Introduction
Mismatch repair (MMR) deficiency (dMMR) has been
used as a predictive biomarker to guide the clinical application of
immune checkpoint inhibitor (ICI) therapy (1–3). dMMR
mainly results from germline mutations and epigenetic alterations
in any of the MMR genes, including MutL homologue 1 (MLH1),
MutS protein homologue 2 (MSH2), MutS homologue 6
(MSH6) and PMS1 homologue 2 (PMS2) (4). In addition, dMMR can be caused by
deletions in the epithelial cell adhesion molecule (EPCAM)
gene, which leads to the inhibition of MSH2 gene expression
via promoter methylation (5). A
previous study has reported that patients with cancer combined with
dMMR and/or high microsatellite instability (MSI-H), who had no
apparent germline mutations or MLH1 promoter hypermethylation,
acquired somatic mutations in MMR genes, leading to a hypermutated
tumor phenotype (6). Accumulating
evidence supports the use of tumor mutational burden (TMB) as a
biomarker for predicting the therapeutic response in patients with
advanced cancer receiving ICIs, including antibodies that target
cytotoxic T lymphocyte antigen 4 (CTLA-4) or programmed death
1/programmed death ligand 1 (PD-1/PD-L1) (7–10). TMB
is associated with the production of new antigens, which may
trigger antitumor immunity (11–13). A
number of panels created based on targeted sequencing technology,
such as the Memorial Sloan Kettering-Integrated Mutation Profiling
of Actionable Cancer Targets (MSK-IMPACT) panel, have been approved
by the US Food and Drug Administration (FDA) for the clinical
evaluation of TMB (14,15).
Hypermutation ability is an important feature of
tumor development that may lead to the production of new antigens,
which may be the result of functional defects in DNA repair,
including that of dMMR (16,17). Thus, it may be hypothesized that
somatic mutations in genes associated with MMR may in turn affect
MMR function, which may be of the underlying causes of the
therapeutic effects exhibited by ICIs, making it a potential
prognostic biomarker of ICI treatment. The Memorial Sloan Kettering
Cancer Center (MSKCC) have disclosed their mutation data obtained
from 1,661 patients with advanced cancer who received ICI treatment
obtained by next generation sequencing (8), which are publicly available on the
cBioPortal database. In the present study, these data were obtained
with the aim of analyzing the prognostic value of somatic
mutationsin genes involved in MMR in 1,661 patients with advanced
cancer treated with ICIs; the potential association between somatic
mutations in the MMR genes and TMB were also investigated.
Materials and methods
Data retrieval
Information regarding somatic mutations in genes
associated with MMR and survival time in patients with advanced
cancer who were treated with ICIs was downloaded from The Cancer
Genome Atlas Database, an open access database that is publicly
available at http://www.cbioportal.org (18,19). The
MSK-IMPACT Clinical Sequencing Cohort (https://www.cbioportal.org/study/summary?id=tmb_mskcc_2018)
was selected as the data source, containing only patients with
advanced cancer who were administered with ICIs (8), and the number of samples was 1,661.
Only data including mutations was obtained. The queried targeted
genes included 4 main genes associated with MMR: MLH1, MSH2,
MSH6 and PMS2. Genomic and survival data from 1,661
patients with various types of cancer sequenced using the
MSK-IMPACT assay were subsequently downloaded from the cBioPortal
website after submitting the query' MLH1, MSH2, MSH6 and
PMS2' in the input box. In total, 1,661 pieces of mutation
and survival data, each containing the mutation status of the MMR
genes, survival time and the status of patient (deceased or
censored), were downloaded and analyzed. The TMB score was defined
as the total number of nonsynonymous mutations in the somatic
coding region which was normalized to the total number of megabases
sequenced.
Statistical analysis
Statistical analyses were performed using the SPSS
(version 17.0; SPSS, Inc.) and GraphPad Prism 7 (GraphPad Software,
Inc.) software. The survival curves were produced using the
Kaplan-Meier method and compared using log-rank tests. Overall
survival (OS) data was obtained from the cBioPortal website. The
definition of OS was the time between the date of first ICI
treatment and the time of death or last follow-up visit (8). Hazard ratios of somatic mutations in
the MMR genes for overall survival following adjustments for other
prognostic factors was assessed using Cox proportional hazards
regression. Unpaired t-test or one-way analysis of variance (ANOVA)
was used for comparing the TMB scores between different groups, and
the TMB scores were expressed as the mean ± SD. All P-values were
two-sided. P<0.05 was considered to indicate a statistically
significant difference.
Results
Somatic mutation analysis of genes
associated with MMR
The genomic profiles of four MMR genes, specifically
MLH1, MSH2, MSH6 and PMS2, in 1,661 patients were
queried. Patients with any form of somatic mutations in these genes
were assigned to the MMR mutation group. The queried genes were
identified to be altered in 114 of the 1,661 patients; the total
somatic mutation frequency of the MMR genes among all patients was
7%. Variations were observed in the somatic mutation frequencies of
the MMR genes among different types of tumors (Table I). Only patients with colorectal
cancer possessed >20% somatic mutations. Tumors with somatic
mutation frequencies of >7% included melanoma and cancer of
unknown origin. Of note, patients with melanoma and somatic
mutations in MMR exhibited superior survival benefits following ICI
treatment in the present study.
 | Table I.Total somatic mutation frequency of
MMR genes across different types of tumors. |
Table I.
Total somatic mutation frequency of
MMR genes across different types of tumors.
| Type | CC | CUP | M | BLC | NSCLC | HNC | Glioma | EC | BC | RCC | SCNM |
|---|
| Mutation frequency,
% | 21.82 | 7.95 | 7.5 | 6.98 | 4.86 | 6.47 | 5.13 | 4.76 | 4.54 | 1.99 | 100 |
Prognostic value of somatic mutations
in the MMR genes in patients with metastatic cancer following ICI
treatment
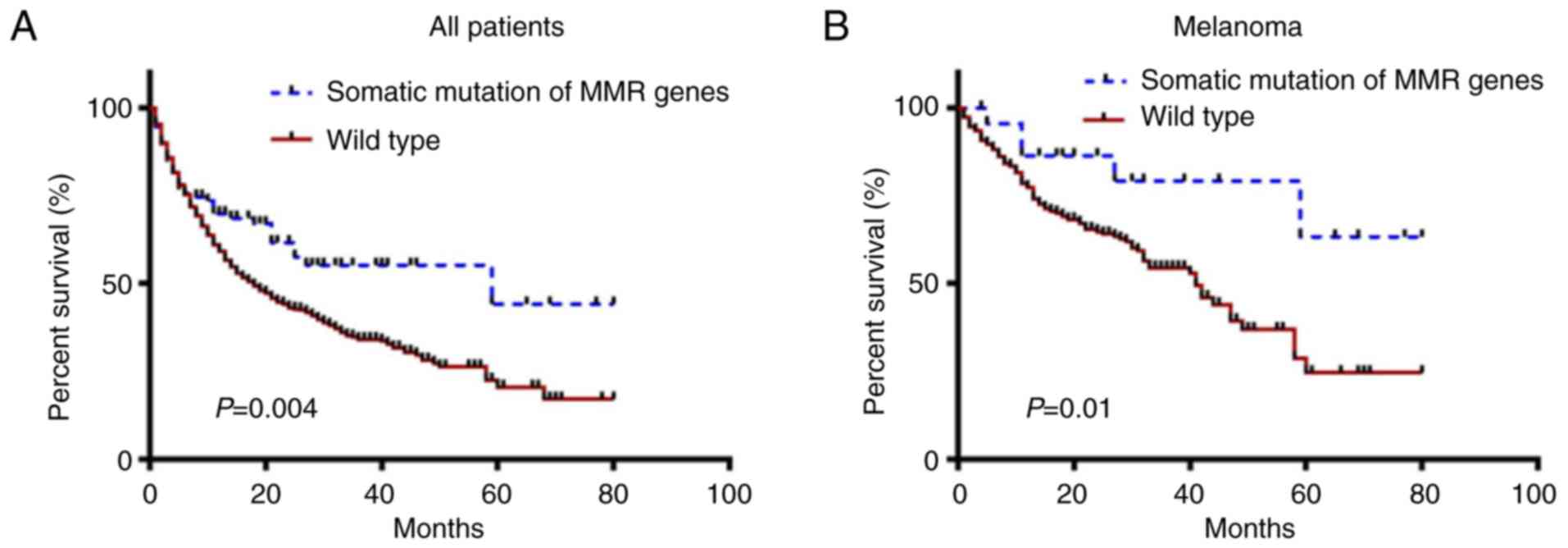
The prognostic value of somatic mutations in genes
associated with MMR was first determined. Kaplan-Meier survival
curves indicated that MMR gene mutation was a positive prognostic
factor for OS. The median OS times for patients with MMR gene
mutations and those in the wild-type group were 59.0 and 17.0
months, respectively (P=0.004; Fig.
1A), and the hazard ratio (HR) was 0.637 (95% CI, 0.491-0.827),
which was less than 1.0. Since mutations in the MMR genes include
deleterious variants, variants of unknown significance and benign
variants, the survival time in 114 cases were analyzed further; the
Kaplan-Meier survival curve demonstrated that there was no
significant difference in the OS time among the three types of
mutations (P=0.727; data not shown).
The prognostic value of somatic mutations in the MMR
genes in different types of tumors was next analyzed. Mutations in
the MMR genes were significantly associated with prolonged survival
in patients with melanoma (P=0.010; Fig.
1B). In patients with colorectal and bladder cancer, the
associations were not statistically significant, although the HRs
were 0.608 (95% CI, 0.294-1.256) and 0.578 (95% CI, 0.271-1.235),
respectively (data not shown).
To confirm the prognostic value of somatic mutations
in genes associated with MMR in patients treated with ICIs, Cox
proportional hazards regression analysis was performed. The
presence of somatic mutations in the MMR genes was demonstrated to
be significantly associated with OS following adjustment for age,
sex, ICI treatment and tumor type (Table II).
| Table II.Hazard ratios for overall survival
analysis. |
Table II.
Hazard ratios for overall survival
analysis.
| Variable | HR | 95% CI | P-value |
|---|
| Mutation status of
MMR genes |
|
Wild-type (reference) | 1 |
|
|
|
Mutation | 0.683 | 0.497-0.938 | 0.018a |
| Treatment |
|
| 0.001a |
| CTLA-4
(reference) | 1 |
|
|
|
PD-1/PDL-1 | 1.423 | 0.999-2.025 | 0.050 |
|
Combination | 1.528 | 1.219-1.914 |
<0.001a |
| Age |
|
| 0.035a |
|
<30 | 1 |
|
|
|
31-50 | 0.871 | 0.582-1.304 | 0.502 |
|
51-60 | 0.648 | 0.435-0.966 | 0.033a |
|
61-70 | 0.708 | 0.476-1.052 | 0.087 |
|
>71 | 0.725 | 0.484-1.087 | 0.120 |
| Tumor type |
|
|
<0.001a |
| Other
(reference) | 1 |
|
|
| Bladder
cancer | 0.901 | 0.628-1.294 | 0.574 |
|
Colorectal cancer | 0.575 | 0.427-0.774 |
<0.001a |
|
Melanoma | 1.305 | 1.025-1.661 | 0.031a |
|
Non-small lung cancer | 1.078 | 0.854-1.361 | 0.529 |
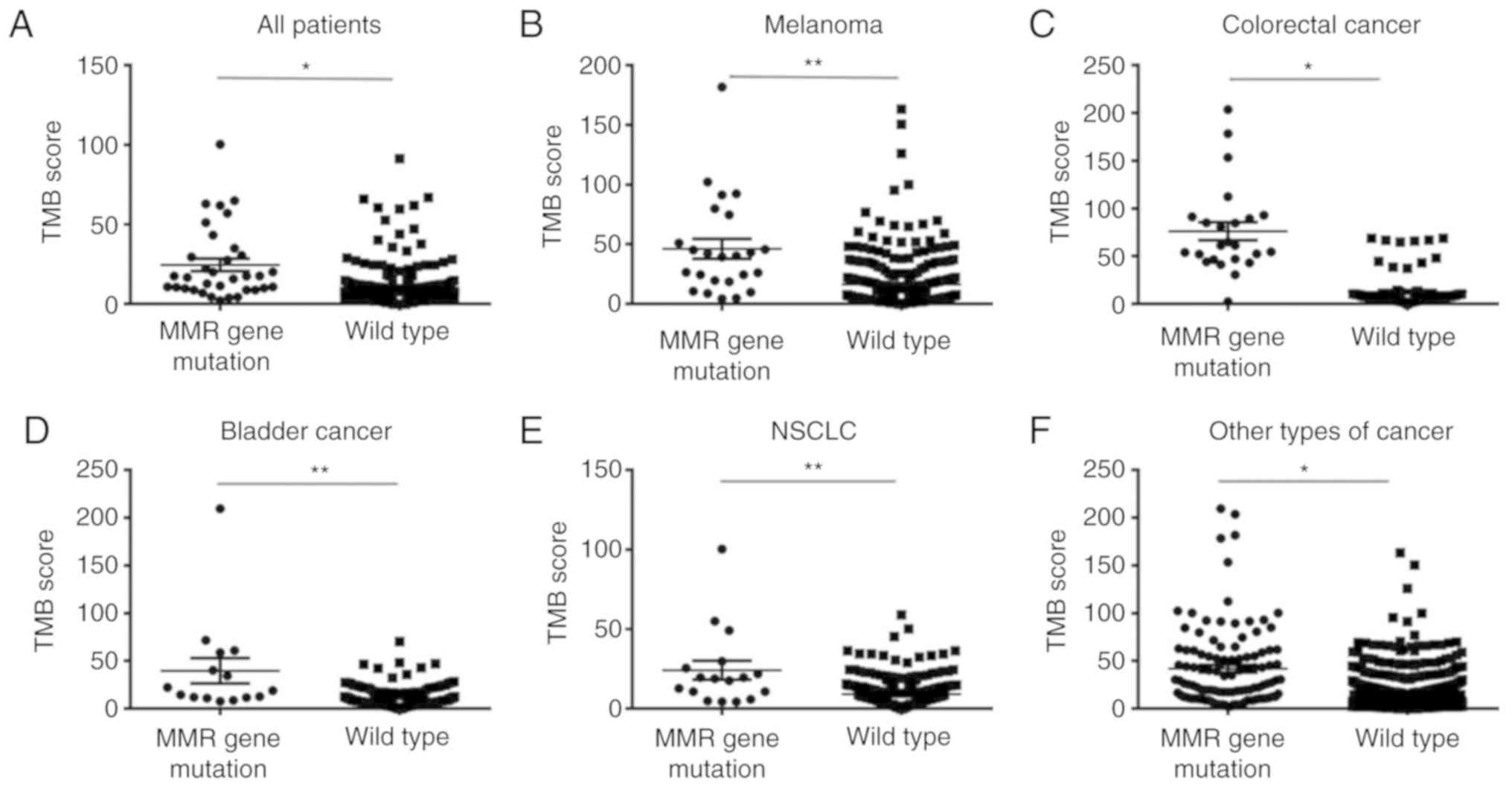
Association between somatic mutations
in the MMR genes and TMB score
To verify whether the presence of somatic mutations
in MMR genes may affect tumor mutation load, analysis of TMB scores
in groups of patients with different mutation status of the MMR
genes was performed. Among all 1,661 patients, the TMB score in the
MMR gene mutation group was significantly higher compared with that
in the wild-type MMR gene group (P<0.0001; Fig. 2A). In the 114 patients with MMR gene
mutations, the difference in the TMB scores among the three types
of variants were not significant (F=0.6028; P=0.5490) (one-way
ANOVA; data not shown). Following stratification by type of cancer,
the association between TMB score and MMR mutation status remained
significant, and the TMB scores were higher in patients with MMR
mutations, including melanoma (t=3.542; P=0.0017), non-small cell
lung cancer (t=2.550, P=0.0230), colorectal cancer (t=6.533;
P<0.0001), bladder cancer (t=2.155, P=0.0490) and other types of
cancer (t=8.080; P<0.0001) (Fig.
2B-F). The other types of cancer included renal cell carcinoma,
head and neck cancer, esophagogastric cancer, glioma and cancer of
unknown primary origin; somatic mutations in the MMR genes were
infrequent in these types of tumors, the data from these patients
were combined for this analysis.
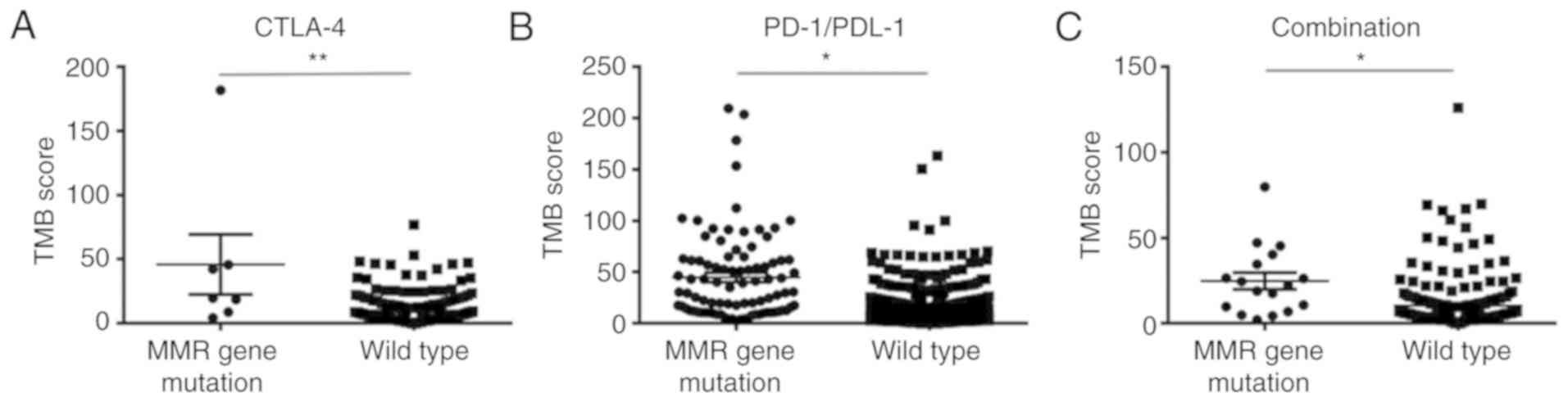
The association between somatic mutations in MMR
genes and TMB score in patients treated with different types of ICI
was subsequently analyzed. The TMB scores were significantly higher
in patients with MMR mutations treated with the CTLA-4 inhibitor
(P=0.0039), PD-1/PD-L1 inhibitor (P<0.0001) and a combination of
the two drugs (P=0.0096) compared with those in the corresponding
wild-type groups (Fig. 3).
Co-mutation analysis of the MMR genes
and other genes with the highest frequency
To clarify the reasons for the presence of somatic
mutations in the MMR genesis associating with TMB, the profiles of
genes with the high frequency of mutations alongside those of MMR
were screened. A total of 286 genes were identified to be
significantly co-mutated with somatic mutations in the MMR genes.
Compared with those in the wild-type group, the top 10 gene
mutation frequencies in the MMR gene mutation group were
significantly increased (Table
III).
| Table III.Top 10 genes with the highest
frequency between the MMR gene mutation and wild-type groups. |
Table III.
Top 10 genes with the highest
frequency between the MMR gene mutation and wild-type groups.
|
| Mutation frequency,
% |
|
|---|
|
|
|
|
|---|
| Gene | MMR mutation | MMR wild-type | P-value |
|---|
| KMT2D | 50.00 | 11.57 |
1.50×10−21 |
| NOTCH1 | 31.58 | 4.85 |
1.88×10−17 |
| CREBBP | 28.95 | 4.72 |
2.39×10−15 |
| RNF43 | 21.05 | 2.33 |
5.23×10−14 |
| NOTCH3 | 25.44 | 4.14 |
1.68×10−13 |
| KMT2C | 33.33 | 8.08 |
4.16×10−13 |
| ARID1B | 23.68 | 3.62 |
4.27×10−13 |
| ARID1A | 35.96 | 9.63 |
5.92×10−13 |
| PTPRS | 22.81 | 3.36 |
6.55×10−13 |
| GLI1 | 23.40 | 2.83 |
1.64×10−12 |
Discussion
The application of ICIs has been beneficial to the
survival of patients with tumors of certain molecular phenotypes,
including tumors with MMR or a high TMB. Compared with patients
with advanced cancer with a low TMB, a retrospective large-sample
clinical study from the MSKCC has confirmed that patients with a
high TMB were more likely to benefit from ICI treatment (8). In the present study, to clarify whether
somatic mutations in the MMR genes may be applied as a prognostic
marker for patients receiving ICI treatment, relevant clinical and
genomic data from the same cohort of patients treated with ICI were
downloaded from the cBioPortal database. The association between
the presence of somatic mutations in MMR genes and OS was analyzed,
and the results demonstrated that somatic MMR gene mutations were
significantly associated with improved OS in all patients with
cancer, especially those with melanoma, compared with those with
wild-type MMR genes. In addition, the TMB score was also found to
be significantly higher in patients with MMR gene mutations
compared with that in patients without MMR gene mutations. Somatic
mutations in the MMR genes include three types of mutation
variants, which are deleterious variants, variants of unknown
significance and benign variants. It was demonstrated that there
was no significant difference in the total survival times and the
TMB scores among the three types of mutation variants.
The MMR system is mainly composed of four specific
DNA MMR enzymes encoded by MLH1, PMS2, MSH2 and MSH6,
the main function of which is to identify and repair mismatched
bases during DNA replication. dMMR leads to microsatellite
instability, susceptibility to cancer, accumulation of mutation
burden of cancer-associated genes and the production of
neoantigens, thus increasing the antitumor immune response. dMMR
has been used as a potential biomarker inpredicting the responses
of patients with solid tumors to ICIs, irrespective of cancer type
(2,20). dMMR mainly result from germline
mutations, transcriptional inactivation of the aforementioned MMR
genes through epigenetic alterations (21,22),
deletions in the EPCAM gene, leading to the constitutive
repression of MSH2 expression by promoter methylation
(5), or inflammation-mediated
transcriptional repression (23).
FDA has approved the use of a PD-1 antibody for the treatment of
adult and pediatric patients with unresectable or metastatic solid
tumors with MSI-H or dMMR (1). Since
mutations in the MLH1, MSH2, MSH6 and PMS2 genes
appear to be the main causes of functional defects in MMR proteins
(20), these four genes were
selected for analysis in the present study. As showed in Table I, patients with colorectal cancer
possessed >20% somatic mutations. Tumors with somatic mutation
frequencies of >7% included melanoma and cancer of unknown
origin. Of note, patients with somatic mutations of MMR in melanoma
exhibited superior survival benefits following ICI treatment in the
present study.
A previous study reported that although a number of
patients with tumors with dMMR did not harbor germline mutations in
the MMR genes, ~70% of them had somatic mutations in genes
associated with the MMR genes (6),
suggesting this to be a potential cause of MSI-H or high TMB.
Therefore, it may be hypothesized that somatic mutations in the MMR
genes may serve as a novel prognostic biomarker for the outcome of
ICI treatment. The present study demonstrated that the occurrence
of somatic mutations in the MMR genes had a similar effect as TMB
predicting the outcome of ICI treatment; it was not only associated
with longer OS times in all patients treated with ICIs, but also in
those with melanoma. Cox proportional hazards regression analysis
revealed that somatic mutations in the MMR genes may serve as a
prognostic indictor for longer OS in patients with cancer following
ICI treatment. In addition to dMMR, MSI-H and high TMB scores being
good predictors of ICI efficacy, the association between somatic
mutations in genes associated with MMR and ICI efficacy may provide
a new method for exploring the mechanism underlying the effects of
dMMR on the efficacy of ICIs.
Somatic mutations in the MMR genes may be partly
caused by dMMR due to the mismatched genes not being repaired in
time, in turn increasing the TMB and tumor immunogenicity (6). The results of the present study
demonstrated that somatic mutations in the MMR genes were
associated with the TMB score. Following analysis of the entire
cohort or in the stratified categories of patients with tumors
treated with ICIs, the TMB score was revealed to be significantly
higher in the group with MMR gene mutations compared with that in
the wild-type group. This association remained significant in the
different ICI treatment groups, suggesting that somatic mutations
in the MMR genes may serve as a prognostic marker for the ICI
treatments.
In addition to MMR, other types of DNA damage
repair/response are also important for maintaining genomic
integrity under normal cellular conditions (24). Failure to repair DNA damage can also
result in a variety of genomic aberrations, leading to increased
mutational load and neoantigen burden (25). However, this was beyond the scope of
the present study and requires further analysis.
In the present study, a total of 286 genes were
identified to be co-mutated with the MMR genes, which may be the
result of dMMR. These co-mutations may be the underlying cause of
the effects of MMR gene mutations on the TMB score. New antigens
may be produced from the genetic mutations, which need to be
further verified (11,26). In the present study, the top 10 genes
with the highest frequencies of mutation associated with MMR gene
mutations have been listed in Table
III. Histone-lysine N-methyltransferase 2D (KMT2D), belonging
to a family of mammalian histone H3 lysine 4 (H3K4)
methyltransferases, is frequently mutated in developmental
diseases, such as in various forms of cancer (27). A study showed that ARID1A (the
AT-rich interaction domain 1A, also known as BAF250a), KMT2D and
SOX9 is sufficient to detect mismatch repair-deficient colorectal
adenocarcinomas with 76% sensitivity and 98% specificity (28). ARID1A is one of the most commonly
mutated genes in cancer, and its deficiency is correlated with
microsatellite instability and increased mutation load across
multiple human cancer types (29).
Notch1 inhibition reduces immune-suppressive cells. The inhibition
of Notch1 improves the antitumor activity of nivolumab and
ipilimumab, particularly when given in combination (30). One gene implicated in ALL relapse
encodes cyclic adenosine monophosphate (cAMP) response element
binding protein (CREB) binding protein (CREBBP/CBP), a member of
the KAT3 family of histone acetyltransferases (HAT). CREBBP
knockdown enhances RAS/RAF/MEK/ERK signaling in Ras pathway mutated
acute lymphoblastic leukemia but does not modulate chemotherapeutic
response (31). Mutation of ARID1A
and CREBBP may be poor prognostic factors for follicular lymphoma
receiving immunochemotherapy (32).
Genomic alteration frequency of ring finger protein 43 (RNF43) are
higher in PD-L1-positive patients with biliary tract cancer (BTC)
compared with PD-L1-negative patients, which suggest that mutation
status of RNF43 may be a poor prognostic factor for BTC receiving
immunotherapy (33). Treg cell
expansion requires Notch3 signaling, which imply that the mutation
status of Notch3 may affect the function of Treg cells (34). NOTCH1/2 and KMT2C/D were the most
frequently mutated genes in recurrent or metastatic skin squamous
cell cancer (35). PTPRS, a
receptor-type protein tyrosine phosphatase, appears to regulate RAS
pathway activation through ERK. Native mutations in PTPRS, may
reduce its phosphatase activity while increasing ERK activation and
downstream transcriptional signaling (36). Glioma oncogene homolog 1 (GLI1) is an
oncogenic transcription factor playing important roles in cancer.
Patients with GLI1 activation and breast tumors had worse
metastasis-free survival compared with those with low levels
(37). The association between the
aforementioned gene variants and the efficacy of immunologic
checkpoint inhibitors is not clear and needs to be further
verified. However, the role of these mutated genes in MMR and the
possible underlying mechanisms in regulating the efficacy of ICIs
remain to be fully elucidated.
In the present study, the effects of chemotherapy
and radiotherapy on the dMMR involvement in predicting the efficacy
of ICIs were not examined. The majority of patients with advanced
cancer receive multiple courses of radiotherapy and chemotherapy,
which may affect the increase in TMB and the efficacy of ICIs; this
requires further exploration.
In a conclusion, the results of the present study
suggested that somatic mutations in the MMR genes may be used as a
prognostic marker of a positive outcome in patients with metastatic
cancer receiving ICI treatment; since somatic mutations in the MMR
genes may be one of the main factors affecting the tumor mutation
load.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Science and
Technology Planning Project of Changzhou, Jiangsu Province (grant
no. CE20165052), the Changzhou Health Bureau Project (grant no.
ZD201616), the Jiangsu Province Health Department Project (grant
no. Z201616), the 333 Talents Training Project of Jiangsu Province
(grant nos. 2016 III-0727 and BRA2017114) and the Talents Training
Project for Key Medical Innovation of Changzhou (grant no.
2016CZLJ021).
Availability of data and materials
The datasets generated and/or analyzed during the
present study are available in The Cancer Genome Atlas database, an
open access database that is publicly available at http://www.cbioportal.org.
Authors' contributions
YPL conceived the study and wrote the manuscript. YL
participated in the study design. LC and SLZ analyzed and
interpreted a part of the data. YMS interpreted part of the data.
QFQ, MZ and YP analyzed a part of the data. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Lemery S, Keegan P and Pazdur R: First FDA
approval agnostic of cancer site-when a biomarker defines the
indication. N Engl J Med. 377:1409–1412. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Le DT, Uram JN, Wang H, Bartlett BR,
Kemberling H, Eyring AD, Skora AD, Luber BS, Azad NS, Laheru D, et
al: PD-1 Blockade in tumors with mismatch-repair deficiency. N Engl
J Med. 372:2509–2520. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Le DT, Durham JN, Smith KN, Wang H,
Bartlett BR, Aulakh LK, Lu S, Kemberling H, Wilt C, Luber BS, et
al: Mismatch repair deficiency predicts response of solid tumors to
PD-1 blockade. Science. 357:409–413. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mills AM, Liou S, Ford JM, Berek JS, Pai
RK and Longacre TA: Lynch syndrome screening should be considered
for all patients with newly diagnosed endometrial cancer. Am J Surg
Pathol. 38:1501–1509. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Giardiello FM, Allen JI, Axilbund JE,
Boland CR, Burke CA, Burt RW, Church JM, Dominitz JA, Johnson DA,
Kaltenbach T, et al: Guidelines on genetic evaluation and
management of Lynch syndrome: A consensus statement by the US
Multi-society task force on colorectal cancer. Am J Gastroenterol.
109:1159–1179. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Haraldsdottir S, Hampel H, Tomsic J,
Frankel WL, Pearlman R, de la Chapelle A and Pritchard CC: Colon
and endometrial cancers with mismatch repair deficiency can arise
from somatic, rather than germline, mutations. Gastroenterology.
147:1308–1316.e1. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wang F, Wei XL, Wang FH, Xu N, Shen L, Dai
GH, Yuan XL, Chen Y, Yang SJ, Shi JH, et al: Safety, efficacy and
tumor mutational burden as a biomarker of overall survival benefit
in chemo-refractory gastric cancer treated with toripalimab, a PD-1
antibody in phase Ib/II clinical trial NCT02915432. Ann Oncol.
30:1479–1486. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Samstein RM, Lee CH, Shoushtari AN,
Hellmann MD, Shen R, Janjigian YY, Barron DA, Zehir A, Jordan EJ,
Omuro A, et al: Tumor mutational load predicts survival after
immunotherapy across multiple cancer types. Nat Genet. 51:202–206.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hellmann MD, Ciuleanu TE, Pluzanski A, Lee
JS, Otterson GA, Audigier-Valette C, Minenza E, Linardou H, Burgers
S, Salman P, et al: Nivolumab plus ipilimumab in lung cancer with a
high tumor mutational burden. N Engl J Med. 378:2093–2104. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yi M, Jiao D, Xu H, Liu Q, Zhao W, Han X
and Wu K: Biomarkers for predicting efficacy of PD-1/PD-L1
inhibitors. Mol Cancer. 17:1292018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gubin MM, Artyomov MN, Mardis ER and
Schreiber RD: Tumor neoantigens: Building a framework for
personalized cancer immunotherapy. J Clin Invest. 125:3413–3421.
2015. View
Article : Google Scholar : PubMed/NCBI
|
|
12
|
Schumacher TN, Kesmir C and van Buuren MM:
Biomarkers in cancer immunotherapy. Cancer Cell. 27:12–14. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Grizzi G, Caccese M, Gkountakos A,
Carbognin L, Tortora G, Bria E and Pilotto S: Putative predictors
of efficacy for immune checkpoint inhibitors in non-small-cell lung
cancer: Facing the complexity of the immune system. Expert Rev Mol
Diagn. 17:1055–1069. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zehir A, Benayed R, Shah RH, Syed A,
Middha S, Kim HR, Srinivasan P, Gao J, Chakravarty D, Devlin SM, et
al: Mutational landscape of metastatic cancer revealed from
prospective clinical sequencing of 10,000 patients. Nat Med.
23:703–713. 2017. View
Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chalmers ZR, Connelly CF, Fabrizio D, Gay
L, Ali SM, Ennis R, Schrock A, Campbell B, Shlien A, Chmielecki J,
et al: Analysis of 100,000 human cancer genomes reveals the
landscape of tumor mutational burden. Genome Med. 9:342017.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hanahan D and Weinberg RA: Hallmarks of
cancer: The next generation. Cell. 144:646–674. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Burrell RA, McGranahan N, Bartek J and
Swanton C: The causes and consequences of genetic heterogeneity in
cancer evolution. Nature. 501:338–345. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cerami E, Gao J, Dogrusoz U, Gross BE,
Sumer SO, Aksoy BA, Jacobsen A, Byrne CJ, Heuer ML, Larsson E, et
al: The cBio cancer genomics portal: an open platform for exploring
multidimensional cancer genomics data. Cancer Discov. 2:401–404.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gao J, Aksoy BA, Dogrusoz U, Dresdner G,
Gross B, Sumer SO, Sun Y, Jacobsen A, Sinha R, Larsson E, et al:
Integrative analysis of complex cancer genomics and clinical
profiles using the cBioPortal. Sci Signal. 6:pl12013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Marcus L, Lemery SJ, Keegan P and Pazdur
R: FDA approval summary: Pembrolizumab for the treatment of
microsatellite instability-high solid tumors. Clin Cancer Res.
25:3753–3758. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Seth S, Ager A, Arends MJ and Frayling IM:
Lynch syndrome-cancer pathways, heterogeneity and immune escape. J
Pathol. 246:129–133. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lynch HT, Snyder CL, Shaw TG, Heinen CD
and Hitchins MP: Milestones of Lynch syndrome: 1895–2015. Nat Rev
Cancer. 15:181–194. 2015. View
Article : Google Scholar : PubMed/NCBI
|
|
23
|
Eso Y, Takai A, Matsumoto T, Inuzuka T,
Horie T, Ono K, Uemoto S, Lee K, Edelmann W, Chiba T and Marusawa
H: MSH2 dysregulation is triggered by proinflammatory cytokine
stimulation and is associated with liver cancer development. Cancer
Res. 76:4383–4393. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Arora S, Velichinskii R, Lesh RW, Ali U,
Kubiak M, Bansal P, Borghaei H, Edelman MJ and Boumber Y: Existing
and emerging biomarkers for immune checkpoint immunotherapy in
solid tumors. Adv Ther. 36:2638–2678. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Teo MY, Seier K, Ostrovnaya I, Regazzi AM,
Kania BE, Moran MM, Cipolla CK, Bluth MJ, Chaim J, Al-Ahmadie H, et
al: Alterations in DNA damage response and repair genes as
potential marker of clinical benefit from PD-1/PD-L1 blockade in
advanced urothelial cancers. J Clin Oncol. 36:1685–1694. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Türeci Ö, Löwer M, Schrörs B, Lang M,
Tadmor A and Sahin U: Challenges towards the realization of
individualized cancer vaccines. Nat Biomed Eng. 2:566–569. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Froimchuk E, Jang Y and Ge K: Histone H3
lysine 4 methyltransferase KMT2D. Gene. 627:337–342. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Lv J, Zhu Y, Ji A, Zhang Q and Liao G:
Mining TCGA database for tumor mutation burden and their clinical
significance in bladder cancer. Biosci Rep. 40:BSR201943372020.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Shen J, Ju Z, Zhao W, Wang L, Peng Y, Ge
Z, Nagel ZD, Zou J, Wang C, Kapoor P, et al: ARID1A deficiency
promotes mutability and potentiates therapeutic antitumor immunity
unleashed by immune checkpoint blockade. Nat Med. 24:556–562. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Qiu H, Zmina PM, Huang AY, Askew D and
Bedogni B: Inhibiting Notch1 enhances immunotherapy efficacy in
melanoma by preventing Notch1 dependent immune suppressive
properties. Cancer Lett. 434:144–151. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Dixon ZA, Nicholson L, Zeppetzauer M,
Matheson E, Sinclair P, Harrison CJ and Irving JA: CREBBP knockdown
enhances RAS/RAF/MEK/ERK signaling in Ras pathway mutated acute
lymphoblastic leukemia but does not modulate chemotherapeutic
response. Haematologica. 102:736–745. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Pastore A, Jurinovic V, Kridel R, Hoster
E, Staiger AM, Szczepanowski M, Pott C, Kopp N, Murakami M, Horn H,
et al: Integration of gene mutations in risk prognostication for
patients receiving first-line immunochemotherapy for follicular
lymphoma: A retrospective analysis of a prospective clinical trial
and validation in a population-based registry. Lancet Oncol.
16:1111–1122. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Mody K, Starr J, Saul M, Poorman K,
Weinberg BA, Salem ME, VanderWalde A and Shields AF: Patterns and
genomic correlates of PD-L1 expression in patients with biliary
tract cancers. J Gastrointest Oncol. 10:1099–1109. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Kared H, Adle-Biassette H, Foïs E, Masson
A, Bach JF, Chatenoud L, Schneider E and Zavala F:
Jagged2-expressing hematopoietic progenitors promote regulatory T
cell expansion in the periphery through notch signaling. Immunity.
25:823–834. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Cavalieri S, Perrone F, Miceli R, Ascierto
PA, Locati LD, Bergamini C, Granata R, Alfieri S, Resteghini C,
Galbiati D, et al: Efficacy and safety of single-agent pan-human
epidermal growth factor receptor (HER) inhibitor dacomitinib in
locally advanced unresectable or metastatic skin squamous cell
cancer. Eur J Cancer. 97:7–15. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Davis TB, Yang M, Schell MJ, Wang H, Ma L,
Pledger WJ and Yeatman TJ: PTPRS regulates colorectal cancer RAS
pathway activity by inactivating Erk and preventing its nuclear
translocation. Sci Rep. 8:92962018. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Sirkisoon SR, Carpenter RL, Rimkus T,
Anderson A, Harrison A, Lange AM, Jin G, Watabe K and Lo HW:
Interaction between STAT3 and GLI1/tGLI1 oncogenic transcription
factors promotes the aggressiveness of triple-negative breast
cancers and HER2-enriched breast cancer. Oncogene. 37:2502–2514.
2018. View Article : Google Scholar : PubMed/NCBI
|