Introduction
Breast cancer is the most commonly reported type of
cancer worldwide and was the second leading cause of
cancer-associated mortality in females (1). In recent years, with increasing
prevalence, particularly in young patients, breast cancer is
considered to be one of the most common malignancies (2). Breast cancer is often characterized as
highly heterogeneous at the molecular level. On the basis of the
expression of estrogen receptor (ER), progesterone receptor (PR),
human epidermal growth factor receptor 2 (HER-2) and Ki67, four
different molecular subtypes of breast cancer have been identified,
including luminal A, luminal B, triple-negative and
HER-2-overexpression. Luminal A is characterized as ER+
and/or PR+, HER-2−, cytokeratin 5/6
(CK5/6)+/− and Ki67 <14%. Luminal B is ER+
and/or PR+, CK5/6+/−, HER-2+ and
Ki67 ≥14%. The HER-2-overexpression subtype is characterized as
ER−, PR−, HER-2+ and
CK5/6+/−. Lastly, triple-negative is ER−,
PR−, HER-2−, CK5/6+ and/or
epidermal growth factor receptor (EGFR) +(3–6). The
clinical manifestations, treatment response and prognosis vary
significantly between different molecular subtypes of breast
cancer. Patients with breast cancer exhibit different
manifestations in lymph node metastasis, histological grade and
5-year survival rate. Luminal A and luminal B tumors are
well-differentiated and exhibit a low rate of metastasis (7,8).
In clinical practice, it is understood that early
recognition of breast cancer molecular subtypes is important for
early specific treatment of breast cancer, and patients may benefit
from earlier detection and improved therapeutic options with a
prolonged survival time (9,10). In recent years, with the development
of imaging techniques, digital breast tomosynthesis (DBT) has had
an impact on the diagnosis of breast diseases as images of breasts
may be obtained from different angles in the process of scanning
(11). These independent images can
be rebuilt into a series of tomographic images with high
resolution, which eliminates the problems caused by the tissue
overlap and structural noise in a two-dimensional breast
mammography (12,13). Currently, DBT technology is developing
in China. The majority of previous studies have focused on
comparing the diagnostic efficacy of DBT with traditional digital
mammography (14). Furthermore, DBT
has been revealed to improve the characterization of magnetic
resonance imaging results that are not identified by targeted
breast ultrasound in preoperative breast cancer staging (15). However, there is a lack of evidence
demonstrating an association between breast cancer molecular
subtypes and imaging characteristics based on the DBT imaging
technique. A previous study revealed that DBT has important
influence and significance in the classification of breast
imaging-reporting and data system (BI-RADS). The diagnostic
sensitivity increased from 60% with traditional digital mammography
to 82.9% with DBT and the specificity of the two techniques used
together was 93.2% (16). Primary
indicators for BI-RADS classification include tumor margin,
surrounding bright ring of tumor, vascular images and calcification
foci, lymph node size, and associations with surrounding glandular
tissue (17–19), and identification of these indicators
is improved in a tomographic image (20).
On the basis of previous studies, it was
hypothesized that characteristics of DBT imaging could be used to
assist the diagnosis of breast cancer molecular subtypes. The use
of digital imaging to diagnose and authenticate molecular subtypes
of breast cancer is of great interest in this field. The aim of the
present study was to investigate the characteristics of each
molecular subtype of breast cancer based on DBT. In addition, the
associations between imaging features of DBT and molecular subtypes
of breast cancer were evaluated for the accurate diagnosis of tumor
features, with the aim to provide an accurate treatment strategy
for clinical use.
Patients and methods
Patients
Complete pathology and immunohistochemistry data
were collected from 134 female patients with breast cancer with a
mean age of 46.5 years (range, 26–81 years) who had undergone
surgery at The Second Clinical College of Fujian Medical University
(Quanzhou, China) between May 2012 and October 2014. The patients
were divided into the four following groups depending on the
molecular subtype of breast cancer: Luminal A, luminal B,
triple-negative and HER-2-overexpression, according to the
expression of ER, PR, HER-2 and Ki67. For each subtype, there were
a total of 9, 87, 9 and 29 lesions, respectively. The clinical
characteristics and pathological features of different molecular
subtypes of breast cancer were evaluated. The present study was
approved by the Ethics Committee of The Second Clinical College of
Fujian Medical University and each patient involved in the study
provided written informed consent.
Digital mammary gland
three-dimensional tomosynthesis examination
Images captured by a digital mammary gland
three-dimensional tomosynthesis system (Selenia Dimensions;
Hologic, Inc., Marlborough, MA, USA) were analyzed for all
patients. Craniocaudal position and mediolateral oblique (MLO) were
observed. Each rotation of the X-ray tube was limited within 15°,
with a low-dose exposure once at a single 1° rotation and a series
of high-resolution computed tomography images were reconstructed by
15 frames. The full-field digital mammography and the DBT were
obtained at the same stress position, also termed the COMBO
mode.
Image post-processing
The securView 8.1 software (Hologic, Inc.) was used
to post-process the acquired images, with the aim to display more
gray shading and fine structure of the mammary gland, and improve
the ability of image reading.
Evaluation methods
The selected 134 cases of breast cancer were
classified according to the BI-RADS classification diagnosis
criteria (21). During the process of
classification, four physicians were involved to review the images,
reaching a consensus for each patient.
Statistical analysis
SPSS software (version 20.0; IBM Corp., Armonk, NY,
USA) was used for statistical analysis. Data with a normal
distribution are presented as the mean ± standard deviation. Data
without a normal distribution are presented as the median (range).
Numerical data of age was assessed for normal distribution with a
Kolmogorov-Smirnov test followed by one-way analysis of variance
and Fisher's Least Significant Difference test for pairwise
comparisons within the group. Tumor size, calcification score and
lymph node size were compared using a Kruskal-Wallis H test. All
other indicators, including gland type, menopause, tumor margin,
change in nipple position, change in peripheral glands, skin
adhesion, thick blood vessels and lymphatic metastasis, and the
thresholds of indicators, including tumor size, calcification score
and lymph node size, were analyzed using a χ2 test or
Fisher's exact test.
Results
Baseline characteristics of patients
with different molecular subtypes of breast cancer
A total of 134 eligible patients were included in
the present study. According to the expression of ER, PR, HER-2 and
KI67, these patients were divided into four groups as follows:
Luminal A subtype (9 cases with a age of 50.78±13.20 years),
luminal B subtype (87 cases with a age of 47.37±9.60 years),
triple-negative subtype (9 cases with a age of 47.00±8.32 years)
and HER-2-overexpression subtype (29 cases with a age of 51.45±9.64
years). Four types of mammary glands were also included, including
fat, few, mickle and dense. According to fat classification, the
number of patients with the luminal B subtype was significantly
higher compared with those with the luminal A subtype (Table I). Overall, no statistical differences
were identified with regard to age, type of gland and menopause
status in patients with different molecular subtypes of breast
cancer (P<0.05; Table I).
 | Table I.General information of patients with
different molecular subtypes of breast cancer. |
Table I.
General information of patients with
different molecular subtypes of breast cancer.
| Characteristic | Luminal A subtype
(n=9) | Luminal B subtype
(n=87) | Triple-negative
subtype (n=9) | HER-2-overexpression
subtype (n=29) | P-value |
|---|
| Age, years (mean ±
standard deviation) Mammary gland type, n (%) | 50.78±13.20 | 47.37±9.60 | 47.00±8.32 | 51.45±9.64 | 0.219 0.161 |
|
| 1 (11.11) | 4 (4.6)a | 0 (0.00) | 3 (10.34) |
|
|
| 3 (33.33) | 12 (13.79) | 1 (11.11) | 6 (20.69) |
|
|
| 2 (22.22) | 63 (72.41) | 7 (77.78) | 18 (62.07) |
|
|
| 3 (33.33) | 8 (9.2) | 1 (11.11) | 2 (6.90) |
|
| Menopause, n (%) |
| Yes | 4 (44.44) | 30(34.48) | 3 (33.33) | 1 (48.15) |
|
| No | 5 (55.56) | 57(65.52) | 6 (66.67) | 14 (51.85) |
|
Comparative analysis of clinical data
and pathological characteristic data in patients with different
molecular subtypes of breast cancer
Indicators including tumor size, tumor margin
(rough, partial or finishing), calcification score, change in
nipple position (yes or no), change in peripheral glands
(transition, invasion or obvious), skin adhesions (yes or no),
thick blood vessels (yes or no), lymph node metastasis (yes or no)
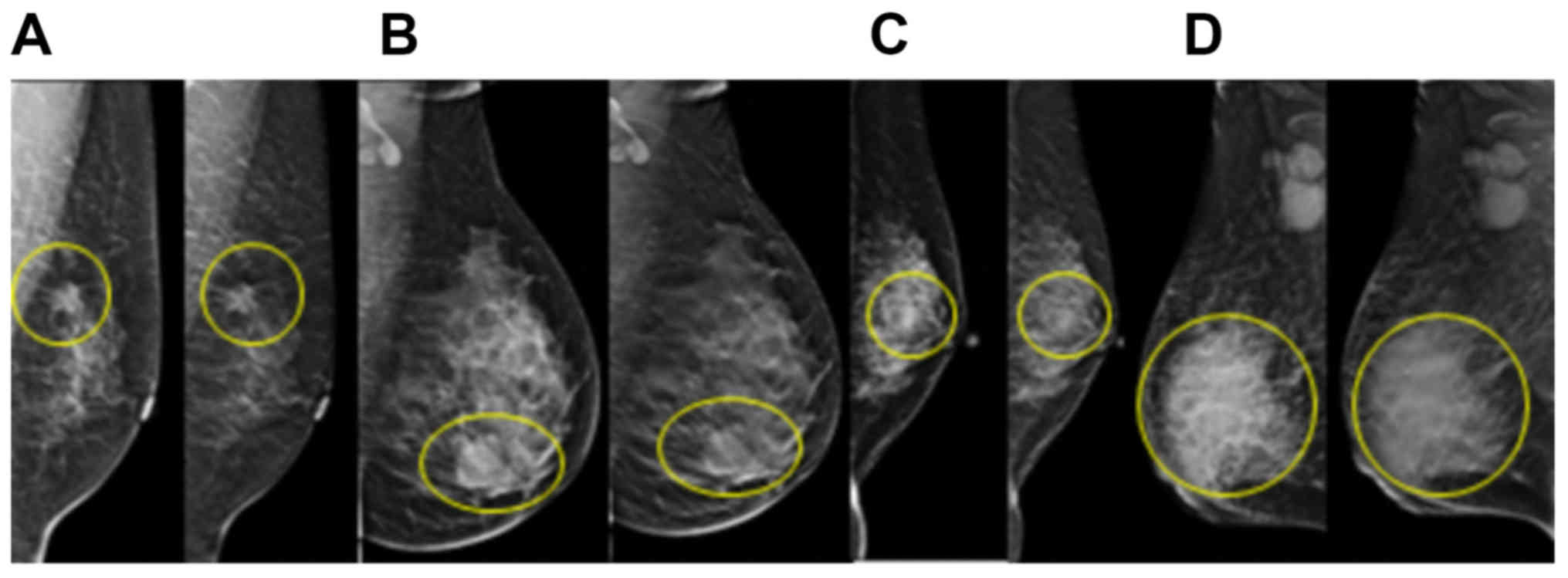
and lymph node size were determined using DBT. The results
demonstrated that tumor size was larger in the triple-negative and
HER-2-overexpression subtypes compared with in the luminal A and
luminal B subtypes (Fig. 1). The
tumor sizes in the luminal A, luminal B, triple-negative and
HER-2-overexpression subtypes were 1.86±0.59, 2.31±0.92, 3.74±1.94
and 3.26±1.81, respectively. However, statistical analysis revealed
no significant differences between these four groups with regard to
tumor size (Table II). The
calcification score was significantly higher in the
HER-2-overexpression subtype compared with in the luminal B
subtype. Calcification scores for luminal A, luminal B,
triple-negative and HER-2-overexpression subtypes were 9.57±1.99,
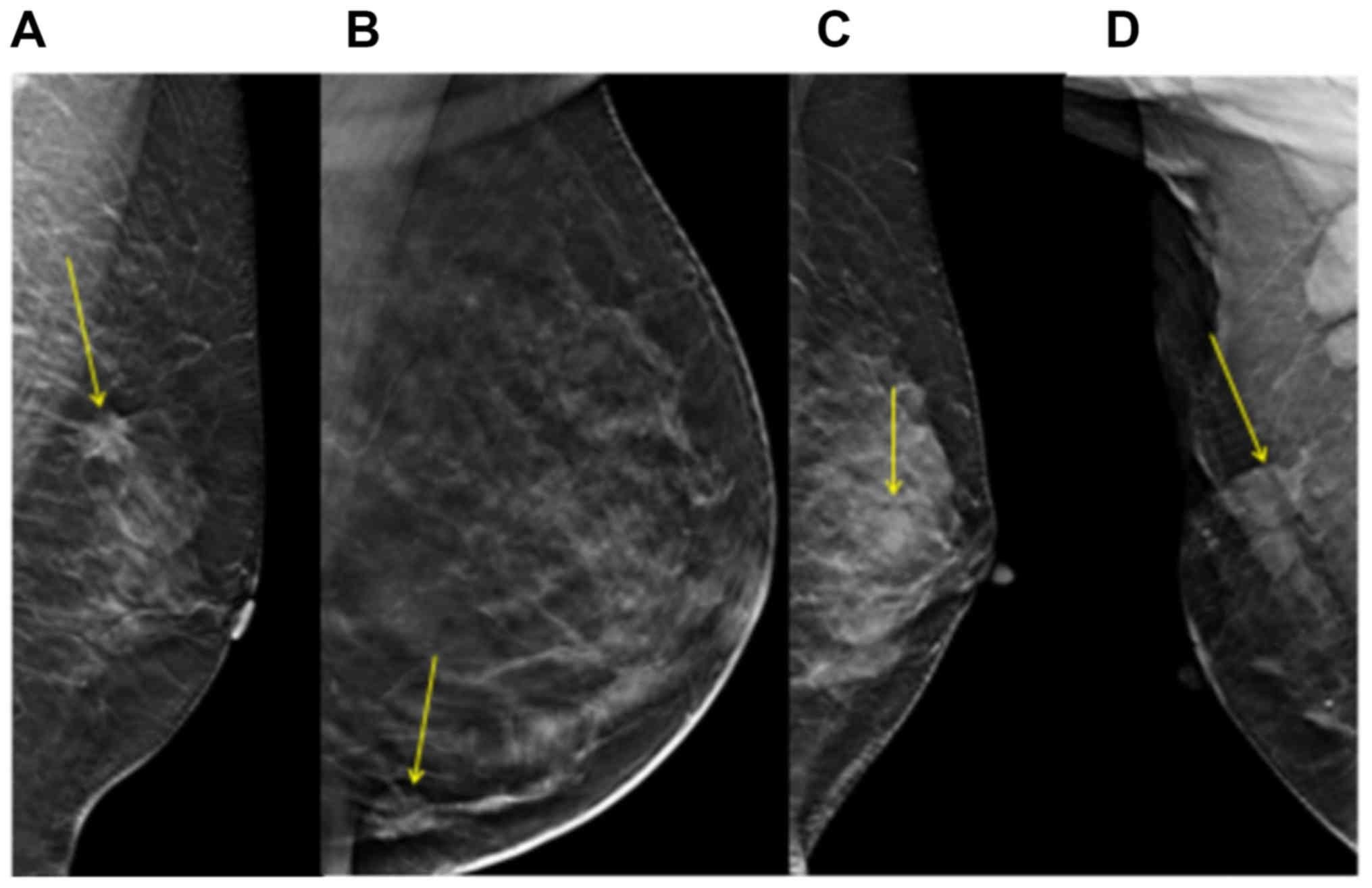
9.45±1.55, 9.43±1.8 and 11±1.41, respectively. For the shape of
tumor margin, no differences were revealed between the different
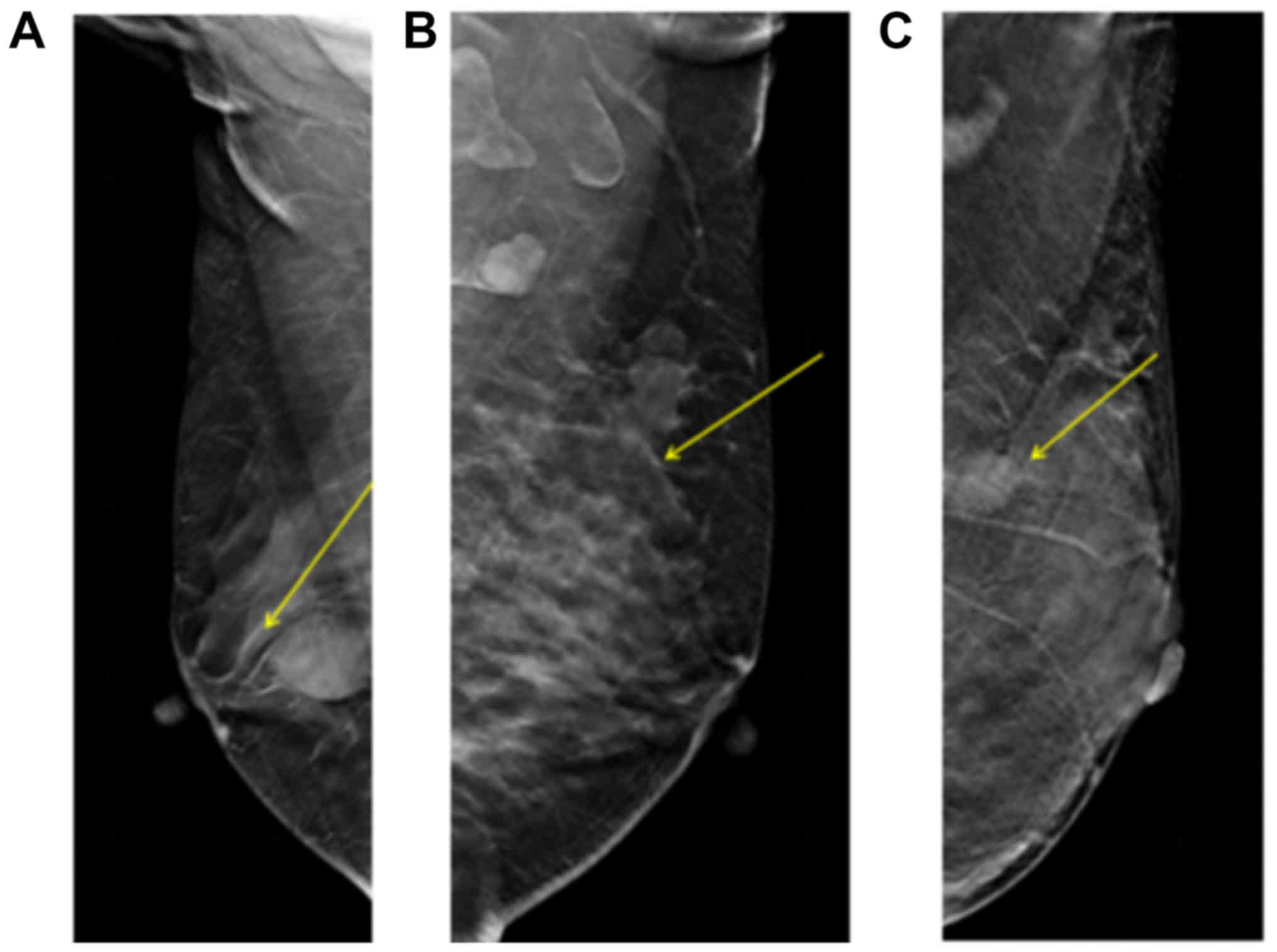
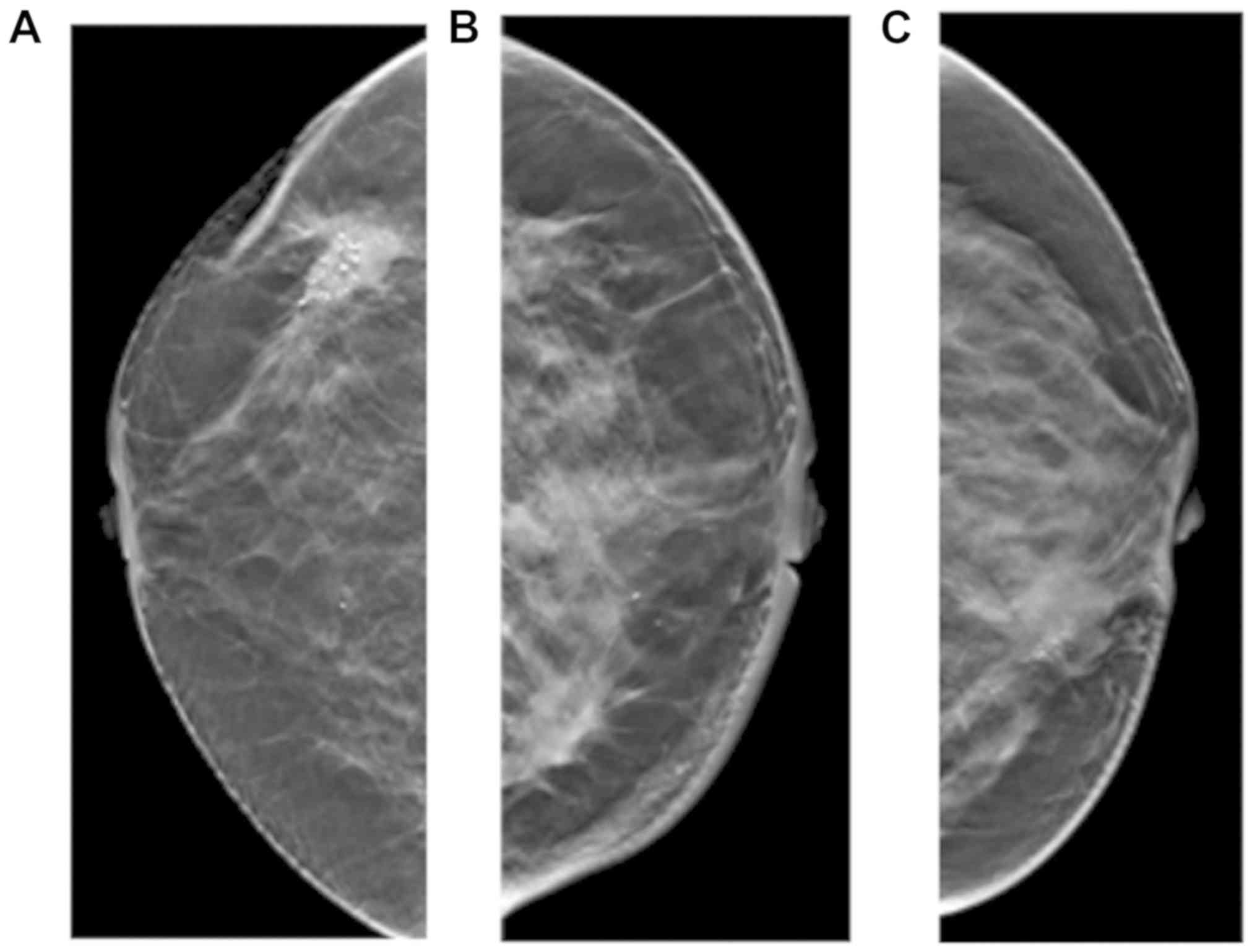
molecular subtypes (Fig. 2). The
change in peripheral glands included types of transition, invasion
and no change. No significant differences were identified between
the various subtypes with regard to change in peripheral glands,
skin adhesion, change in nipple position and (Figs. 3 and 4;
Table II).
| Table II.Clinical and pathological features of
different molecular subtypes of breast cancer. |
Table II.
Clinical and pathological features of
different molecular subtypes of breast cancer.
| Characteristic | Luminal A
subtype | Luminal B
subtype | Triple-negative
subtype | HER-2-overexpression
subtype | P-value |
|---|
| Tumor size, cm
(mean ± SD) | 1.86±0.59 | 2.31±0.92 | 3.74±1.94 | 3.26±1.81 | 0.035,
1.000a,
0.199b,
0.341c,
0.282d,
0.310e,
1.000f |
| Tumor margin, n
(%) |
|
|
|
| 0.093 |
|
Coarse | 4 (80.00) | 46 (63.01) | 3 (42.86) | 10 (50.00) |
|
|
Partial | 0 (0.00) | 24 (32.88) | 4 (57.14) | 6 (30.00) |
|
|
Finishing | 1 (20.00) | 3 (4.11) | 0 (0.00) | 4 (20.00) |
|
| Calcification score
(mean ± SD) | 9.57±1.99 | 9.45±1.55 | 9.43±1.81 | 11±1.41 | 0.003,
1.000a,
1.000b,
0.273c,
1.000d,
0.002e,
0.157f |
| Change in nipple
position, n (%) |
|
|
|
| 0.266 |
|
Yes | 1 (11.11) | 9 (10.34) | 2 (22.22) | 7 (24.14) |
|
| No | 8 (88.89) | 78 (89.66) | 7 (77.78) | 22 (75.86) |
|
| Change in
peripheral glands, n (%) |
|
Transition | 1 (11.11) | 5 (6.17) | 2 (22.22) | 3 (10.34) |
|
|
Invasion | 5 (55.56) | 4 (54.2) | 5 (55.56) | 16 (55.17) |
|
|
Unobvious | 3 (33.33) | 35 (40.23) | 2 (22.22) | 10 (34.48) |
|
| Skin adhesion, n
(%) |
|
|
|
| 0.389 |
|
Yes | 2 (22.22) | 22 (25.29) | 3 (33.33) | 12 (41.38) |
|
| No | 7 (77.78) | 65 (74.71) | 6 (66.67) | 17 (58.62) |
|
| Thick blood
vessels, n (%) |
|
|
|
| 0.978 |
|
Yes | 5 (55.56) | 49 (56.32) | 5 (55.56) | 15 (51.72) |
|
| No | 4 (44.44) | 38 (43.68) | 4 (44.44) | 14 (48.28) |
|
| Lymphatic
metastasis, n (%) |
|
|
|
| 0.435 |
|
Yes | 1 (11.11) | 31 (35.63) | 2 (22.22) | 10 (34.48) |
|
| No | 8 (88.89) | 56 (64.37) | 7 (77.78) | 19 (65.52) |
|
| Lymph node size, cm
(mean ± SD) | 2.2±0.00 | 1.4±0.79 | 1.2±0.28 | 2.01±0.59 | 0.001,
0.982a,
1.000b,
1.000c,
1.000d,
0.006e,
0.387f |
In addition, the lymph node size for luminal A,
luminal B, triple-negative and HER-2-overexpression subtypes was
2.2±0.00, 1.4±0.79, 1.2±0.28 and 2.01±0.59, respectively. The lymph
node size was significantly higher in the HER-2-overexpression
subtype compared with in the luminal B subtype and the differences
were statistically significant among the four groups (P<0.05;
Table II). But no significant
differences were found between these four groups in tumor size. In
summary, calcification score and lymph node size were revealed to
be significantly different in the four molecular subtypes of breast
cancer (Table II).
Subgroup analysis
To further analyze the clinical value of indices
determined by DBT for the diagnosis of breast cancer molecular
subtypes, the thresholds of indicators including tumor size,
calcification score and lymph node size were calculated. According
to the sixth edition of the breast cancer Tumor-Node-Metastasis
staging system published by the American Joint Committee on Cancer
(22), T1 stage tumors exhibit a
maximum diameter ≤2 cm and tumor size is associated with prognosis,
therefore 2 cm was selected in the present study as a cut-off value
for tumor size. Lu et al (23)
reported that a calcification score of 9 to 12 points indicates
malignant calcification, therefore 10 points was selected as the
cut-off value for calcification score in the present study. The
incidence rate of ≥1.5 cm lymph node size has been identified to be
significantly different from that of ≤1.5 cm lymph node size, which
was significantly different from that of 0.6–1.4 cm lymph node size
(24). Therefore, 15 mm was selected
as the cut-off value for lymph node size in the present study. The
analysis demonstrated that lymph node size and calcification score
exhibited statistically significant differences among the four
groups (P<0.05; Table III).
| Table III.Cut-off values of tumor size,
calcification score and lymph node size measured by digital breast
three-dimensional tomosynthesis for diagnosing breast cancer
molecular subtypes. |
Table III.
Cut-off values of tumor size,
calcification score and lymph node size measured by digital breast
three-dimensional tomosynthesis for diagnosing breast cancer
molecular subtypes.
| Characteristic | Luminal A
subtype | Luminal B
subtype | Triple- negative
subtype | HER-2-
overexpression subtype | χ2 | P-value |
|---|
| Tumor size, cm |
|
|
|
| 1.82 | 0.610 |
|
<2 | 3 (60.00) | 28 (38.36) | 2 (28.57) | 6 (30.00) |
|
|
| ≥2 | 2 (40.00) | 45 (61.64) | 5 (71.43) | 14 (70.00) |
|
|
| Calcification
score |
|
|
|
| 13.31 | 0.002,
1.000a,
1.000b,
0.038c,
1.000d,
<0.001e,
0.038f |
|
<10 | 4 (57.14) | 36 (56.25) | 4 (57.14) | 3 (13.64) |
|
|
|
≥10 | 3 (42.86) | 28 (43.75) | 3 (42.86) | 19 (86.36) |
|
|
| Lymph node size,
cm |
|
|
|
| 14.12 | <0.001,
0.300a,
0.333b,
1.000c,
1.000d,
0.001e,
0.045f |
|
<1.5 | 0 (0.00) | 21 (72.41) | 2 (100.00) | 1 (10.00) |
|
|
|
≥1.5 | 1 (100.00) | 8 (27.59) | 0 (0.00) | 9 (90.00) |
|
|
Discussion
Breast cancer is a clinically heterogeneous disease
with a varied clinical profile. The results of the present study
highlighted that diagnostic imaging features, including
calcification score and lymph node size, determined using DBT may
be used as assistant diagnostic markers of breast cancer molecular
subtypes. Existing histological classifications may not be fully
consistent with the clinical behavior of this disease (25). ER, PR, HER-2, EGFR and basal marker
expression status indicates the molecular subtype of breast cancer,
and may predict or influence the prognosis and response to hormonal
and targeted therapies (5). However,
there are a lack of non-invasive methods for the molecular
classification of breast cancer. On the basis of a previous study
that indicated that the sensitivity of breast cancer diagnosis
increases from 60% using traditional digital mammography to 82.9%
using DBT (16), the present study
investigated further the associations between breast cancer
molecular subtypes and DBT imaging characteristics, including tumor
margin, surrounding bright ring of tumor, vascular images and
calcification foci, lymph node size and associations with
surrounding glandular tissue. The aim of the present study was to
demonstrate that DBT may serve as a clinical diagnostic tool for
diagnosing molecular subtypes of breast cancer.
Immunohistochemistry may be used easily and widely
to classify molecular subtypes of breast tumors, and these subtypes
have been demonstrated to exhibit significant differences regarding
tumor size, histological grade, lymph node positivity and
lymphovascular emboli, which is important for treatment planning
and targeted therapy (26,27). In the present study, calcification
score and lymph node size were identified as indicators with
significant differences when compared between the four molecular
subtypes of breast cancer. Subgroup analysis based on tumor size,
calcification score and lymph node size revealed significant
differences in the distribution of patients with calcification
scores ≥10 and <10, and lymph node size ≥1.5 and <1.5 cm;
however, no significant differences were identified for tumor size
≥2 and <2 cm. In addition, DBT effectively detected the tumor
margin, surrounding bright ring of tumor, vascular images and
calcification foci, lymph node size and associations with
surrounding glandular tissue, which indicates that DBT may be used
as a diagnostic tool for the determination of breast cancer
molecular subtypes.
The present study identified that patients with
HER-2-overexpression subtype exhibited a larger tumor size and
higher calcification score compared with Luminal B subtype.
Additionally, the calcification score was significantly associated
with molecular subtypes of breast cancer. This was in accordance
with a number of previous studies, which have identified an
association between HER-2 expression and calcification. Yang and
Tse (28) reported that the
calcification rates of triple-negative, HER-2-positive and
ER-positive breast cancer, identified by breast X-ray photography
examination, were 15, 67 and 61%, respectively, which indicates
that the calcification rate is higher in patients with ER and HER-2
expression. Ko et al (29)
revealed that tumor mass or partial structural asymmetry, and not
fine calcification, were the most common signs in patients with
triple-negative breast cancer during X-ray examination. In
addition, Kim et al (30)
identified that the presence of calcification was significantly
higher in patients with an ER-negative subtype of breast cancer
compared with patients with HER-2 expression. The results of the
present study identified that the highest calcification score was
associated with HER-2-overexpressed breast cancer, which suggests
that evaluation of calcification score may be used to predict
molecular subtypes and prognosis. Notably, a threshold analysis of
calcification score was performed in the present study and
statistically significant differences were revealed among the four
groups when the threshold of calcification score was 10 points.
Furthermore, the present study identified that lymph
node size for the four molecular subtypes of breast cancer was
significantly different and lymph node size was significantly
associated with molecular subtypes. Statistically significant
differences between different subtypes were revealed when the
threshold of lymph node size was 1.5 cm. When certain cases could
not be observed through the MLO view, lymph nodes were also
observed by magnification mammography (data not shown); however,
the lymph node could generally only be observed by MLO view. It has
been suggested that the ratio of metastatic to dissected lymph
nodes, termed the lymph node ratio (LNR), can be used as a superior
prognostic factor with a high sensitivity for evaluating lymph
nodes (31). In a previous study,
among 640 early breast cancer cases, data collected from 469 cases
with axillary lymph node metastasis were retrospectively analyzed
(31). The LNR in luminal A, luminal
B HER-2+, HER-2-overexpression and basal-like subtypes
was 35.2, 43.2, 46.9 and 39.1%, respectively. A significant
difference was identified between subtypes luminal A and
HER-2-overexpression (P=0.023). LNR was significantly associated
with tumor size and lymphovascular invasion; however, no
significant association was observed for other prognostic factors,
including menopausal status, laterality, grade and perineural
invasion. When the cut-off value was defined as 29.8% for LNR,
significant differences in survival rates were identified between
basal-like type and both luminal A (P=0.003) and luminal B
HER-2+ (P=0.04) subtypes. In summary, the LNR was
different in certain molecular subtypes of breast cancer and was
associated with prognostic indicators and survival. These results
support the use of LNR to evaluate breast cancer (31). In the present study, the imaging
characteristics detected by DBT, including tumor margin,
surrounding bright ring of tumor, vascular images and associations
with surrounding glandular tissue were not markedly different in
different molecular subtypes of breast cancer.
The present study was retrospective with a limited
sample size, therefore the individuals in each subtype were not
particularly uniform. Future studies should increase the sample
size and perform receiver operator characteristic analysis to
calculate the sensitivity and specificity of each indicator. In
addition, this may detect more characteristics associated with
different molecular subtypes, which may promote pre-operative
clinical judgment and personalized treatment strategies.
Furthermore, calcifications are a common sign of invasive ductal
carcinoma with ductal carcinoma in situ, therefore future
studies may focus on the associations between imaging features of
DBT and pathological subtypes of breast cancer.
In conclusion, the results of the present study
suggest that diagnostic imaging features determined using DBT,
including calcification score and lymph node size, are
significantly associated with molecular subtypes of breast cancer
and may be used as assistant diagnostic markers of molecular
subtypes of breast cancer.
Acknowledgements
Not applicable.
Funding
Not applicable.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
SC designed the study. MY performed data analysis,
drafted the manuscript and revised the manuscript. DC, JY, MH, LY
and HH made contributions to data acquisition, analysis and
interpretation.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of The Second Clinical College of Fujian Medical
University and each patient involved in the study provided written
informed consent.
Patient consent for publication
Patients provided written informed consent for the
publication of their data.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Hortobagyi GN, de la Garza Salazar J,
Pritchard K, Amadori D, Haidinger R, Hudis CA, Khaled H, Liu MC,
Martin M, Namer M, et al: The global breast cancer burden:
Variations in epidemiology and survival. Clin Breast Cancer.
6:391–401. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tao Z, Shi A, Lu C, Song T, Zhang Z and
Zhao J: Breast cancer: Epidemiology and etiology. Cell Biochem
Biophys. 72:333–338. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Perou CM, Sørlie T, Eisen MB, van de Rijn
M, Jeffrey SS, Rees CA, Pollack JR, Ross DT, Johnsen H, Akslen LA,
et al: Molecular portraits of human breast tumours. Nature.
406:747–752. 2000. View
Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sørlie T, Perou CM, Tibshirani R, Aas T,
Geisler S, Johnsen H, Hastie T, Eisen MB, van de Rijn M, Jeffrey
SS, et al: Gene expression patterns of breast carcinomas
distinguish tumor subclasses with clinical implications. Proc Natl
Acad Sci USA. 98:10869–10874. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Carey LA, Perou CM, Livasy CA, Dressler
LG, Cowan D, Conway K, Karaca G, Troester MA, Tse CK, Edmiston S,
et al: Race, breast cancer subtypes, and survival in the Carolina
breast cancer study. JAMA. 295:2492–2502. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Li X, Huang Y, Shuqin Z, Chen Z and Zhang
S: Re: Association between imaging characteristics and different
molecular subtypes of breast cancer. Acad Radiol. 24:11842017.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Eroles P, Bosch A, Pérez-Fidalgo JA and
Lluch A: Molecular biology in breast cancer: Intrinsic subtypes and
signaling pathways. Cancer Treat Rev. 38:698–707. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Liedtke C and Kiesel L: Breast cancer
molecular subtypes-modern therapeutic concepts for targeted therapy
of a heterogeneous entity. Maturitas. 73:288–294. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Di Gioia D, Stieber P, Schmidt GP, Nagel
D, Heinemann V and Baur-Melnyk A: Early detection of metastatic
disease in asymptomatic breast cancer patients with whole-body
imaging and defined tumour marker increase. Br J Cancer.
112:809–818. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zelig U, Barlev E, Bar O, Gross I, Flomen
F, Mordechai S, Kapelushnik J, Nathan I, Kashtan H, Wasserberg N
and Madhala-Givon O: Early detection of breast cancer using total
biochemical analysis of peripheral blood components: A preliminary
study. BMC Cancer. 15:4082015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Rao M, Stough J, Chi YY, Muller K, Tracton
G, Pizer SM and Chaney EL: Comparison of human and automatic
segmentations of kidneys from CT images. Int J Radiat Oncol Biol
Phys. 61:954–960. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Takamoto Y, Tsunoda H, Kikuchi M, Hayashi
N, Honda S, Koyama T, Ohde S, Yagata H, Yoshida A and Yamauchi H:
Role of breast tomosynthesis in diagnosis of breast cancer for
Japanese women. Asian Pac J Cancer Prev. 14:3037–3040. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Roth RG, Maidment AD, Weinstein SP, Roth
SO and Conant EF: Digital breast tomosynthesis: Lessons learned
from early clinical implementation. Radiographics. 34:E89–E102.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Tang W, Li R, Gao Y, Wang Q, Shen Q, Gu Y
and Peng W: A comparative study of diagnostic performance between
digital breast tomosynthesis and conventional imaging methods.
China Oncol. 27:487–495. 2017.
|
|
15
|
Mariscotti G, Houssami N, Durando M,
Campanino PP, Regini E, Fornari A, Bussone R, Castellano I, Sapino
A, Fonio P and Gandini G: Digital breast tomosynthesis (DBT) to
characterize MRI-detected additional lesions unidentified at
targeted ultrasound in newly diagnosed breast cancer patients. Eur
Radiol. 25:2673–2681. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cai SQ, Yan JX, Chen QS, Huang ML and Cai
DL: Significance and application of digital breast tomosynthesis
for the BI-RADS classification of breast cancer. Asian Pac J Cancer
Prev. 16:4109–4114. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wiechmann L, Sampson M, Stempel M, Jacks
LM, Patil SM, King T and Morrow M: Presenting features of breast
cancer differ by molecular subtype. Ann Surg Oncol. 16:2705–2710.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cen D, Xu L, Li N, Chen Z, Wang L, Zhou S,
Xu B, Liu Cl, Liu Z and Luo T: BI-RADS 3–5 microcalcifications can
preoperatively predict breast cancer HER2 and Luminal a molecular
subtype. Oncotarget. 8:13855–13862. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Pan B, Yao R, Zhou YD, Zhu QL, Shi J, Xu
QQ, Wang CJ, You SS, Mao F, Lin Y, et al: Tumor biology,
clinicopathological characteristics and prognosis of screen
detected T1 invasive non-palpable breast cancer in asymptomatic
Chinese women (2001–2014). Oncotarget. 8:26221–26230.
2017.PubMed/NCBI
|
|
20
|
Partyka L, Lourenco AP and Mainiero MB:
Detection of mammographically occult architectural distortion on
digital breast tomosynthesis screening: Initial clinical
experience. AJR Am J Roentgenol. 203:216–222. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sickles EA, D'Orsi CJ, Bassett LW, et al:
ACR BI-RADS®Mammography. In: ACR
BI-RADS®Atlas, Breast Imaging Report and Date System.
American College of Radiology; Reston, VA: pp. 15–75. 2013
|
|
22
|
Wang W, Bai YH, Deng YM, et al:
Stsage-specific Survival Analysis according to the 2002 American
Joint Committee on breast cancer staging system. Pract J Cancer.
22:286–289. 2007.(in Chinese).
|
|
23
|
Lu J, Ni C and Wu D: Breast benign and
malignant calcification score and clinical application. Chin J Med
Imaging. 385–387. 2008.
|
|
24
|
Shaolin L, Jun L, Licong F, Peikun Z and
Han L: Correlation between size and metastasis of mediastinal lymph
nodes in lung cancer by CT examination. Qilu Tumor J. 75:1998.
|
|
25
|
Goldhirsch A, Winer EP, Coates AS, Gelber
RD, Piccart-Gebhart M, Thürlimann B and Senn HJ; Panel Members:
Personalizing the treatment of women with early breast cancer:
Highlights of the St gallen international expert consensus on the
primary therapy of early breast cancer 2013. Ann Oncol.
24:2206–2223. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kumar N, Patni P, Agarwal A, Khan MA and
Parashar N: Prevalence of molecular subtypes of invasive breast
cancer: A retrospective study. Med J Armed Forces India.
71:254–258. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bennis S, Abbass F, Akasbi Y, Znati K,
Joutei KA, El Mesbahi O and Amarti A: Prevalence of molecular
subtypes and prognosis of invasive breast cancer in north-east of
Morocco: Retrospective study. BMC Res Notes. 5:4362012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yang WT and Tse GM: Sonographic,
mammographic, and histopathologic correlation of symptomatic ductal
carcinoma in situ. AJR Am J Roentgenol. 182:101–110. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ko ES, Lee BH, Kim HA, Noh WC, Kim MS and
Lee SA: Triple-negative breast cancer: Correlation between imaging
and pathological findings. Eur Radiol. 20:1111–1117. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kim SH, Seo BK, Lee J, Kim SJ, Cho KR, Lee
KY, Je BK, Kim HY, Kim YS and Lee JH: Correlation of ultrasound
findings with histology, tumor grade, and biological markers in
breast cancer. Acta Oncol. 47:1531–1538. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Demircioglu F, Demirci U, Kilic D, Ozkan S
and Karahacioglu E: Clinical significance of lymph node ratio in
locally advanced breast cancer molecular subtypes. Onkologie.
36:637–640. 2013. View Article : Google Scholar : PubMed/NCBI
|