Introduction
Mesothelin is a 40-kDa cell surface glycoprotein
that is expressed on normal mesothelial cells that line the pleura,
pericardium, and peritoneum (1).
Mesothelin is overexpressed in various types of malignant tumors,
including malignant mesothelioma, ovarian cancer, and pancreatic
cancer (2–4). The full-length human mesothelin gene
encodes a 71-kDa precursor protein, which can be physiologically
cleaved by some fern-like proteases into a membrane-bound 40-kDa
C-terminal fragment and a 31-kDa N-terminal fragment, which is
secreted into the blood (5). The
40-kDa C-terminal fragment, mesothelin, is attached to the cell
membrane through a glycosyl-phosphatidylinositol anchor (5,6).
The biological functions of mesothelin are unclear,
although recent studies have suggested that overexpression of
mesothelin increases cell proliferation and migration (7). Furthermore, positive mesothelin
expression (ME) is associated with an unfavorable prognosis in
pancreatic cancer, gastric cancer, and colorectal cancer (4,8–10).
The number of studies on ME in breast cancer is
limited. Wang et al (11)
suggested that the ME level in invasive breast cancer tissue was
inversely correlated with overall survival (OS). Furthermore, based
on subtype classification, Parinyanitikul et al (12) and Bayoglu et al (13) showed that mesothelin was
overexpressed in most triple-negative breast cancers (TNBCs), but
was not correlated with survival outcomes in TNBC. Tchou et
al (14) demonstrated that
ME-positivity was rare and was not correlated with patient outcome
in estrogen receptor (ER)-positive or human epithelial growth
factor receptor type 2 (HER2)-positive breast cancers. Moreover,
Einama et al (9) reported
that the localization of ME was related to OS in gastric cancer. To
the best of our knowledge, there have been no previous studies on
the relationship between the cellular localization of mesothelin
and the prognosis of breast cancer patients.
In this study, we investigated ME in each subtype of
breast cancer using immunohistology, with special reference to its
cellular localization, and analyzed its clinicopathological
significance, including patient outcome.
Materials and methods
Ethics approval and consent to
participate
This study was performed in accordance with the
Declaration of Helsinki and was approved by the Institutional
Review Board of the National Defense Medical College (registration
no. 3003). All patients agreed to participate in this study, and
written informed consent was obtained from all patients.
Patients
The subjects of this study comprised 482 patients
who underwent radical surgery for primary breast cancer between
2002 and 2013. Patients with stage IV and non-primary breast cancer
were excluded. The ER and progesterone receptor (PgR) statuses of
the tumor were assessed using immunohistochemistry and defined as
positive if 1% or more of the constituent carcinoma cells were
immunoreactive. The HER2 status of the tumor was evaluated
immunohistochemically (IHC), and fluorescence in situ hybridization
(FISH) was performed in cases with a score of 2+. HER2 was
considered positive when the IHC score was 3+ or FISH was positive
according to the 2013 American Society of Clinical Oncology/College
of American Pathologists guidelines. The nuclear grade (NG) was
determined by the sum of the nuclear atypia score and the mitosis
count score (15). Ki-67 was
evaluated according to the recommendation of the Breast Cancer
Working Group (16), and the Ki-67
labeling index (LI) was defined as high if 14% or more of the
constituent carcinoma cells were immunoreactive (17). Breast cancers were classified into
four subtypes according to the St. Gallen consensus as follows
(18): Luminal type, ER+ and/or
PgR+/HER2-; luminal HER2 type, ER+ and/or PgR+/HER2+; HER2 type,
ER-/PgR-/HER2+; TNBC type, ER-/PgR-/HER2-.
Immunohistochemistry
Tissue microarrays of 482 breast cancer patients
were used in this study. Sections with a thickness of 4 µm were cut
from formalin-fixed paraffin-embedded tissue blocks and mounted on
charged glass slides, deparaffinized, and rehydrated through a
graded ethanol series. For antigen retrieval, a target retrieval
solution at pH 9.0 (catalogue number, S2368; Dako Japan) was used,
and the slides were boiled in a pressure cooker (Pascal Pressure
Cooker, Model: S2800; Dako) at 125°C for 3 min. Endogenous
peroxidase was blocked with 0.3% hydrogen peroxidase. The slides
were incubated with a 1:50 dilution of a mouse monoclonal antibody
in mesothelin (clone 5B2, diluted 1:50; Novocastra) at room
temperature for 30 min, and then reacted with a dextran polymer
reagent combined with secondary antibodies and peroxidase
(Envision/HRP; Dako) for 30 min at room temperature. Specific
antigen-antibody reactions were visualized with 0.2%
diaminobenzidine tetrahydrochloride and hydrogen peroxide. Slides
were counterstained with hematoxylin for 10 min and then rinsed
gently in reagent quality water.
Immunohistochemical evaluation
All assessments were made on the tumor region of the
specimen (×200). Each slide was independently evaluated by two
observers who were blinded to the clinical outcomes (Y.Y. and
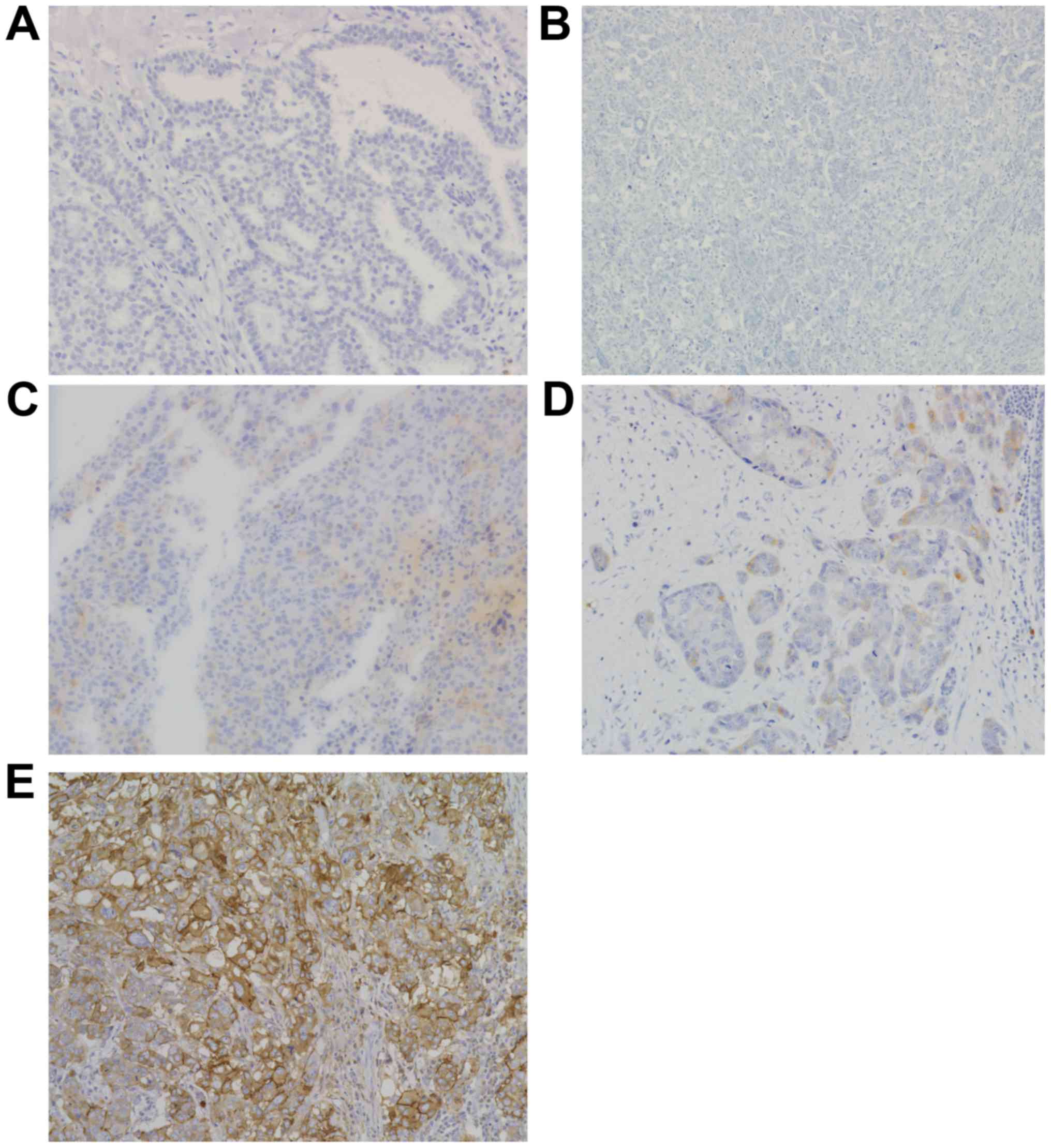
T.E.). Immunostaining for mesothelin was evaluated for both the
proportion and staining intensity of tumor cells in each case. The
proportion of ME-positive cancer cells was assessed as 1–10%,
>10-50%, and >50%. The staining intensity was evaluated as
weak (+1) or moderate to strong (+2). The staining proportion and
intensity were judged separately between the membrane and cytoplasm
(Fig. 1). No mesothelin staining was
observed in the normal breast tissue. ME was defined as positive
when the percentage of positive cells was ≥1% of the tumor cells,
regardless of the intensity. Furthermore, among the ME-positive
cases, the staining localization of mesothelin was evaluated as
membrane, cytoplasm, or both. When the entire circumference of the
membrane was evenly or partially stained throughout the whole
section, ‘membrane mesothelin expression (MME)’ was defined as
positive. When cytoplasmic staining, including cytoplasmic granular
staining, was clearly observed in ≥1% of the tumor cells,
‘cytoplasmic mesothelin expression (CME)’ was defined as
positive.
Statistical analysis
The χ2 test or Fisher's exact test were
used to determine the correlation between ME and
clinicopathological parameters. Survival curves were drawn using
the Kaplan-Meier method, and compared using the log-rank test. The
prognostic implications of these parameters were analyzed using
Cox's univariate and multivariate proportional hazards models. All
differences were considered significant at a P-value <0.05.
Statistical analyses were performed using JMP® 14 (SAS
Institute Inc.).
Results
Clinicopathological analysis of
mesothelin expression
Representative membrane and cytoplasmic ME are shown
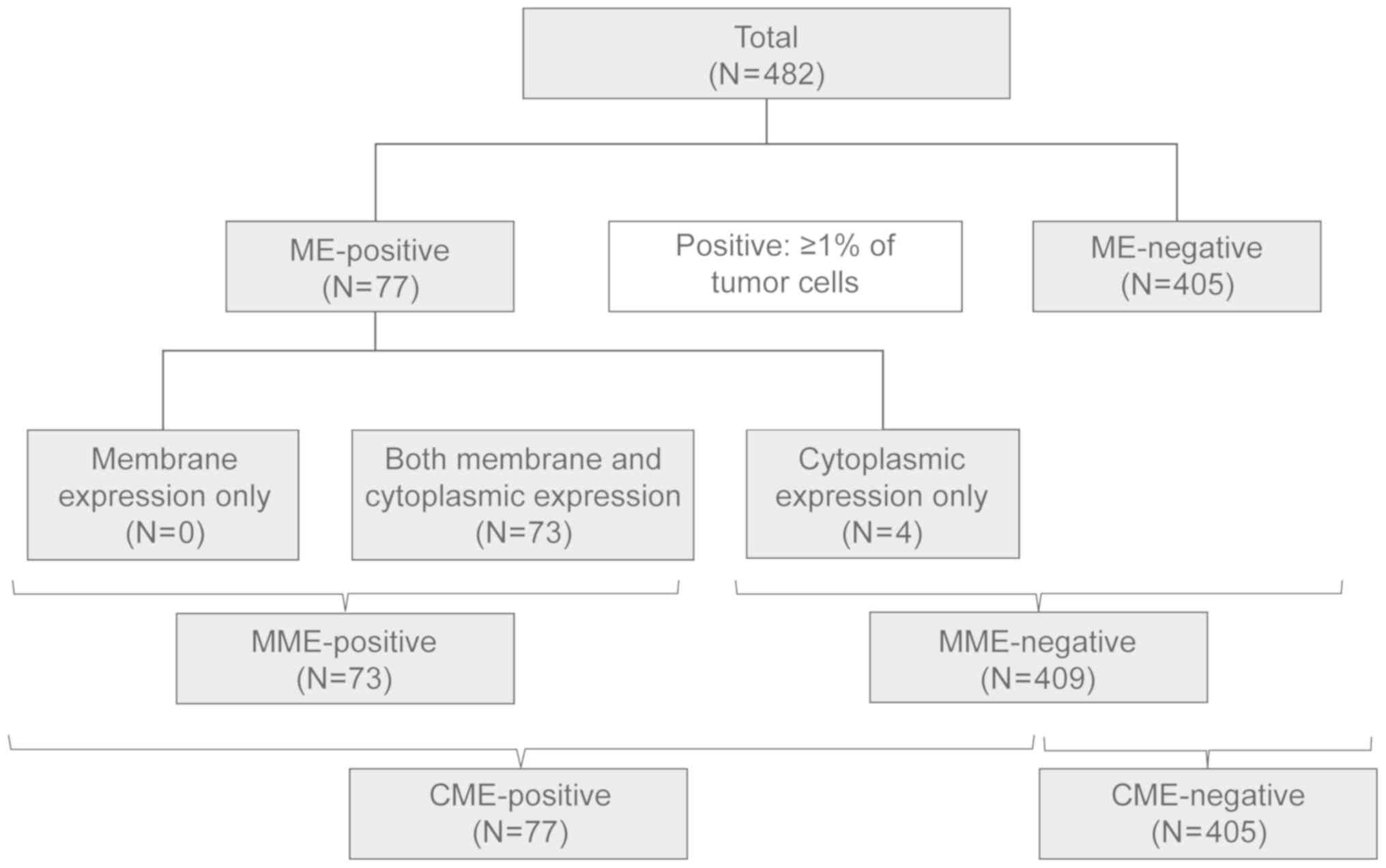
in Fig. 1. Of the 482 breast cancer
tissue samples, ME-positivity was detected in 77 cases (16.0%),
MME-positivity in 73, and CME-positivity in 77, which included all
73 MME-positive cases (Fig. 2).
The total clinicopathological demography of patients
is shown in Table I. The mean
patient age was 59.1 years [±11.3 standard deviation (SD)]. Total
mastectomies were performed on 226 patients (46.9%), and partial
mastectomies were performed on 256 patients (53.1%). Luminal type
breast cancer was the most common (71.2%), followed by TNBC
(15.6%). Neoadjuvant chemotherapy was administered to 31 patients,
while adjuvant chemotherapy was administered to 190 patients
(including administration of trastuzumab to 15 patients). Adjuvant
endocrine therapy was administered to 311 patients, and
postoperative radiation therapy was administered to 209 patients. A
total of 70 patients had a relapse of breast cancer, with a median
relapse-free survival (RFS) of 7.5 years (±3.9 SD).
 | Table I.Demographics of 482 patients with
breast cancer in the present study. |
Table I.
Demographics of 482 patients with
breast cancer in the present study.
| Parameter | Value |
|---|
| Age, years (mean ±
SD) | 59.1±11.3 |
| Surgery, n (%) |
|
|
Mastectomy | 226 (46.9) |
| Partial
resection | 256 (53.1) |
| pT, n (%) |
|
|
Tis | 1 (0.2) |
| T1 | 267 (55.4) |
| T2 | 195 (40.5) |
| T3 | 19 (3.9) |
| pN, n (%) |
|
| N0 | 304 (63.1) |
| N1 | 124 (25.7) |
| N2 | 34 (7.1) |
| N3 | 20 (4.1) |
| Subtype, n (%) |
|
| Luminal
HER2- | 343 (71.2) |
| Luminal
HER2+ | 33 (6.8) |
|
HER2 | 31 (6.4) |
|
TNBC | 75 (15.6) |
| Neoadjuvant
chemotherapy, n (%) |
|
|
Yes | 31 (6.4) |
| No | 451 (93.6) |
| Adjuvant therapy, n
(%) |
|
|
Chemotherapy | 185 (38.4) |
|
Anti-HER2 therapy | 15 (3.1) |
|
Endocrine therapy | 311 (64.5) |
|
Radiation therapy | 209 (43.4) |
| Postoperative
radiation therapy, n (%) |
|
|
Yes | 209 (43.4) |
| No | 273 (56.6) |
| Recurrence, n
(%) |
|
|
Yes | 70 (14.5) |
| No | 412 (85.5) |
| Death, n (%) |
|
|
Yes | 51 (10.6) |
| No | 431 (89.4) |
The correlation between ME and clinicopathological
characteristics is summarized in Table
II. ME was not correlated with age, pT, pN, pStage, lymphatic
invasion (Ly), or vascular invasion (V). ME-positivity was more
frequent in NG 3 cases (58/221, 26.2%) than in NG 1/2 cases
(19/261, 7.3%) (P<0.001), more frequent in ER-negative cases
(43/115, 37.4%) than in ER-positive cases (34/367, 9.3%)
(P<0.001), and more frequent in PgR-negative cases (45/139,
32.4%) than in PgR-positive cases (32/343, 9.3%) (P<0.001). The
mean Ki-67 LI was also higher in ME-positive cases (27.6% ±26.5 SD)
than in negative cases (13.4% ±13.9 SD) (P<0.001), while HER2
positivity was similar between the ME-positive and negative groups.
Neoadjuvant chemotherapy had no significant impact on ME positivity
(P=0.629) or other clinicopathological factors, such as Ki-67.
Furthermore, in these 31 patients, ME was not associated with the
pathological response after neoadjuvant chemotherapy. ME-positivity
was the highest in TNBC (44.0%), followed by HER2 (21.2%), luminal
(10.5%), and luminal HER2 (3.2%) subtypes.
| Table II.Association between mesothelin
expression and clinicopathological parameters in 482 patients with
breast cancer. |
Table II.
Association between mesothelin
expression and clinicopathological parameters in 482 patients with
breast cancer.
|
|
| MME |
| CME |
|
|---|
|
|
|
|
|
|
|
|---|
| Clinicopathological
parameters | Total (n=482) | Positive | Negative | P-value | Positive | Negative | P-value |
|---|
| Age, years (mean ±
SD)a |
| 59.5±11.5 | 59.1±11.3 | 0.766 | 60.1±11.5 | 58.9±11.3 | 0.429 |
| pT, n (%) |
|
|
|
|
|
|
|
|
Tis | 1 | 0 (0.0) | 1 (100.0) | 0.071 | 0 (0.0) | 1 (100.0) | 0.071 |
| T1 | 267 | 32 (12.0) | 235 (88.0) |
| 34 (12.7) | 233 (87.3) |
|
| T2 | 195 | 35 (17.9) | 160 (82.1) |
| 37 (19.0) | 158 (81.0) |
|
| T3 | 19 | 6 (31.6) | 13 (68.4) |
| 6 (31.6) | 13 (68.4) |
|
| pN, n (%) |
|
|
|
|
|
|
|
| N0 | 304 | 45 (14.8) | 259 (85.2) | 0.433 | 49 (16.1) | 255 (83.9) | 0.464 |
| N1 | 124 | 16 (12.9) | 108 (87.1) |
| 16 (12.9) | 108 (87.1) |
|
| N2 | 34 | 8 (23.5) | 26 (76.5) |
| 8 (23.5) | 26 (76.5) |
|
| N3 | 20 | 4 (20.0) | 16 (80.0) |
| 4 (20.0) | 16 (80.0) |
|
| pStage, n (%) |
|
|
|
|
|
|
|
| 0 | 1 | 0 (0.0) | 1 (100.0) | 0.298 | 0 (0.0) | 1 (100.0) | 0.405 |
| 1 | 204 | 28 (13.7) | 176 (86.3) |
| 30 (14.7) | 174 (85.3) |
|
| 2 | 222 | 32 (14.4) | 190 (85.6) |
| 34 (15.3) | 188 (84.7) |
|
| 3 | 55 | 13 (23.6) | 190 (76.4) |
| 13 (23.6) | 42 (76.4) |
|
| NG, n (%) |
|
|
|
|
|
|
|
| 1 | 119 | 12 (10.1) | 107 (89.9) | <0.001 | 13 (10.9) | 106 (89.1) | <0.001 |
| 2 | 142 | 6 (4.2) | 136 (95.8) |
| 6 (4.2) | 136 (95.8) |
|
| 3 | 221 | 55 (24.9) | 166 (75.1) |
| 58 (26.2) | 163 (73.8) |
|
| Ly, n (%) |
|
|
|
|
|
|
|
|
Negative | 197 | 31 (15.7) | 166 (84.3) | 0.764 | 31 (15.7) | 166 (84.3) | 0.965 |
|
Positive | 285 | 42 (14.7) | 243 (85.3) |
| 46 (16.1) | 239 (83.9) |
|
| V, n (%) |
|
|
|
|
|
|
|
|
Negative | 312 | 48 (15.4) | 264 (84.6) | 0.843 | 51 (16.3) | 261 (83.7) | 0.763 |
|
Positive | 170 | 25 (14.7) | 145 (85.3) |
| 26 (15.3) | 144 (84.7) |
|
| ER, n (%) |
|
|
|
|
|
|
|
|
Negative | 115 | 40 (34.8) | 75 (65.2) | <0.001 | 43 (37.4) | 72 (62.6) | <0.001 |
|
Positive | 367 | 33 (9.0) | 334 (91.0) |
| 34 (9.3) | 333 (90.7) |
|
| PgR, n (%) |
|
|
|
|
|
|
|
|
Negative | 154 | 42 (27.3) | 112 (72.7) | <0.001 | 45 (29.2) | 109 (70.8) | <0.001 |
|
Positive | 328 | 31 (9.5) | 297 (90.5) |
| 32 (9.8) | 296 (90.2) |
|
| HER2, n (%) |
|
|
|
|
|
|
|
|
Negative | 418 | 66 (15.8) | 352 (84.2) | 0.313 | 69 (16.5) | 349 (83.5) | 0.415 |
|
Positive | 64 | 7 (10.9) | 57 (89.1) |
| 8 (12.5) | 56 (87.5) |
|
| Ki-67 labeling
index, % (mean ± SD)a |
| 28.7±26.7 | 13.4±13.8 | <0.001 | 27.6±26.5 | 13.4±13.9 | <0.001 |
| <14,
n (%) | 301 | 31 (10.3) | 270 (89.7) | <0.001 | 34 (11.3) | 267 (88.7) | <0.001 |
| ≥14, n
(%) | 181 | 42 (23.2) | 139 (76.8) |
| 43 (23.8) | 138 (76.2) |
|
| Neoadjuvant
chemotherapy, n (%) |
|
|
|
|
|
|
|
|
Yes | 31 | 4 (12.9) | 27 (87.1) | 0.719 | 4 (12.9) | 27 (87.1) | 0.629 |
| No | 451 | 69 (15.3) | 382 (84.7) |
| 73 (16.2) | 378 (83.8) |
|
| Subtype, n (%) |
|
|
|
|
|
|
|
| Luminal
type | 343 | 35 (10.2) | 308 (89.8) | <0.001 | 36 (10.5) | 307 (89.5) | <0.001 |
| Luminal
HER2 type | 31 | 1 (3.2) | 30 (96.8) |
| 1 (3.2) | 30 (96.8) |
|
| HER2
type | 33 | 6 (18.2) | 27 (81.8) |
| 7 (21.2) | 26 (78.8) |
|
| TNBC
type | 75 | 31 (41.3) | 44 (58.7) |
| 33 (44.0) | 42 (56.0) |
|
Survival analysis associated with
mesothelin expression
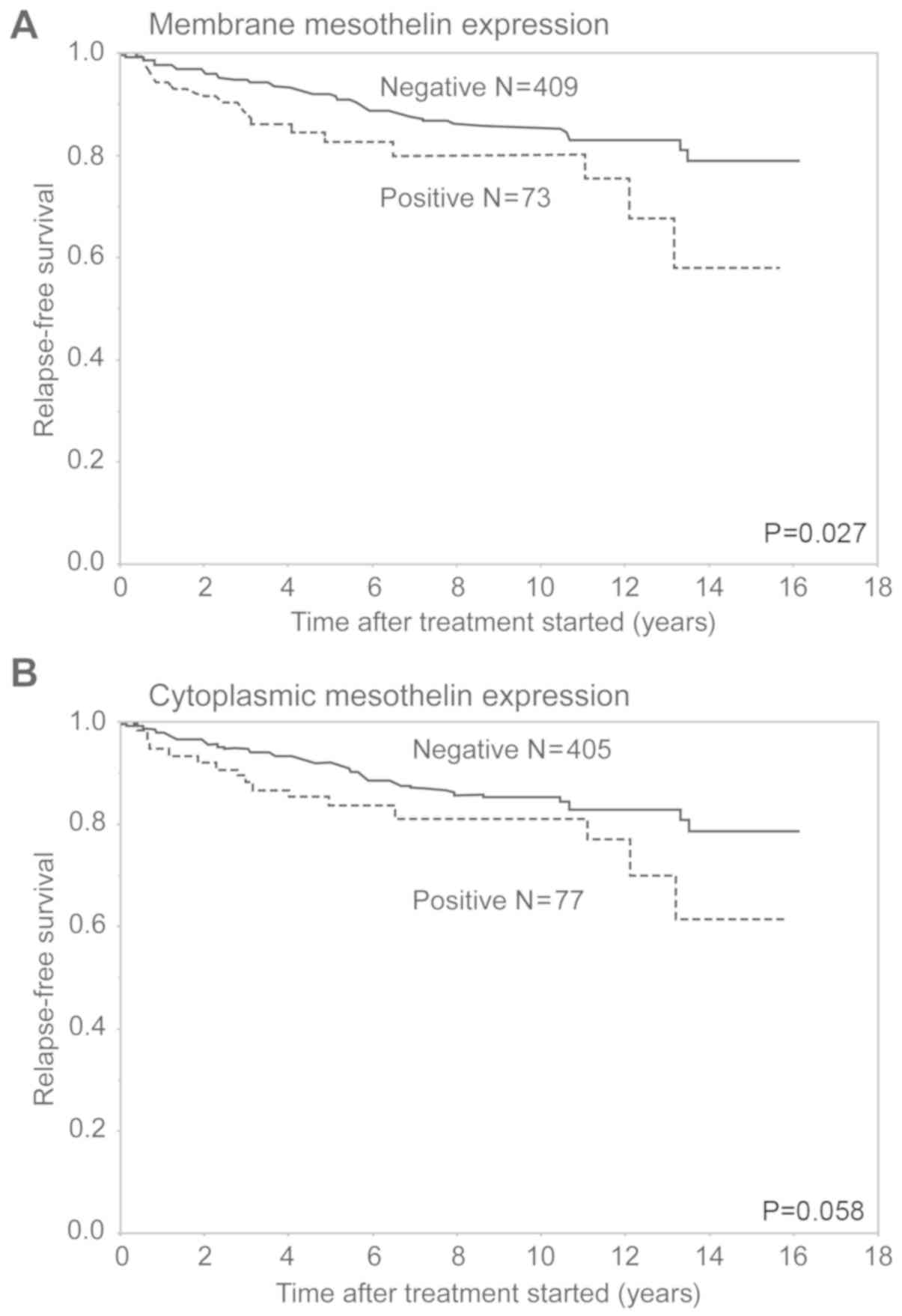
In analysis of RFS, the MME-positive group had a
significantly worse outcome than the MME-negative group (P=0.027).
In contrast, the CME-positive group had a relatively worse RFS than
the CME-negative group (P=0.058) (Fig.
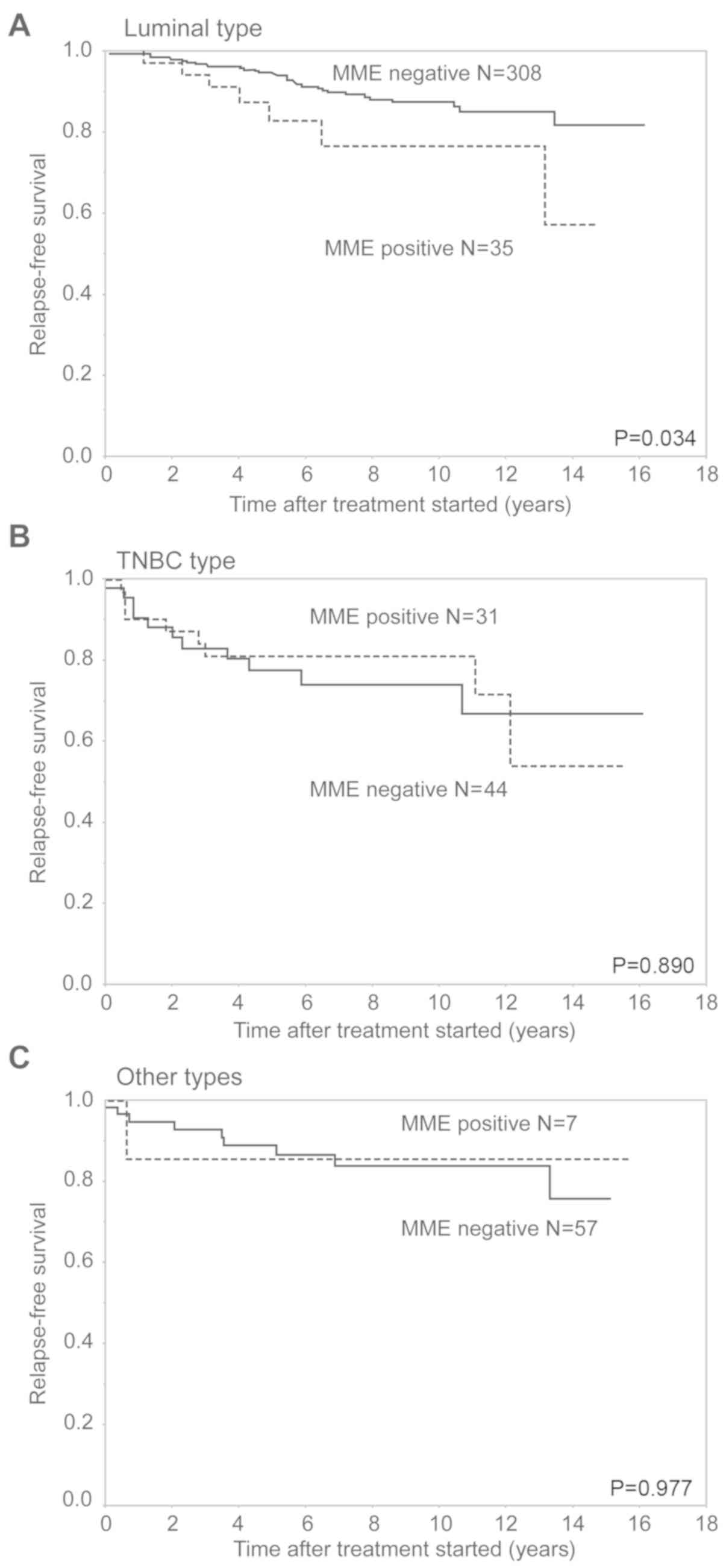
3). In the analysis of the luminal subtype, the MME-positive
group had a significantly worse prognosis than the MME-negative
group (P=0.034). The 5-year RFS rates of the MME-positive and
negative groups with luminal subtype were 82.6 and 94.1%,
respectively. There were no significant differences in RFS curves
between the MME-positive and negative patients in the TNBC subtype
and other subtypes. The 5-year RFS rates of the ME-positive and
negative groups were 80.7 and 77.5% with TNBC, and 85.7 and 88.8%
with the other types, respectively (Fig.
4).
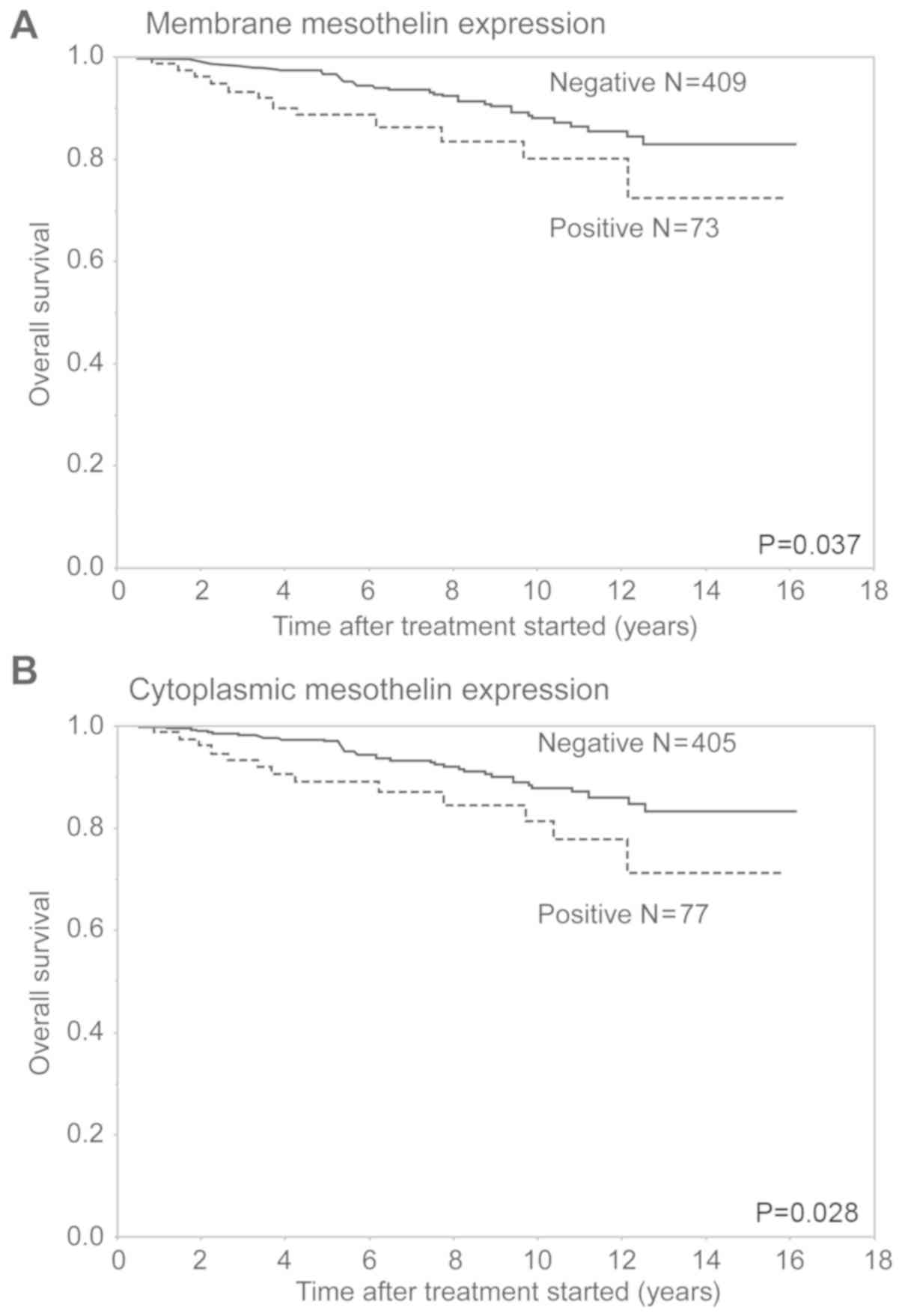
In terms of OS, the MME-positive and CME-positive
groups had a significantly worse outcome than the corresponding
MME-negative and CME-negative groups, respectively (P=0.037 and
P=0.028, respectively) (Fig. 5).
There was no significant difference in OS curves between the
MME-positive and negative patients in any of the included subtypes.
In the analysis of the luminal subtype, the MME-positive group had
a relatively worse prognosis than the MME-negative group
(P=0.068).
We performed univariate analyses of all 482 cases
using the Cox proportional hazards model and found that pT, pN, Ly,
V, ER, PgR, Ki-67 LI, NG and MME significantly correlated with the
risk of relapse, whereas CME did not correlate with RFS.
Furthermore, in Cox multivariate analysis, pT and pN were finally
chosen as independent prognostic factors for RFS (Table III). In addition, Cox's univariate
and multivariate analyses were performed for the 343 luminal type
cases (Table IV). Univariate
analyses showed that pT, pN, Ly, V and NG significantly correlated
with the risk of relapse, whereas MME had no independent impact
(P=0.062). In multivariate analysis, pT and pN were independent
prognostic factors for RFS.
| Table III.Cox's univariate and multivariate
analysis including clinicopathological parameters and mesothelin
expression of recurrence-free survival in 482 patients with breast
cancer. |
Table III.
Cox's univariate and multivariate
analysis including clinicopathological parameters and mesothelin
expression of recurrence-free survival in 482 patients with breast
cancer.
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Parameter | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| pT |
|
|
|
|
| Tis,
T1 | 1 | <0.001 | 1 | 0.003 |
| T2,
T3 | 3.64
(2.19–6.32) |
| 2.27
(1.31–4.08) |
|
| pN |
|
|
|
|
|
Negative | 1 | <0.001 | 1 | 0.002 |
|
Positive | 3.76
(2.30–6.35) |
| 2.78
(1.61–4.84) |
|
| NG |
|
|
|
|
|
1,2 | 1 | <0.001 | 1 | 0.471 |
| 3 | 2.26
(1.40–3.73) |
| 1.04
(0.57–1.92) |
|
| Ly |
|
|
|
|
|
Negative | 1 | 0.002 | 1 | 0.646 |
|
Positive | 2.32
(1.34–4.27) |
| 1.16
(0.63–2.22) |
|
| V |
|
|
|
|
|
Negative | 1 | 0.003 | 1 | 0.066 |
|
Positive | 2.05
(1.28–3.30) |
| 1.59
(0.97–2.60) |
|
| ER |
|
|
|
|
|
Negative | 1 | 0.003 | 1 | 0.497 |
|
Positive | 0.47
(0.29–0.77) |
| 0.72
(0.35–1.68) |
|
| PgR |
|
|
|
|
|
Negative | 1 | 0.007 | 1 | 0.412 |
|
Positive | 0.52
(0.32–0.84) |
| 0.72
(0.35–1.61) |
|
| Ki-67 labeling
index, % |
|
|
|
|
|
<14 | 1 | 0.035 | 1 | 0.374 |
|
≥14 | 1.68
(1.04–2.69) |
| 1.26
(0.75–2.10) |
|
| MME |
|
|
|
|
|
Negative | 1 | 0.040 | 1 | 0.659 |
|
Positive | 1.86
(1.03–3.17) |
| 1.11
(0.57–2.07) |
|
| CME |
|
|
|
|
|
Negative | 1 | 0.075 |
|
|
|
Positive | 1.71
(0.94–2.91) |
|
|
|
| Table IV.Cox's univariate and multivariate
analysis including clinicopathological parameters and mesothelin
expression of recurrence-free survival in 343 patients with luminal
type breast cancer. |
Table IV.
Cox's univariate and multivariate
analysis including clinicopathological parameters and mesothelin
expression of recurrence-free survival in 343 patients with luminal
type breast cancer.
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Parameter | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| pT |
|
|
|
|
| Tis,
T1 | 1 | <0.001 | 1 | 0.011 |
| T2,
T3 | 4.82
(2.45–10.35) |
| 2.58
(1.24–5.79) |
|
| pN |
|
|
|
|
|
Negative | 1 | <0.001 | 1 | <0.001 |
|
Positive | 6.58
(3.26–14.71) |
| 4.74
(2.27–10.91) |
|
| NG |
|
|
|
|
| 1,
2 | 1 | 0.003 | 1 | 0.185 |
| 3 | 2.62
(1.41–4.86) |
| 1.55
(0.81–2.98) |
|
| Ly |
|
|
|
|
|
Negative | 1 | 0.024 | 1 | 0.923 |
|
Positive | 2.18
(1.10–4.71) |
| 1.04
(0.51–2.27) |
|
| V |
|
|
|
|
|
Negative | 1 | 0.005 | 1 | 0.113 |
|
Positive | 2.45
(1.32–4.58) |
| 1.68
(0.88–3.21) |
|
| Ki-67 labeling
index, % |
|
|
|
|
|
<14 | 1 | 0.113 |
|
|
|
≥14 | 1.72
(0.87–3.25) |
|
|
|
| MME |
|
|
|
|
|
Negative | 1 | 0.062 |
|
|
|
Positive | 2.35
(0.95–5.02) |
|
|
|
| CME |
|
|
|
|
|
Negative | 1 | 0.067 |
|
|
|
Positive | 2.31
(0.94–4.93) |
|
|
|
Discussion
In the current study, breast cancer cases were
divided into ME-positive and ME-negative groups. In the ME-positive
cases, the cellular localization was further divided into MME and
CME, and the relationship between ME patterns and
clinicopathological factors, including prognosis, was
retrospectively investigated. Our results demonstrated that ME was
related to conventional prognostic factors, including negative ER,
negative PgR, higher Ki-67 LI, and higher NG. Furthermore, we
revealed that MME-positivity was associated with lower RFS and OS
rates. These results suggest that ME-positivity was an unfavorable
prognostic factor in patients with breast cancer, as well as some
other cancer types (4,8–10).
In the present study, we showed that MME in the
luminal type, but not in other subtypes, was significantly
associated with poor RFS. Several previous studies have reported
that the ME-positive rates in TNBC were 30–40%, which was in
agreement with the results of our study (12–14,19).
TNBC has a relatively higher relapse rate and worse OS rates than
the other subtypes of breast cancer (20). Moreover, since there are few
effective therapies that can improve the prognosis of TNBC
patients, mesothelin has been researched as a potential candidate
for targeted therapies. However, whether ME correlates with
survival outcomes in TNBC remains unclear (12).
However, there were few studies on the
clinicopathological implications of ME in the luminal type, which
comprises 60–70% of all breast cancers. In the luminal type, the
frequency of ME-positivity was lower than that of TNBC (10.2 vs.
41.3%); however, MME-positivity was associated with a lower RFS
rate, and consequently, MME might be useful as a biomarker to
predict poor prognosis in luminal type breast cancer. In this
group, Cox's multivariate analysis indicated that pT and pN were
independent prognostic factors, whereas MME was not, likely because
it was strongly related to biological factors, such as negative ER,
negative PgR, a higher Ki-67 LI, and a higher NG, and not to
anatomical factors, such as pT and pN. These results suggest that
MME was not superior to pT and pN as a prognostic factor. ME was
defined positive when the percentage of positive cells was ≥1% of
tumor cells in this study. If we had defined ME-positivity more
strictly, MME could have become an independent prognostic factor.
Therefore, additional studies are necessary to determine whether ME
can be used as a powerful prognostic factor.
The biological function of mesothelin remains
unclear. Recent studies have suggested that overexpression of
mesothelin increased cell proliferation and migration (7,21).
Moreover, it has also been suggested that mesothelin can elicit
cytotoxic T lymphocyte (CTL) responses, and could efficiently
activate CTL to lyse human tumors. Previous studies have shown that
response to chemotherapy was improved in patients with pancreatic
cancer and other solid cancers using amatuximab, a chimeric
monoclonal antibody that targets mesothelin (22,23).
TNBC is considered a good target of immunotherapy, and Tchou et
al (14) reported that
genetically modified T-cells expressing a chimeric antibody
receptor (CAR) specific for mesothelin (mesoCAR T-cells) had high
anti-tumor cytotoxicity. In the present study, we showed that the
target for molecular target therapy could be expanded to the
luminal type.
We demonstrated that MME-positivity was
significantly associated with RFS and that CME-positive patients
had relatively worse RFS. Both MME and CME are significantly
related to OS, and previous studies have shown that MME-positivity
was a poorer prognostic factor than CME in various cancer types
(4,8–10,21).
Furthermore, Kawamata et al (21) presumed that mesothelin in the
cytoplasm was in the 71 kDa precursor form and might behave in a
dominant-negative manner as a tumor suppressor in extrahepatic bile
duct cancer. In this study, there were only four cases of
cytoplasmic-only ME, and additional studies in a greater number of
cases are required to prove this hypothesis in breast cancer.
In conclusion, we suggest that MME-positivity in
breast cancer, especially in luminal type, is associated with
poorer clinical outcomes. The clinical utility of the
immunohistochemical examination of ME in surgically resected tumor
specimens is expected to be useful for prognostication and decision
making with regards to further treatment procedures after surgical
therapy in breast cancer patients.
Acknowledgements
Not applicable.
Funding
Data extraction and analysis were supported by JSPS
KAKENHI (grant no. JP 18K07340). JSPS did not influence the study
design, data collection, data analysis, data interpretation or
writing of the manuscript.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
TK, TY, MFK, YI, YT and TSh collected the data and
assisted in data analysis. YM, TI, ES and KS contributed to
interpretation of data and manuscript preparation. TSu analyzed the
data and wrote the original draft. YY, TE and HT conceived the
study and reviewed and revised the manuscript. JY and YK made
substantial contributions to the conception and design. HU made
substantial contributions to analysis and interpretation of data.
JY, YK and HU provided supervision of the manuscript. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was performed in accordance with
the Declaration of Helsinki, and was approved by the Institutional
Review Board of the National Defense Medical College (registration
no. 3003). All patients agreed to participate in the present study,
and written informed consent was obtained from all patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
CAR
|
chimeric antibody receptor
|
|
CME
|
cytoplasmic mesothelin expression
|
|
CTL
|
cytotoxic T lymphocytes
|
|
ER
|
estrogen receptor
|
|
FISH
|
fluorescence in situ
hybridization
|
|
HER2
|
human epithelial growth factor
receptor type 2
|
|
IHC
|
immunohistochemically
|
|
LI
|
labeling index
|
|
Ly
|
lymphatic invasion
|
|
ME
|
mesothelin expression
|
|
MME
|
membrane mesothelin expression
|
|
NG
|
nuclear grade
|
|
OS
|
overall survival
|
|
PgR
|
progesterone receptor
|
|
RFS
|
relapse-free survival
|
|
TNBCs
|
triple-negative breast cancers
|
|
V
|
vascular invasion
|
References
|
1
|
Chang K, Pastan I and Willingham MC:
Isolation and characterization of a monoclonal antibody, K1,
reactive with ovarian cancers and normal mesothelium. Int J Cancer.
50:373–381. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Argani P, Iacobuzio-Donahue C, Ryu B,
Rosty C, Goggins M, Wilentz RE, Murugesan SR, Leach SD, Jaffee E,
Yeo CJ, et al: Mesothelin is overexpressed in the vast majority of
ductal adenocarcinomas of the pancreas: Identification of a new
pancreatic cancer marker by serial analysis of gene expression
(SAGE). Clin Cancer Res. 7:3862–3868. 2001.PubMed/NCBI
|
|
3
|
Ordonez NG: Value of mesothelin
immunostaining in the diagnosis of mesothelioma. Mod Pathol.
16:192–197. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Einama T, Kamachi H, Nishihara H, Homma S,
Kanno H, Takahashi K, Sasaki A, Tahara M, Okada K, Muraoka S, et
al: Co-expression of mesothelin and CA125 correlates with
unfavorable patient outcome in pancreatic ductal adenocarcinoma.
Pancreas. 40:1276–1282. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chang K and Pastan I: Molecular cloning of
mesothelin, a differentiation antigen present on mesothelium,
mesotheliomas, and ovarian cancers. Proc Natl Acad Sci USA.
93:136–140. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hassan R, Bera T and Pastan I: Mesothelin:
A new target for immunotherapy. Clin Cancer Res. 10:3937–3942.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Li M, Bharadwaj U, Zhang R, Zhang S, Mu H,
Fisher WE, Brunicardi FC, Chen S and Yao Q: Mesothelin is a
malignant factor and therapeutic vaccine target for pancreatic
cancer. Mol Cancer Ther. 7:286–296. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shiraishi T, Shinto E, Mochizuki S, Tsuda
H, Kajiwara Y, Okamoto K, Einama T, Hase K and Ueno H: Mesothelin
expression has prognostic value in stage II/III colorectal cancer.
Virchows Arch. 474:297–307. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Einama T, Homma S, Kamachi H, Kawamat F,
Takahashi K, Takahashi N, Taniguchi M, Kamiyama T, Furukawa H,
Matsuno Y, et al: Luminal membrane expression of mesothelin is a
prominent poor prognostic factor for gastric cancer. Br J Cancer.
107:137–142. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Shiraishi T, Shinto E, Nearchou IP, Tsuda
H, Kajiwara Y, Einama T, Caie PD, Kishi Y and Ueno H: Prognostic
significance of mesothelin expression in colorectal cancer
disclosed by area-specific four-point tissue microarrays. Virchows
Arch. Feb 27–2020.(Epub ahead of print). doi:
10.1007/s00428-020-02775-y. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wang L, Niu Z, Zhang L, Liu X, Wang X, Li
F and Wang Y: Clinicopathological significance of mesothelin
expression in invasive breast cancer. J Int Med Res. 40:909–916.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Parinyanitikul N, Blumenschein GR, Wu Y,
Lei X, Chavez-Macgregor M, Smart M and Gonzalez-Angulo AM:
Mesothelin expression and survival outcomes in triple receptor
negative breast cancer. Clin Breast Cancer. 13:378–384. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bayoglu IV, Kucukzeybek BB, Kucukzeybek Y,
Varol U, Yildiz I, Alacacioglu A, Akyol M, Demir L, Dirican A and
Yildiz Y: Prognostic value of mesothelin expression in patients
with triple negative and HER2-positive breast cancers. Biomed
Pharmacother. 70:190–195. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Tchou J, Wang LC, Selven B, Zhang H,
Conejo-Garcia J, Borghaei H, Kalos M, Vondeheide RH, Albelda SM,
June CH and Zhang PJ: Mesothelin, a novel immunotherapy target for
triple negative breast cancer. Breast Cancer Res Treat.
133:799–804. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Tsuda H, Akiyama F, Kurosumi M, Sakamoto G
and Watanabe T: Establishment of histological criteria for
high-risk node-negative breast carcinoma for a multi-institutional
randomized clinical trial of adjuvant therapy. Japan National
Surgical Adjuvant Study of Breast Cancer (NSAS-BC) pathology
section. Jpn J Clin Oncol. 28:486–491. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Dowsett M, Nielsen TO, A'Hern R, Bartlett
J, Coombes RC, Cuzick J, Ellis M, Henry NL, Hugh JC, Lively T, et
al: Assessment of Ki67 in breast cancer: Recommendations from the
international Ki67 in Breast Cancer working group. J Natl Cancer
Inst. 103:1656–1664. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Cheang MC, Chia SK, Voduc D, Gao D, Leung
S, Snider J, Watson M, Davies S, Bernard PS, Parker JS, et al: Ki67
index, HER2 status, and prognosis of patients with luminal B breast
cancer. J Natl Cancer Inst. 101:736–750. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Curigliano G, Burstein HJ, Winer EP, Gnant
M, Dubsky P, Loibl S, Colleoni M, Regan MM, Piccart-Gebhart M, Senn
HJ, et al: De-escalating and escalating treatments for early-stage
breast cancer: The St. Gallen international expert consensus
conference on the primary therapy of early breast cancer 2017. Ann
Oncol. 30:11812019. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wang M, Li A, Sun G, Mbuagbaw L, Reid S,
Lovrics PJ and Thabane L: Association between mesothelin expression
and survival outcomes in patients with triple-negative breast
cancer: A protocol for a systematic review. Syst Rev. 5:1332016.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tan AR and Swain SM: Therapeutic
strategies for triple-negative breast cancer. Cancer J. 14:343–351.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kawamata F, Kamachi H, Einama T, Homma S,
Tahara M, Miyazaki M, Tanaka S, Kamiyama T, Nishihara H, Taketomi A
and Todo S: Intracellular localization of mesothelin predicts
patient prognosis of extrahepatic bile duct cancer. Int J Oncol.
41:2109–2118. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mizukami T, Kamachi H, Fujii Y, Matsuzawa
F, Einama T, Kawamata F, Kobayashi N, Hatanaka Y and Taketomi A:
The anti-mesothelin monoclonal antibody amatuximab enhances the
anti-tumor effect of gemcitabine against mesothelin-high expressing
pancreatic cancer cells in a peritoneal metastasis mouse model.
Oncotarget. 9:33844–33852. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Fujisaka Y, Kurata T, Tanaka K, Kudo T,
Okamoto K, Tsurutani J, Kaneda H, Okamoto I, Namiki M, Kitamura C
and Nakagawa K: Phase I study of amatuximab, a novel monoclonal
antibody to mesothelin, in Japanese patients with advanced solid
tumors. Invest New Drugs. 33:380–388. 2015. View Article : Google Scholar : PubMed/NCBI
|