Introduction
Due to its aggressive nature and poor survival
rates, esophageal cancer is the 6th leading cause of
cancer-associated deaths and is the 8th most common cancer
worldwide, according to GLOBOCAN 2008 (1). In Chinese men, esophageal cancer was
the 5th most common cancer and the 4th leading cause of
cancer-associated deaths in 2013 (2). Esophageal squamous cell carcinoma
(ESCC) accounts for 88% of esophageal cancers (3). Myelodysplastic syndrome (MDS) is a
disorder that is found in hematopoietic stem or progenitor cells,
which is characterized by abnormal differentiation, dysplasia and
peripheral blood cytopenias (4).
Approximately 30% of patients with MDS subsequently develop acute
myeloid leukemia (AML) (5). However,
the underlying molecular mechanism of this process is unknown
(5). MDS occurs more frequently in
older patients (≥60 years of age) and individuals who have been
exposed to prior chemotherapy or radiation therapy, and has an
overall survival (OS) time ranging from several months to 10 years
(6). The prevalence of multiple
primary malignant neoplasms (MPMN) has been demonstrated to range
from 0.73 to 11.7% worldwide (7).
The majority of synchronous malignancies are solid tumors; however,
cases of primary MDS/AML occurring alongside solid tumors have
rarely been reported. The current case report describes a patient
with ESCC and MDS that rapidly progressed to AML. Next-generation
gene sequencing was also performed to elucidate the associations
between these types of cancer.
Case report
Clinical experiments
Bone marrow smear and cytochemical staining analysis
were performed according to routine protocols by the clinical
laboratory of the Department of Hematology of The Third Affiliated
Hospital of Sun Yat-sen University (Guangzhou, China). The
Wright-Giemsa stain was applied onto the whole smear for 10 sec at
room temperature, then the same amount (0.5–0.8 ml) of phosphoric
acid buffer was added and mixed with the dye solution at room
temperature for 25 min. Subsequently, the smear was washed with
distilled water and the slides were air-dried.
Histopathology and hematoxylin and eosin (HE)
staining analysis were performed by the Department of Pathology of
The Third Affiliated Hospital of Sun Yat-sen University. HE
staining was performed according to routine protocols. Briefly,
after deparaffinization and rehydration, 5-µm-thick sections were
stained with hematoxylin solution for 5 min at room temperature,
followed by 5 washes in 1% acid ethanol and then rinsed in
distilled water. Subsequently, the sections were stained with eosin
solution for 3 min at room temperature, followed by dehydration in
a graded alcohol series and clearing in xylene. The mounted slides
were then examined and photographed using a light microscope
(Olympus BX43; Olympus Corporation; magnification, ×100).
Flow cytometry and next-generation sequencing were
performed by Kind Med Diagnostics Group Co., Ltd.
Results
A 51-year-old male patient had dysphagia,
particularly with coarse food, for 10 days without the symptoms
subsiding. After visiting a local hospital (Heyuan People's
Hospital; Heyuan, Guangdong, China), the patient was diagnosed with
ESCC after receiving biopsy using gastroscopy. He was subsequently
admitted to The Third Affiliated Hospital of Sun Yat-Sen University
(Guangdong, China) for further evaluation and treatment on 27th
November 2018. He had no history of previous malignancies, exposure
to ionizing radiation or chemotherapy. He also had no family
history of cancer. He was a frequent smoker (>30 cigarettes per
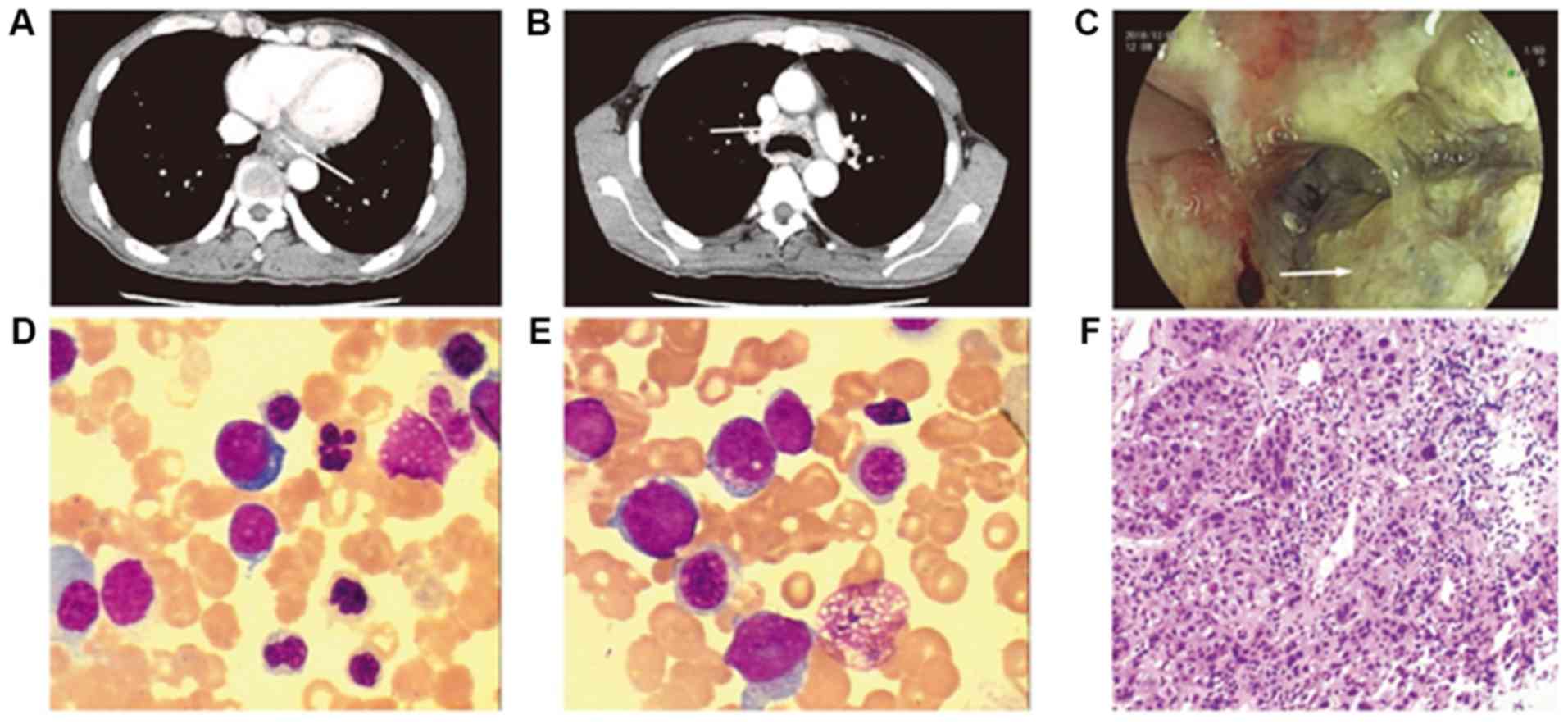
day) and consumed 150 ml alcohol per day for ~30 years. Enhanced
computer tomography scans of the chest and upper abdomen indicated
an esophageal neoplasm with multiple swollen lymph nodes within the
mediastinum, and an unascertained nodule in the superior lobe of
the left lung (Fig. 1A and B). The
results of the endoscopy revealed a large semi-circular mass,
covered with white moss in the lower esophagus (Fig. 1C). Following endoscopic biopsy, the
mass was determined to be moderately differentiated squamous cell
carcinoma (Fig. 1F). According to
the 8th edition of the American Joint Committee on Cancer/Union for
International Cancer Control TNM staging system, the clinical stage
of the patient was cT3N2M0, stage IVA (8). Routine blood analysis revealed elevated
white blood cells (8.99×109/1), and hemoglobin (90 g/l)
and platelet (25×109//1) counts. MDS with excess blasts
was diagnosed according to the 2016 World Health Organization
classification after bone marrow aspiration (9). The bone marrow smear revealed
pathological hematopoiesis and 10.5% primordial immature
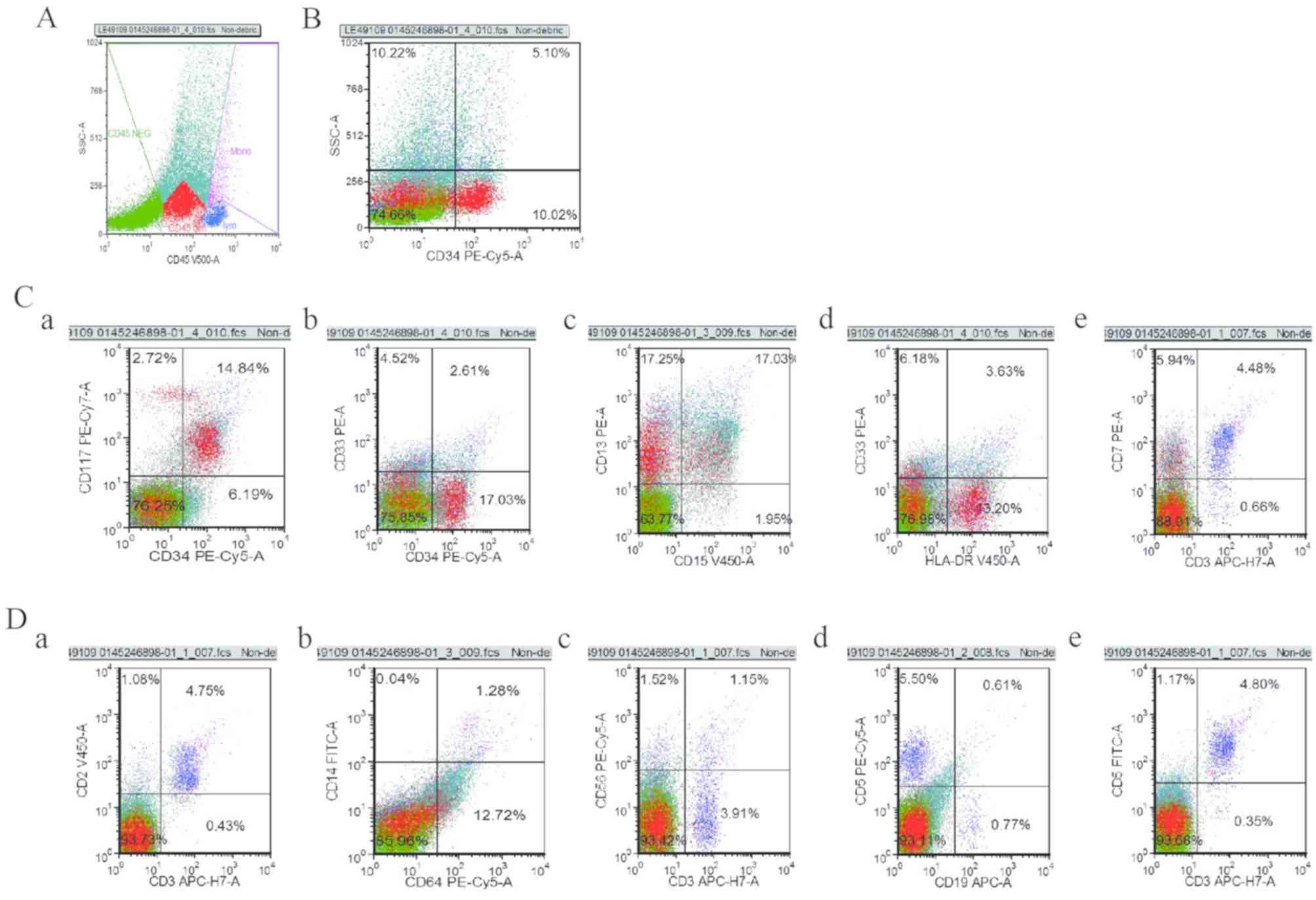
granulocytes (Fig. 1D). Flow
cytometry analysis of the bone marrow revealed 10% medullary
primitive cells with abnormal immunophenotype, exhibiting
CD34+, CD117+, CD33+, human
leukocyte antigen-DR phenotype+, CD14−,
CD64−, CD56−, CD19−,
CD7+ (few), CD5− and CD2−
(Fig. 2). Cytogenetics analysis
revealed that the patient exhibited a complex karyotype, with
44–48, xy, −4, 5, +6, del(7)(q21), del(9)(q21;q32), del(11)(q14),
+12, +12, del (12)(p10), −15, +22,
+mar, 1–5dmin (9)46,xy(1), with one
of these chromosome karyotypes shown in Fig. 3. After 10 days, the bone marrow smear
demonstrated 25% primitive cell transformation to AML (Fig. 1E). The next-generation sequencing
result revealed genetic mutations in TP53, ALK receptor tyrosine
kinase (ALK), ROS proto-oncogene 1, receptor tyrosine kinase
(ROS1), AT-rich interaction domain 1A (ARID1A), platelet-derived
growth factor receptor β (PDGFRB), cyclin-dependent kinase
inhibitor 2A (CDKN2A) and neurofibromin 1 (NF1) in the ESCC
samples, while mutations in TP53 and ROS1 were found in the bone
marrow fluid (10). In ESCC samples,
there were three point mutations of TP53, and the mutation
frequencies were 6% for TP53:NM_000546.5:c.764dupT(p.T256fs) exon
7, 4.5% for TP53:NM_000546.5:c.711G>A(p.M237I) exon 7 and 14.1%
for TP53:NM_000546.5:c.580C>T (p.L194F) exon 6. In the bone
marrow fluid, there were two mutations of TP53, and the mutation
frequencies were 37.3% for TP53:NM_000546.5:c.764dupT(p.T256fs)
exon 7 and 55.6% for TP53:NM_000546.5:c.711G>A(p.M237I) exon 7.
The mutation frequency of ROS1:NM_002944.2:c.5842C>T (p.R1948C)
exon 36 was 41.4% in ESCC samples and 45.2% in the bone marrow
fluid (10). Due to the poor
financial position of the patient, therapeutic intervention was
refused and the patient died within 20 days.
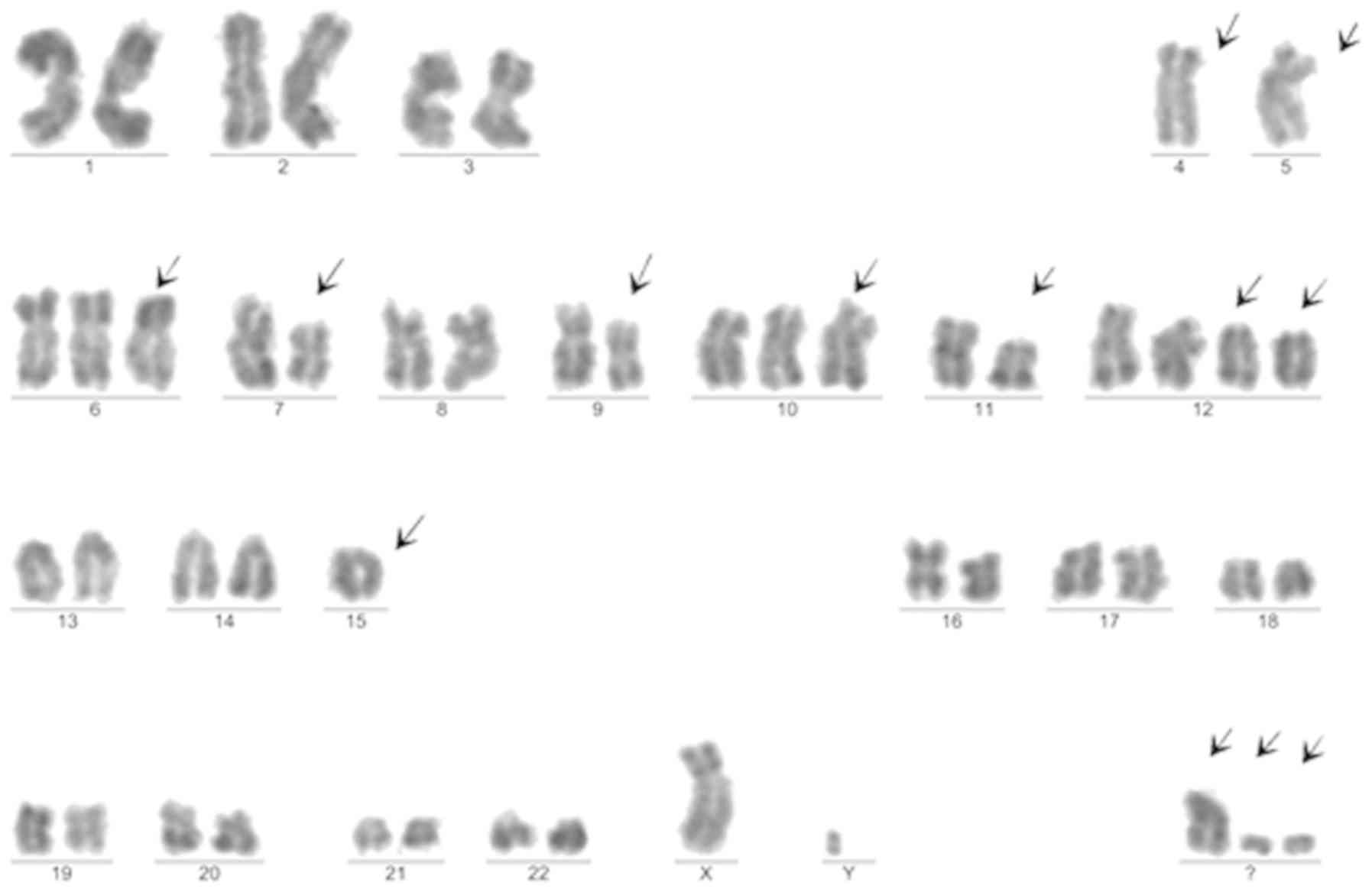 | Figure 3.One of the chromosome karyotypes of
the patient. 48, xy, −4, −5, +6, del(7)(q21), del(9)(q21;q32),
del(11)(q14), +12, +12, del(12)(p10), −15, +22, +mar, 2dmin. The
arrows indicate the abnormal chromosomes. |
Discussion
The etiology of ESCC is multi-factorial. It has been
found that tobacco, alcohol, poverty, betel quid, pickled
vegetables, hot foods, X-rays, γ-radiation and achalasia increase
the risk of developing ESCC (11).
Genetic variants, such as frameshift or missense mutations, in
TP53, RB transcriptional corepressor 1, CDKN2A,
phosphatidylinositol-4,5-bisphosphate 3-kinase, catalytic subunit
α, notch receptor 1, nuclear factor, erythroid 2 like 2, family
with sequence similarity 135 member B, lysine methyltransferase 2A
(KMT2A), ASH1 like histone lysine methyltransferase, KMT2C, SET
domain containing 1B, histone lysine methyltransferase,
CREB-binding protein and E1A binding protein p300, may serve
important roles in the development of ESCC (12). The etiology and pathogenesis of
MDS/AML has not been elucidated, as the primary cause of MDS is
only established in 15% of cases (13). Benzene exposure is one of the few
well-known risk factors for myeloid malignancy (14). However, exposure to soot, creosote,
inks, dyes, tanning solutions and coal dust may also serve a role
in the etiology of myeloid malignancy (14). Du et al (15), found that MDS was significantly
associated with smoking, but not with alcohol consumption. The
patient in that study, was a frequent tobacco and alcohol consumer,
exhibited various well-known cancer-associated genetic mutations
and suffered from ESCC. Multiple primary malignant neoplasms
(MPMNs) are rare malignant neoplasms that simultaneously or
successively occur in one patient, as two or more primary
malignancies (16). In general,
MPMNs are more common as two solid tumors or as two hematological
malignancies. Cases of MPMN that involve solid tumors and
hematological malignancies are; however, rare (16). To the best of our knowledge, only one
previous report has described a patient with AML with ESCC
(17). Li et al (16), reported a case of colorectal cancer
and multiple myeloma (MM) with chest wall involvement. In that
case, MM was confirmed following two cycles of chemotherapy for
colorectal cancer. The authors were therefore unable to conclude
whether the two malignancies were associated. However, in the
present case, ESSC and MDS/AML were confirmed almost at the same
time. Unexplained thrombocytopenia required the patient in the
present case report to undergo a bone marrow aspiration, which was
important for the diagnosis of MDS/AML.
A karyotype with >4 aberrations, including
translocations, inversions and copy number insertions or deletions,
was found to be a significant adverse-risk abnormality in AML
(18). The complex karyotype of the
patient in the present case study containing >4 aberrations
suggested a poor prognosis. Next-generation sequencing revealed
that several gene variants existed in the bone marrow and ESCC of
the patient. ARID1A, as a novel tumor suppressor, is essential for
maintaining the frequency and function of hematopoietic stem cells,
and was found to be associated with gynecological, liver, gastric
and breast cancer, as well as leukemia (19). While NF1 mutations, including
missense, frameshift and nonsense mutations, in patients with AML
were indicative of an poor prognosis (20), they are also found in patients with
ESCC (21). The PDGFRB gene, is
located on chromosome 5q31-33 (22).
Patients with lymphocytic leukemia and AML with PDGFRB fusions
could be treated with tyrosine kinase inhibitors (23,24).
PDGFRB regulates the mRNA expression of transforming growth
factor-α and serves a central role in esophageal carcinoma tumor
invasion and metastasis (25). The
next-generation sequencing results, from the patient in the present
study, revealed that the genetic mutations in TP53 and ROS1 were
found in both ESCC and MDS/AML. The ROS1 mutation frequency was
45.2% in MDS/AML and 41.4% in ESCC (10). The ROS1 gene belongs to the sevenless
subfamily of tyrosine kinase insulin receptor genes (26). ROS1 protein expression in adult
humans is highest in the kidney; however, it is also found in the
cerebellum, peripheral neural tissue, stomach, small intestine, and
colon, with lower expression levels in parathyroid, larynx, adrenal
gland and skeletal muscle tissues (27). However, to the best of our knowledge,
this is the first time that ROS1 was detected in ESCC in the
patient, in the present case report. The ROS1 gene often forms
fusion gene with other genes, such as ALK (26). The signaling pathways, such as
Ras/Raf/MEK/ERK1/2 and JAK/STAT, activated by ROS1 fusions appear
to primarily involve common growth and survival pathways (26,28). The
Food and Drug Administration approval of tyrosine kinase inhibitors
for the treatment of ALK- and ROS1-rearranged non-small cell lung
cancer led to the understanding that receptor tyrosine kinase
fusions could be targets for the treatment of oncogenic driver
alterations in a diverse group of solid malignancies, such as
gastric cancer (29). However, the
function of ROS1 mutations in ESCC of the present patient requires
further investigation. The TP53 point mutations frequency was much
lower in ESCC [6% for NM_000546.5:c.764dupT(p.T256fs) exon 7 and
4.5% for NM_000546.5:c.711G>A(p.M237I) exon 7] compared with
that in MDS/AML [37.3% for NM_000546.5:c.764dupT(p.T256fs) exon 7
and 55.6% for NM_000546.5:c.711G>A(p.M237I) exon 7] in the
patient in the present case study. There are two possible reasons
that may explain this phenomenon: First, ESCC may have had fewer
TP53 mutations; second, TP53 mutations in ESCC may have resulted
from a small quantity of MDS/AML cell infiltration, which would
also explain the lower detection rate of TP53 mutation frequency in
ESCC. TP53, a tumor suppressor gene located on chromosome 17p13,
serves crucial roles in tumor genesis (30) and is the most frequently mutated gene
in human cancer, with a frequency of ~50% in squamous cell skin
carcinoma (31). In addition, TP53
has been identified in numerous different types of hematological
malignancies, such as AML, MDS and acute lymphoblastic leukemia
(31). The p53 mutation in codon 248
(p53R248W) was revealed to enhance leukemia-initiating cell
self-renewal to promote leukemia development (32). Thus, genetic mutations in TP53 and
ROS1 were the most important oncogenes that were identified in the
patient, in the present case report.
Variants in the TP53, ROS1, ALK, ARID1A, PDGFRB,
CDKN2A and NF1 genes are important in patients with ESCC and
MDS/AML as they have been associated with tumor formation,
recurrence and metastasis. In the patient in the present case
study, mutations in these genes might have been involved in the
development of ESSC and MDS/AML. However, further investigation
regarding how the gene mutations may promote the proliferation of
tumor cells is required for confirmation. The presence of these
gene variants, in addition to tobacco and alcohol consumption, may
have resulted in the patient developing MPMN. The patient refused
chemotherapy; therefore, the effect of therapeutic intervention was
unknown, although there is no standard treatment regimen for MPMN
and it is unknown which malignant neoplasm should be prioritized.
Thus, further research is required to determine this.
In conclusion, the current case report describes an
extremely rare case of ESCC presenting in conjunction with MDS/AML.
The results indicated that for patients with solid tumors and
unexplained blood changes, the presence of a hematological
malignancy should be considered and bone marrow puncture should
also be performed. The application of next-generation gene
sequencing may also provide more information regarding gene
mutations, which may also guide future treatment. The poor
lifestyle of the patient in the current case study may have
promoted the development of MPMN, which requires multiple gene
mutations. However, the underlying molecular mechanism of this
process requires further investigation.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Fundamental
Research Funds for the Central Universities (grant no. 20YKPY29)
and the Science and Information Technology Bureau of Guangzhou
Haizhu District (grant no. 2012-ZD-02).
Availability of data and materials
The data that support the findings of this study are
available from reference (10)
(dataset posted in May 2020).
Authors' contributions
RX supervised the writing of the manuscript and
diagnosis and treatment of the patient. JL supervised the overall
care of the patient. XYL wrote the manuscript. LL performed bone
marrow aspiration and revised the manuscript. YS analyzed the data
and edited the figures. XT helped revise the manuscript. XXL
performed next-generation gene sequencing and acquired the data
form Kind Med Diagnostics Group Co., Ltd. YZ performed the
karyotype analysis. All authors approved the final version of the
manuscript.
Ethics approval and consent to
participate
The patients next of kin provided written informed
consent.
Patient consent for publication
The patients next of kin provided consent for
publication.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ferlay J, Shin HR, Bray F, Forman D,
Mathers C and Parkin DM: Estimates of worldwide burden of cancer in
2008: GLOBOCAN 2008. Int J Cancer. 127:2893–2917. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen W, Zheng R, Zhang S, Zeng H, Xia C,
Zuo T, Yang Z, Zou X and He J: Cancer incidence and mortality in
China, 2013. Cancer Lett. 401:63–71. 2010. View Article : Google Scholar
|
|
3
|
Arnold M, Soerjomataram I, Ferlay J and
Forman D: Global incidence of oesophageal cancer by histological
subtype in 2012. Gut. 64:381–387. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tefferi A and Vardiman JW: Myelodysplastic
syndromes. N Engl J Med. 361:1872–1885. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
da Silva-Coelho P, Kroeze LI, Yoshida K,
Koorenhof-Scheele TN, Knops R, van de Locht LT, de Graaf AO, Massop
M, Sandmann S, Dugas M, et al: Clonal evolution in myelodysplastic
syndromes. Nat Commun. 8:150992017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Montalban-Bravo G and Garcia-Manero G:
Myelodysplastic syndromes: 2018 update on diagnosis,
risk-stratification and management. Am J Hematol. 93:129–147. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Demandante CG, Troyer DA and Miles TP:
Multiple primary malignant neoplasms: Case report and a
comprehensive review of the literature. Am J Clin Oncol. 26:79–83.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rice TW, Ishwaran H, Ferguson MK,
Blackstone EH and Goldstraw P: Cancer of the esophagus and
esophagogastric junction: An eighth edition staging primer. J
Thorac Oncol. 12:36–42. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Arber DA, Orazi A, Hasserjian R, Thiele J,
Borowitz MJ, Le Beau MM, Bloomfield CD, Cazzola M and Vardiman JW:
The 2016 revision to the World Health Organization classification
of myeloid neoplasms and acute leukemia. Blood. 127:2391–2405.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Liu L, Liu X, Sun Y, Zeng Y, Tang X, Li X,
Liu J, Xiao R, et al: Esophageal squamous cell cancer coincidence
with myelodysplastic syndrome/acute myelogenous leukemia. Figshare.
simpledoi.org/10.6084/m9.figshare.12349877.v1May
21–2020
|
|
11
|
Abnet CC, Arnold M and Wei WQ:
Epidemiology of esophageal squamous cell carcinoma.
Gastroenterology. 154:360–373. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Song Y, Li L, Ou Y, Gao Z, Li E, Li X,
Zhang W, Wang J, Xu L, Zhou Y, et al: Identification of genomic
alterations in oesophageal squamous cell cancer. Nature. 509:91–95.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Adès L, Itzykson R and Fenaux P:
Myelodysplastic syndromes. Lancet. 383:2239–2252. 2018. View Article : Google Scholar
|
|
14
|
Poynter JN, Richardson M, Roesler M, Blair
CK, Hirsch B, Nguyen P, Cioc A, Cerhan JR and Warlick E: Chemical
exposures and risk of acute myeloid leukemia and myelodysplastic
syndromes in a population-based study. Int J Cancer. 140:23–33.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Du Y, Fryzek J, Sekeres MA and Taioli E:
Smoking and alcohol intake as risk factors for myelodysplastic
syndromes (MDS). Leuk Res. 34:1–5. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Li QL, Ma JA, Li HP, Huang RB, Hu CH, Liu
XL, Gao YW, Feng GH and Wu F: Synchronous colorectal cancer and
multiple myeloma with chest wall involvement: Is this a
coincidence? Curr Probl Cancer. 41:413–418. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hara M and Hoshijima T: Philadelphia
chromosome (Ph1) positive acute myelomonocytic leukemia with
esophageal cancer: A case report. Rinsho Ketsueki. 33:964–968.
1992.(In Japanese). PubMed/NCBI
|
|
18
|
Stölzel F, Mohr B, Kramer M, Oelschlagel
U, Bochtler T, Berdel WE, Kaufmann M, Baldus CD, Schafer-Eckart K,
Stuhlmann R, et al: Karyotype complexity and prognosis in acute
myeloid leukemia. Blood Cancer J. 6:e3862016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Han L, Madan V, Mayakonda A, Dakle P, Woon
TW, Shyamsunder P, Nordin HBM, Cao Z, Sundaresan J, Lei I, et al:
Chromatin remodeling mediated by ARID1A is indispensable for normal
hematopoiesis in mice. Leukemia. 33:2291–2305. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Eisfeld AK, Kohlschmidt J, Mrozek K, Mims
A, Walker CJ, Blachly JS, Nicolet D, Orwick S, Maharry SE, Carroll
AJ, et al: NF1 mutations are recurrent in adult acute myeloid
leukemia and confer poor outcome. Leukemia. 32:2536–2545. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hu N, Kadota M, Liu H, Abnet CC, Su H, Wu
H, Freedman ND, Yang HH, Wang C, Yan C, et al: Genomic landscape of
somatic alterations in esophageal squamous cell carcinoma and
gastric cancer. Cancer Res. 76:1714–1723. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Golub TR, Barker GF, Lovett M and
Gilliland DG: Fusion of PDGF receptor beta to a novel ets-like
gene, tel, in chronic myelomonocytic leukemia with t(5;12)
chromosomal translocation. Cell. 22:307–316. 1994. View Article : Google Scholar
|
|
23
|
Heilmann AM, Schrock AB, He J, Nahas M,
Curran K, Shukla N, Cramer S, Draper L, Verma A, Erlich R, et al:
Novel PDGFRB fusions in childhood B- and T-acute lymphoblastic
leukemia. Leukemia. 31:1989–1992. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Shimomura Y, Maruoka H and Ishikawa T:
Marked response to imatinib mesylate in a patient with
platelet-derived growth factor receptor beta-associated acute
myeloid leukemia. Int J Hematol. 105:697–701. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Yoshida K, Kuniyasu H, Yasui W, Kitadai Y,
Toge T and Tahara E: Expression of growth factors and their
receptors in human esophageal carcinomas: Regulation of expression
by epidermal growth factor and transforming growth factor alpha. J
Cancer Res Clin Oncol. 119:401–407. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Uguen A and De Braekeleer M: ROS1 fusions
in cancer: A review. Future Oncol. 12:1911–1928. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Rimkunas VM, Crosby KE, Li D, Hu Y, Kelly
ME, Gu TL, Mack JS, Silver MR, Zhou X and Haack H: Analysis of
receptor tyrosine kinase ROS1-positive tumors in non-small cell
lung cancer: Identification of a FIG-ROS1 fusion. Clin Cancer Res.
18:4449–4457. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Roskoski R Jr: ROS1 protein-tyrosine
kinase inhibitors in the treatment of ROS1 fusion protein-driven
non-small cell lung cancers. Pharmacol Res. 121:202–212. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Drilon A, Ou SI, Cho BC, Kim DW, Lee J,
Lin JJ, Zhu VW, Ahn MJ, Camidge DR, Nguyen J, et al: Repotrectinib
(TPX-0005) is a next-generation ROS1/TRK/ALK inhibitor that
potently inhibits ROS1/TRK/ALK solvent-front mutations. Cancer
Discov. 8:1227–1236. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Isobe M, Emanuel BS, Givol D, Oren M and
Croce CM: Localization of gene for human p53 tumour antigen to band
17p13. Nature. 320:84–85. 1986. View
Article : Google Scholar : PubMed/NCBI
|
|
31
|
Preudhomme C and Fenaux P: The clinical
significance of mutations of the P53 tumour suppressor gene in
haematological malignancies. Br J Haematol. 98:502–511. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Nabinger SC, Chen S, Gao R, Yao C,
Kobayashi M, Vemula S, Fahey AC, Wang C, Daniels C, Boswell HS, et
al: Mutant p53 enhances leukemia-initiating cell self-renewal to
promote leukemia development. Leukemia. 33:1535–1539. 2019.
View Article : Google Scholar : PubMed/NCBI
|