Introduction
Breast cancer (BC) is the most common cancer
diagnosed among women in Japan and globally (1). The number of breast cancer cases
among women in Japan was estimated to be the highest at ~92,000 in
2020 (2).
Identification of clinically predictive and
prognostic factors is important in the treatment of BC. Various
prognostic and predictive factors for BC have been recognized by
the College of American Pathologists (CAP) to guide the clinical
management of BC patients. The prognostic factors for BC are lymph
node status, tumor size, lymphatic/vascular invasion, age,
histologic grade, histologic subtypes (i.e. tubular, mucinous, or
papillary), response to neoadjuvant therapy, estrogen receptor
(ER)/progesterone receptor (PgR) status, HER2 gene amplification or
HER2 protein overexpression (3).
Metastasis of the axillary lymph nodes is an indication that the BC
may have spread to other organs. Survival and recurrence are
independent of level of involvement but are directly related to the
number of involved nodes.
There are five main intrinsic or molecular subtypes
of BC that are derived from immunohistochemistry (IHC) of ER/PgR,
HER2, and Ki-67. They are Luminal A, Luminal B, Luminal/HER2, HER2
enriched and Triple Negative (TN) subtypes. The subtypes are
important to predict the biology, response to therapy and prognosis
of each case.
Lymphovascular invasion (LVI) is defined as the
invasion of the vessel walls by tumor cells and/or the presence of
tumor emboli within an endothelial-lined space. LVI may be
considered as the initial stage for lymph node metastasis and other
types of organ metastases. Moreover, LVI is associated with a poor
outcome in several types of cancer such as colorectal (4), urothelial (5), prostate (6) and uterine endometrial cancer
(7) other than BC. The first study
on the prognostic significance of LVI in BC was published in 1964
(8). The purpose of this study was
to evaluate the clinical significance of LVI in primary BC and to
investigate disease-free survival (DFS) as a prognostic marker
according to the BC subtypes. The clinical significance of LVI was
analyzed to investigate the biology and prognosis.
Patients and methods
Patients
This study examined 4,652 consecutive invasive BC
cases excluding the patients with non-invasive cancer, Stage IV and
those who underwent neo-adjuvant therapy from February 2002 to
February 2021 at Kumamoto City Hospital and Kumamoto Shinto General
Hospital. The study protocol was approved by the Institutional
Review Board at Kumamoto Shinto General Hospital. The
clinicopathological factors investigated were menopausal status,
nodal status, lymphovascular invasion (LVI), tumor size, nuclear
grade, ER/PgR and HER2 status, p53 overexpression and the Ki-67
index value. Invasive BC was divided into 5 subtypes according to
the IHC data derived from ER/PgR, HER2 and the Ki-67 index values
(cutoff point: 20%). Informed consent to participate in this study
was obtained from all of the patients. The clinicopathological
characteristics and prognosis of LVI positive and negative tumors
were compared.
Histopathological examination
Immunostaining for ER, PgR, p53, Ki-67 and HER2 was
conducted using the same procedure (9) as the autostainer (Benchmark XT;
Ventana Medical Systems, Inc., Tucson, USA). The positive cell
rates for ER/PgR were determined by IHC using the monoclonal rabbit
ER-antibody SP1/PgR-antibody 1E2 and a value of ≥1% was considered
positive. The antibodies used for IHC were HER2 (clone 4B5; rabbit
monoclonal; all Ventana Medical Systems, Inc.), p53 (clone DO7;
mouse monoclonal) and Ki-67 (clone MIB-1; mouse monoclonal; both
Dako; Agilent Technologies, Inc., Santa Clara, CA, USA). The
positive rate for Ki-67 was calculated based on a count of at least
500 tumor cells in the hot spot and the value was represented as a
percentage. The p53 overexpression was predetermined to be the
number of cases with a positive cell count of ≥50% (10). The HER2 status was dichotomized
into positive and negative cases using IHC and the FISH test. Cases
with IHC3+ (strong and diffuse staining) or FISH amplified were
identified as HER2 positive.
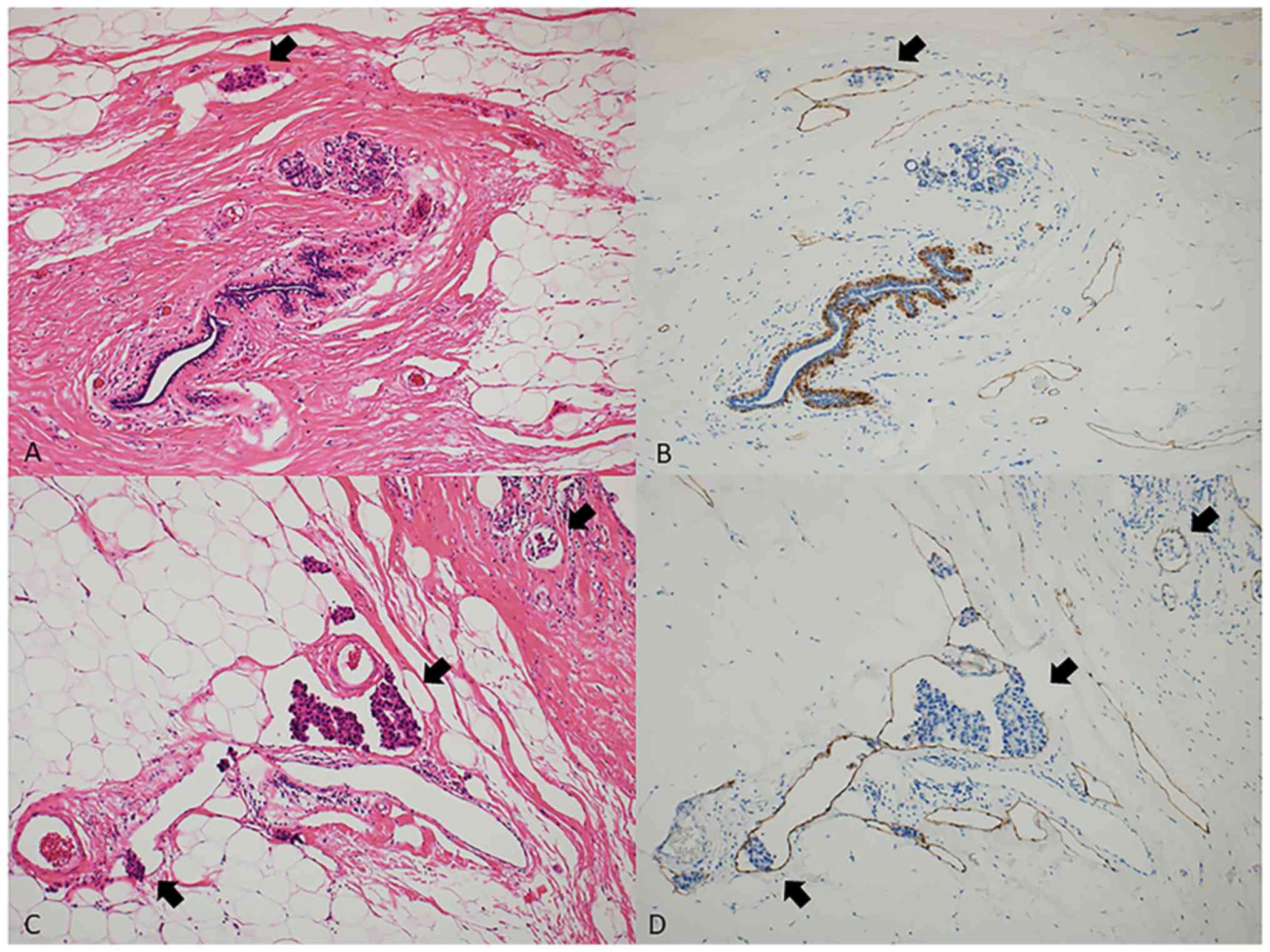
Lymphovascular invasion (LVI)
LVI was routinely evaluated at peritumoral areas in
hematoxylin and eosin (H&E) staining specimens from surgically
resected samples. LVI was defined as the presence of carcinoma
cells (LVI positive; high and low) within the lymphatic vessel.
When the results were undetermined mainly due to the difficulty in
excluding tissue retraction artifacts, a specific marker for
lymphatic endothelium (podoplanin, clone D2-40, mouse monoclonal,
Dako) was used to identify the endothelium-lined lymphatic spaces.
Fig. 1 shows the detection of low
(A and B) and high (C and D) expression of LVI in H&E staining
(A and C, ×100) and D2-40 immunostaining (B and D, ×100) specimens.
A previous study demonstrated that there was a significant
association between routine H&E-stained sections and
immunostaining for D2-40 in 976 lymph node-negative patients
(11). Proper tissue handling of
surgically removed BC tumors is critical for an accurate assessment
of the predictive and prognostic biomarkers (i.e. Ki-67 index
value) and the tissue retraction artifacts are also known to be
caused by insufficient fixation (12). At our hospital great care is taken
to avoid insufficient tissue fixation (13) because an inaccurate assessment of
blood vessel invasion of tumor cells does not provide sufficient
data on the key antibodies CD31, CD34, and podoplanin/D2-40 and
produces a lower frequency of blood vessel invasion (~3%) (12). In this study, we did not use both
CD31 and CD34 antibodies for the detection of LVI.
BC subtypes and adjuvant therapy
Hormone receptor (HR) positive (ER/PgR) and HER2
negative tumors with lower Ki-67 index values (<20%) were
classified as luminal A type, those with higher Ki-67 index values
(≥20%) as luminal B type, HR positive and HER2 positive tumors as
luminal HER2 type, HR negative and HER2 positive tumors as HER2
enriched, and HR negative and HER2 negative tumors as TN type. Most
of the cases with luminal type tumors received endocrine therapy
(tamoxifen or aromatase inhibitor) and most of the cases with TN
and HER2 type were treated with chemotherapy (anthracycline
containing regimen +/- taxane, and anti-HER2 therapy if HER2
positive). Anti-HER2 therapy (trastuzumab) was used in Japan after
receiving approval in 2008.
Statistical analysis
The intergroup comparisons between the LVI-positive
(low and high) and LVI-negative groups were conducted using the
chi-square test and the Fisher's exact test; the P-value applies to
the overall comparison of the three groups. The Kaplan-Meier test
was used to calculate cumulative disease-free survival (DFS) and
tested with the log rank procedure. The univariate and multivariate
analyses for factors related to DFS were performed using the Cox
proportional hazard model (SPSS version 21). The prognosis was
compared between LVI-positive and LVI-negative groups. The median
follow-up period was 95.0 months.
Results
Patient characteristics
Table I shows the
patient characteristics. Out of 4652 cases, 65% of the cases were
postmenopausal, and 70% of the cases had a T1 (<2 cm) tumor and
pathologically negative nodes. In terms of the biological markers,
the ER- and PgR-positive rates were 80.9 and 72.1%, respectively.
HER2 positive cases had a rate of 13.4% and the p53 overexpression
cases had a rate of 15.1%. Low proliferation (Ki-67 ≤20%) was
observed in 40.6% of the cases and high proliferation (50%≤ Ki-67)
in 16% of the cases.
 | Table I.Characteristics of 4,652 patients with
primary breast cancer. |
Table I.
Characteristics of 4,652 patients with
primary breast cancer.
| Characteristic | Number of patients, n
(%) |
|---|
| Menopausal
status |
|
|
Premenopausal | 1,614 (34.7) |
|
Postmenopausal | 3,026 (65.0) |
| Male | 12 (0.3) |
| Tumor size |
|
| T1 | 3,286 (70.6) |
| T2 | 1,205 (25.9) |
| T3,
4 | 120 (2.6) |
|
Unknown | 41 (0.9) |
| Number of involved
nodes |
|
| 0 | 3,242 (69.7) |
| 1-3 | 1,062 (22.8) |
| ≥4 | 338 (7.3) |
|
Unknown | 10 (0.2) |
| Estrogen
receptor |
|
|
Negative | 888 (19.1) |
|
Positive | 3,764 (80.9) |
| Progesterone
receptor |
|
|
Negative | 1,299 (27.9) |
|
Positive | 3,353 (72.1) |
| HER2 |
|
|
Negative | 4,030 (86.6) |
|
Positive | 622 (13.4) |
|
p53-overexpression |
|
|
Without | 3,769 (81.0) |
| With | 701 (15.1) |
|
Unknown | 182 (3.9) |
| Ki-67 |
|
| ≤20% | 1,887 (40.6) |
|
21–49% | 2,022 (43.4) |
| ≥50% | 743 (16.0) |
| Grade |
|
| 1 | 2,466 (53.0) |
| 2 | 1,078 (23.2) |
| 3 | 1,108 (23.8) |
| Total | 4,652 |
Clinicopathological factors and LVI in
primary BC
The LVI expression rates were 29.2% (low: 19.7% and
high: 9.5%) in all primary cases. Table II shows a significant positive
association between the LVI positive rate and the ER/PgR negative
rate (P=0.007 and P=0.01, respectively), HER2 positive rate
(P<0.0001), p53 overexpression (P<0.0001), higher Ki-67 index
values (P<0.0001), higher nuclear grade (P<0.0001), positive
nodes (P<0.0001), and larger tumors (P<0.0001).
| Table II.Clinicopathological factors and LVI in
primary breast cancer (n=4652). |
Table II.
Clinicopathological factors and LVI in
primary breast cancer (n=4652).
|
|
|
| LVI-negative |
|
|
|---|
|
|
|
|
|
|
|
|---|
| Variables | Category | LVI-positive | Low | High | Total |
P-valuea |
|---|
| Menopausal
status | Premenopausal | 1,066 (66.0) | 342 | 206 (12.8) | 1,614 |
|
|
| Postmenopausal | 2,218 (73.3) | 574 | 234 (7.7) | 3,026 | <0.0001 |
|
| Male | 9 (75.0) | 1 | 2 (16.7) | 12 |
|
| Tumor size | T1 | 2,589 (78.8) | 538 | 159 (4.8) | 3,286 |
|
|
| T2 | 623 (51.7) | 342 | 240 (19.9) | 1,205 | <0.0001 |
|
| T3, 4 | 54 (45.0) | 28 | 38 (31.7) | 120 |
|
| Number of Involved
Nodes | 0 | 2,656 (81.9) | 486 | 100 (3.1) | 3,242 |
|
|
| 1-3 | 528 (49.7) | 333 | 201 (18.9) | 1,062 | <0.0001 |
|
| > 4 | 104 (30.8) | 92 | 141 (41.7) | 338 |
|
| Estrogen
receptor | Negative | 597 (67.2) | 184 | 107 (12.0) | 888 |
|
|
| Positive | 2,696 (71.6) | 733 | 335 (8.9) | 3,764 | 0.007 |
| Progesterone
receptor | Negative | 906 (69.7) | 243 | 150 (11.5) | 1,299 |
|
|
| Positive | 2,387 (71.2) | 674 | 292 (8.7) | 3,353 | 0.01 |
| HER2 | Negative | 2,918 (72.4) | 761 | 351 (8.7) | 4,030 |
|
|
| Positive | 375 (60.3) | 156 | 91 (14.6) | 622 | <0.0001 |
| p53
overexpression | Without | 2,693 (71.5) | 741 | 335 (8.9) | 3,769 | ≥ |
|
| With | 442 (63.1) | 160 | 99 (14.1) | 701 | <0.0001 |
| Ki-67 | ≤20% | 1,501 (79.5) | 299 | 87 (4.6) | 1,887 |
|
|
| 21–49% | 1,297 (64.1) | 469 | 256 (12.7) | 2,022 | <0.0001 |
|
| ≥50% | 495 (66.6) | 149 | 99 (13.3) | 743 |
|
| Nuclear grade | 1 | 1,980 (80.3) | 360 | 126 (5.1) | 2,466 |
|
|
| 2 | 615 (57.1) | 315 | 148 (13.7) | 1,078 | <0.0001 |
|
| 3 | 698 (63.0) | 242 | 168 (15.2) | 1,108 |
|
| Total |
| 3,293 | 917 | 442 | 4,652 |
|
BC subtypes and LVI
The subtypes was significantly associated with LVI
positivity; 20% in Luminal A, 34.6% in Luminal B, 40.9% in
Luminal/HER2, 38.1% in HER2 enriched, and 29.8% in TN cases
(Table III).
| Table III.Breast cancer subtypes and LVI. |
Table III.
Breast cancer subtypes and LVI.
|
|
| LVI-positive |
|
|
|---|
|
|
|
|
|
|
|---|
| Subtype | LVI-negative | Low | High | Total | P-value (vs.
Luminal A) |
|---|
| Luminal A | 1,409 (80.0) | 277 | 75 (4.3) | 1,761 | - |
| Luminal B | 1,149 (65.4) | 390 | 219 (12.5) | 1,758 | <0.0001 |
| Luminal/HER2 | 182 (59.1) | 77 | 49 (15.9) | 308 | <0.0001 |
| HER2-enriched | 193 (61.9) | 78 | 41 (13.1) | 312 | <0.0001 |
| Triple
negative | 360 (70.2) | 95 | 58 (11.3) | 513 | <0.0001 |
| Total | 3,293 | 917 | 442 | 4,652 | <0.0001 |
Adjuvant therapy and LVI in primary
BC
There was a significant relationship between the
level of LVI and adjuvant therapy. Most of the cases with negative
LVI did not receive chemotherapy and more than 50% of the cases
with positive LVI had chemo-endocrine therapy (Table IV).
| Table IV.Adjuvant therapy and LVI in primary
breast cancer. |
Table IV.
Adjuvant therapy and LVI in primary
breast cancer.
|
|
| LVI-positive |
|
|
|---|
|
|
|
|
|
|
|---|
| Adjuvant
therapy | LVI-negative | Low | High | Total | P-value (vs.
none) |
|---|
| None | 477 (85.0) | 67 | 17 (3.0) | 561 | - |
| Chemotherapy | 399 (62.1) | 147 | 97 (15.1) | 643 | <0.0001 |
| Endocrine
therapy | 2,034 (78.3) | 445 | 118 (4.5) | 2,597 | 0.0004 |
| Chemo-endocrine
therapy | 378 (44.8) | 258 | 209 (24.8) | 845 | <0.0001 |
| Total | 3,288 | 917 | 441 | 4,644 |
|
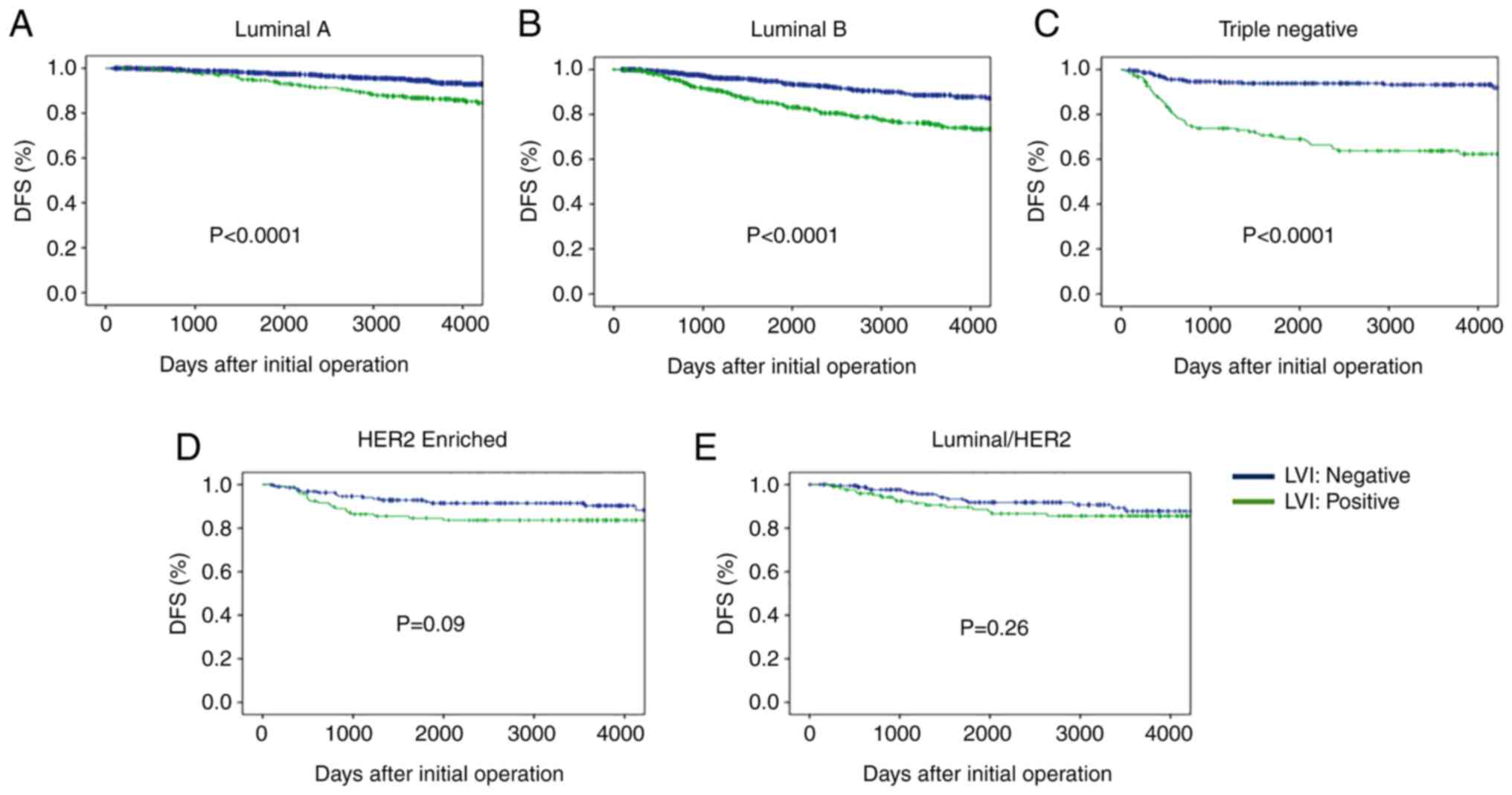
Disease-free survival (DFS) according
to BC subtypes and LVI status
DFS rates after initial treatment according to BC
subtypes are shown in Fig. 2.
Cases with negative LVI had a significantly higher DFS rate than
those with positive LVI in the Luminal A type cases. Similar
findings were observed in the Luminal B type cases. There were
significant differences in DFS between the LVI positive and
negative status in the TN subtypes, but there was no difference in
the Luminal/HER2 and HER2 enriched subtypes (Fig. 2).
Univariate and multivariate analysis of the factors
for DFS were performed using the following factors: tumor size,
nodal status, Ki-67 index value, p53 overexpression, nuclear grade
and LVI. A multivariate analysis revealed that LVI was a
significant factor in Luminal B and TN subtypes and not in
Luminal/HER2 and HER2 enriched subtypes (Table V).
| Table V.Univariate and multivariate analysis
of the factors for DFS according to breast cancer subtypes. |
Table V.
Univariate and multivariate analysis
of the factors for DFS according to breast cancer subtypes.
| A, Luminal A |
|---|
|
|---|
|
|
| P-value |
|---|
|
|
|
|
|---|
| Variables | Category | Univariate | Multivariate |
|---|
| Tumor size | <2/≥2 cm | <0.0001 | 0.006 |
| Nodal status |
Negative/positive | <0.0001 | <0.0001 |
| Ki-67 | ≤20%/>20% | - | - |
| p53
overexpression | With/without | <0.0001 | <0.0001 |
| Nuclear grade | 1+2/3 | 0.065 | 0.25 |
| LVI |
Negative/positive | <0.0001 | 0.12 |
|
| B, Luminal
B |
|
|
|
| P-value |
|
|
|
|
|
Variables |
Category |
Univariate |
Multivariate |
|
| Tumor size | <2/≥2 cm | <0.0001 | 0.0001 |
| Nodal status |
Negative/positive | <0.0001 | 0.007 |
| Ki-67 | ≤20%/>20% | - | - |
| p53
overexpression | With/without | 0.69 | - |
| Nuclear grade | 1+2/3 | 0.064 | 0.17 |
| LVI |
Negative/positive | <0.0001 | <0.0001 |
|
| C,
Luminal/HER2 |
|
|
|
| P-value |
|
|
|
|
|
Variables |
Category |
Univariate |
Multivariate |
|
| Tumor size | <2/≥2 cm | 0.041 | 0.095 |
| Nodal status |
Negative/positive | 0.023 | 0.17 |
| Ki-67 | ≤20%/>20% | 0.18 | - |
| p53
overexpression | With/without | 0.53 | - |
| Nuclear grade | 1+2/3 | 0.41 | - |
| LVI |
Negative/positive | 0.27 | - |
|
| D,
HER2-enriched |
|
|
|
| P-value |
|
|
|
|
|
Variables |
Category |
Univariate |
Multivariate |
|
| Tumor size | <2/≥2cm | 0.033 | 0.092 |
| Nodal status |
Negative/positive | 0.025 | 0.14 |
| Ki-67 | ≤20%/>20% | 0.73 | - |
| p53
overexpression | With/without | 0.23 | - |
| Nuclear grade | 1+2/3 | 0.96 | - |
| LVI |
Negative/positive | 0.09 | 0.75 |
|
| E, Triple
negative |
|
|
|
| P-value |
|
|
|
|
|
Variables |
Category |
Univariate |
Multivariate |
|
| Tumor size | <2/≥2 cm | <0.0001 | <0.0001 |
| Nodal status |
Negative/positive | <0.0001 | <0.0001 |
| Ki-67 | ≤20%/>20% | 0.024 | 0.068 |
| p53
overexpression | With/without | 0.29 | - |
| Nuclear grade | 1+2/3 | 0.23 | - |
| LVI |
Negative/positive | <0.0001 | <0.0001 |
Discussion
The clinical and prognostic significance of LVI in
primary BC, especially in relation to BC subtypes, was investigated
in this retrospective study. The LVI expression rates were 29.2%
(low: 19.7% and high: 9.5%) in all primary BC cases which is
similar to the findings in some studies (11,14–18),
but lower in other studies (19,20).
LVI was significantly associated with premenopausal status, larger
tumors, positive nodes, negative ER/PgR, HER2 positivity, p53
overexpression, higher Ki-67 index value and higher grade. These
findings suggest that a positive LVI may be an indication of
advanced and aggressive characteristics of primary BC tumors.
Our results demonstrate that LVI is a prognostic
factor for predicting patient outcomes. Previous studies reported
the prognostic value of LVI independent of lymph node metastasis as
well as other tumor characteristics such as histological grade, PgR
and HER2 status (11,21,22).
However, some studies reported that LVI was not independently
associated with the outcome in primary BC cases (23,24)
and others reported no association (25,26).
In this study, the clinical significance of LVI was evaluated
according to BC subtypes. Moreover, the subtypes were significantly
associated with LVI positivity (20% in Luminal A, 34.6% in Luminal
B, 40.9% in Lumina/HER2, 38.1% in HER2 enriched, and 29.8% in TN).
Furthermore, a multivariate analysis revealed that LVI was a
significant factor for DFI only in the Luminal B and TN subtypes.
LVI is not a significant prognostic factor for Luminal/HER2 and
HER2 enriched subtypes. Moreover, LVI was found to be a predictive
factor for recurrence in TN BC (27). In a previous study it was reported
(28) that there was a
relationship between Luminal B/HER2(−) and LVI, basal-like and LVI
(P<0.0001, and that there was no significant statistical
difference between LVI and other molecular subtypes. A different
study reported (29) that the
presence of LVI has an independent negative prognostic impact on
survival in early BC patients, except in ER-positive grade 3 tumors
and in those with Luminal A-like tumors treated with adjuvant
chemotherapy. The current study demonstrated that LVI is a
significant predictor for DFS in Luminal B and TN subtypes treated
with chemotherapy. Furthermore, LVI with more than a pathological
complete response (pCR) in surgical BC specimens obtained after
neoadjuvant chemotherapy (NAC) was a significant independent
prognostic factor (29,30). These data suggest that LVI at
initial surgery as well as after chemotherapy is a prognostic
predictor for DFS in early BC.
Kariri et al (2020) stated that LVI develops
through complex molecular pathways and the acquisition of more
invasive migration abilities and that this is an important
phenomenon required for the process of LVI (31). Further mechanistic evaluation is
necessary to explore the inter-relationship of these processes in
BC. Asaoka et al (2020) reported that LVI correlated with
higher genome copy number aberrations, aneuploidy, and homologous
recombination defects. Moreover, tumor immune cell composition and
cytolytic activity was not associated with LVI status, but the
expression of cell proliferation-related genes significantly
increased in LVI positive tumors (32). Kurozumi et al (2019)
reported that LVI correlated with a specific transcriptomic profile
with a potential prognostic value (33). An examination of the potential
factors influencing cell migration in LVI can contribute to an
understanding of the mechanisms of LVI so that a targeted therapy
for BC can be identified (31).
There are two potential limitations in this study.
First, it was a retrospective study. However, the follow-up period
was 95.0 months in more than 4,000 cases and adjuvant treatment was
performed based on the recommendations of the St. Gallen's
International Meeting. Second, the subtypes were identified using
IHC markers. However, the IHC method is cost efficient and does not
need highly experienced technicians.
In conclusion, the clinical significance of LVI was
analyzed to investigate the biology and prognosis of BC cases. LVI
significantly was associated with larger tumors, positive nodes and
aggressive characteristics (i.e. Ki-67, p53 overexpression, nuclear
grade and subtype). Luminal A type had a lower LVI rate and the
HER2 type had a higher LVI rate. Moreover, LVI was a significant
prognostic factor in Luminal B and TN subtypes. These data suggest
that the LVI status is useful in predicting the prognosis for DFS
in HER2 negative BC cases.
Acknowledgements
The abstract was presented at the San Antonio Breast
Cancer Symposium Dec 7–10, 2021 in San Antonio, TX and published as
abstract no. P4-07-12 in Cancer Res 82 (Suppl 4): 2022. The authors
would like thank Dr Toyozumi (Department of Pathology, Kumamoto
City Hospital, Kumamoto, Japan) for their technical assistance and
for the collection of cancer tissue samples.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
RN and NA performed the experiments and conducted
the data analysis. RN was a major contributor to the preparation of
the manuscript. TO, YO, MN, HO and MF made substantial
contributions to the design of the study. RN and NA confirm the
authenticity of all the raw data in this study. All authors have
read and approved the final manuscript.
Ethics approval and consent to
participate
The study protocol was approved by the Institutional
Review Board at Kumamoto Shinto General Hospital (approval no.
2021-J14-001). Written informed consent to participate in this
study was obtained from all of the patients.
Patient consent for publication
All patients or guardians of the patients provided
informed consent for the publication of any associated data.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Torre LA, Siegel RL, Ward EM and Jemal A:
Global cancer incidence and mortality rates and trends-an update.
Cancer Epidemiol Biomarkers Prev. 25:16–27. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Estimated number of cancer cases diagnosed
in women in Japan in 2020 by cancer site. Statista Research
Department; May 7–2021, www.statista.com/statistics/950381/japan-estimated-cancer-incidence-female-by-cancer-site/
|
|
3
|
Chalasani P: What are the prognostic and
predictive factors for breast cancer? Medscape. Feb
04–2021.www.medscape.com/answers/1947145-155277
|
|
4
|
Meguerditchian AN, Bairati I, Lagacé R,
Harel F and Kibrité A: Prognostic significance of lymphovascular
invasion in surgically cured rectal carcinoma. Am J Surg.
189:707–713. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lotan Y, Gupta A, Shariat SF, Palapattu
GS, Vazina A, Karakiewicz PI, Bastian PJ, Rogers CG, Amiel G,
Perotte P, et al: Lymphovascular invasion is independently
associated with overall survival, cause-specific survival, and
local and distant recurrence in patients with negative lymph nodes
at radical cystectomy. J Clin Oncol. 23:6533–6539. 2005. View Article : Google Scholar
|
|
6
|
Herman CM, Wilcox GE, Kattan MW, Scardino
PT and Wheeler TM: Lymphovascular invasion as a predictor of
disease progression in prostate cancer. Am J Surg Pathol.
24:859–863. 2000. View Article : Google Scholar
|
|
7
|
Stålberg K, Bjurberg M, Borgfeldt C,
Carlson J, Dahm-Kähler P, Flöter-Rådestad A, Hellman K, Hjerpe E,
Holmberg E, Kjølhede P, et al: Lymphovascular space invasion as a
predictive factor for lymph node metastases and survival in
endometrioid endometrial cancer-a Swedish gynecologic cancer group
(SweGCG) study. Acta Oncol. 58:1628–1633. 2019. View Article : Google Scholar
|
|
8
|
Teel P: Vascular invasion as a prognostic
factor in breast carcinoma. Surg Gynecol Obstet. 118:1006–1008.
1964.
|
|
9
|
Kai K, Nishimura R, Arima N, Miyayama H
and Iwase H: p53 expression status is a significant molecular
marker in predicting the time to endocrine therapy failure in
recurrent breast cancer: A cohort study. Int J Clin Oncol.
11:426–433. 2006. View Article : Google Scholar
|
|
10
|
Kikuchi S, Osako T, Nishiyama Y, Nakano M,
Tashima R, Fujisue M, Toyozumi Y and Arima N: P53 overexpression in
ductal carcinoma in situ of the breast. J Cytol Histol. 5:269–274.
2014.
|
|
11
|
Rakha EA, Martin S, Lee AH, Morgan D,
Pharoah PD, Hodi Z, Macmillan D and Ellis IO: The prognostic
significance of lymphovascular invasion in invasive breast
carcinoma. Cancer. 118:3670–3680. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hoda SA, Brogi E, Koerner FC and Rosen PP:
Rosen's Breast Pathology. fifth edition. Wolters Kluwer; pp.
p477–482. 2014
|
|
13
|
Arima N, Nishimura R, Osako T, Nishiyama
Y, Fujisue M, Okumura Y, Nakano M, Tashima R and Toyozumi Y: The
importance of tissue handling of surgically removed breast cancer
for an accurate assessment of the Ki-67 index. J Clin Pathol.
69:255–259. 2016. View Article : Google Scholar
|
|
14
|
Debled M, de Mascarel I, Brouste V,
Mauriac L and MacGrogan G: Re: Population-based study of
peritumoral lymphovascular invasion and outcome among patients with
operable breast cancer. J Natl Cancer Inst. 102:275–277. 2010.
View Article : Google Scholar
|
|
15
|
Ejlertsen B, Jensen MB, Rank F, Rasmussen
BB, Christiansen P, Kroman N, Kvistgaard ME, Overgaard M, Toftdahl
DB and Mouridsen HT; Danish Breast Cancer Cooperative Group, :
Population-based study of peritumoral lymphovascular invasion and
outcome among patients with operable breast cancer. J Natl Cancer
Inst. 101:729–735. 2009. View Article : Google Scholar
|
|
16
|
Chas M, Boivin L, Arbion F, Jourdan ML,
Body G and Ouldamer L: Clinicopathologic predictors of lymph node
metastasis in breast cancer patients according to molecular
subtype. J Gynecol Obstet Hum Reprod. 47:9–15. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Houvenaeghel G, Cohen M, Classe JM, Reyal
F, Mazouni C, Chopin N, Martinez A, Daraï E, Coutant C, Colombo PE,
et al: Lymphovascular invasion has a significant prognostic impact
in patients with early breast cancer, results from a large,
national, multicenter, retrospective cohort study. ESMO Open.
6:1003162021. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zhang S, Zhang D, Gong M, Wen L, Liao C
and Zou L: High lymphatic vessel density and presence of
lymphovascular invasion both predict poor prognosis in breast
cancer. BMC Cancer. 17:3352017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Akrami M, Meshksar A, Ghoddusi JM,
Safarpour MM, Tahmasebi S, Zangouri V and Talei A: Prognostic role
of lymphovascular invasion in patients with early breast cancer.
Indian J Surg Oncol. 12:671–677. 2021. View Article : Google Scholar
|
|
20
|
Mohammed ZM, McMillan DC, Edwards J,
Mallon E, Doughty JC, Orange C and Going JJ: The relationship
between lymphovascular invasion and angiogenesis, hormone
receptors, cell proliferation and survival in patients with primary
operable invasive ductal breast cancer. BMC Clin Pathol. 13:312013.
View Article : Google Scholar
|
|
21
|
Mohammed RA, Martin SG, Mahmmod AM,
Macmillan RD, Green AR, Paish EC and Ellis IO: Objective assessment
of lymphatic and blood vascular invasion in lymph node-negative
breast carcinoma: Findings from a large case series with long-term
follow-up. J Pathol. 223:358–365. 2011. View Article : Google Scholar
|
|
22
|
Pinder SE, Ellis IO, Galea M, O'Rouke S,
Blamey RW and Elston CW: Pathological prognostic factors in breast
cancer. III. Vascular invasion: Relationship with recurrence and
survival in a large study with long-term follow-up. Histopathology.
24:41–47. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Freedman GM, Li T, Polli LV, Anderson PR,
Bleicher RJ, Sigurdson E, Swaby R, Dushkin H, Patchefsky A and
Goldstein L: Lymphatic space invasion is not an independent
predictor of outcomes in early stage breast cancer treated by
breast-conserving surgery and radiation. Breast J. 18:415–419.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ovcaricek T, Frkovic SG, Matos E, Mozina B
and Borstnar S: Triple negative breast cancer-prognostic factors
and survival. Radiol Oncol. 45:46–52. 2011. View Article : Google Scholar
|
|
25
|
Camp RL, Rimm EB and Rimm DL: A high
number of tumor free axillary lymph nodes from patients with lymph
node negative breast carcinoma is associated with poor outcome.
Cancer. 88:108–113. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kim SH, Simkovich-Heerdt A, Tran KN,
Maclean B and Borgen PI: Women 35 years of age or younger have
higher locoregional relapse rates after undergoing breast
conservation therapy. J Am Coll Surg. 187:1–8. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Na YM, Ryu YJ, Cho JS, Park MH and Yoon
JH: Lymphovascular invasion as a predictive factor for recurrence
in triple-negative breast cancer. Indian J Surg. 83:475–483. 2021.
View Article : Google Scholar
|
|
28
|
Morkavuk ŞB, Güner M, Çulcu S, Eroğlu A,
Bayar S and Ünal AE: Relationship between lymphovascular invasion
and molecular subtypes in invasive breast cancer. Int J Clin Pract.
75:e138972021. View Article : Google Scholar
|
|
29
|
Hamy AS, Lam GT, Laas E, Darrigues L,
Balezeau T, Guerin J, Livartowski A, Sadacca B, Pierga JY,
Vincent-Salomon A, et al: Lymphovascular invasion after neoadjuvant
chemotherapy is strongly associated with poor prognosis in breast
carcinoma. Breast Cancer Res Treat. 169:295–304. 2018. View Article : Google Scholar
|
|
30
|
Ryu YJ, Kang SJ, Cho JS, Yoon JH and Park
MH: Lymphovascular invasion can be better than pathologic complete
response to predict prognosis in breast cancer treated with
neoadjuvant chemotherapy. Medicine (Baltimore). 97:e116472018.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kariri YA, Aleskandarany MA, Joseph C,
Kurozumi S, Mohammed OJ, Toss MS, Green AR and Rakha EA: Molecular
complexity of lymphovascular invasion: The role of cell migration
in breast cancer as a prototype. Pathobiology. 87:218–231. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Asaoka M, Patnaik SK, Zhang F, Ishikawa T
and Takabe K: Lymphovascular invasion in breast cancer is
associated with gene expression signatures of cell proliferation
but not lymphangiogenesis or immune response. Breast Cancer Res
Treat. 181:309–322. 2020. View Article : Google Scholar
|
|
33
|
Kurozumi S, Joseph C, Sonbul S, Alsaeed S,
Kariri Y, Aljohani A, Raafat S, Alsaleem M, Ogden A, Johnston SJ,
et al: A key genomic subtype associated with lymphovascular
invasion in invasive breast cancer. Br J Cancer. 120:1129–1136.
2019. View Article : Google Scholar : PubMed/NCBI
|