | 64 | 96 | 160 |
| Table XII.Comparison of the diagnostic efficacy
between combined diagnosis with MRI or CT alone. |
Table XII.
Comparison of the diagnostic efficacy
between combined diagnosis with MRI or CT alone.
| Factors | Combination | MRI | CT | P-value |
|---|
| Stage Ia-Ib |
|
Sensitivity | 78.13% (50/64) | 75.00% (54/64) | 62.50% (40/64) | 0.013 |
|
Specificity | 87.50% (84/96) | 72.92% (70/96) | 56.25% (54/96) | <0.001 |
|
Diagnostic accordance
rate | 83.75%
(134/160) | 77.50%
(124/160) | 58.75%
(94/160) | <0.001 |
| Stage IIa-IIb |
|
Sensitivity | 91.66% (90/96) | 79.17% (76/96) | 62.50% (60/96) | <0.001 |
|
Specificity | 82.81% (53/64) | 78.13% (50/64) | 68.75% (44/64) | 0.161 |
|
Diagnostic accordance
rate | 88.13%
(143/160) | 78.75%
(126/160) | 58.75%
(94/160) | <0.001 |
Discussion
Cervical cancer is particularly harmful to women in
developing countries, and screening its level is very important
(13,14). However, two imaging techniques, CT
and MRI, play a vital role in the early stage of cancer, treatment
strategy and treatment of response evaluation (15–17). In
many studies on lung cancer, prostate cancer and breast cancer, MRI
and CT are widely used (18–20). These technologies have their own
advantages and disadvantages, and are suitable for examining
different tumors (21). Therefore,
the purpose of this study was to compare the diagnostic value of
the two imaging methods in the detection of lymph node metastasis
of early cervical cancer.
In this study, different stages of patients with
early cervical cancer were examined with MRI, and CT alone, and MRI
combined with CT, and their diagnostic efficacy such as
sensitivity, specificity, diagnostic accordance rate was compared.
According to the results, the sensitivity, specificity and
diagnostic accordance rate of MRI in the diagnosis of lymph node
metastasis of early cervical cancer with stage I (Ia-Ib) were
significantly higher than those of CT in the diagnosis of lymph
node metastasis of early cervical cancer with stage I (Ia-Ib). In
addition to specificity, the sensitivity, diagnostic accordance
rate of MRI in the diagnosis of lymph node metastasis of early
cervical cancer with stage II (IIa-IIb) were significantly higher
than the sensitivity, specificity, and diagnostic accordance rate
by CT diagnosis. In another study on cervical cancer, it was found
that MRI is better than CT in diagnosing cervical cancer. It can
not only be useful for the discovery of early cervical cancer, but
also for reasonable staging (22).
However, in the study of Li and Room (23) on invasive cervical cancer, MRI was
shown to be better than CT in observing tumor size and boundary,
the signal was easy to identify, and the diagnostic accordance rate
for lymphatic metastasis was also very high. It was concluded that
MRI has better diagnostic efficiency and higher clinical diagnostic
value than CT in the diagnosis of lymph node metastasis of early
cervical cancer.
In a study on lymphoma, it was found that MRI
combined with CT has good examination effect (24). Therefore, in this study, we also
carried out combined examination of MRI and CT on patients.
According to the results, besides the specificity index for
diagnosing lymph node metastasis of early cervical cancer in stage
II (IIa-IIb), the sensitivity and diagnostic accordance rate of MRI
combined with CT diagnosis were significantly higher than those of
MRI and CT alone. CT has good density resolution, can avoid
intestinal peristalsis and other effects to a certain extent. It is
visual and has certain advantages in finding lymph node diffusion,
but its diagnostic sensitivity to cancer staging is not strong, and
its differentiation specificity for lesions is not high. However,
MRI has higher tissue resolution and better tissue contrast. It can
directly display the tumor condition and can change imaging
parameters to improve its contrast, thus improving the prediction
range of tumors (25). Complementary
advantages of the two can have a better examination effect.
Therefore, we conclude that the diagnostic value of MRI and CT
combined diagnosis was higher than that each alone. In the study of
Kim et al (26) on non-small
cell lung cancer, the combination of MRI and CT was more helpful to
significantly improve the sensitivity of detecting lymph node
metastasis than CT alone. In a clinical study of calcified
meningioma, it was found that CT combined with MRI diagnosis has a
higher diagnostic accordance rate for tumors and a more
comprehensive and obvious reflection on the characteristics of
tumors (27). These are all similar
to the results of the present study.
In conclusion, the diagnostic value of MRI in the
clinical diagnosis of lymph node metastasis of early cervical
cancer is significantly higher than that of CT and the sensitivity,
specificity and diagnostic accordance rate are significantly
improved when they are combined. Therefore, we consider that MRI
and CT should be combined in clinic to improve the diagnostic
accuracy of diseases.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
LL wrote the manuscript, interpreted and analyzed
the data. QL designed the study and performed the experiments. LT
was responsible for the analysis and discussion of the data. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Jining No. 1 People's Hospital (Jining, China). Patients who
participated in this research had complete clinical data. Signed
informed consents were obtained from the patients and/or the
guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Small W Jr, Bacon MA, Bajaj A, Chuang LT,
Fisher BJ, Harkenrider MM, Jhingran A, Kitchener HC, Mileshkin LR,
Viswanathan AN, et al: Cervical cancer: A global health crisis.
Cancer. 123:2404–2412. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wentzensen N, Schiffman M, Palmer T and
Arbyn M: Triage of HPV positive women in cervical cancer screening.
J Clin Virol. 76 (Suppl 1):S49–S55. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Denny L: Cervical cancer: Prevention and
treatment. Discov Med. 14:125–131. 2012.PubMed/NCBI
|
|
4
|
Sreedevi A, Javed R and Dinesh A:
Epidemiology of cervical cancer with special focus on India. Int J
Womens Health. 7:405–414. 2015.PubMed/NCBI
|
|
5
|
Dornhöfer N and Höckel M: New developments
in the surgical therapy of cervical carcinoma. Ann NY Acad Sci.
1138:233–252. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tsili AC, Tsangou V, Koliopoulos G, Stefos
T and Argyropoulou MI: Early-stage cervical carcinoma: The role of
multidetector CT in correlation with histopathological findings. J
Obstet Gynaecol. 33:882–887. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hosaka M, Watari H, Mitamura T, Konno Y,
Odagiri T, Kato T, Takeda M and Sakuragi N: Survival and
prognosticators of node-positive cervical cancer patients treated
with radical hysterectomy and systematic lymphadenectomy. Int J
Clin Oncol. 16:33–38. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Petersen LJ, Nielsen JB, Langkilde NC,
Petersen A, Afshar-Oromieh A, De Souza NM, De Paepe K, Fisker RV,
Arp DT, Carl J, et al: 68Ga-PSMA PET/CT compared with
MRI/CT and diffusion-weighted MRI for primary lymph node staging
prior to definitive radiotherapy in prostate cancer: a prospective
diagnostic test accuracy study. World J Urol. 2019.doi:
10.1007/s00345-019-02846-z. [Epub ahead of print]. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kinahan PE, Townsend DW, Beyer T and
Sashin D: Attenuation correction for a combined 3D PET/CT scanner.
Med Phys. 25:2046–2053. 1998. View
Article : Google Scholar : PubMed/NCBI
|
|
10
|
Shin S, Pak K and Kim SJ, Kim H and Kim
SJ: Pulmonary tumor embolism derived from stomach cancer
observation with serial 18F-FDG PET/CT. Clin Nucl Med.
40:270–272. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Nie D, Cao X, Gao Y, Wang L and Shen D:
Estimating CT image from MRI data using 3D fully convolutional
networks. Deep Learn Data Label Med Appl (2016). 2016:170–178.
2016.PubMed/NCBI
|
|
12
|
Low RN and Gurney J: Diffusion-weighted
MRI (DWI) in the oncology patient: Value of breathhold DWI compared
to unenhanced and gadolinium-enhanced MRI. J Magn Reson Imaging.
25:848–858. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Marth C, Landoni F, Mahner S, McCormack M,
Gonzalez-Martin A and Colombo N; ESMO Guidelines Committee, :
Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis,
treatment and follow-up. Ann Oncol. 28 (Suppl 4):iv72–iv83. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Landy R, Pesola F, Castañón A and Sasieni
P: Impact of cervical screening on cervical cancer mortality:
Estimation using stage-specific results from a nested case-control
study. Br J Cancer. 115:1140–1146. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lucia F, Visvikis D, Desseroit MC, Miranda
O, Malhaire JP, Robin P, Pradier O, Hatt M and Schick U: Prediction
of outcome using pretreatment 18F-FDG PET/CT and MRI
radiomics in locally advanced cervical cancer treated with
chemoradiotherapy. Eur J Nucl Med Mol Imaging. 45:768–786. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Choi J, Kim HJ, Jeong YH, Lee JH, Cho A,
Yun M, Lee JD, Kim YB, Kim YT and Kang WJ: The role of
18F-FDG PET/CT in assessing therapy response in cervix
cancer after concurrent chemoradiation therapy. Nucl Med Mol
Imaging. 48:130–136. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Patel CN, Nazir SA, Khan Z, Gleeson FV and
Bradley KM: 18F-FDG PET/CT of cervical carcinoma. AJR Am
J Roentgenol. 196:1225–1233. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kim HS, Lee KS, Ohno Y, van Beek EJ and
Biederer J: PET/CT versus MRI for diagnosis, staging, and follow-up
of lung cancer. J Magn Reson Imaging. 42:247–260. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Shen G, Deng H, Hu S and Jia Z: Comparison
of choline-PET/CT, MRI, SPECT, and bone scintigraphy in the
diagnosis of bone metastases in patients with prostate cancer: A
meta-analysis. Skeletal Radiol. 43:1503–1513. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sawicki LM, Grueneisen J, Schaarschmidt
BM, Buchbender C, Nagarajah J, Umutlu L, Antoch G and Kinner S:
Evaluation of 18F-FDG PET/MRI, 18F-FDG
PET/CT, MRI, and CT in whole-body staging of recurrent breast
cancer. Eur J Radiol. 85:459–465. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Cazzato RL, Garnon J, Shaygi B, Koch G,
Tsoumakidou G, Caudrelier J, Addeo P, Bachellier P, Namer IJ and
Gangi A: PET/CT-guided interventions: Indications, advantages,
disadvantages and the state of the art. Minim Invasive Ther Allied
Technol. 27:27–32. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Yong HE: Comparative analysis of
diagnostic value of imaging of cervical cancers by
B-ultrasonography, CT and MRI. Acta Med Sin. 03:413–415. 2009.
|
|
23
|
Li LC and Room C: Clinical value of
preoperative CT and MRI on diagnosing invasive cervical cancer. Han
Shao Ji Bing Za Zhi. 01:62–63. 2018.(In Chinese).
|
|
24
|
Heacock L, Weissbrot J, Raad R, Campbell
N, Friedman KP, Ponzo F and Chandarana H: PET/MRI for the
evaluation of patients with lymphoma: Initial observations. AJR Am
J Roentgenol. 204:842–848. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Bin D and Li ZL: Value analysis and
efficacy observation of CT in combination with MRI on staging
diagnosis of endometrial carcinoma. Chin J Ct Mri. 04:107–109.
2016.
|
|
26
|
Kim YN, Yi CA, Lee KS, Kwon OJ, Lee HY,
Kim BT, Choi JY, Kim SW, Chung MP, Han J, et al: A proposal for
combined MRI and PET/CT interpretation criteria for preoperative
nodal staging in non-small-cell lung cancer. Eur Radiol.
22:1537–1546. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ren F, Gao L, Yao FM, Hu TB and Lin MJ:
The technological efficacy of CT combined with MRI in diagnosing
calcified meningioma. Health Res. 3:259–260. 2014.
|