Introduction
Liver cancer is the sixth most commonly diagnosed
cancer worldwide and ranks among the top four leading causes of
cancer-associated deaths in 2018 (1). It is estimated that both incidences and
deaths caused by liver cancer will increase in the United States
during the next ten years, resulting in liver cancer becoming the
third leading cause of cancer-associated mortality by 2030
(2). Although ultrasound and
optional combination of alpha-fetoprotein (AFP) testing have
enabled the regular screening of liver cancer among at-risk
individuals (3), biomarkers are
urgently required for early diagnosis and better prognostic
classification; which is essential for optimal treatment strategies
(4,5).
β-site APP-cleaving enzyme 1 (BACE1) is a key
β-secretase enzyme that initiates the formation of β-amyloid (Aβ)
peptide, which is the central player in the pathogenesis of
Alzheimer's disease (AD) (6). The
expression levels, and the enzymatic activities of BACE1 protein,
as well as BACE1 SNP, have been reported to be associated
with specific clinical features, for example, patients with
Alzheimer's disease tend to have higher brain BACE1 levels compared
with normal controls (7–9). A long non-coding RNA (lncRNA)
BACE1 antisense (BACE1-AS, also known as
BACE1-AS1) was identified in 2008 as a regulator of
BACE1 expression by increasing BACE1 mRNA stability,
and whose deregulation is crucial in AD (10). Although BACE1-AS is
universally expressed in various tissues including in malignancies,
such as ovarian cancer (11), its
functions in cancer have thus far remained largely unknown
(11,12).
Based on data extracted from The Cancer Genome Atlas
(TCGA) database, the present study investigated the roles of
BACE1-AS in a liver cancer cohort. It was found that
BACE1-AS is highly expressed in liver cancer and that
BACE1-AS expression is an independent prognostic factor of
overall survival (OS) and relapse-free survival (RFS) in patients
with liver cancer.
Materials and methods
TCGA data mining
The RNA-Seq expression data and clinical information
of patients (mean average=61 years; range, 16–90 years) with liver
cancer were downloaded and based upon data generated by TCGA
Research Network: https://www.cancer.gov/tcga. A total of 371 patients
were included for the study including 121 female and 250 male
patients. RNA-Seq by Expectation-Maximization (RSEM) (13) was used for accurate transcript
abundance quantification, and the resulting values were used for
subsequent statistical analysis. The age cut-off was set as 55:
Young (aged <55 years) and old patients (aged ≥55 years). The
grading system used was Edmondson grade (14). The TNM staging system refers to the
newest NCCN guidelines (15).
Statistical analysis
All statistical analyses were performed using R
(version 3.5.1) (16). Differential
expression within a category was analyzed using nonparametric
Wilcoxon rank sum test and Kruskal-Wallis test, depending on the
numbers of variables tested. Receiver-operating characteristic
curve (ROC) was drawn by the pROC package to evaluate the
diagnostic capability, and Youden's J index was used for
determining the threshold value for dividing patients into
BACE1-AS high and BACE1-AS low groups. Fisher's exact
or Pearson's χ2 test was applied to study the
association between BACE1-AS expression and the clinical
characteristics of patients. Survival analysis was performed with
Kaplan-Meier curves using the survival package in R (17); the statistical significance was
assessed using the log-rank test. Univariate and multivariate Cox
regression analyses were performed using Cox proportional hazard
models. Data visualization was performed using the ggplot2 package
in R (18). P<0.05 was considered
to indicate a statistically significant difference.
Results
Patients' characteristics
A total of 370 patients along with their RNA-Seq
data were included for analysis in the present study. The patients
were followed up for ten years and their information, such as
histological types, stages and vital status were summarized and
detailed in Table I.
 | Table I.Clinical characteristics of the
patients included in the present study. |
Table I.
Clinical characteristics of the
patients included in the present study.
| Characteristics | Number of patients
(%) |
|---|
| Age, years |
|
|
<55 | 117 (31.54) |
|
≥55 | 253 (68.19) |
| NA | 1 (0.27) |
| Sex |
|
|
Female | 121 (32.61) |
|
Male | 250 (67.39) |
| Histological
type |
|
|
Fibrolamellar carcinoma | 3 (0.81) |
|
Hepatocellular carcinoma | 361 (97.3) |
|
Hepatocholangiocarcinoma | 7 (1.89) |
| Edmondson
grade |
|
| G1 | 55 (14.82) |
| G2 | 177 (47.71) |
| G3 | 122 (32.88) |
| G4 | 12 (3.23) |
| NA | 5 (1.35) |
| TNM stage |
|
| I | 171 (46.09) |
| II | 86 (23.18) |
|
III | 85 (22.91) |
| IV | 5 (1.35) |
| NA | 24 (6.47) |
| T
classification |
|
| T1 | 181 (48.79) |
| T2 | 94 (25.34) |
| T3 | 80 (21.56) |
| T4 | 13 (3.5) |
| TX | 1 (0.27) |
| NA | 2 (0.54) |
| N
classification |
|
| N0 | 252 (67.92) |
| N1 | 4 (1.08) |
| NX | 114 (30.73) |
| NA | 1 (0.27) |
| M
classification |
|
| M0 | 266 (71.7) |
| M1 | 4 (1.08) |
| MX | 101 (27.22) |
| Radiation
therapy |
|
| No | 338 (91.11) |
|
Yes | 8 (2.16) |
| NA | 25 (6.74) |
| Residual tumor |
|
| R0 | 324 (87.33) |
| R1 | 17 (4.58) |
| R2 | 1 (0.27) |
| RX | 22 (5.93) |
| NA | 7 (1.89) |
| Vital status |
|
|
Deceased | 130 (35.04) |
|
Living | 241 (64.96) |
| Relapse |
|
| No | 179 (48.25) |
|
Yes | 139 (37.47) |
| NA | 53 (14.28) |
| BACE1-AS1 |
|
|
High | 153 (41.24) |
|
Low | 218 (58.76) |
BACE1-AS is overexpressed in liver
cancer and the levels of which varies among different
subgroups
The abundances of BACE1-AS transcript were
analyzed in all patients included in the present study and were
further compared within different categories (Fig. 1). BACE1-AS was highly elevated
in liver cancer tissues compared with healthy liver tissues
(P<2.210−16). Furthermore, a significant difference
was observed among patients with different histological grades,
with a trend of higher levels of expression corresponding to
advanced histological grades (P=7.910−6). The analysis
of patients at different tumor stages also presented with the
aforementioned trend, with an exception at stage IV where the
levels of BACE1-AS displayed a sudden fall (P=0.0079). A
similar trend was also observed in the tumor size staging
classification subgroups (T classification; P=0.017). Notably, when
patients were divided according to histological types, there was a
trend of higher levels of BACE1-AS in the mixed
hepatocellular carcinoma (HCC)/hepatocellular cholangiocarcinoma
(CAA) compared with HCC alone; the P-value indicated a
near-significant trend overall (P=0.063).
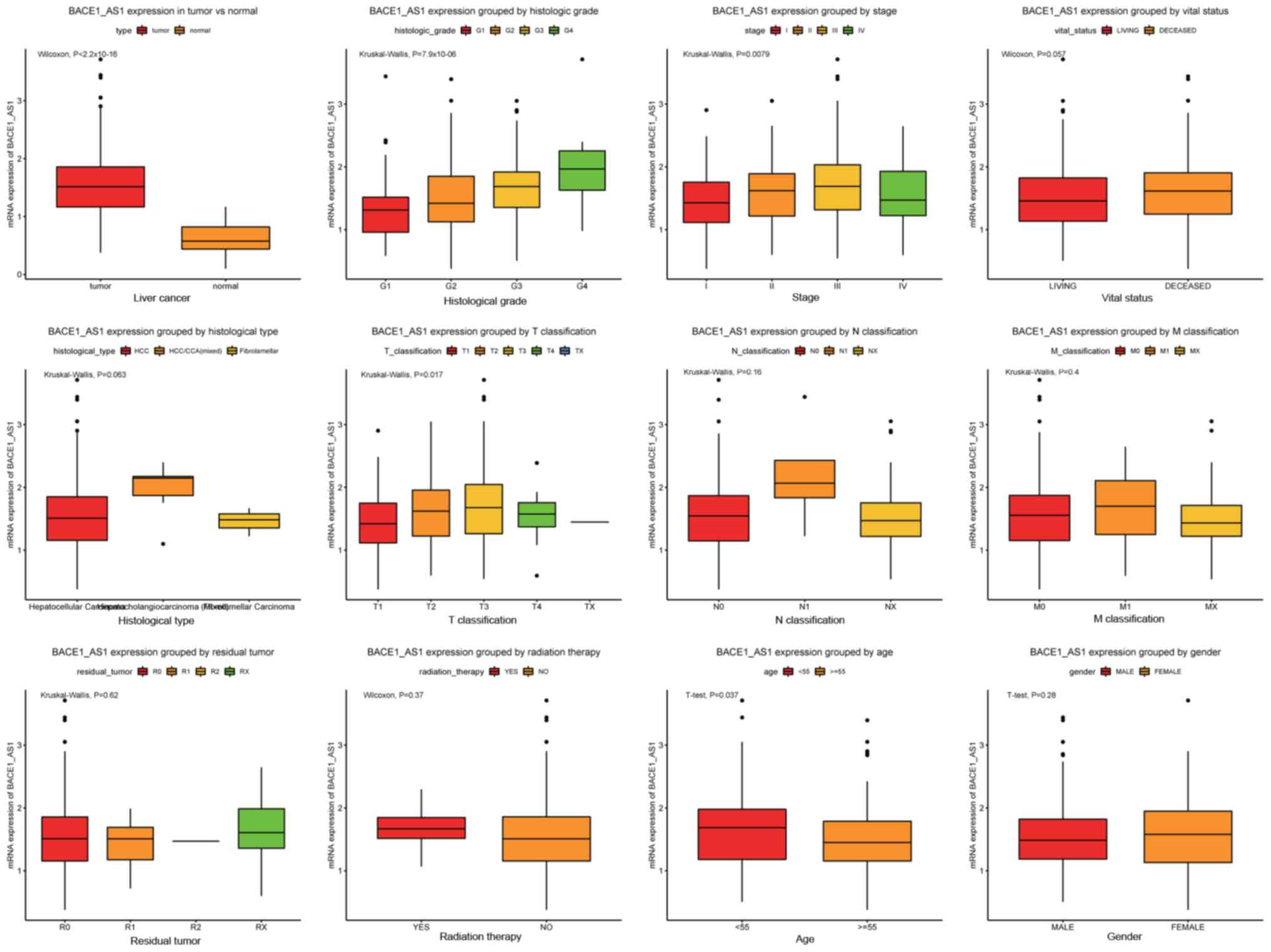 | Figure 1.BACE1-AS is overexpressed in liver
cancer and is differentially expressed in various subtypes. The
significance was calculated based on nonparametric Wilcoxon and
Kruskal-Wallis tests. The subgroups include tumors vs. healthy
liver tissue, histological grades, stages, vital status,
histological types, T classification, N classification, M
classification, residual tumor, radiation therapy, age and sex.
BACE1-AS, β-site APP-cleaving enzyme 1 antisense. |
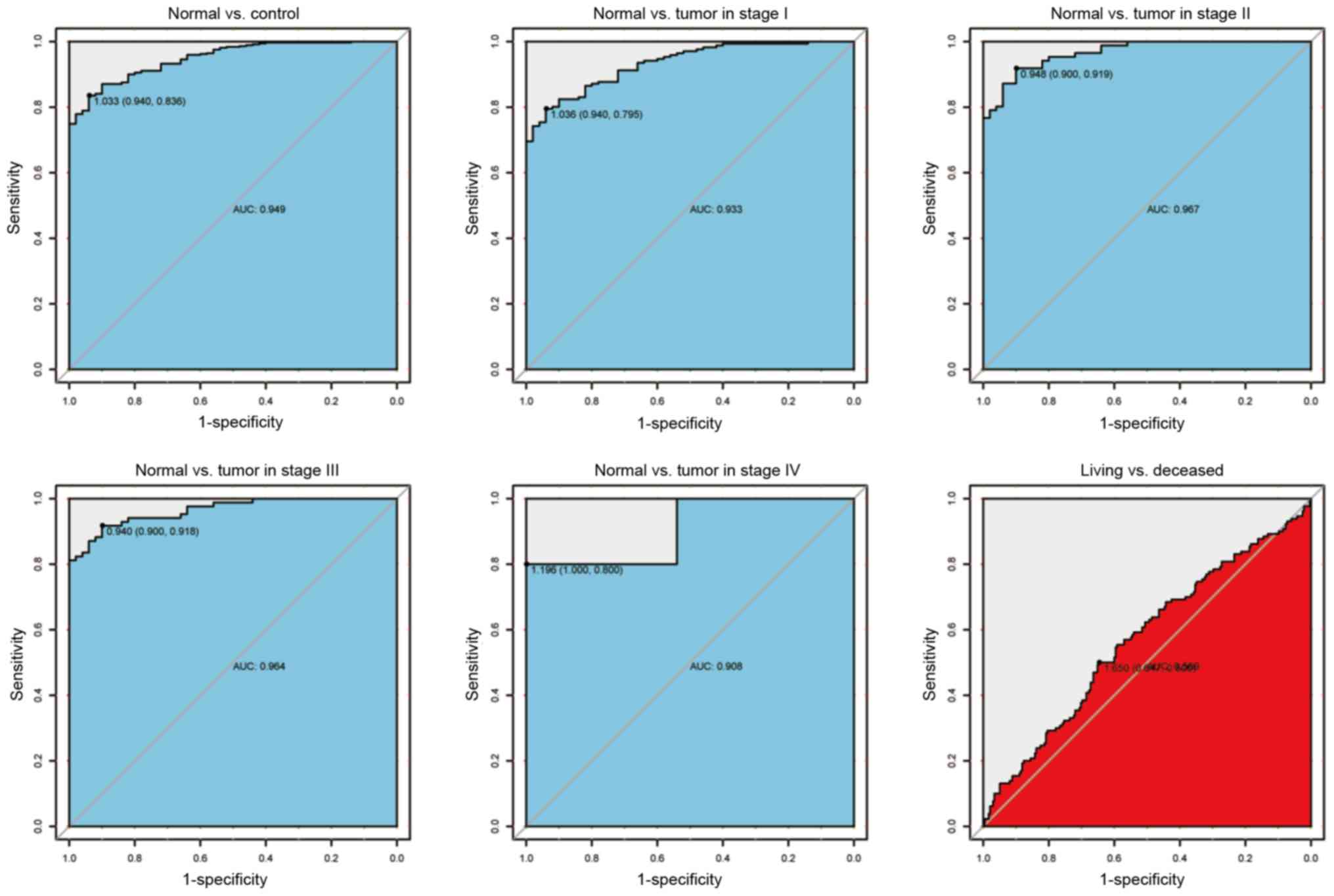
Accessing the diagnostic capability of
BACE1-AS
To further verify the aforementioned findings, the
ROC curves were plotted to evaluate the diagnostic ability of
BACE1-AS as a biomarker (Fig.
2). Consistent with the aforementioned results, BACE1-AS
showed both high sensitivity and specificity when differentiating
tumors from healthy tissues. The sensitivity and specificity was
0.94 and 0.836, respectively, with an area under the curve (AUC)
value of 0.949, demonstrating high differential diagnostic
potential. The AUC remained high when healthy individuals were
compared with patients with cancer of different clinical stages
(AUCs:, 0.933 for stage I; 0.967 for stage II; 0.964 for stage III;
and 0.908 for stage IV), which indicates BACE1-AS as a good
diagnostic marker of liver cancer, regardless of the tumor stage.
In order to simplify the subsequent analysis, Youden's J statistic
was calculated to determine the optimal cut-off point of
BACE1-AS expression (1.650), which was subsequently used to
divide patients with liver cancer into two groups: BACE1-AS
high group and BACE1-AS low group.
Associations between BACE1-AS
expression levels and clinicopathological parameters of patients
with liver cancer
The expression of BACE1-AS was significantly
associated with patients' histological grades, clinical stages and
tumor (T) classification (Table
II). This was consistent with the aforementioned results.
Notably, a modest but significant association was found between
tumor histological types and BACE1-AS levels (P=0.043).
Furthermore, the age of patients was associated with
BACE1-AS, with younger patients (aged <55 years)
presenting with higher levels of BACE1-AS (P=0.001).
| Table II.Associations between the
clinicopathologic variables and BACE1-AS expression. |
Table II.
Associations between the
clinicopathologic variables and BACE1-AS expression.
|
|
| BACE1-AS1
expression |
|
|
|---|
|
|
|
|
|
|
|---|
| Clinical
characteristics | Variable | No. of
patients | High, n (%) | Low, n (%) | χ2 | P-value |
|---|
| Age | <55 | 117 | 63
(41.45) | 54
(24.77) | 10.7607 | 0.001 |
|
| ≥55 | 253 | 89
(58.55) | 164 (75.23) |
|
|
| Sex | Female | 121 | 58
(37.91) | 63
(28.9) | 2.9231 | 0.087 |
|
| Male | 250 | 95
(62.09) | 155 (71.1) |
|
|
| Histological
type | Fibrolamellar | 3 | 1
(0.65) | 2
(0.92) | 5.8857 | 0.040 |
|
| Hepatocellular | 361 | 146 (95.42) | 215 (98.62) |
|
|
|
|
Hepatocholangiocarcinoma | 7 | 6
(3.92) | 1
(0.46) |
|
|
| Histologic
grade | G1 | 55 | 11
(7.24) | 44
(20.56) | 28.2803 | 0.000 |
|
| G2 | 177 | 64
(42.11) | 113 (52.8) |
|
|
|
| G3 | 122 | 68
(44.74) | 54
(25.23) |
|
|
|
| G4 | 12 | 9
(5.92) | 3
(1.4) |
|
|
| Stage | I | 171 | 58
(39.46) | 113 (56.5) | 10.3777 | 0.011 |
|
| II | 86 | 42
(28.57) | 44
(22) |
|
|
|
| III | 85 | 45
(30.61) | 40
(20) |
|
|
|
| IV | 5 | 2
(1.36) | 3
(1.5) |
|
|
| T
classification | T1 | 181 | 60
(39.22) | 121 (56.02) | 11.3008 | 0.015 |
|
| T2 | 94 | 46
(30.07) | 48
(22.22) |
|
|
|
| T3 | 80 | 41
(26.8) | 39
(18.06) |
|
|
|
| T4 | 13 | 6
(3.92) | 7
(3.24) |
|
|
|
| TX | 1 | 0
(0) | 1
(0.46) |
|
|
| N
classification | N0 | 252 | 111 (72.55) | 141 (64.98) | 5.0198 | 0.079 |
|
| N1 | 4 | 3
(1.96) | 1
(0.46) |
|
|
|
| NX | 114 | 39
(25.49) | 75
(34.56) |
|
|
| M
classification | M0 | 266 | 119 (77.78) | 147 (67.43) | 5.2756 | 0.055 |
|
| M1 | 4 | 2
(1.31) | 2
(0.92) |
|
|
|
| MX | 101 | 32
(20.92) | 69
(31.65) |
|
|
| Radiation
therapy | No | 338 | 138 (96.5) | 200 (98.52) | 0.7519 | 0.386 |
|
| Yes | 8 | 5
(3.5) | 3
(1.48) |
|
|
| Residual tumor | R0 | 324 | 133 (88.67) | 191 (89.25) | 1.6516 | 0.771 |
|
| R1 | 17 | 6
(4) | 11
(5.14) |
|
|
|
| R2 | 1 | 0
(0) | 1
(0.47) |
|
|
|
| RX | 22 | 11
(7.33) | 11
(5.14) |
|
|
| Vital status | Deceased | 130 | 65
(42.48) | 65
(29.82) | 5.7932 | 0.016 |
|
| Living | 241 | 88
(57.52) | 153 (70.18) |
|
|
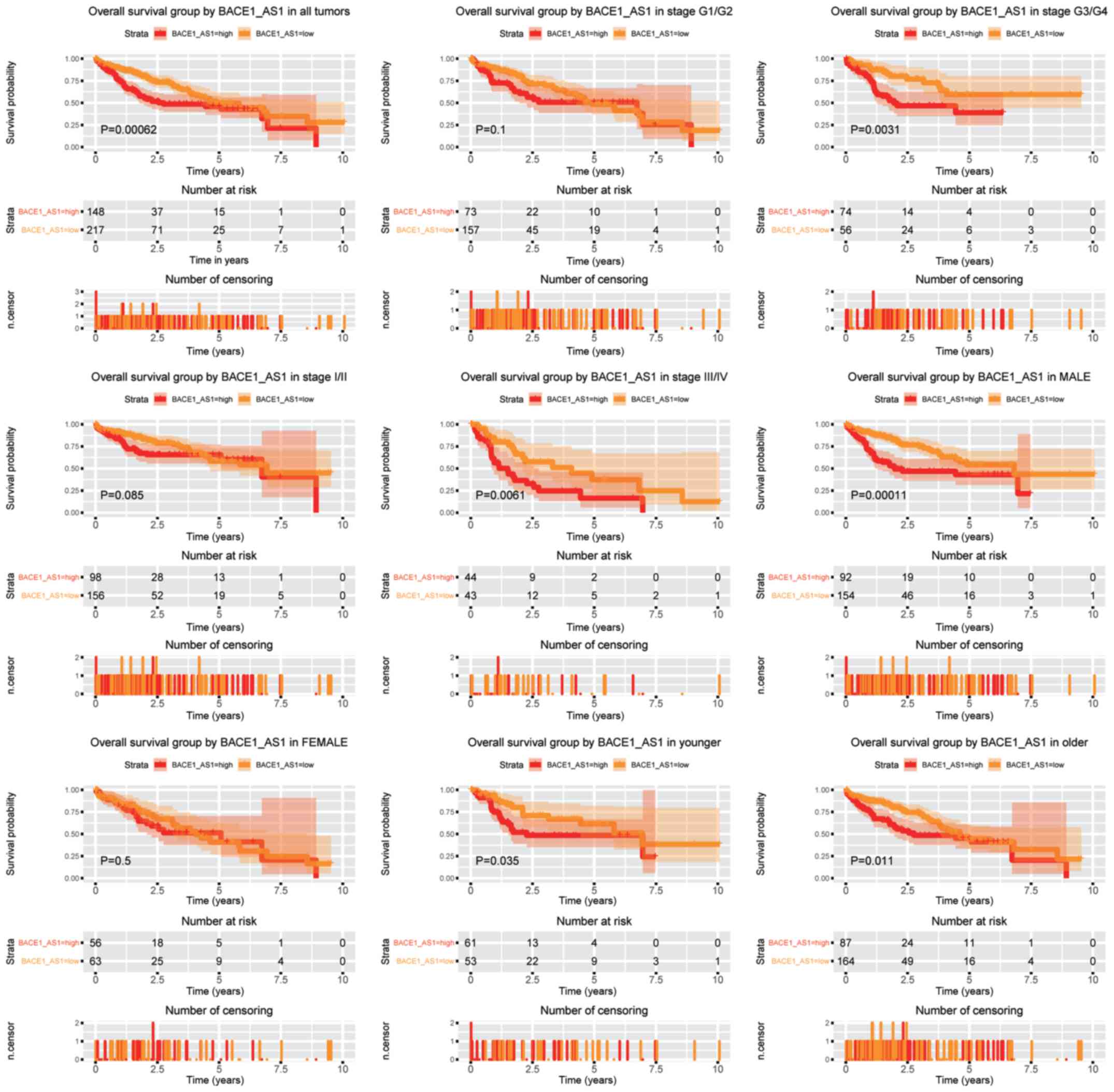
High expression of BACE1-AS predicts
poorer OS in patients with liver cancer
To verify the prognostic value of BACE1-AS in
patients with liver cancer, Kaplan-Meier curves were generated
(Fig. 3). Log-rank test was used for
comparison between groups. The BACE1-AS high group had a
significantly lower OS time compared with the BACE1-AS low
group (P=0.00062). Subsequently, the prognostic value of
BACE1-AS within different subgroups was studied.
BACE1-AS remained a negative prognostic factor in tumors of
advanced clinical stages (stage III/IV) and tumors of advanced
histopathology stages (G3/G4) (P=0.0061 and P=0.0031,
respectively). The aforementioned trend was not observed in tumors
of lower stages (stage I/II). High BACE1-AS expression was a
poorer prognostic marker in male patients (P=0.00011), while no
such significance was detected in females. Meanwhile,
BACE1-AS was a poor prognostic marker both in young (aged
<55 years) and old patients (aged ≥55 years).
In line with the aforementioned data, univariate Cox
regression analysis (Table III)
showed that patients with high BACE1-AS expression had a
significantly shorter OS time (P=0.001; HR, 1.81; 95% CI,
1.28–2.56). Furthermore, other prognostic parameters were also
analyzed and clinical stage, T classification and residual tumor
were identified as negative prognostic factors. Based on these
results, multivariate Cox regression analysis was applied to
validate the four established factors, which were all revealed be
significant prognostic factors except clinical stage. Thus,
BACE1-AS is an independent prognostic factor in liver
cancer; specifically, the adjusted HR was 1.76 (95% CI,
1.24–2.49).
| Table III.Univariate and multivariate analysis
of overall survival in patients with liver cancer. |
Table III.
Univariate and multivariate analysis
of overall survival in patients with liver cancer.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Parameters | Hazard Ratio | 95% CI
(lower-upper) | P-value | Hazard Ratio | 95% CI
(lower-upper) | P-value |
|---|
| Age | 1.02 | 0.7–1.48 | 0.926 |
|
|
|
| Sex | 0.82 | 0.57–1.16 | 0.263 |
|
|
|
| Histological
type | 0.98 | 0.27–3.63 | 0.982 |
|
|
|
| Histologic
grade | 1.05 | 0.85–1.31 | 0.651 |
|
|
|
| Stage | 1.38 | 1.15–1.65 | 0.001 | 0.85 | 0.69–1.06 | 0.151 |
| T
classification | 1.65 | 1.38–1.98 | 0.000 | 1.83 | 1.46–2.3 | 0.000 |
| N
classification | 0.71 | 0.5–1.03 | 0.071 |
|
|
|
| M
classification | 0.70 | 0.48–1.02 | 0.061 |
|
|
|
| Radiation
therapy | 0.52 | 0.26–1.03 | 0.061 |
|
|
|
| Residual tumor | 1.42 | 1.12–1.79 | 0.004 | 1.43 | 1.12–1.83 | 0.004 |
| BACE1-AS1 | 1.81 | 1.28–2.56 | 0.001 | 1.76 | 1.24–2.49 | 0.001 |
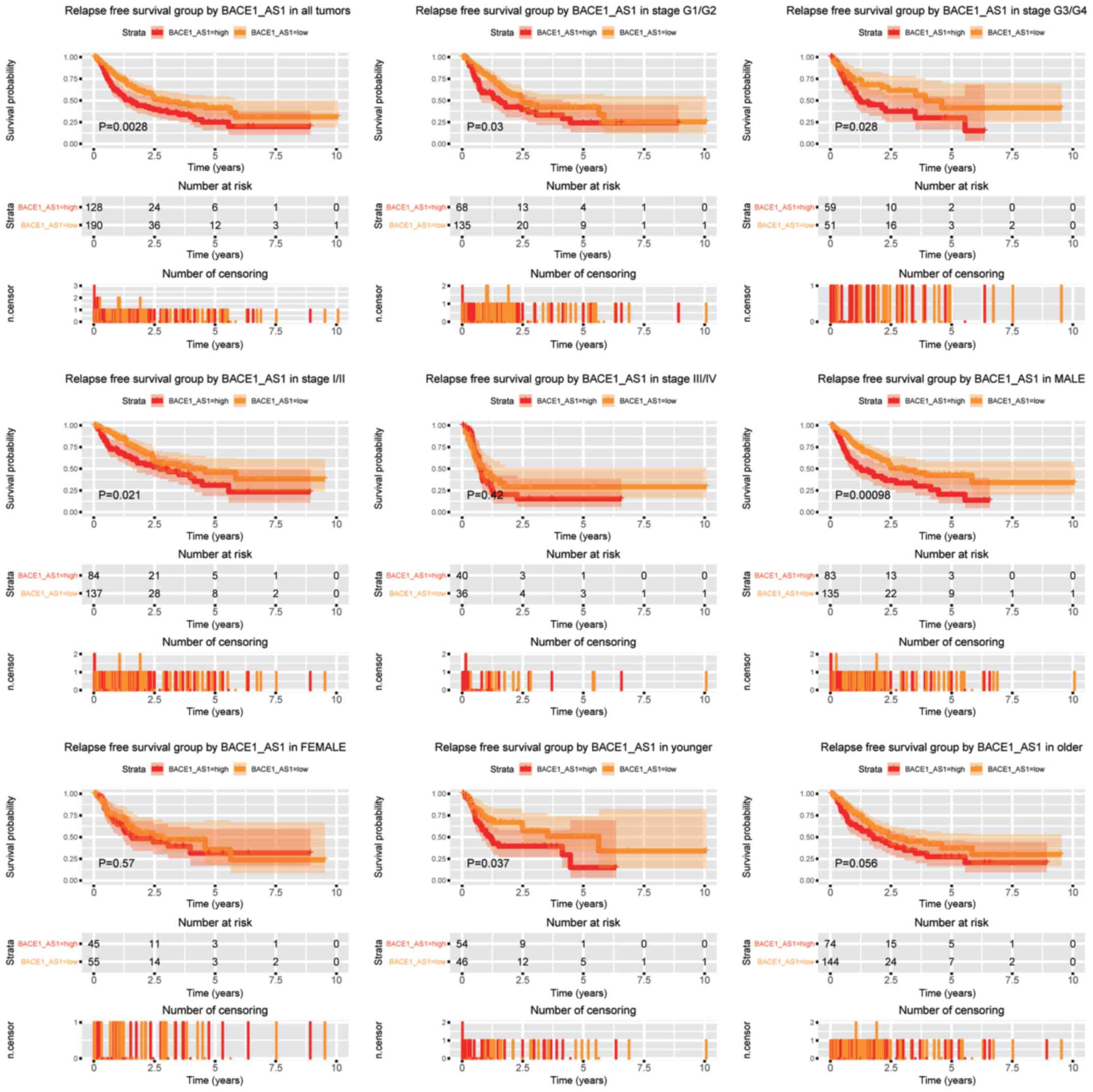
The upregulation of BACE1-AS predicts
poorer RFS in liver cancer cells
Subsequently, the role of BACE1-AS in the
prediction of RFS was analyzed (Fig.
4). Patients expressing higher levels of BACE1-AS had a
significantly shorter RFS time compared with patients with lower
BACE1-AS (P=0.0028). Subgroup analysis indicated that
BACE1-AS expression was a negative predictor in liver cancer
for both lower and advanced histopathological grades (G1/G2 and
G3/G4, respectively). For clinical stage, BACE1-AS
expression was associated with shorter RFS time in patients with
stage I/II, whereas patients with advanced cancer (stage III/IV)
were unaffected. Consistent with the OS analysis, BACE1-AS
retained its prognostic ability in male patients (P=0.00098), which
was not observed in female patients. Moreover, the expression of
BACE1-AS predicted shorter RFS time in younger patients
(aged <55 years) (P=0.037), whereas no prognostic potential was
demonstrated in older patients (aged ≥55 years).
Univariate Cox regression analysis revealed
BACE1-AS, tumor stage, T classification and residual tumor
as prognostic factors (Table IV).
Furthermore, multivariate Cox analysis identified BACE1-AS
expression, T classification and residual tumor as independent
predictive factors for RFS, and the adjusted HR for BACE1-AS
expression was 1.58 (95% CI, 1.13–2.22).
| Table IV.Univariate and multivariate analysis
of relapse free survival in patients with liver cancer. |
Table IV.
Univariate and multivariate analysis
of relapse free survival in patients with liver cancer.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Parameters | Hazard Ratio | 95% CI
(lower-upper) | P-value | Hazard Ratio | 95% CI
(lower-upper) | P-value |
|---|
| Age | 0.89 | 0.63–1.27 | 0.521 |
|
|
|
| Sex | 0.98 | 0.69–1.4 | 0.919 |
|
|
|
| Histological
type | 2.03 | 0.66–6.29 | 0.218 |
|
|
|
| Histologic
grade | 0.98 | 0.8–1.21 | 0.873 |
|
|
|
| Stage | 1.66 | 1.38–1.99 | 0.000 | 1.09 | 0.85–1.4 | 0.495 |
| T
classification | 1.78 | 1.49–2.12 | 0.000 | 1.67 | 1.29–2.17 | 0.000 |
| N
classification | 0.98 | 0.68–1.42 | 0.926 |
|
|
|
| M
classification | 1.19 | 0.8–1.78 | 0.394 |
|
|
|
| Radiation
therapy | 0.75 | 0.26–2.17 | 0.592 |
|
|
|
| Residual tumor | 1.27 | 1.01–1.61 | 0.042 | 1.36 | 1.07–1.72 | 0.013 |
| BACE1-AS1 | 1.65 | 1.18–2.31 | 0.003 | 1.58 | 1.13–2.22 | 0.008 |
Discussion
The increasing liver cancer incidence and liver
cancer-associated mortality warrants the discovery of new
biomarkers both for early diagnosis and improved treatment
surveillance. Previous studies have discovered a few biomarkers
that can be used as potential diagnostic and prognostic markers
(19–21). It has recently been shown that
BACE1-AS, an antisense lncRNA of BACE1 frequently
discussed in AD, is also involved in tumors, particularly as a
tumor suppressor (11,12). The present study demonstrated, using
the TCGA database, that BACE1-AS was highly elevated in
liver cancer, which was significantly associated with tumor grade
and staging. Besides, elevated BACE1-AS expression was an
independent prognostic factor for both poor OS and RFS in patients
with liver cancer. Overall, the data in the present study suggests
BACE1-AS as a potential biomarker for diagnosis and
prognostic classification of liver cancer.
BACE1-AS was found to be upregulated in liver
cancer compared with healthy individuals, indicating its potential
oncogenic role. Although AFP has been widely used as a marker for
liver cancer, the low sensitivity and specificity has largely
limited its value in cancer screening (3,22).
Subsequently, the potential of BACE1-AS as a diagnostic
marker in liver cancer was investigated. ROC analysis demonstrated
both high sensitivity and specificity of BACE1-AS for
diagnosing liver cancer. In order to test the clinical
applicability of BACE1-AS, comparison with other well
established/gold standard biomarkers is required. Although
ultrasound combined with AFP testing represents currently the most
popular strategy for liver cancer screening, such data are
currently not available in the TCGA database. Nonetheless, the
potential of BACE1-AS as a surrogate to AFP in liver cancer
screening is worthy of further studies.
Subgroup analysis revealed that BACE1-AS was
differentially expressed in liver cancer among different
categories. For example, BACE1-AS were highly associated
with liver cancer histological grades, and BACE1-AS levels
gradually increased as tumor grade was moving from G1 to G4,
indicating that BACE1-AS may be an important factor in
controlling tumor cell differentiation and the degrees of
malignancy. Moreover, differential expression was also found in
subgroups of different tumor staging and tumor size staging that
constitutes the main parameter in tumor staging, suggesting its
roles in tumor progression. The relative downregulation of
BACE1-AS in stage IV and also T4 tumors may be a result of
inadequate sample size in this particular subgroup. Thus, further
analysis is urgently required. Interestingly, it was found that
BACE1-AS levels varied among liver cancer of different
histopathological groups, with a near significant overall trend
P=0.063. BACE1-AS expression levels are significantly
associated with histological types, when the continuous variable of
BACE1-AS level is converted into binary value (P=0.043).
This is important since the differential diagnosis between HCC and
mixed HCC-CAA can be rather difficult in clinical settings through
imaging (23,24). Traditional diagnostic method requires
resection followed by thorough pathological examination. The
implementation of BACE1-AS could be a potential marker in
assisting differential diagnosis, which is crucial for later
clinical decisions.
BACE1-AS is closely associated with clinical
prognosis in liver cancer. However, subgroup analysis revealed that
BACE1-AS may not predict clinical outcome in some subgroups,
such as in female patients. Overall, BACE1-AS is an
unfavorable independent prognostic factor for both OS and RFS in
liver cancer.
Mechanistically, BACE1-AS was first
identified in AD as an antisense lncRNA to BACE1. The latter
encodes a key β-secretase enzyme that is responsible for the
formation of β-amyloid (Aβ) peptide, which is the central player in
the pathogenesis of AD. It was experimentally confirmed that
BACE1-AS could pair with the BACE1 mRNA and induce notable changes
to the secondary or tertiary structures of the BACE1 mRNA, leading
to increased BACE1 mRNA stability and translation in a positive
feed-forward pathway. The present study explored whether this
association also occurred in liver cancer. However, the results of
the present study demonstrated no association between BACE1-AS and
BACE mRNA expression (data not shown).
Furthermore, it is noteworthy that the results of
the present study is in contrast to previous studies (11,12), in
which BACE1-AS was demonstrated to function as a tumor
suppressor. BACE1-AS was shown to be a novel target for
anisomycin-mediated suppression of ovarian cancer stem cell
proliferation and invasion (11).
Elevated BACE1-AS, triggered by anisomycin treatment, leads
to an increased accumulation of Aβ, which ultimately caused
apoptosis of the ovarian cancer stem cells. Another study showed
that BACE1-AS is downregulated in 5-fluorouracil-resistant
colon cancer cells, suggesting its positive roles in
chemosensitivity (12). The
discrepancy could be generated from the type of studies. Previous
studies mainly focused on in vitro experiments, whereas the
present study was clinically centered. Moreover, the possibility
that BACE1-AS might work in a context-dependent manner
cannot be ruled out, the determination of which requires further
studies both in vitro and in vivo.
It is worth noting that one possible limitation of
the present study is the lack of validation by additional patient
cohorts. Furthermore, other major prognostic factors such as liver
function and liver-etiology were not included in the analysis,
since such data are currently unavailable in the TCGA database.
Nonetheless, the results of the present study raise the potential
possibility of incorporating next generation sequencing data into
clinical decision-making and paves way for further studies.
Overall, the present study is the first to
demonstrate BACE1-AS as a potential diagnostic and
prognostic biomarker in liver cancer. Further basic and clinical
research is required in order to verify the results of the present
study.
Acknowledgements
Not applicable.
Funding
This study was partly supported by the National
Natural Science Foundation of China (grant no. 81670143).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
YN and YJ conceived and designed the study. YJ
analyzed and interpreted the data with help from YL and YX. YN
drafted the manuscript. WL analyzed and interpreted data and revise
the manuscript for important intellectual content. All authors have
read and approved of the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patients' consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rahib L, Smith BD, Aizenberg R, Rosenzweig
AB, Fleshman JM and Matrisian LM: Projecting cancer incidence and
deaths to 2030: The unexpected burden of thyroid, liver, and
pancreas cancers in the United States. Cancer Res. 74:2913–2921.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tzartzeva K, Obi J, Rich NE, Parikh ND,
Marrero JA, Yopp A, Waljee AK and Singal AG: Surveillance imaging
and Alpha fetoprotein for early detection of hepatocellular
carcinoma in patients with cirrhosis: A Meta-analysis.
Gastroenterology. 154:1706–1718 e1. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Liu CY, Chen KF and Chen PJ: Treatment of
liver cancer. Cold Spring Harb Perspect Med. 5:a0215352015.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2019. CA Cancer J Clin. 69:7–34. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Vassar R: BACE1: The beta-secretase enzyme
in Alzheimer's disease. J Mol Neurosci. 23:105–14. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Borghi R, Patriarca S, Traverso N, Piccini
A, Storace D, Garuti A; Gabriella Cirmena, ; Patrizio Odetti and
Massimo Tabaton: The increased activity of BACE1 correlates with
oxidative stress in Alzheimer's disease. Neurobiol Aging.
28:1009–1014. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Dislich B and Lichtenthaler SF: The
membrane-bound aspartyl protease BACE1: Molecular and functional
properties in Alzheimer's disease and beyond. Front Physiol.
3:82012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nogalska A, Engel WK and Askanas V:
Increased BACE1 mRNA and noncoding BACE1-antisense transcript in
sporadic inclusion-body myositis muscle fibers-possibly caused by
endoplasmic reticulum stress. Neurosci Lett. 474:140–143. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Faghihi MA, Modarresi F, Khalil AM, Wood
DE, Sahagan BG, Morgan TE, Finch CE, St Laurent G III, Kenny PJ and
Wahlestedt C: Expression of a noncoding RNA is elevated in
Alzheimer's disease and drives rapid feed-forward regulation of
beta-secretase. Nat Med. 14:723–730. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chen Q, Liu X, Xu L, Wang Y, Wang S, Li Q,
Huang Y and Liu T: Long non-coding RNA BACE1-AS is a novel target
for anisomycin-mediated suppression of ovarian cancer stem cell
proliferation and invasion. Oncol Rep. 35:1916–1924. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lee H, Kim C, Ku JL, Kim W, Yoon SK, Kuh
HJ, Lee JH, Nam SW and Lee EK: A long non-coding RNA snaR
contributes to 5-fluorouracil resistance in human colon cancer
cells. Mol Cells. 37:540–546. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Deschamps-Francoeur G, Simoneau J and
Scott MS: Handling multi-mapped reads in RNA-seq. Comput Struct
Biotechnol J. 18:1569–1576. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Qu LS and Zhang HF: Significance of viral
status on prognosis of hepatitis B-related hepatocellular carcinoma
after curative resection in East Asia. Hepatol Res. 46:40–49. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
National Comprehensive Cancer Network,
Hepatobiliary Cancers (Version 1, 2020). https://www.nccn.org/professionals/physician_gls/default.aspx#hepatobiliaryMarch
23–2020
|
|
16
|
R. Development Core Team, . R: A language
and environment for statistical computing. R Foundation for
Statistical Computing; Vienna, Austria: 2018, https://www.R-project.org/July 5–2018
|
|
17
|
Therneau TM and Grambsch PM: Modeling
Survival Data: Extending the Cox Model. Springer-Verlag New York;
NY: 2000, View Article : Google Scholar
|
|
18
|
Wickham H: Ggplot2: Elegant Graphics for
Data Analysis. Springer-Verlag New York; New York, USA: pp.
245–246. 2016
|
|
19
|
Jiao Y, Fu Z, Li Y, Meng L and Liu Y: High
EIF2B5 mRNA expression and its prognostic significance in liver
cancer: A study based on the TCGA and GEO database. Cancer Manag
Res. 10:6003–6014. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Jiao Y, Fu Z, Li Y, Zhang W and Liu Y:
Aberrant FAM64A mRNA expression is an independent predictor of poor
survival in pancreatic cancer. PLoS One. 14:e02112912019.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Jiao Y, Li Y, Lu Z and Liu Y: High
Trophinin-associated protein expression is an independent predictor
of poor survival in liver cancer. Dig Dis Sci. 64:137–143. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Waidely E, Al-Yuobi AR, Bashammakh AS,
El-Shahawi MS and Leblanc RM: Serum protein biomarkers relevant to
hepatocellular carcinoma and their detection. Analyst. 141:36–44.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Gera S, Ettel M, Acosta-Gonzalez G and Xu
R: Clinical features, histology, and histogenesis of combined
hepatocellular-cholangiocarcinoma. World J Hepatol. 9:300–309.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Li R, Yang D, Tang CL, Cai P, Ma KS, Ding
SY, Zhang XH, Guo DY and Yan XC: Combined hepatocellular carcinoma
and cholangiocarcinoma (biphenotypic) tumors: Clinical
characteristics, imaging features of contrast-enhanced ultrasound
and computed tomography. BMC Cancer. 16:1582016. View Article : Google Scholar : PubMed/NCBI
|