Endometrial cancer (EC) is a malignant gynecological
disease that is prevalent in the developed world. It has been
estimated that ~63,230 women were diagnosed with EC and 11,350
women succumbed to this malignancy in 2018 in the United States
alone (1). The etiology of EC has
not yet been clearly elucidated. Traditionally, the ‘unopposed
estrogen’ hypothesis has been considered to explain the
carcinogenesis of EC (2). According
to this theory, without sufficient progestins to oppose them,
excessive endogenous and/or exogenous estrogens stimulate
proliferation and inhibit apoptosis of the endometrium. This
process has been considered to contribute to the pathogenesis of
EC. Data from numerous studies suggest that insulin resistance is
associated with a high risk of EC (3). Our previous study revealed that
elevated insulin levels, which is associated with insulin
resistance, is an independent risk factor for EC in premenopausal
women (4). Another study has
reported that insulin resistance-induced hyperinsulinemia
independently increases the risk of EC in postmenopausal women
(5). Furthermore, another of our
previous studies demonstrated that hyperinsulinemia is positively
associated with lymph node metastasis in patients with EC and
indicates a poor prognosis (6).
At present, surgery is the most effective treatment
option for this malignant disease. According to the National
Comprehensive Cancer Network guidelines, a surgical procedure
including total hysterectomy and bilateral accessory resection,
pelvic lymph node dissection and para-aortic lymph node dissection
is the most effective treatment method for EC (7). However, this surgical procedure leads
to a permanent loss of fertility in patients with EC. According to
a previous report (8), ~25% of
patients with EC are premenopausal, and 3~5% of these patients are
<40 years old and want to retain fertility. Among the latter
patients, 70–88% have not completed childbearing, and most of them
exhibit early-stage highly differentiated endometrioid endometrial
carcinoma with a good prognosis. Additionally, some patients cannot
undergo surgery due to serious complications. Currently,
progesterone is widely used in the conservative treatment of EC.
However, >30% of patients are insensitive or resistant to
progesterone treatment (9).
Furthermore, side effects, including thrombosis, liver damage,
weight gain and progesterone resistance, greatly limit the
application of this agent (10).
Metformin is a well-known first-line agent for the
treatment of type 2 diabetes, which inhibits hepatic glucose output
and intestinal glucose absorption, and promotes the uptake of
glucose by skeletal muscle to alleviate insulin resistance.
Metformin has also been suggested to be a potential anticancer
agent (11). Studies have reported
that metformin inhibits the proliferation of a variety of tumor
cells, including gastric cancer, pancreatic cancer, medullary
thyroid carcinoma and EC cells, in a dose-dependent manner
(12–15). The mechanism of this inhibitory
effect has been suggested to be associated with cell cycle arrest
and the promotion of apoptosis (16). Our previous study revealed that the
combined application of metformin and progestins synergistically
inhibits the proliferation of EC cells, and suggested that
downregulation of the expression levels of cyclin D1 and cyclin E
may be an underlying mechanism of this synergistic inhibitory
effect (17). Based on the
aforementioned results, it may be concluded that metformin is a
promising therapeutic option for EC. The anticancer effect of
metformin in EC appears to be mediated via direct and indirect
mechanisms, which are described in the following sections of this
review. Relevant articles and studies were identified using Medline
with the following key words alone or in combination: ‘Endometrial
cancer’, ‘metformin’, ‘treatment’, ‘signaling pathway’, ‘insulin
resistance’, ‘insulin’, ‘inflammatory factor’ and ‘adipokines’.
Insulin resistance is characterized as a reduction
in the insulin sensitivity of body tissues during metabolic
activity, leading to an increase in circulating insulin levels
(18). Insulin resistance is known
to reduce the insulin-mediated utilization of glucose by the body.
This has been suggested to be one of the most important mechanisms
of the pathogenesis of diabetes (19). Furthermore, it has been noted that
conditions other than diabetes that are closely associated with
insulin resistance, namely hypertension, coronary heart disease and
hyperlipidemia, also serve important roles in the pathogenesis of
certain malignant diseases such as EC, breast cancer and colon
cancer (20).
In cases of insulin resistance, particularly in the
early stages, circulating insulin levels may be higher than normal
(21). Insulin, which is produced
and secreted by pancreatic β cells, regulates glucose homeostasis
by regulating hepatic glucose production and the uptake of glucose
by fat and muscle tissue (22). The
role insulin serves in tissues is mediated via the insulin
receptor, which comprises insulin receptor α (IRα) and IRβ
subtypes. IRα has a ligand-binding domain that is activated by
insulin-induced autophosphorylation. Total insulin receptor and IRα
expression levels in EC tissues have been identified to be higher
than those in normal endometrial tissues in vivo, whereas
in vitro, the overexpression of IRα has been shown to be
positively associated with EC cell proliferation (23). This suggests that the activation of
insulin signaling is likely to be closely associated with the
carcinogenesis of EC. Furthermore, insulin has been suggested to
act as a direct mitogenic promoter in the malignant transformation
of the endometrium (24).
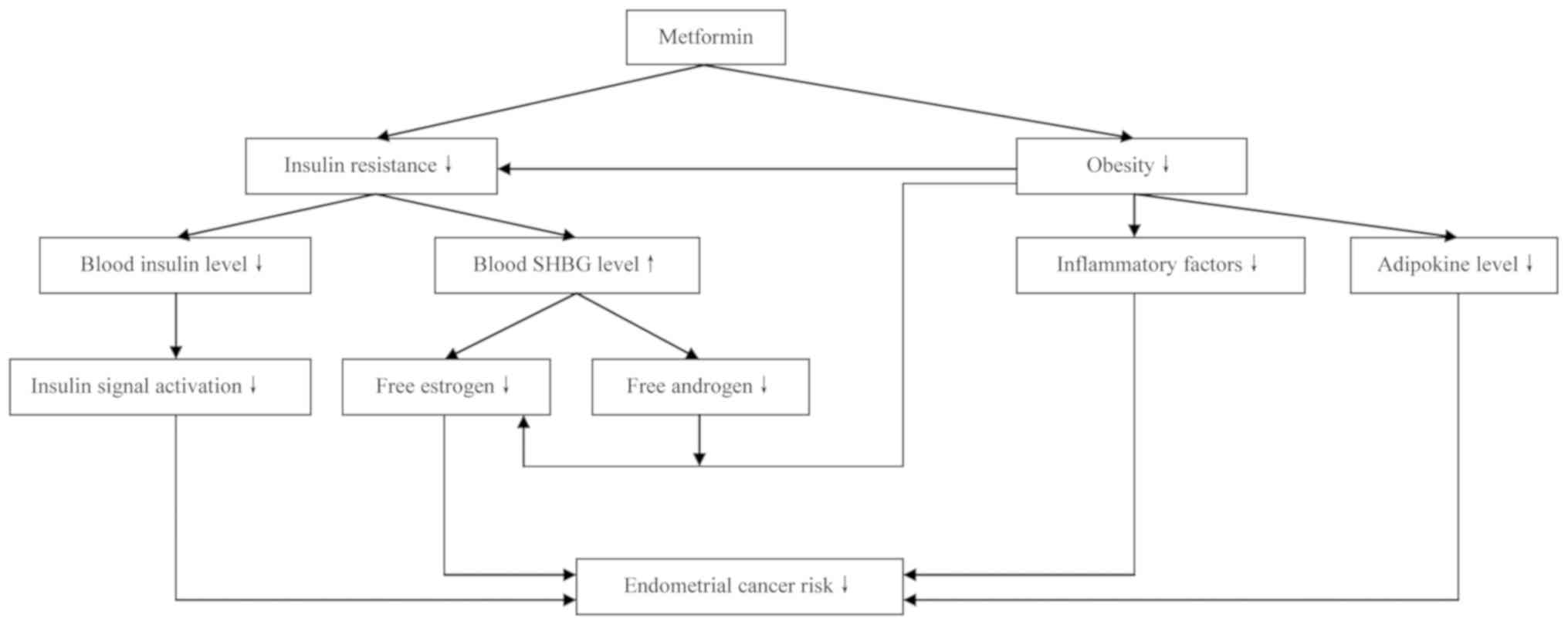
Additionally, it has been reported that excessive insulin inhibits
the production of sex hormone binding globulin (SHBG), leading to
increased levels of free estrogens and androgens (25). Subsequently, excessive estrogens
promote the carcinogenesis of EC according to the ‘unopposed
estrogen’ hypothesis, while excessive androgens provide additional
substrate for aromatase-catalyzed biotransformation to estrogen in
adipose tissue, resulting in increased circulating levels of
estrogen that stimulate the pathogenesis of EC.
There is evidence to suggest that diseases
associated with insulin resistance are also risk factors of EC.
Body mass index (BMI) is an effective indicator of obesity. It has
been reported that patients with a higher BMI usually have a higher
risk of EC (26). A clinical study
found that elevated BMI value means increased EC risk (27). Furthermore, in another study, the
waist-to-hip ratio of patients with EC was shown to be markedly
higher than that of control patients with benign endometrial
lesions (28), which is consistent
with previous findings that upper body obesity is closely
associated with EC risk (29). Obese
patients often have excessive adipose tissue in which estrogen
biosynthesis can occur. Additionally, greater amounts of adipose
tissue are usually associated with higher levels of adipokines and
inflammatory factors, and these have been suggested to serve an
important role in the carcinogenesis of EC (30,31).
Type 2 diabetes is another risk factor for both insulin resistance
and EC. Increased serum insulin levels have been reported to
increase the risk of EC in the early stage of diabetes in a
dose-dependent manner (32), and
hyperinsulinemia is considered to be an independent risk factor for
EC (33). In addition to increasing
the incidence of EC, type 2 diabetes also increases the risk of
death in patients with EC (34).
Furthermore, type 2 diabetes combined with obesity markedly
increases EC risk (35). The fasting
insulin levels and insulin resistance index values of patients with
EC have been shown to be higher than those of controls with benign
endometrial lesions (28). Insulin
resistance is not only a disease, but also a key pathophysiological
process in obesity, diabetes, hypertension and metabolic syndrome.
Strategies to promote weight loss, including dietary adjustments
and regular physical activity, have been suggested to effectively
decrease the risk of insulin resistance as well as that of EC
(36).
Our previous review suggested that insulin
resistance serves a central role in the pathogenesis of EC
(3). As an effective insulin
sensitizer, metformin greatly improves the utilization of insulin
by body tissues to ameliorate insulin resistance. As a result,
circulating insulin levels are decreased, which decreases the risk
of EC induced by excessive insulin (37). Additionally, the downregulation of
circulating insulin levels is considered helpful in the control of
body weight, and reductions in body weight have been suggested to
inhibit the carcinogenesis of EC (38). This may be at least partly explained
by downregulated levels of adipokines and inflammatory factors. A
clinical trial has demonstrated that metformin delays the
development of obesity by improving the resistance status of leptin
and insulin growth factor-1 decreasing the levels of insulin, which
inhibits the development of EC (39). Additionally, metformin has been
reported to increase adiponectin gene expression levels in obese
patients, promote the secretion of adiponectin from adipose tissue
and thereby induce the apoptosis of EC cells (40). Furthermore, the loss of adipose
tissue due to body weight reduction results in less tissue being
available for aromatase-catalyzed estrogen biosynthesis. Overall,
it may be concluded that metformin indirectly inhibits the
development of EC by ameliorating insulin resistance.
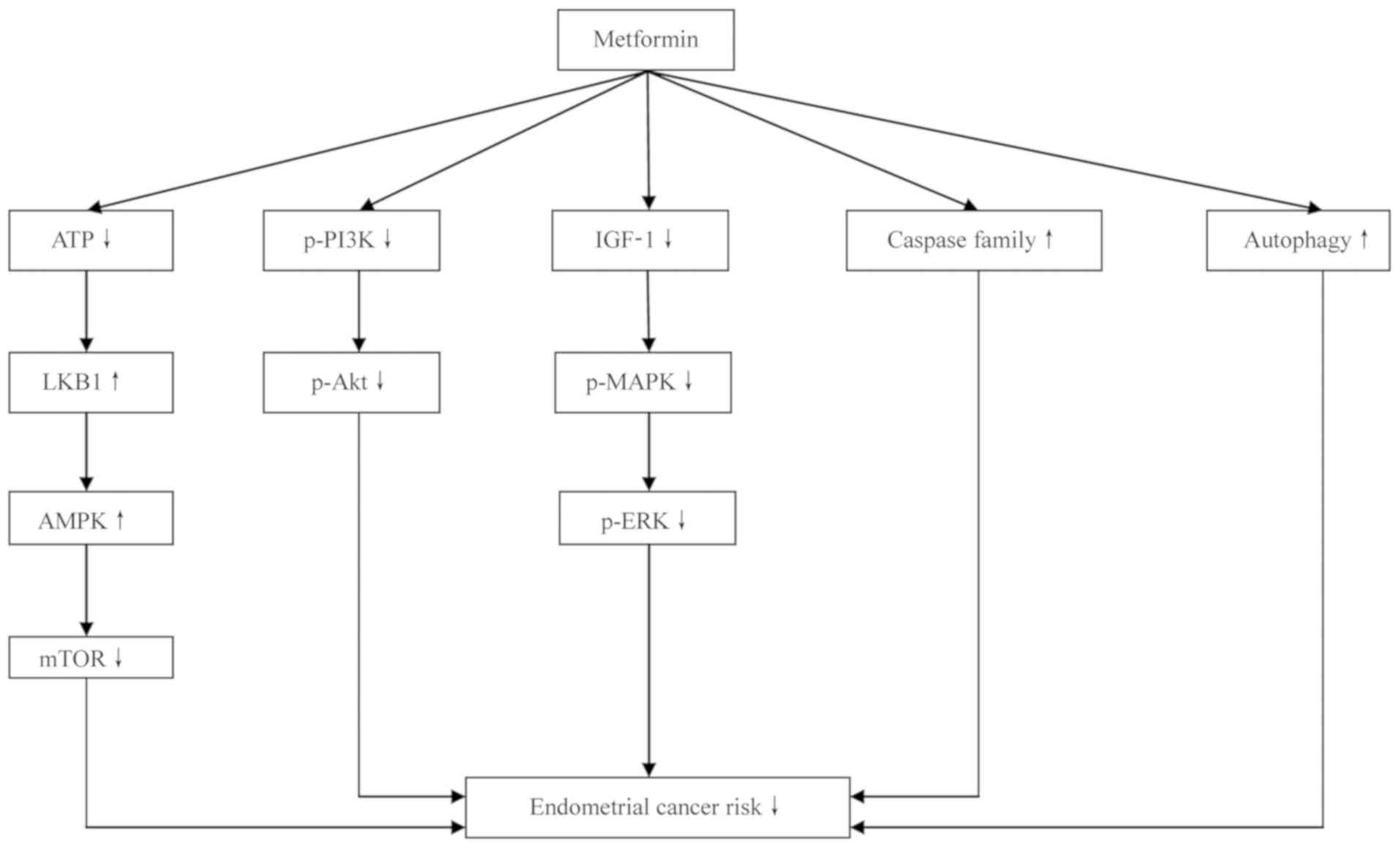
Metformin has been reported to inhibit the
proliferation, migration and invasion of EC cells, and to promote
tumor cell apoptosis. However, the specific mechanism remains
unclear. Current data suggest that metformin may inhibit the
development of EC via a number of pathways described
hereinafter.
Metformin has been reported to increase glucose
uptake by activating the AMPK signaling pathway (41). AMPK is a heterotrimeric
serine/threonine protein kinase complex composed of a catalytic α
subunit and regulatory β and γ subunits. AMPK has been suggested to
be responsible for the regulation of energy metabolism. It is
activated by the cellular stress induced by decreased cellular
energy levels and an increased AMP/ATP ratio (42). Once activated, AMPK restores cellular
energy levels by stimulating catabolic signaling pathways,
including glucose uptake, glycolysis and fatty acid oxidation, and
inhibiting ATP-depleting processes, such as fatty acid, cholesterol
and protein synthesis (43). LKB1,
also known as serine/threonine kinase 11, is an upstream kinase of
AMPK that is generally considered to be a tumor suppressor gene.
Biochemical and genetic analyses have revealed that under energy
stress, LKB1 activates AMPK by phosphorylating AMPK (44). Loss of LKB1 gene expression has been
identified in ~65% of patients with EC (45). LKB1 expression is inversely
associated with tumor grade and stage; the inactivation or
downregulation of LKB1 promotes the progression of EC and its loss
promotes a highly invasive phenotype. As a tumor suppressor gene,
LKB1 may inhibit the occurrence and development of EC via the
LKB1-AMPK-mTOR signaling pathway (46).
Metformin enters cancer cells via the organic
cationic transporter, and inhibits the activity of the respiratory
transporter complex, thereby reducing ATP production. The reduction
in ATP level activates the tumor suppressor gene LKB1, which then
phosphorylates AMP (46). AMPK
regulates several signaling pathways and controls cell
proliferation, primarily via inhibition of the mTOR signaling
pathway. The available data suggest that the antiproliferative
effect of metformin on cancer cells is likely to be mediated via
the LKB1-AMPK signaling pathway. For example, in a study of breast
cancer cells, metformin activated AMPK by phosphorylating LKB1, and
thus inhibited tuberous sclerosis complex 2 phosphorylation and
mTOR pathway activation, resulting in the proliferation and
apoptosis of the cells being decreased and increased, respectively
(47). Also, the results of an in
vitro study using ECC-1 and Ishikawa cells demonstrated that
metformin reduced cell proliferation and increased AMPK activation
in a dose-dependent manner, and indicated that the mTOR signaling
pathway inhibition contributed to these effects (48). Metformin has been found to be
functionally similar to an mTOR inhibitor, and the PTEN signaling
pathway, which is tightly associated with the carcinogenesis of EC,
may also be a target of metformin (49). Experiments in mice demonstrated a 50%
reduction in the weight of EC xenografts following treatment with
metformin, mediated via inhibition of the LKB1-AMPK-mTOR signaling
pathway (50). Metformin has also
been revealed to suppress the development of EC xenografts and
ameliorate metabolism disorders in obese mice, with the
LKB1-AMPK-mTOR signaling pathway being suggested to be partly
responsible for the therapeutic effects (51).
PI3K is a cytoplasmic enzyme that is an important
member of the phospholipase family, promoting cell proliferation
(52). It has both lipid and protein
kinase activities. According to the composition of the lipid
kinase, PI3K is divided into three subclasses: I, II and III. Class
I PI3K is a heterodimer consisting of a catalytic subunit and a
regulatory subunit. It is divided into two subclasses: IA (composed
by PIK3 CA, PIK3 CB and PIK3 CD) and IB (encoded by PIK3 CG). PIK3
CA is more susceptible to mutation than PIK3 CB (53), and has been reported to serve an
important role in the development of several malignant diseases
(54). Class I PI3K phosphorylates
phosphatidylinositol 4,5 diphosphate (PIP2) to form
3,4,5-trisphosphate phosphatidylinositol (PIP3). Subsequently, PIP3
acts as a second intracellular messenger that is involved in
several molecular biological events such as the promotion of cell
proliferation and the inhibition of apoptosis (55). PTEN is a phosphatase gene homologous
to tensin, which is located on human chromosome 10 q23 and acts as
a tumor suppressor gene. PTEN dephosphorylates PIP3 to form PIP2,
which serves a negative regulatory role in the downstream signaling
pathway of PI3K (56). The
activation of PI3K and functional inactivation of PTEN by mutation
have been identified in several human malignant tumors, suggesting
that PI3K is associated with tumor pathogenesis (57). Protein kinase B, also known as Akt,
is a downstream signaling molecule of PI3K that is activated by the
phosphorylation of phosphatidylinositol family members on the cell
membrane. Subsequently, activated Akt phosphorylates the Ser196 of
cysteinyl aspartate specific proteinase (caspase)-3 and caspase-9,
thereby inhibiting apoptosis. The lipid phosphatase activity of
PTEN has a tumor-suppressing effect mediated via specific
dephosphorylation of the phosphatidylinositol D3 ring, which
antagonizes phosphorylation of the PI3K substrate and negatively
regulates the PIK3-Akt signal transduction pathway (58).
As an insulin sensitizer, metformin decreases
circulating insulin levels and thereby inhibits the IGF-1-induced
phosphorylation of Akt (39).
Metformin has been found to not only block the regulatory effect of
feedback from the IGF-1R signaling pathway, but also to induce
tumor cell apoptosis when combined with IGF-1R inhibitors (73). Clinical data suggest that a regular
dose (500 mg/time, 3 times per day) of metformin effectively
reduces elevated IGF-1 levels in the circulation of patients with
EC and decreases IGF-1 expression in cancer tissues (74). In an in vitro study, metformin
delayed and prevented the IGF-1R feedback-induced proliferation of
EC cells, with high concentrations of metformin markedly promoting
the apoptosis of EC cells (67). In
an in vivo study, the intraperitoneal injection of metformin
markedly reduced the circulating IGF-1 levels in mice and strongly
inhibited the development of xenograft tumors (75). In addition to suppressing the
proliferation-promoting effect of IGF-1 and IGF-2, metformin has
also been shown to increase progesterone receptor expression, which
appears to be beneficial in the treatment of EC (72).
Caspases are a group of cytoplasmic proteases with
similar structures. They are responsible for selectively cleaving
certain proteins, which leads to apoptosis. Genetic polymorphisms
in caspase genes may affect the risk of cancer by altering the
expression levels and function of these genes (76). Caspase-3 and −7 have been identified
as key performers of cell apoptosis and serve a central role in the
execution phase of apoptosis (77).
Caspase-8 is required for death receptor-mediated apoptosis,
whereas caspase-9 is required for mitochondria-mediated apoptosis.
The activation of caspase-8 and −9 induces the subsequent
activation of other cysteine proteases and promotes cell apoptosis
(78). Inactivating mutations of the
caspase gene have been suggested to be associated with the
pathogenesis of certain human solid cancers, including EC (76). Metformin activates caspase-8/9 by
promoting the electron transport chain and membrane permeability,
and the activation of caspase 8/9 leads to the subsequent
activation of other caspase enzymes, thereby reducing cell
proliferation and promoting apoptosis (79,80). The
stimulating effect of metformin on members of the caspase family is
dose-dependent (81).
Autophagy refers to the process of cell degradation
induced by exogenous stimuli, in which degradation products, such
as those derived from the endoplasmic reticulum and Golgi apparatus
are recovered and transported to the lysosome for catabolism in
order to recycle energy and maintain the stability of the
intracellular environment (82). As
a signaling pathway for cell survival, autophagy suppresses the
cellular stress response and genomic damage by eliminating
abnormally folded proteins and organelles, such as mitochondria and
lysosomes, from tumor cells, thereby suppressing the occurrence of
cancer. The expression levels of Beclin 1, an autophagy-associated
gene, have been shown to be positively associated with the tumor
grade and degree of myometrial infiltration in EC (83). High Beclin expression is associated
with high expression of hypoxia inducible factor 1α. Increased
autophagy appears to aid tumor survival in a hypoxic
microenvironment (84).
Microtubule-associated protein 1A/1B-light chain 3 (LC3) expression
may be considered a marker of excessive autophagy in EC (85). It has been reported that metformin
induces autophagy in colon cancer, melanoma and Ishikawa EC cells
(86). Upregulation of the
expression levels of autophagy-associated genes, including LC3 and
Beclin 1, is considered to be a mechanism via which metformin
promotes cell autophagy (87).
Furthermore, the knockdown of Beclin 1 expression or inhibition of
caspase-3/7 has been shown to inhibit metformin-induced cell
autophagy and promote cell proliferation (88). Therefore, metformin promoted
autophagy, induced apoptosis and suppressed cell survival in
ovarian cancer cells (89).
Unfortunately, clinical data regarding the effect of
metformin in EC are limited. The results provided by different
studies are conflicting. One study revealed that the use of
metformin in women with diabetes is associated with a lower overall
risk of EC (90). However, another
study indicated that metformin does not significantly affect the
risk of EC (91). Although some
studies have investigated the association between metformin use and
the survival of patients with EC, whether the use of metformin is
associated with improved clinical outcomes in patients with EC
remains unclear. In one study, it was demonstrated that patients
who did not receive metformin had a 2.3-fold increased risk of
mortality compared with patients receiving metformin after
adjustments for age, stage, grade, histology and adjuvant treatment
(92). However, another study
revealed that the overall survival of patients with EC who had or
had not received metformin treatment was similar after adjusting
for confounding covariates (93).
Endometrial hyperplasia is an important precancerous condition of
EC. Clinically, progesterone agents and levonorgestrel intrauterine
devices have been widely used in the treatment of endometrial
hyperplasia. However, the side effects and continued risk of
recurrence associated with these therapeutic methods have been
reported in several studies (94).
In a small-scale clinical study, metformin was used in combination
with medroxyprogesterone acetate in the treatment of endometrial
hyperplasia and EC limited to the endometrium. After 36 weeks, 29
out of 36 patients achieved a complete response. It was noted that
6 of 36 patients suffered diarrhea and nausea when the daily dose
of metformin was 2,250 mg (95).
However, it was not confirmed whether there were any other
potential causes of these side effects. As a novel medication in
the treatment of endometrial hyperplasia and EC, the effect of
metformin requires further investigation.
In conclusion, although the experimental data
support the therapeutic effect of metformin in EC, the detailed
mechanisms of the therapeutic effect of metformin remain unclear.
Furthermore, the clinical applicability of metformin alone or in
combination with other medications remains uncertain. These topics
warrant further investigation in the future.
Not applicable.
No funding was received.
Not applicable.
JH and YY designed and arranged the manuscript. NM,
TX and MG wrote the article. MD, QT, LH, GW, ZL and WW found and
analyzed the references in Medline, participated in writing the
current paper and gave final approval of the version to be
published. NM and TX revised the paper. All authors read and
approved the final manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2018. CA Cancer J Clin. 68:7–30. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
van Weelden WJ, Massuger LFAG, ENITE C,
Pijnenborg JMA and Romano A: Anti-estrogen treatment in endometrial
cancer: A systematic review. Front Oncol. 9:3592019. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mu N, Zhu Y, Wang Y, Zhang H and Xue F:
Insulin resistance: A significant risk factor of endometrial
cancer. Gynecol Oncol. 125:751–757. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Shao Y, Cheng S, Hou J, Zuo Y, Zheng W,
Xia M and Mu N: Insulin is an important risk factor of endometrial
cancer among premenopausal women: A case-control study in China.
Tumour Biol. 37:4721–4726. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Arthur RS, Kabat GC, Kim MY, Wild RA,
Shadyab AH, Wactawski-Wende J, Ho GYF, Reeves KW, Kuller LH, Luo J,
et al: Metabolic syndrome and risk of endometrial cancer in
postmenopausal women: A prospective study. Cancer Causes Control.
30:355–363. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mu N, Dong M, Liu C, Wang X, Cong J, Wang
L, Wang X, Lakhani I, Liu X, Hou J, et al: Association between
preoperative serum insulin levels and lymph node metastasis in
endometrial cancer-a prospective cohort study. Cancer Med.
7:1519–1527. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Amant F, Moerman P, Neven P, Timmerman D,
Van Limbergen E and Vergote I: Endometrial cancer. Lancet.
366:491–505. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Carneiro MM, Lamaita RM, Ferreira MC and
Silva-Filho AL: Fertility-preservation in endometrial cancer: Is it
safe? Review of the literature. JBRA Assist Reprod. 20:232–239.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Koopman E, Blok LJ, Brinkmann AO,
Helmerhorst TJ and Huikeshoven FJ: Differential gene expression in
progesterone-sensitive and progesterone-insensitive endometrial
carcinoma cells. Eur J Obstet Gynecol Reprod Biol. 82:135–138.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Marjoribanks J, Farquhar C, Roberts H,
Lethaby A and Lee J: Long-term hormone therapy for perimenopausal
and postmenopausal women. Cochrane Database Syst Rev.
1:CD0041432017.PubMed/NCBI
|
|
11
|
Mallik R and Chowdhury TA: Metformin in
cancer. Diabetes Res Clin Pract. 143:409–419. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gadducci A, Biglia N, Tana R, Cosio S and
Gallo M: Metformin use and gynecological cancers: A novel treatment
option emerging from drug repositioning. Crit Rev Oncol Hematol.
105:73–83. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yamana H, Kato K, Kobara H, Fujihara S,
Fujita K, Namima D, Fujita N, Kobayashi K, Kamada H, Morishita A,
et al: Metformin inhibits proliferation and tumor growth of QGP-1
pancreatic neuroendocrine tumor cells by inducing cell cycle arrest
and apoptosis. Anticancer Res. 40:121–132. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Klubo-Gwiezdzinska J, Jensen K, Costello
J, Patel A, Hoperia V, Bauer A, Burman KD, Wartofsky L and Vasko V:
Metformin inhibits growth and decreases resistance to anoikis in
medullary thyroid cancer cells. Endocr Relat Cancer. 19:447–456.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Liu S, Yue C, Chen H, Chen Y and Li G:
Metformin promotes Beclin1-Dependent autophagy to inhibit the
progression of gastric cancer. Onco Targets Ther. 13:4445–4455.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ye J, Qi L, Chen K, Li R, Song S, Zhou C
and Zhai W: Metformin induces TPC-1 cell apoptosis through
endoplasmic reticulum stress-associated pathways in vitro and in
vivo. Int J Oncol. 55:331–339. 2019.PubMed/NCBI
|
|
17
|
Mu N, Dong M, Li L, Xia M, Qv L, Wang Y,
Dong C, Chen Y, Zuo Y, Hou J and Xue F: Synergistic effect of
metformin and medroxyprogesterone 17acetate on the development of
endometrial cancer. Oncol Rep. 39:2015–2021. 2018.PubMed/NCBI
|
|
18
|
Hari Kumar KVS: The good, the bad, and the
ugly facets of insulin resistance. Med J Armed Forces India.
76:4–7. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Luc K, Schramm-Luc A, Guzik TJ and
Mikolajczyk TP: Oxidative stress and inflammatory markers in
prediabetes and diabetes. J Physiol Pharmacol. 70:809–824.
2019.
|
|
20
|
Patel TP, Rawal K, Bagchi AK, Akolkar G,
Bernardes N, Dias DDS, Gupta S and Singal PK: Insulin resistance:
An additional risk factor in the pathogenesis of cardiovascular
disease in type 2 diabetes. Heart Fail Rev. 21:11–23. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yang C, Qu H, Zhao X, Hu Y, Xiong J, Jiang
X, Chen Y and Li Z: Plasma secretagogin is increased in individuals
with glucose dysregulation. Exp Clin Endocrinol Diabetes. Sep
23–2019.(Epub ahead of print). doi: 10.1055/a-1001-2244.
|
|
22
|
Kheirandish M, Mahboobi H, Yazdanparast M,
Kamal W and Kamal MA: Anti-cancer effects of metformin: Recent
evidences for its role in prevention and treatment of cancer. Curr
Drug Metab. 19:793–797. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pollak M: The insulin and insulin-like
growth factor receptor family in neoplasia: An update. Nat Rev
Cancer. 12:159–169. 2012. View
Article : Google Scholar : PubMed/NCBI
|
|
24
|
Eritja N, Mirantes C, Llobet D, Yeramian
A, Bergadà L, Dosil MA, Domingo M, Matias-Guiu X and Dolcet X:
Long-term estradiol exposure is a direct mitogen for
insulin/EGF-primed endometrial cells and drives PTEN loss-induced
hyperplasic growth. Am J Pathol. 183:277–287. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Arcidiacono B, Iiritano S, Nocera A,
Possidente K, Nevolo MT, Ventura V, Foti D, Chiefari E and Brunetti
A: Insulin resistance and cancer risk: An overview of the
pathogenetic mechanisms. Exp Diabetes Res. 2012:7891742012.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kliemann N, Murphy N, Viallon V, Freisling
H, Tsilidis KK, Rinaldi S, Mancini FR, Fagherazzi G, Boutron-Ruault
MC, Boeing H, et al: Predicted basal metabolic rate and cancer risk
in the European prospective investigation into cancer and
nutrition. Int J Cancer. 147:648–661. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bjorge T, Haggstrom C, Ghaderi S, Nagel G,
Manjer J, Tretli S, Ulmer H, Harlid S, Rosendahl AH, Lang A, et al:
BMI and weight changes and risk of obesity-related cancers: A
pooled European cohort study. Int J Epidemiol. 48:1872–1885. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Lai Y and Sun C: Association of abnormal
glucose metabolism and insulin resistance in patients with atypical
and typical endometrial cancer. Oncol Lett. 15:2173–2178.
2018.PubMed/NCBI
|
|
29
|
Xu WH, Matthews CE, Xiang YB, Zheng W,
Ruan ZX, Cheng JR, Gao YT and Shu XO: Effect of adiposity and fat
distribution on endometrial cancer risk in Shanghai women. Am J
Epidemiol. 161:939–947. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Yoon YS, Kwon AR, Lee YK and Oh SW:
Circulating adipokines and risk of obesity related cancers: A
systematic review and meta-analysis. Obes Res Clin Pract.
13:329–339. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Che Q, Xiao X, Liu M, Lu Y, Dong X and Liu
S: IL-6 promotes endometrial cancer cells invasion and migration
through signal transducers and activators of transcription 3
signaling pathway. Pathol Res Pract. 215:1523922019. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Wang Y, Hua S, Tian W, Zhang L, Zhao J,
Zhang H, Zhang W and Xue F: Mitogenic and anti-apoptotic effects of
insulin in endometrial cancer are phosphatidylinositol 3-kinase/Akt
dependent. Gynecol Oncol. 125:734–741. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Gunter MJ, Hoover DR, Yu H,
Wassertheil-Smoller S, Manson JE, Li J, Harris TG, Rohan TE, Xue X,
Ho GY, et al: A prospective evaluation of insulin and insulin-like
growth factor-I as risk factors for endometrial cancer. Cancer
Epidemiol Biomarkers Prev. 17:921–929. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Anastasi E, Filardi T, Tartaglione S,
Lenzi A, Angeloni A and Morano S: Linking type 2 diabetes and
gynecological cancer: An introductory overview. Clin Chem Lab Med.
56:1413–1425. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Yang X and Wang J: The role of metabolic
syndrome in endometrial cancer: A review. Front Oncol. 9:7442019.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
MacKintosh ML, Derbyshire AE, McVey RJ,
Bolton J, Nickkho-Amiry M, Higgins CL, Kamieniorz M, Pemberton PW,
Kirmani BH, Ahmed B, et al: The impact of obesity and bariatric
surgery on circulating and tissue biomarkers of endometrial cancer
risk. Int J Cancer. 144:641–650. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Mitsuhashi A, Kiyokawa T, Sato Y and Shozu
M: Effects of metformin on endometrial cancer cell growth in vivo:
A preoperative prospective trial. Cancer. 120:2986–2995. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Zhang K, Luo Y, Dai H and Deng Z: Effects
of bariatric surgery on cancer risk: Evidence from meta-analysis.
Obes Surg. 30:1265–1272. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Soliman PT, Zhang Q, Broaddus RR, Westin
SN, Iglesias D, Munsell MF, Schmandt R, Yates M, Ramondetta L and
Lu KH: Prospective evaluation of the molecular effects of metformin
on the endometrium in women with newly diagnosed endometrial
cancer: A window of opportunity study. Gynecol Oncol. 143:466–471.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Yates MS, Coletta AM, Zhang Q, Schmandt
RE, Medepalli M, Nebgen D, Soletsky B, Milbourne A, Levy E, Fellman
B, et al: Prospective randomized biomarker study of metformin and
lifestyle intervention for prevention in obese women at increased
risk for endometrial cancer. Cancer Prev Res (Phila). 11:477–490.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Zhou G, Myers R, Li Y, Chen Y, Shen X,
Fenyk-Melody J, Wu M, Ventre J, Doebber T, Fujii N, et al: Role of
AMP-activated protein kinase in mechanism of metformin action. J
Clin Invest. 108:1167–1174. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Vallianou NG, Evangelopoulos A and Kazazis
C: Metformin and cancer. Rev Diabet Stud. 10:228–235. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Wang Y, An H, Liu T, Qin C, Sesaki H, Guo
S, Radovick S, Hussain M, Maheshwari A, Wondisford FE, et al:
Metformin improves mitochondrial respiratory activity through
activation of AMPK. Cell Rep. 29:1511–1523 e5. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Jiang S, Wang Y, Luo L, Shi F, Zou J, Lin
H, Ying Y, Luo Y, Zhan Z, Liu P, et al: AMP-activated protein
kinase regulates cancer cell growth and metabolism via nuclear and
mitochondria events. J Cell Mol Med. 23:3951–3961. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Pena CG, Nakada Y, Saatcioglu HD, Aloisio
GM, Cuevas I, Zhang S, Miller DS, Lea JS, Wong KK, DeBerardinis RJ,
et al: LKB1 loss promotes endometrial cancer progression via
CCL2-dependent macrophage recruitment. J Clin Invest.
125:4063–4076. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Saraei P, Asadi I, Kakar MA and Moradi-Kor
N: The beneficial effects of metformin on cancer prevention and
therapy: A comprehensive review of recent advances. Cancer Manag
Res. 11:3295–3313. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
El-Sisi AE, Sokar SS, El-Sayad ME, Moussa
EA and Salim EI: Anticancer effect of metformin against
2-amino-1-methyl-6-phenylimidazo [4,5-b]pyridine-induced rat
mammary carcinogenesis is through AMPK pathway and modulation of
oxidative stress markers. Hum Exp Toxicol. 38:703–712. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Cantrell LA, Zhou C, Mendivil A, Malloy
KM, Gehrig PA and Bae-Jump VL: Metformin is a potent inhibitor of
endometrial cancer cell proliferation-implications for a novel
treatment strategy. Gynecol Oncol. 116:92–98. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Pabona JMP, Burnett AF, Brown DM, Quick
CM, Simmen FA, Montales MTE, Liu SJ, Rose T, Alhallak I, Siegel ER
and Simmen RC: Metformin promotes anti-tumor biomarkers in human
endometrial cancer cells. Reprod Sci. 27:267–277. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Iglesias DA, Yates MS, van der Hoeven D,
Rodkey TL, Zhang Q, Co NN, Burzawa J, Chigurupati S, Celestino J,
Bowser J, et al: Another surprise from Metformin: Novel mechanism
of action via K-Ras influences endometrial cancer response to
therapy. Mol Cancer Ther. 12:2847–2856. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Guo H, Kong W, Zhang L, Han J, Clark LH,
Yin Y, Fang Z, Sun W, Wang J, Gilliam TP, et al: Reversal of
obesity-driven aggressiveness of endometrial cancer by metformin.
Am J Cancer Res. 9:2170–2193. 2019.PubMed/NCBI
|
|
52
|
Moroi AJ and Watson SP: Impact of the
PI3-kinase/Akt pathway on ITAM and hemITAM receptors: Haemostasis,
platelet activation and antithrombotic therapy. Biochem Pharmacol.
94:186–194. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Martini M, De Santis MC, Braccini L,
Gulluni F and Hirsch E: PI3K/AKT signaling pathway and cancer: An
updated review. Ann Med. 46:372–383. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Guo S, Loibl S, von Minckwitz G,
Darb-Esfahani S, Lederer B and Denkert C: PIK3CA H1047R mutation
associated with a lower pathological complete response rate in
triple-negative breast cancer patients treated with
anthracycline-taxane-based neoadjuvant chemotherapy. Cancer Res
Treat. 52:689–696. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Jhanwar-Uniyal M, Wainwright JV, Mohan AL,
Tobias ME, Murali R, Gandhi CD and Schmidt MH: Diverse signaling
mechanisms of mTOR complexes: mTORC1 and mTORC2 in forming a
formidable relationship. Adv Biol Regul. 72:51–62. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Johnston SB and Raines RT: Catalysis by
the tumor-suppressor enzymes PTEN and PTEN-L. PLoS One.
10:e01168982015. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Kim SM, Nguyen TT, Ravi A, Kubiniok P,
Finicle BT, Jayashankar V, Malacrida L, Hou J, Robertson J, Gao D,
et al: PTEN Deficiency and AMPK activation promote nutrient
scavenging and anabolism in prostate cancer cells. Cancer Discov.
8:866–883. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Leitner MG, Hobiger K, Mavrantoni A, Feuer
A, Oberwinkler J, Oliver D and Halaszovich CR: A126 in the active
site and TI167/168 in the TI loop are essential determinants of the
substrate specificity of PTEN. Cell Mol Life Sci. 75:4235–4250.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Salvesen HB, Werner HM and Krakstad C:
PI3K pathway in gynecologic malignancies. Am Soc Clin Oncol Educ
Book. Jun 31–2013.(Epub ahead of print). doi:
10.1200/EdBook_AM.2013.33.e218. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Mackay HJ, Eisenhauer EA, Kamel-Reid S,
Tsao M, Clarke B, Karakasis K, Werner HM, Trovik J, Akslen LA,
Salvesen HB, et al: Molecular determinants of outcome with
mammalian target of rapamycin inhibition in endometrial cancer.
Cancer. 120:603–610. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
de Melo AC, Paulino E and Garces AH: A
review of mTOR pathway inhibitors in gynecologic cancer. Oxid Med
Cell Longev. 2017:48097512017. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Kosmas K, Mitropoulou G, Provatas I,
Stamoulas M and Marouga A: Expression of phosphatase and tensin
homologue in imprint smears of endometrial carcinoma.
Cytopathology. 29:558–564. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Roncolato F, Lindemann K, Willson ML,
Martyn J and Mileshkin L: PI3K/AKT/mTOR inhibitors for advanced or
recurrent endometrial cancer. Cochrane Database Syst Rev.
10:CD0121602019.PubMed/NCBI
|
|
64
|
Saini N and Yang X: Metformin as an
anti-cancer agent: Actions and mechanisms targeting cancer stem
cells. Acta Biochim Biophys Sin (Shanghai). 50:133–143. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Qiang P, Shao Y, Sun YP, Zhang J and Chen
LJ: Metformin inhibits proliferation and migration of endometrial
cancer cells through regulating PI3K/AKT/MDM2 pathway. Eur Rev Med
Pharmacol Sci. 23:1778–1785. 2019.PubMed/NCBI
|
|
66
|
Kasprzak A, Kwasniewski W, Adamek A and
Gozdzicka-Jozefiak A: Insulin-like growth factor (IGF) axis in
cancerogenesis. Mutat Res Rev Mutat Res. 772:78–104. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Zhang Y, Li MX, Wang H, Zeng Z and Li XM:
Metformin down-regulates endometrial carcinoma cell secretion of
IGF-1 and expression of IGF-1R. Asian Pac J Cancer Prev.
16:221–225. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Tandon M, Chen Z, Othman AH and Pratap J:
Role of Runx2 in IGF-1Rβ/Akt- and AMPK/Erk-dependent growth,
survival and sensitivity towards metformin in breast cancer bone
metastasis. Oncogene. 35:4730–4740. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Chen G, Yuan C, Duan F, Liu Y, Zhang J, He
Z, Huang H, He C and Wang H: IGF1/MAPK/ERK signaling
pathway-mediated programming alterations of adrenal cortex cell
proliferation by prenatal caffeine exposure in male offspring rats.
Toxicol Appl Pharmacol. 341:64–76. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Wang CF, Zhang G, Zhao LJ, Qi WJ, Li XP,
Wang JL and Wei LH: Overexpression of the insulin receptor isoform
A promotes endometrial carcinoma cell growth. PLoS One.
8:e690012013. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Shehab MA, Biggar K, Singal SS, Nygard K,
Shun-Cheng Li S, Jansson T and Gupta MB: Exposure of decidualized
HIESC to low oxygen tension and leucine deprivation results in
increased IGFBP-1 phosphorylation and reduced IGF-I bioactivity.
Mol Cell Endocrinol. 452:1–14. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Xie Y, Wang JL, Ji M, Yuan ZF, Peng Z,
Zhang Y, Wen JG and Shi HR: Regulation of insulin-like growth
factor signaling by metformin in endometrial cancer cells. Oncol
Lett. 8:1993–1999. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Du J, Shi HR, Ren F, Wang JL, Wu QH, Li X
and Zhang RT: Inhibition of the IGF signaling pathway reverses
cisplatin resistance in ovarian cancer cells. BMC Cancer.
17:8512017. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Cai D, Sun H, Qi Y, Zhao X, Feng M and Wu
X: Insulin-Like growth factor 1/mammalian target of rapamycin and
AMP-Activated protein kinase signaling involved in the effects of
metformin in the human endometrial cancer. Int J Gynecol Cancer.
26:1667–1672. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Cao C, Zhou JY, Xie SW, Guo XJ, Li GT,
Gong YJ, Yang WJ, Li Z, Zhong RH, Shao HH and Zhu Y: Metformin
enhances nomegestrol acetate suppressing growth of endometrial
cancer cells and may correlate to downregulating mTOR activity in
vitro and in vivo. Int J Mol Sci. 20:33082019. View Article : Google Scholar
|
|
76
|
Xu HL, Xu WH, Cai Q, Feng M, Long J, Zheng
W, Xiang YB and Shu XO: Polymorphisms and haplotypes in the
caspase-3, caspase-7, and caspase-8 genes and risk for endometrial
cancer: A population-based, case-control study in a Chinese
population. Cancer Epidemiol Biomarkers Prev. 18:2114–2122. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
77
|
McComb S, Chan PK, Guinot A,
Hartmannsdottir H, Jenni S, Dobay MP, Bourquin JP and Bornhauser
BC: Efficient apoptosis requires feedback amplification of upstream
apoptotic signals by effector caspase-3 or −7. Sci Adv.
5:eaau94332019. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Aral K, Aral CA and Kapila Y: The role of
caspase-8, caspase-9, and apoptosis inducing factor in periodontal
disease. J Periodontol. 90:288–294. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Jang JH, Song IH, Sung EG, Lee TJ and Kim
JY: Metformin-induced apoptosis facilitates degradation of the
cellular caspase 8 (FLICE)-like inhibitory protein through a
caspase-dependent pathway in human renal cell carcinoma A498 cells.
Oncol Lett. 16:2030–2038. 2018.PubMed/NCBI
|
|
80
|
Zhao Y, Luo Q, Mo J, Li J, Ye D, Ao Z,
Chen L and Liu J: Metformin in combination with JS-K inhibits
growth of renal cell carcinoma cells via reactive oxygen species
activation and inducing DNA breaks. J Cancer. 11:3701–3712. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Zhou X, Zhang P and Wang Q, Ji N, Xia S,
Ding Y and Wang Q: Metformin ameliorates experimental diabetic
periodontitis independently of mammalian target of rapamycin (mTOR)
inhibition by reducing NIMA-related kinase 7 (Nek7) expression. J
Periodontol. 90:1032–1042. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Guo Y, Yuan J, Yin S, Wang X, Shuai R and
Kang J: MAP2K6-FP enhances the sensitiveness of paclitaxel for
ovarian cancer via inducing autophagy. Int J Gynecol Cancer.
27:1082–1087. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Giatromanolaki A, Koukourakis MI,
Koutsopoulos A, Chloropoulou P, Liberis V and Sivridis E: High
Beclin 1 expression defines a poor prognosis in endometrial
adenocarcinomas. Gynecol Oncol. 123:147–151. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Bermudez M, Aguilar-Medina M,
Lizarraga-Verdugo E, Avendaño-Félix M, Silva-Benítez E,
López-Camarillo C and Ramos-Payán R: LncRNAs as regulators of
autophagy and drug resistance in colorectal cancer. Front Oncol.
9:10082019. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Ran X, Zhou P and Zhang K: Autophagy plays
an important role in stemness mediation and the novel dual function
of EIG121 in both autophagy and stemness regulation of endometrial
carcinoma JEC cells. Int J Oncol. 51:644–656. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Tomic T, Botton T, Cerezo M, Robert G,
Luciano F, Puissant A, Gounon P, Allegra M, Bertolotto C, Bereder
JM, et al: Metformin inhibits melanoma development through
autophagy and apoptosis mechanisms. Cell Death Dis. 2:e1992011.
View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Zhang D, Xuan J, Zheng BB, Zhou YL, Lin Y,
Wu YS, Zhou YF, Huang YX, Wang Q, Shen LY, et al: Metformin
improves functional recovery after spinal cord injury via autophagy
flux stimulation. Mol Neurobiol. 54:3327–3341. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Takahashi A, Kimura F, Yamanaka A,
Takebayashi A, Kita N, Takahashi K and Murakami T: Metformin
impairs growth of endometrial cancer cells via cell cycle arrest
and concomitant autophagy and apoptosis. Cancer Cell Int.
14:532014. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Zou G, Bai J, Li D and Chen Y: Effect of
metformin on the proliferation, apoptosis, invasion and autophagy
of ovarian cancer cells. Exp Ther Med. 18:2086–2094.
2019.PubMed/NCBI
|
|
90
|
Tseng CH: Metformin and endometrial cancer
risk in Chinese women with type 2 diabetes mellitus in Taiwan.
Gynecol Oncol. 138:147–153. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Franchi M, Asciutto R, Nicotra F, Merlino
L, La Vecchia C, Corrao G and Bosetti C: Metformin, other
antidiabetic drugs, and endometrial cancer risk: A nested
case-control study within Italian healthcare utilization databases.
Eur J Cancer Prev. 26:225–231. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Ko EM, Walter P, Jackson A, Clark L,
Franasiak J, Bolac C, Havrilesky LJ, Secord AA, Moore DT, Gehrig PA
and Bae-Jump V: Metformin is associated with improved survival in
endometrial cancer. Gynecol Oncol. 132:438–442. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Rossi A, Garber CE, Ortiz M, Shankar V,
Goldberg GL and Nevadunsky NS: Feasibility of a physical activity
intervention for obese, socioculturally diverse endometrial cancer
survivors. Gynecol Oncol. 142:304–310. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Clement NS, Oliver TR, Shiwani H, Sanner
JR, Mulvaney CA and Atiomo W: Metformin for endometrial
hyperplasia. Cochrane Database Syst Rev. 10:CD0122142017.PubMed/NCBI
|
|
95
|
Mitsuhashi A, Sato Y, Kiyokawa T,
Koshizaka M, Hanaoka H and Shozu M: Phase II study of
medroxyprogesterone acetate plus metformin as a fertility-sparing
treatment for atypical endometrial hyperplasia and endometrial
cancer. Ann Oncol. 27:262–266. 2016. View Article : Google Scholar : PubMed/NCBI
|