Introduction
Neuroendocrine carcinoma (NEC) of the esophagus
(E-NEC) is rare, accounting for ~1% of all esophageal malignancies
(1,2). NEC is defined as a poorly
differentiated carcinoma with neuroendocrine differentiation and a
Ki-67 proliferation index >20%, consisting of small cell
carcinoma and large cell carcinoma, as described in the World
Health Organization (WHO) classification (3). It is an aggressive disease with high
rates of lymph node and distant metastases at the time of diagnosis
(4–6). In addition, even patients with
surgically resectable E-NEC often experience postoperative tumor
relapse, resulting in poor prognosis (6). Thus, a careful decision on the optimal
surgery is required (7,8). However, postoperative prognostic
predictors for E-NEC have yet to be established.
MicroRNAs (miRNAs/miRs) are small, non-coding RNAs
of 18–22 nucleotides in length that bind to their target mRNAs and
play a key role in cancer initiation and progression by regulating
post-transcriptional gene expression (9). A number of miRNAs have been reported
to be potential biomarkers for the detection, classification,
therapeutic effects and prognosis of different types of cancer
(10–12). In addition, miRNAs are stable and
can be detected in formalin-fixed paraffin-embedded (FFPE) archive
specimens (13,14), enabling the molecular features of
rare diseases to be analyzed.
The aim of the present study was to assess the role
of surgery in the multidisciplinary treatment of the patients with
resectable E-NEC. Furthermore, the miRNAs that are associated with
treatment outcome were investigated.
Materials and methods
Patients and surgical specimens
The present work was conducted as a multicenter
retrospective study of the Japan Neuroendocrine Tumor Society
(JNETS). The study protocol was approved by the ethics review board
of the University of Toyama Hospital (approval no. R27-109; Toyoma,
Japan), and by institutional review board of each participating
JNETS partner hospital (Table SI).
Written informed consent or opt-out consent was obtained from all
participants.
A total of 36 patients with E-NEC who underwent
curative surgery at JNETS partner hospitals and whose FFPE tumor
sections were available were recruited. The mean age of the 36
enrolled patients was 62.6 years old (range, 52–75 years) with a
male-to-female ratio of 2.6:1. The patients were enrolled and
samples were collected between February 2017 and August 2019.
Patients who met all of the following criteria were eligible: i)
Patients who underwent curative surgery and were diagnosed with
E-NEC based on histopathological findings of the resection
specimen; ii) patients with a preserved FFPE block in both the
cancerous and non-cancerous areas of the surgical specimen; iii)
patients with available prognostic and clinicopathological data;
and iv) patients between the ages of 20 and 80 years at the time of
surgery. Patients with concurrent or iatrogenic multiple advanced
cancers were excluded from this study.
All tumors were histologically diagnosed as poorly
differentiated NEC, based on the WHO Classification of Endocrine
Organs (2017) (15) and Digestive
System (2019) histologic criteria (3). Pathological diagnosis was made by the
bord certificated pathologist in each participating hospital. In
available cases, the diagnosis was made with reference to the
neuroendocrine marker expression, such as synaptophysin,
chromogranin A, neural cell adhesion molecule 1 (NCAM) and neuron
specific enolase (NSE). All cases were staged according to the 7th
edition of the Union for International Cancer Control system
(16). Response evaluation for
preoperative treatment was performed according to the response
evaluation criteria in solid tumors (RECIST) (17).
RNA extraction and miRNA expression
profiling
The FFPE samples of the tumors (T) and their normal
counterparts (N) were obtained for each case, sections (100 µm)
were prepared, and total RNA was extracted. The detailed procedure
of this experiment is previously described (14). The boundaries of the tumor margins
in the tumor or the mucosal layer in the normal counterparts were
marked with loupe images, and the RNA was extracted using a
silica-based spin column (Toray Industries Inc.) after trimming the
sections (Fig. S1), so that
>70% of the target cells are harvested.
Samples in which electrophoresis was performed using
an Agilent 2100 Bioanalyzer (Agilent Technologies, Inc.) showed
either the majority of RNAs at ≥4,000 nucleotides due to
cross-linking, or the majority of RNAs at ≤1,000 nucleotides due to
degradation, were deemed unsuitable for miRNA analysis.
Extracted RNA samples were labeled with the 3D-Gene
miRNA labeling kit (Toray Industries, Inc.) and hybridized to a
3D-Gene Human miRNA Oligo chip (cat. no. IH201; Toray Industries
Inc.) mounted with 2,632 genes. The fluorescent signals were
scanned with the 3D-Gene Scanner (Toray Industries, Inc.). The
miRNAs with low expression levels (less than threshold 100 of the
global normalization value) were excluded from comparison between
relapse and non-relapse groups. The tumor-to-normal ratio (T/N
ratio) was calculated based on the miRNA expression levels in each
tumor and the corresponding normal counterpart.
Statistical analysis
Relationships between clinicopathological factors
and postoperative tumor relapse were assessed using Fisher's exact
test. Survival times were calculated either from the date of
surgery to the death of the patient or the last clinical follow-up
date, with survival distributions estimated using the Kaplan-Meier
method and compared using the log-rank test. Relationships between
miRNA expression and clinicopathological factors were assessed
using unpaired Student's t-test. P<0.05 was considered to
indicate a statistically significant difference. Hierarchical
clustering analysis was performed by Ward's method. Pearson's
correlation coefficients of 0.6<r<1 and −1<r<-0.6
(|r|>0.6) were considered as significant positive and negative
relationships respectively.
For the importance analysis of miRNAs,
machine-learning classifier was employed to distinguish between the
relapse and non-relapse group. As a model-dependent method, a model
was trained to classify the presence of recurrence using Random
Forest (18). The miRNAs that
contributed to the classification in the model were evaluated using
Gini importance. On the other hand, Permutation Importance
(19) was used as a
model-independent method to determine the importance of features
associated with recurrence. A permutation importance P<0.05 and
Gini importance (GI) ≥0.015 were considered to indicate a
statistically significant difference.
Results
Clinical information and tumor
characteristics of 36 enrolled patients
The mean age of the 36 enrolled patients was 62.6
years old (ranging from 52 to 75 years) with a male-to-female ratio
of 2.6:1. A total of 34 (94.4%) patients had small cell type,
whereas 2 (5.6%) patients had large cell type; 18 (50.0%) patients
had pure NEC, whereas 18 (50.0%) patients had mixed
neuroendocrine-non-neuroendocrine neoplasm (MiNEN), in which NEC
was combined with squamous cell carcinoma or adenocarcinoma, or
both. The neuroendocrine marker synaptophysin, chromogranin A, NCAM
and NSE were positive in 27/28 (96.4%), 17/28 (60.7%), 16/21
(76.2%) and 5/11 (45.5%) of the examined tumors, respectively.
All 36 patients underwent surgery with no residual
tumors (R0). Subsequently, 24 (85.7%) of 28 patients with stage
II–IV disease received perioperative chemo- or
chemoradio-therapy.
Among the 36 patients, 16 (44.4%) patients achieved
disease-free survival within the median observation period of 144
(ranging from 46 to 242) months, whereas 17 (47.2%) patients died
of tumor relapse and 3 (8.3%) patients survived with tumor relapse
at a median observation period of 13 (1–106) months after surgery (P=0.004).
These two groups were referred to as the non-relapse group (n=16)
and relapse group (n=20).
As summarized in Table
I, there was no statistical difference between the relapse and
non-relapse group in terms of clinicopathological parameters, such
as age, sex, tumor location, tumor depth, lymph node metastasis,
distant metastasis (M1 lymph), TNM staging, histological type,
neuroendocrine marker expression (synaptophysin, chromogranin A,
NCAM, NSE), surgical procedures and perioperative chemo- or
chemoradiotherapy. Within the 10 patients who received preoperative
chemo- or chemoradiotherapy, no relationship was seen between
treatment response (RECIST) and tumor relapse.
 | Table I.Clinicopathological characteristics
of the patients. |
Table I.
Clinicopathological characteristics
of the patients.
|
| All patients
(n=36) | Patients with miRNA
analysis (n=11) |
|---|
|
|
|
|
|---|
| Characteristic | Non-relapse | Relapse | P-value | Non-relapse | Relapse | P-value |
|---|
| Case number | 16 | 20 |
| 5 | 6 |
|
| Age (years), mean ±
SD | 62±6 | 63±6 | 0.933 | 65±6 | 61±9 | 0.486 |
| Sex |
|
|
|
|
|
|
|
Male | 11 | 15 | 0.723 | 3 | 4 | >0.999 |
|
Female | 5 | 5 |
| 2 | 2 |
|
| Tumor location |
|
|
|
|
|
|
|
Upper/Middle thoracic | 9 | 13 | 0.734 | 4 | 3 | 0.546 |
| Lower
thoracic | 7 | 7 |
| 1 | 3 |
|
| Pathological tumor
depth |
|
|
|
|
|
|
|
T1-2 | 9 | 14 | 0.493 | 4 | 6 | 0.455 |
|
T3-4 | 7 | 6 |
| 1 | 0 |
|
| Lymph node
metastasis |
|
|
|
|
|
|
| N0 | 7 | 3 | 0.073 | 3 | 2 | 0.567 |
|
N1-2 | 9 | 17 |
| 2 | 4 |
|
| Distant
metastasis |
|
|
|
|
|
|
| M0 | 15 | 18 | 0.840 | 5 | 6 | - |
| M1
lymph | 1 | 2 |
| 0 | 0 |
|
| TNM stage |
|
|
|
|
|
|
|
1-2 | 11 | 8 | 0.107 | 5 | 5 | >0.999 |
|
3-4 | 5 | 12 |
| 0 | 1 |
|
| Histology |
|
|
|
|
|
|
| Small
cell | 16 | 18 | 0.492 | 5 | 6 | - |
| Large
cell | 0 | 2 |
| 0 | 0 |
|
| Pure
NEC | 8 | 10 | >0.999 | 4 | 3 | 0.546 |
|
MiNEN | 8 | 10 |
| 1 | 3 |
|
|
SCC | 7 | 7 |
| 1 | 2 |
|
|
Adeno | 1 | 2 |
| 0 | 0 |
|
| SCC +
Adeno | 0 | 1 |
| 0 | 1 |
|
| Lymphatic vessel
invasion |
|
|
|
|
|
|
|
Negative | 5 | 8 | 0.533 | 1 | 3 | 0.546 |
|
Positive | 10 | 11 |
| 4 | 3 |
|
|
Unknown | 1 | 1 |
| 0 | 0 |
|
| Venous
invasion |
|
|
|
|
|
|
|
Negative | 5 | 7 | 0.861 | 2 | 5 | 0.242 |
|
Positive | 9 | 13 |
| 3 | 1 |
|
|
Unknown | 2 | 0 |
| 0 | 0 |
|
| Synaptophysin |
|
|
|
|
|
|
|
Negative | 1 | 0 | 0.472 | 1 | 0 | 0.456 |
|
Positive | 11 | 16 |
| 4 | 6 |
|
|
Unknown | 4 | 4 |
| 0 | 0 |
|
| Chromogranin A |
|
|
|
|
|
|
|
Negative | 5 | 6 | 0.901 | 1 | 1 | 0.355 |
|
Positive | 8 | 9 |
| 4 | 3 |
|
|
Unknown | 3 | 5 |
| 0 | 2 |
|
| NCAM |
|
|
|
|
|
|
|
Negative | 2 | 3 | 0.964 | 1 | 0 | 0.452 |
|
Positive | 7 | 9 |
| 2 | 4 |
|
|
Unknown | 7 | 8 |
| 2 | 2 |
|
| NSE |
|
|
|
|
|
|
|
Negative | 5 | 1 | 0.057 | 1 | 1 | 0.491 |
|
Positive | 3 | 2 |
| 1 | 0 |
|
|
Unknown | 8 | 17 |
| 3 | 5 |
|
| Operation |
|
|
|
|
|
|
|
Subtotal esophagectomy | 15 | 20 | 0.444 | 5 | 6 | - |
| Lower
esophagectomy | 1 | 0 |
| 0 | 0 |
|
| Lymph node
dissection |
|
|
|
|
|
|
|
Two-field | 7 | 6 | 0.493 | 1 | 2 | >0.999 |
|
Three-field | 9 | 14 |
| 4 | 4 |
|
| D1 | 1 | 0 | 0.459 | 0 | 0 | 0.567 |
| D2 | 11 | 13 |
| 2 | 4 |
|
| D3 | 4 | 7 |
| 3 | 2 |
|
| Curability |
|
|
|
|
|
|
| R0 | 16 | 20 | - | 5 | 6 | - |
| R1 | 0 | 0 |
| 0 | 0 |
|
|
Preoperative chemotherapy | 2 | 7 | 0.133 | 0 | 2 | - |
|
DCF | 1 | 2 |
| 0 | 1 |
|
| FP | 1 | 1 |
| 0 | 0 |
|
|
CDDP/CPT11 | 0 | 3 |
| 0 | 1 |
|
|
CDDP/ETP | 0 | 1 |
| 0 | 0 |
|
| Preoperative
CRT | 0 | 1 | >0.999 | 0 | 0 | - |
| (FP +
radiation) |
|
|
|
|
|
|
| Response to
preoperative treatment (RECIST) |
|
|
|
|
|
|
| CR | 0 | 0 | 0.856 | 0 | 0 | - |
| PR | 1 | 4 |
| 0 | 1 |
|
| SD | 1 | 3 |
| 0 | 1 |
|
| PD | 0 | 0 |
| 0 | 0 |
|
|
Unknown | 0 | 1 |
| 0 | 0 |
|
| Postoperative
chemotherapy | 10 | 10 | - | 4 | 3 | 0.546 |
|
CDDP/5FU | 4 | 4 |
| 0 | 0 |
|
|
CDDP/ETP | 2 | 0 |
| 2 | 0 |
|
|
CDDP/CPT11 | 2 | 5 |
| 2 | 3 |
|
|
NDP/DOC | 1 | 0 |
| 0 | 0 |
|
|
TS1 | 1 | 1 |
| 0 | 0 |
|
| Postoperative
CRT | 2 | 0 | 0.191 | 0 | 0 | - |
| Observation period
(median, range) | 144 (46–242) | 13 (1–106) | 0.004 | 51 (46–82) | 27.5 (7–106) | 0.003 |
| Duration between
surgery and tumor relapse | - | 6 (1–25) | - | - | 8 (3–25) | - |
| Type of tumor
relapse |
|
|
|
|
|
|
| H |
| 7 |
| 1 | - |
|
| Ly |
| 5 |
| 2 |
|
|
| L |
| 0 |
| 0 |
|
|
| Pl |
| 0 |
| 0 |
|
|
| P |
| 0 |
| 0 |
|
|
| H +
Ly |
| 3 |
| 3 |
|
|
| H + Ly
+ L |
| 1 |
| 0 |
|
|
| H + Ly
+ L + Pl |
| 1 |
| 0 |
|
|
| H + Ly
+ L + P |
| 1 |
| 0 |
|
|
| Ly +
L |
| 1 |
| 0 |
|
|
| Ly +
P |
| 1 |
| 0 |
|
|
| Chemotherapy after
relapse |
| 18 |
| - | 5 | - |
|
CDDP/5FU |
| 3 |
|
| 1 |
|
|
CDDP/ETP |
| 6 |
|
| 3 |
|
|
CDDP/CPT11 |
| 6 |
|
| 1 |
|
|
Others |
| 3 |
|
| 0 |
|
| RT after
relapse |
| 7 |
|
| 0 |
|
| Prognosis |
|
|
|
|
|
|
|
Disease-free survival | 16 | 0 |
| 5 | 0 |
|
|
Survival with relapse | 0 | 3 |
| 0 | 1 |
|
| Cancer death |
|
|
|
|
|
|
|
Cause-specific death | 0 | 17 |
| 0 | 5 |
|
| Death
of other diseases | 0 | 0 |
| 0 | 0 |
|
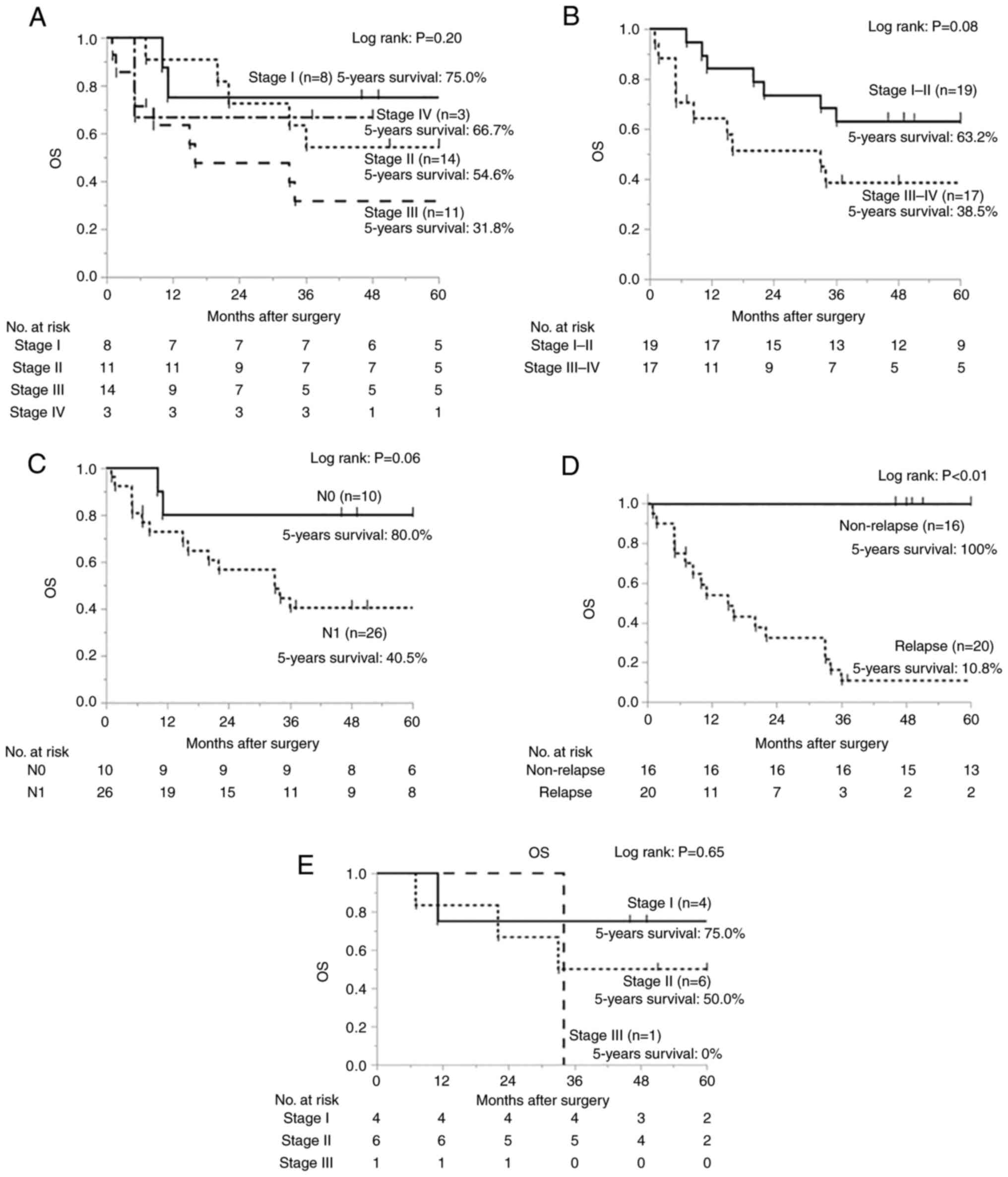
The median follow-up time of the 36 enrolled
patients was 36.5 months (range, 1–242) and the 5-year overall
survival (OS) rate was 51.7%. Kaplan-Meier curves of the OS
stratified by TNM stage showed no significant difference among
patients with stage I, stage II, stage III, and stage IV diseases
(P=0.20; Fig. 1A). Patients with
stage I–II diseases showed a trend to a longer survival time
compared with those with stage III–IV diseases; however, there was
no significant difference (P=0.08; Fig.
1B). Patients with negative lymph node metastasis trended
towards a longer survival time compared with those with positive
lymph node metastasis (P=0.06; Fig.
1C). The 5-year OS rate of the non-relapse and relapse group
were 100% and 10.8%, respectively (P<0.01; Fig. 1D). There was no significant
correlation between adjuvant therapies and postoperative survival
(P=0.45; Fig. S2).
Clinical information and tumor
characteristics of 11 patients whose samples underwent miRNA
expression analysis
In the 36 enrolled patients, total RNA was extracted
from 30 patients with sufficient FFPE blocks to cut sections. Then,
high-quality RNA was obtained for paired T/N samples from 11 of the
30 patients and used in miRNA profiling (Fig. S3).
The mean age of the 11 patients was 62.7 years old
(range, 52–75) with a male-to-female ratio of 1.8:1. All 11
patients had small cell type. Overall, 7 of 11 (63.6%) patients had
pure NEC, whereas 4 (36.4%) patients had MiNEN. A total of 8 of 11
(72.7%) patients, and 6 of 7 (85.7%) patients with stage II–IV
disease received perioperative chemotherapy (data not shown).
Among the 11 patients, 5 (45.5%) patients achieved
disease-free survival with a median observation period of 51
(range, 46–82) months, whereas 5 (45.5%) patients died of tumor
relapse and 1 (9.1%) patient survived with tumor relapse at a
median observation period of 27.5 (range, 7–106) months after
surgery (P=0.003) (Table I). These
two groups were referred to as the non-relapse group (n=5) and
relapse group (n=6). As summarized in Table I, there was no statistical
difference between the relapse and non-relapse group in
clinicopathological parameters.
The median follow-up time of the 11 patients was
46.0 (range, 7–106) months and the 5-year OS rate was 54.6% (data
not shown). Kaplan-Meier curves stratified by TNM stage showed no
significant difference among patients with stage I, stage II and
stage III diseases (P=0.65; Fig.
1E).
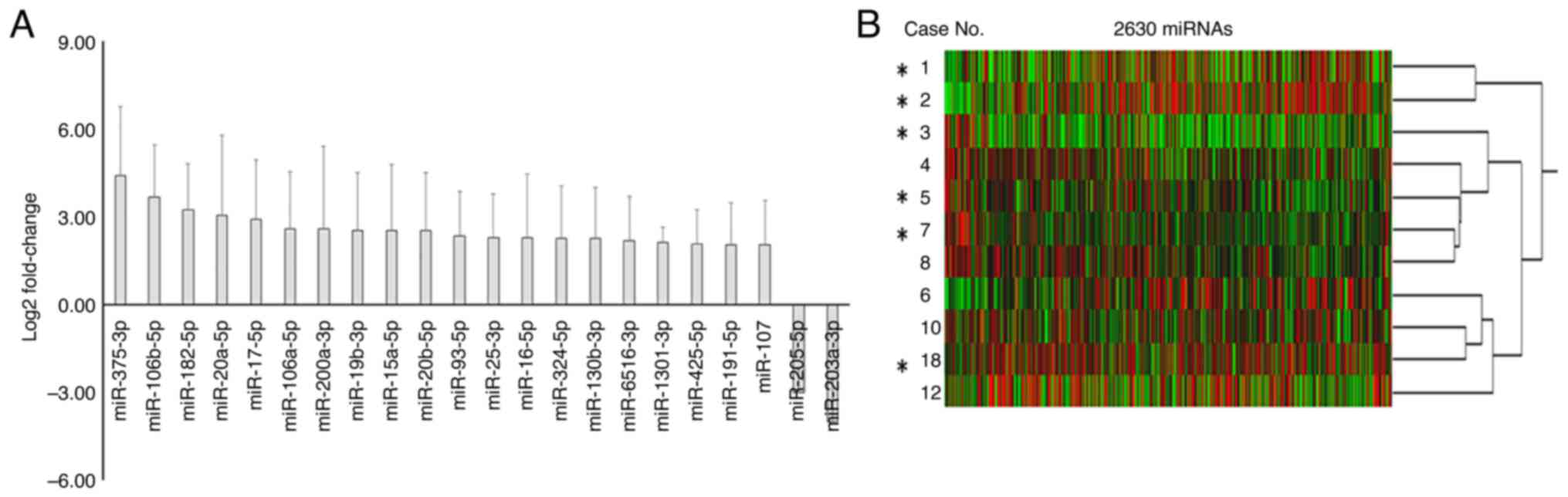
Expression of miRNAs in FFPE samples
of 11 cases detected by microarray
In the 2,632 miRNAs assessed using the miRNA oligo
chip, two miRNAs were not detected in any of the samples, thus
2,630 miRNAs were analyzed. Comparison between the average miRNA
expression levels in the 11 NEC tumors and 11 corresponding normal
tissues revealed that the tumors expressed 20 miRNAs >2-fold
higher, and two miRNAs were expressed >2-fold lower, compared
with their normal counterparts (Fig.
2A). Hierarchical clustering based on 2,630 detected miRNAs did
not show any relationship between clusters and postoperative tumor
relapse (Fig. 2B).
Differentially expressed miRNAs
between patients with and without postoperative tumor relapse
To identify miRNAs that accurately differentiate
patients with and without postoperative tumor relapse, miRNAs with
very low expression (less than threshold 100 of the global
normalization value) were excluded, yielding 337 miRNAs for further
analysis. When the expression (T/N ratio) of miRNAs was compared
between relapse (n=6) and non-relapse (n=5) cases, based on the
difference between the averages of the two groups using the t-test,
the lower expression of five miRNAs (miR-1246, miR-1249-3p,
miR-296-5p, miR-6805-3p and miR-12136) and higher expression of
nine miRNAs (miR-1260a, miR-1260b, miR-4284, miR-612, miR-575,
miR-6822-5p, miR-5088-5p, miR-7977 and miR-4454) correlated with
postoperative tumor relapse (P<0.05; data not shown).
Taking into account correlation coefficients, the
lower expression of five miRNAs and higher expression of 12 miRNAs
correlated with postoperative tumor relapse (|r|>0.6). Using
random forest, the lower expression of four miRNAs and higher
expression of 10 miRNAs correlated with postoperative tumor relapse
(GI≥0.015). Using permutation importance, the lower expression of
five miRNAs and higher expression of 13 miRNAs correlated with
postoperative tumor relapse (P<0.05). A merged table of miRNA
lists identified 22 miRNAs extracted by these analyses (Table II).
| Table II.miRNAs identified by either of the
statistical methods. |
Table II.
miRNAs identified by either of the
statistical methods.
|
|
|
|
|
|
| Random forest |
|
|
|
|---|
|
|
|
|
|
|
|
|
| Hierarchical
cluster analysis |
|---|
|
|
|
|
|
|
|
| 95% CI | Permutation
importance (P-value) |
|
|---|
|
|
|
|
|
|
|
|
| ≤12
differentiatede | ≥3
differentiatede |
|---|
| miRNA |
Non-relapsea |
Relapsea | Up- or
downregulationb |
P-valuec |
R-valued | Giniimportance | Upper | Lower |
|---|
| miR-1260a | −1.10±0.40 | −0.12±0.17 | 0.99 | 0.003 | 0.878f | 0.037f | 0.03734 | 0.03742 | 0.002f | Yes | Yes |
| miR-1260b | −1.22±0.48 | −0.17±0.17 | 1.05 | 0.006 | 0.860f | 0.037f | 0.03734 | 0.03741 | 0.002f | Yes | Yes |
| miR-1246 | 1.54±0.33 | 0.97±0.21 | −0.57 | 0.013 | −0.761f | 0.037f | 0.03733 | 0.03740 | 0.002f | Yes | Yes |
| miR-4284 | −0.36±0.22 | 0.52±0.60 | 0.88 | 0.013 | 0.721f | 0.018f | 0.01756 | 0.01761 | 0.035f | Yes |
|
| miR-612 | −0.51±0.04 | −0.22±0.20 | 0.29 | 0.016 | 0.722f | 0.018f | 0.01805 | 0.01809 | 0.013f | Yes |
|
| miR-1249-3p | 0.00±0.10 | −0.18±0.11 | −0.19 | 0.017 | −0.692f | 0.017f | 0.01736 | 0.01741 | 0.016f | Yes |
|
| miR-296-5p | 0.17±0.12 | −0.04±0.12 | −0.21 | 0.020 | −0.690f | 0.016f | 0.01577 | 0.01581 | 0.023f | Yes |
|
| miR-575 | −0.62±0.13 | −0.25±0.27 | 0.37 | 0.020 | 0.677f | 0.018f | 0.01749 | 0.01754 | 0.010f | Yes |
|
| miR-6805-3p | 0.14±0.09 | −0.02±0.10 | −0.16 | 0.023 | −0.672f | 0.016f | 0.01579 | 0.01583 | 0.022f | Yes |
|
| miR-12136 | 0.62±0.15 | 0.26±0.28 | −0.35 | 0.029 | −0.645f | 0.012 | 0.01172 | 0.01176 | 0.027f | Yes |
|
| miR-6822-5p | −0.86±0.47 | −0.25±0.20 | 0.61 | 0.040 | 0.696f | 0.015f | 0.01501 | 0.01505 | 0.029f | Yes |
|
| miR-5088-5p | −0.14±0.11 | 0.08±0.19 | 0.22 | 0.042 | 0.607f | 0.005 | 0.00530 | 0.00532 | 0.289 |
|
|
| miR-7977 | −0.86±0.60 | −0.13±0.26 | 0.74 | 0.049 | 0.674f | 0.007 | 0.00690 | 0.00693 | 0.082 |
|
|
| miR-4454 | −1.13±0.70 | −0.27±0.34 | 0.85 | 0.049 | 0.663f | 0.015f | 0.01531 | 0.01535 | 0.020f | Yes |
|
| miR-375-5p | −0.79±0.58 | −0.13±0.32 | 0.66 | 0.063 | 0.626f | 0.007 | 0.00666 | 0.00669 | 0.125 |
|
|
| miR-7975 | −1.51±0.97 | −0.45±0.28 | 1.05 | 0.072 | 0.648f | 0.008 | 0.00845 | 0.00848 | 0.105 |
|
|
| miR-4286 | −1.39±1.06 | −0.34±0.26 | 1.05 | 0.091 | 0.619f | 0.015f | 0.01500 | 0.01504 | 0.027f |
|
|
| miR-4746-3p | −0.28±0.09 | −0.15±0.13 | 0.13 | 0.091 | 0.521 | 0.015f | 0.01535 | 0.01540 | 0.013f |
|
|
| miR-4443 | −0.95±0.69 | −0.32±0.19 | 0.63 | 0.114 | 0.581 | 0.015f | 0.01468 | 0.01473 | 0.039f |
|
|
| miR-8069 | −0.15±0.29 | −0.07±0.15 | 0.08 | 0.611 | 0.186 | 0.006 | 0.00569 | 0.00572 | 0.041f |
|
|
| miR-4690-5p | −0.45±0.17 | −0.22±0.19 | 0.23 | 0.067 | 0.566 | 0.009 | 0.00889 | 0.00892 | 0.043f |
|
|
| miR-3917 | −0.34±0.20 | −0.18±0.20 | 0.17 | 0.207 | 0.416 | 0.009 | 0.00874 | 0.00877 | 0.048f |
|
|
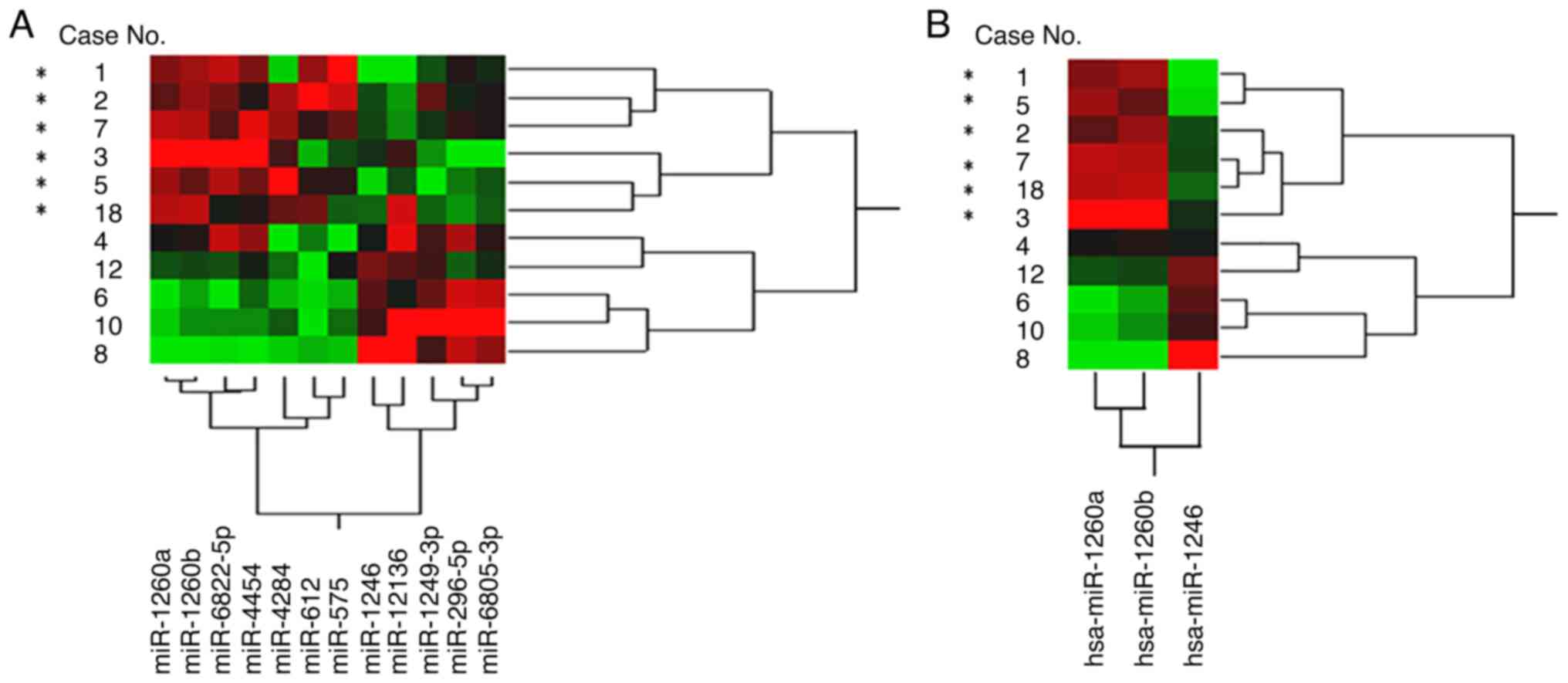
Hierarchical clustering based on the 22 miRNAs did
not show relationships between clusters and postoperative tumor
relapse (Fig. S4); however, a
maximum 12 miRNAs (miR-1260a, miR-1260b, miR-1246, miR-4284,
miR-612, miR-1249-3p, miR-296-5p, miR-575, miR-6805-3p, miR-12136,
miR-6822-5p and miR-4454) and a minimum of three miRNAs (miR-1260a,
miR-1260b and miR-1246) within the 22 miRNAs differentiated between
relapse and non-relapse groups (Fig.
3).
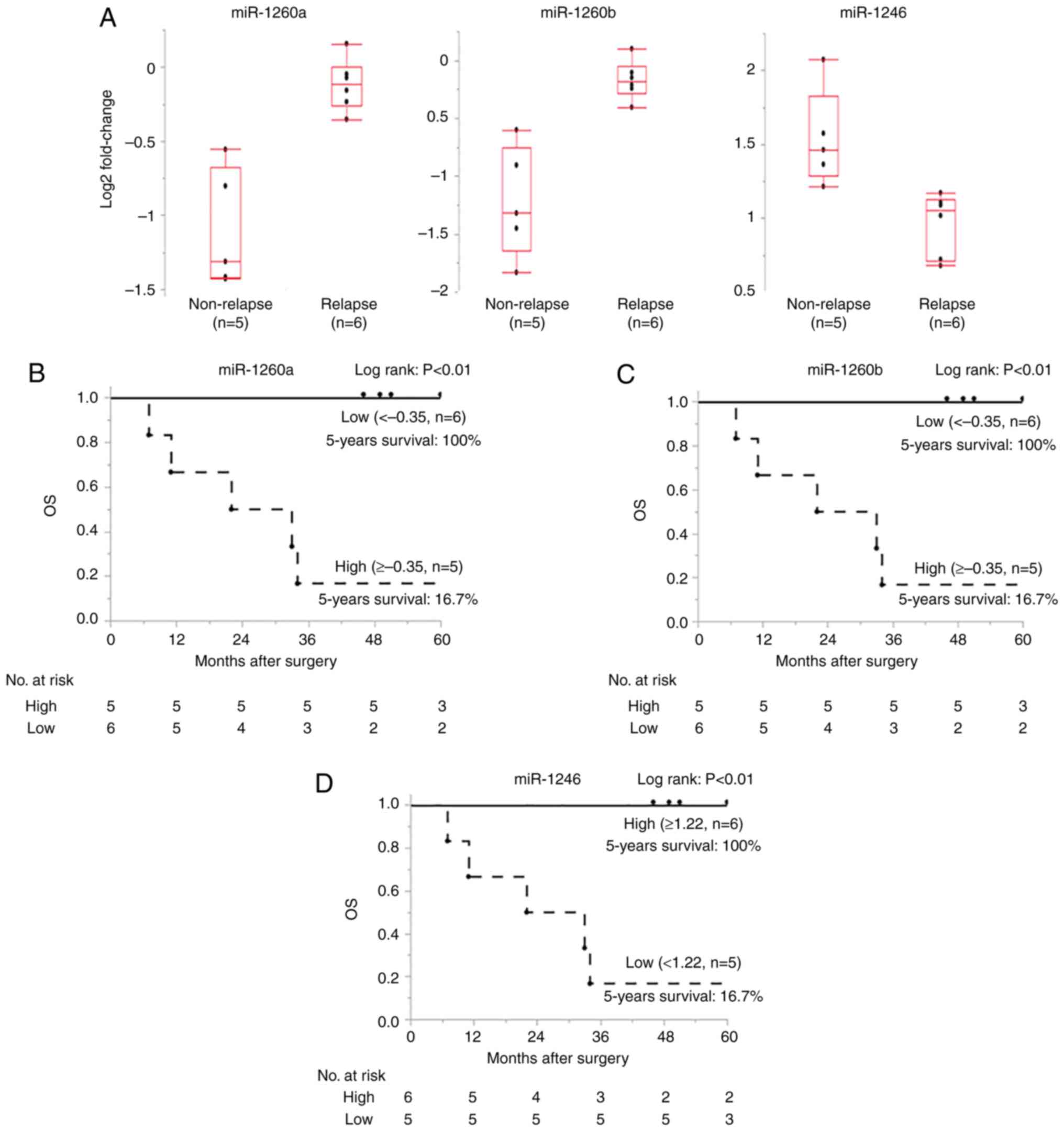
Survival analysis and prognosis
Based on a ROC curve analysis to differentiate
patients with relapse from those without, the cut-off value, the
largest AUC value, sensitivity and specificity for the expression
of the 12 miRNAs in Fig. 3A are
presented in Table III.
| Table III.Cut-off values for predicting relapse
analyzed using receiver operating characteristic curves. |
Table III.
Cut-off values for predicting relapse
analyzed using receiver operating characteristic curves.
| Name | Cut-off | AUC | Sensitivity | Specificity |
|---|
| miR-1246 | 1.172 | 1.00 | 1.00 | 1.00 |
| miR-1260a | −0.352 | 1.00 | 1.00 | 1.00 |
| miR-1260b | −0.404 | 1.00 | 1.00 | 1.00 |
| miR-1249-3p | −0.131 | 0.90 | 0.83 | 1.00 |
| miR-4284 | 0.338 | 0.90 | 0.83 | 1.00 |
| miR-612 | −0.310 | 0.93 | 0.83 | 1.00 |
| miR-296-5p | 0.076 | 0.90 | 1.00 | 0.80 |
| miR-575 | −0.530 | 0.93 | 1.00 | 0.80 |
| miR-6805-3p | 0.056 | 0.90 | 1.00 | 0.80 |
| miR-12136 | 0.304 | 0.90 | 0.67 | 1.00 |
| miR-6822-5p | −0.547 | 0.83 | 1.00 | 0.80 |
| miR-4454 | −0.622 | 0.87 | 1.00 | 0.80 |
The Box-and-Whisker plots for the top three miRNAs
(miR-1260a, miR-1260b and miR-1246) demonstrated that the plots of
the relapse and non-relapse groups were clearly separated near the
cutoff value (Fig. 4A) and thus the
miRNAs differentiated postoperative tumor relapse with both
sensitivity and specificity of 1. The overall survival rates of
patients with a high expression of miR-1260a and miR-1260b, as well
as a low expression of miR-1246, were significantly higher, with a
5-year survival rate of 100% (Fig.
4B-D; P<0.01).
Discussion
E-NEC is an aggressive disease with a lower survival
rate compared with squamous cell carcinomas (SCC) and
adenocarcinomas of the esophagus (6), with the role of surgery controversial
even in the resectable disease stage (20). Earlier researchers regarded E-NEC as
a systemic disease and recommended systemic treatments (6,20).
Whereas, recent meta-analysis of large population-based cohorts
suggested that radical esophagectomy is an effective primary
treatment for certain patients with limited disease stage E-NEC
(5,20). Several potential postoperative
favorable prognostic indicators are reported, such as absence of
lymph node metastasis (4), earlier
TNM stage (5,21) and adjuvant therapy (5,22,23).
In the present study, the postoperative outcome of
the 36 enrolled patients who underwent radical surgery for the
limited disease stage of E-NEC achieved a 5-year survival rate of
51.7%, almost the same postoperative prognosis as patients with
esophageal SCC in Japan (24),
suggesting that radical esophagectomy was effective in the present
cohort. The Kaplan-Meier curves of the overall survival stratified
by lymph node metastasis (N0 vs. N1) and TNM stage (stage I–II vs.
III–IV) showed a trend with prognosis; however, even patients with
stage III–IV disease and patients with positive lymph node
metastasis achieved 5-year survival rate of 38.5 and 40.5%
respectively, suggesting the existence of subgroups independent of
TNM staging and the need for novel indicators for patient response
to surgery based multidisciplinary treatment.
In the present study, postoperative prognosis was
improved compared with reports from other countries. For example,
the 5-year postoperative survival of 25 patients with localized
lymph node-negative (TanyN0M0) small cell NEC in the US population
has been reported as 50% (4),
whereas in the present study, for 10 patients with TanyN0M0, it was
80%. Similarly, another report involving 72 patients with limited
stage (TNM stage I–III) E-NEC in the Chinese population found a
postoperative 5-year survival rate of 28.4% (5), whereas the 33-patient cohort of the
present study showed a 5-year survival rate of 50.3%. One
explanation for this are differences in adjuvant therapies. In the
current study, 75.0% of all patients and 85.7% of the stage II–IV
patients received cisplatin-based adjuvant treatment, which was
higher compared with in previous reports in which only 48.6-66.0%
of the patients received adjuvant therapies (5,21).
Although the impact of adjuvant therapy in the present study was
not significant, possibly due to limited cases, it is suggested
that surgery should be performed as part of multidisciplinary
treatment with adjuvant therapies.
In the current study, as all patients received
surgery, the benefit of surgery compared with definitive chemo- or
chemoradiotherapy cannot be assessed. A Japanese report found a
5-year survival rate of 45.4% in chemoradiotherapy treatment for
patients with locally advanced (stage II–IV) E-NEC (25), indicating that if poor
postoperative-outcome subgroups are identified, then
chemoradiotherapy may be recommended as a primary treatment.
Therefore, as for other types of GI-NEC (26), novel postoperative prognostic
indicators are urgently needed to define a subgroup of limited
disease stage E-NEC patients who may benefit from surgery, to
individualize future treatment.
The current microarray analysis using the miRNA
oligo chip with 2,630 miRNAs identified 22 miRNAs that were
differentially expressed in tumors compared with their normal
counterparts. These miRNAs are well-known to be cancer related, and
six of these, miR-375-3p (27),
miR-17-5p (28), miR-182-5p
(29), miR-25-3p (30), miR-107 (31) and miR-191-5p (32), are involved with neuroendocrine
tumors. The present study suggests these miRNAs function in the
development of E-NEC and shows successful use of hospital archival
FFPE samples to detect differentially expressed miRNAs.
Based on these results, we focused on 12 miRNAs that
were differentially expressed between relapse and non-relapse
cases. Furthermore, the top three miRNAs, miR-1246, miR-1260a and
miR-1260b, completely differentiated patients who had postoperative
tumor relapse with both sensitivity and specificity of 1. Because
radical surgery is a local treatment, response to surgery based
multidisciplinary treatment is dependent on the presence of distant
micrometastases and sensitivity to chemotherapy. Therefore, it
possible that the aberrant expression of miR-1246, miR-1260a and
miR-1260b are linked to metastasis and chemosensitivity in E-NEC,
as reported in colorectal (33) and
breast (34,35) cancer.
As for biological pathways of these miRNAs, miR-1246
has been reported to play a suppressive role in the regulation of
the EMT by targeting dual-specificity
tyro-sine-(Y)-phosphorylation-regulated kinase 1A (DYRK1A) and
progranulin (PGRN) in a breast cancer cell line (36). DYRK1A is linked to a number of
cellular processes, including self-renewal, DNA damage, apoptosis,
and cancer stem cell maintenance (37). PGRN has been reported to promote
lymphangiogenesis and is an independent risk factor in esophageal
cancers (38). An oncogene nuclear
factor I/B, which is overexpressed in neuroendocrine carcinoma
(39,40), has also been identified as a direct
target of miR-1246 (41). An
onco-miR-1260b has been reported to regulate secreted
frizzled-related protein 1 and Smad4 (42), those were reported to upregulated in
neuroendocrine tumors (43,44).
In the present study, neither the expression of the
candidate target molecules, nor the interaction with the three
miRNAs were investigated, however, these reported findings
suggested possible roles of miR-1246, miR-1260a, and miR-1260b in
regulating malignant potential in E-NEC. Investigation of the
molecular mechanisms of these miRNAs may help us to further
understand the importance of them as biological markers, and aid in
developing novel therapeutic strategies, such as miRNA replacement
therapy based on the development of tumor suppressor miRNA delivery
systems (45). After accounting for
low-quality RNA samples, the small remaining number of cases
prevented validation group creation to fully assess the candidate
gene set in postoperative outcome prediction. In comparison with a
previous report, a microarray analysis using gene chips with 885
miRNAs in five cases of esophageal small cell NEC presented 39
miRNAs to predict postoperative tumor relapse (46). Despite the differences in the number
of genes carried on the chip, methods of RNA evaluation and
statistical analysis, miR-1260b was also included in the candidate
gene set. Nevertheless, larger multi-institutional studies are
required to validate the use of our miRNA gene set to predict
postoperative outcomes.
Recently, liquid biopsy entered use as a less
invasive sample collection for various types of cancer. Disrupted
levels of molecules listed in the present study, including miR-1246
(11), miR-1260a (47) and miR-1260b (48), are reported to be diagnostic and
prognostic biomarkers in peripheral blood for several cancer types,
suggesting the use of these molecules in liquid biopsy.
There are several limitations in the present study.
First, this was a retrospective observational study with limited
number of cases. Second, as perioperative chemotherapies with
different regimens have been administered in many cases, the
significance of surgery and chemotherapy in the treatment outcome
and the link to candidate microRNA function are yet to be
elucidated. Third, the sample size for the microarray analysis (11
cases) was too small to determine the use of the miRNAs as
predictive markers for recurrence. Fourth, validation of the
microarray results by RT-qPCR using the same RNA samples was not
performed due to either insufficient amount or denaturation of the
remaining RNA. Fifth, a validation cohort was not used due to the
exclusion of cases after RNA quality check. Therefore, further
validation studies based on larger multi-institutional prospective
studies, preferably dealing with frozen tissue samples or blood,
are needed to assess the use of our miRNA gene set to predict
treatment outcomes of the surgery based multidisciplinary
treatment.
In conclusion, the present results demonstrated that
radical esophagectomy was effective as part of multidisciplinary
treatment basically in combination with adjuvant therapies, for a
distinct subpopulation of limited stage E-NEC. The expression
levels of miRNAs such as miR-1246, miR-1260a and miR-1260b, in
tumors were strongly associated with this postoperative outcome,
suggesting possible involvement of these miRNAs in metastasis and
chemoresistance in E-NEC. Further investigation is needed to assess
possible use of this miRNA gene set as an indicator of surgery
based multidisciplinary treatment in patients with E-NEC.
Supplementary Material
Supporting Data
Supporting Data
Acknowledgements
Not applicable.
Funding
This work was supported by JSPS KAKENHI (grant nos. 18K08642 and
21K08729).
Availability of data and materials
The datasets generated and/or analyzed during the
current study are available in the GEO repository (accession no.
GSE221075; http://www.ncbi.nlm.nih.gov/geo/query/acc.cgi).
Authors' contributions
TO was involved in the conception and design,
experiments, data analysis, data interpretation and manuscript
writing. KTe was involved in the data analysis using machine
learning classifiers, data interpretation and manuscript writing.
TO and KTe confirm the authenticity of all the raw data. TKo, STak,
TKa, KTo, SH, TM, MY, STan, YaS, MF, YH, IH, YN and HY were
involved in case enrollment and sample collection. TF, SU, YuS,
HMat, SO, HMak and MI were involved in the conception and design,
supervised the conduct of this study. All authors critically
revised the report, commented on drafts of the manuscript, and have
read and approved the final manuscript.
Ethics approval and consent to
participate
The protocol of the present study was approved by
the ethics review board of University of Toyama Hospital (approval
no. R27-109). Then the study was approved by each institutional
review board of participating JNETS partner sites. Written informed
consent or opt-out consent was obtained from all participants.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Egashira A, Morita M, Kumagai R, Taguchi
KI, Ueda M, Yamaguchi S, Yamamoto M, Minami K, Ikeda Y and Toh Y:
Neuroendocrine carcinoma of the esophagus: Clinicopathological and
immunohistochemical features of 14 cases. PLoS One.
12:e01735012017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Dasari A, Mehta K, Byers LA, Sorbye H and
Yao JC: Comparative study of lung and extrapulmonary poorly
differentiated neuroendocrine carcinomas: A SEER database analysis
of 162 983 cases. Cancer. 124:807–815. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
WHO Classification of Tumours Editorial
Board, . WHO classification of tumours: Digestive system tumours.
5th edition. International Agency for Research on Cancer; Lyon:
2019
|
|
4
|
Wong AT, Shao M, Rineer J, Osborn V,
Schwartz D and Schreiber D: Treatment and survival outcomes of
small cell carcinoma of the esophagus: An analysis of the national
cancer data base. Dis Esophagus. 30:1–5. 2017.
|
|
5
|
Deng HY, Li G, Luo J, Li XR, Alai G and
Lin YD: The role of surgery in treating resectable limited disease
of esophageal neuroendocrine carcinoma. World J Surg. 42:2428–2436.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cai W, Ge W, Yuan Y, Ding K, Tan Y, Wu D
and Hu H: A 10-year population-based study of the differences
between NECs and carcinomas of the esophagus in terms of
clinicopathology and survival. J Cancer. 10:1520–1527. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
NCCN Clinical Practice Guidelines in
Oncology (NCCN Guidelines®), . Poorly differentiated neuroendocrine
carcinoma/large or small cell. Neuroendocrine and Adrenal Tumors.
NCCN. version 1. 2019
|
|
8
|
Ito T, Masui T, Komoto I, Doi R, Osamura
RY, Sakurai A, Ikeda M, Takano K, Igarashi H, Shimatsu A, et al:
JNETS clinical practice guidelines for gastroenteropancreatic
neuroendocrine neoplasms: diagnosis, treatment, and follow-up: A
synopsis. J Gastroenterol. 56:1033–1044. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Rupaimoole R and Slack FJ: MicroRNA
therapeutics: Towards a new era for the management of cancer and
other diseases. Nat Rev Drug Discov. 16:203–222. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Niwa Y, Yamada S, Sonohara F, Kurimoto K,
Hayashi M, Tashiro M, Iwata N, Kanda M, Tanaka C, Kobayashi D, et
al: Identification of a serum-based miRNA signature for response of
esophageal squamous cell carcinoma to neoadjuvant chemotherapy. J
Transl Med. 17:12019. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hoshino I, Ishige F, Iwatate Y, Gunji H,
Kuwayama N, Nabeya Y, Yokota H, Takeshita N, Iida K, Nagase H and
Matsubara H: Cell-free microRNA-1246 in different body fluids as a
diagnostic biomarker for esophageal squamous cell carcinoma. PLoS
One. 16:e02480162021. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yang H, Su H, Hu N, Wang C, Wang L, Giffen
C, Goldstein AM, Lee MP and Taylor PR: Integrated analysis of
genome-wide miRNAs and targeted gene expression in esophageal
squamous cell carcinoma (ESCC) and relation to prognosis. BMC
Cancer. 20:3882020. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Xi Y, Nakajima G, Gavin E, Morris CG, Kudo
K, Hayashi K and Ju J: Systematic analysis of microRNA expression
of RNA extracted from fresh frozen and formalin-fixed
paraffin-embedded samples. RNA. 13:1668–1674. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Osawa S, Shimada Y, Sekine S, Okumura T,
Nagata T, Fukuoka J and Tsukada K: MicroRNA profiling of gastric
cancer patients from formalin-fixed paraffin-embedded samples.
Oncol Lett. 2:613–619. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lloyd RV, Osamura RY, Klöppel G and Rosai
J: WHO classification of tumours of endocrine organs. Lloyd RV: WHO
classification of tumours. 4th edition. 10. Lyon: International
Agency for Research on Cancer; 2017
|
|
16
|
Sobin LH, Gospodarowicz M and Wittekind C:
TNM Classification of Malignant Tumours. 7th edition. UICC
International Union Against Cancer Hoboken, NJ: Wiley-Blackwell;
2010, PubMed/NCBI
|
|
17
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Breiman L: Random forests. Mach Learn.
45:5–32. 2001. View Article : Google Scholar
|
|
19
|
Altmann A, Toloşi L, Sander O and Lengauer
T: Permutation importance: A corrected feature importance measure.
Bioinformatics. 26:1340–1347. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Jatoi A and Miller RC: Should we recommend
surgery to patients with limited small cell carcinoma of the
esophagus? J Thorac Oncol. 3:1373–1376. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Xu L, Li Y, Liu X, Sun H, Zhang R, Zhang
J, Zheng Y, Wang Z, Liu S and Chen X: Treatment strategies and
prognostic factors of limited-stage primary small cell carcinoma of
the esophagus. J Thorac Oncol. 12:1834–1844. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhang G, Wu B, Wang X and Li J: A
competing-risks nomogram and recursive partitioning analysis for
cause-specific mortality in patients with esophageal neuroendocrine
carcinoma. Dis Esophagus. 32:doy1292019. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zou B, Li T, Zhou Q, Ma D, Chen Y, Huang
M, Peng F, Xu Y, Zhu J, Ding Z, et al: Adjuvant therapeutic
modalities in primary small cell carcinoma of esophagus patients: A
retrospective cohort study of multicenter clinical outcomes.
Medicine (Baltimore). 95:e35072016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Watanabe M, Otake R, Kozuki R, Toihata T,
Takahashi K, Okamura A and Imamura Y: Recent progress in
multidisciplinary treatment for patients with esophageal cancer.
Surg Today. 50:12–20. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Honma Y, Nagashima K, Hirano H, Shoji H,
Iwasa S, Takashima A, Okita N, Kato K, Boku N, Murakami N, et al:
Clinical outcomes of locally advanced esophageal neuroendocrine
carcinoma treated with chemoradiotherapy. Cancer Med. 9:595–604.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sorbye H, Welin S, Langer SW, Vestermark
LW, Holt N, Osterlund P, Dueland S, Hofsli E, Guren MG, Ohrling K,
et al: Predictive and prognostic factors for treatment and survival
in 305 patients with advanced gastrointestinal neuroendocrine
carcinoma (WHO G3): The NORDIC NEC study. Ann Oncol. 24:152–160.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Abraham KJ, Zhang X, Vidal R, Paré GC,
Feilotter HE and Tron VA: Roles for miR-375 in neuroendocrine
differentiation and tumor suppression via notch pathway suppression
in merkel cell carcinoma. Am J Pathol. 186:1025–1035. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
García-Martínez A, López-Muñoz B, Fajardo
C, Cámara R, Lamas C, Silva-Ortega S, Aranda I and Picó A:
Increased E2F1 mRNA and miR-17-5p expression is correlated to
invasiveness and proliferation of pituitary neuroendocrine tumours.
Diagnostics (Basel). 10:2272020. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Calsina B, Castro-Vega LJ, Torres-Pérez R,
Inglada-Pérez L, Currás-Freixes M, Roldán-Romero JM, Mancikova V,
Letón R, Remacha L, Santos M, et al: Integrative multi-omics
analysis identifies a prognostic miRNA signature and a targetable
miR-21-3p/TSC2/mTOR axis in metastatic
pheochromocytoma/paraganglioma. Theranostics. 9:4946–4958. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Zeng Z, Li Y, Pan Y, Lan X, Song F, Sun J,
Zhou K, Liu X, Ren X, Wang F, et al: Cancer-derived exosomal
miR-25-3p promotes pre-metastatic niche formation by inducing
vascular permeability and angiogenesis. Nat Commun. 9:53952018.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Trivellin G, Butz H, Delhove J, Igreja S,
Chahal HS, Zivkovic V, McKay T, Patócs A, Grossman AB and Korbonits
M: MicroRNA miR-107 is overexpressed in pituitary adenomas and
inhibits the expression of aryl hydrocarbon receptor-interacting
protein in vitro. Am J Physiol Endocrinol Metab. 303:E708–E719.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Di W, Amdanee N, Zhang W and Zhou Y:
Long-term exercise-secreted extracellular vesicles promote browning
of white adipocytes by suppressing miR-191a-5p. Life Sci.
263:1184642020. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Peng W, Li J, Chen R, Gu Q, Yang P, Qian
W, Ji D, Wang Q, Zhang Z, Tang J and Sun Y: Upregulated METTL3
promotes metastasis of colorectal cancer via miR-1246/SPRED2/MAPK
signaling pathway. Exp Clin Cancer Res. 38:3932019. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Sugita BM, Pereira SR, de Almeida RC, Gill
M, Mahajan A, Duttargi A, Kirolikar S, Fadda P, de Lima RS, Urban
CA, et al: Integrated copy number and miRNA expression analysis in
triple negative breast cancer of Latin American patients.
Oncotarget. 10:6184–6203. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Park S, Kim J, Cho Y, Ahn S, Kim G, Hwang
D, Chang Y, Ha S, Choi Y, Lee MH, et al: Promotion of tumorigenesis
by miR-1260b-targeting CASP8: Potential diagnostic and prognostic
marker for breast cancer. Cancer Sci. 113:2097–2108. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Wang P, Chen W, Zhang Y, Zhong Q, Li Z and
Wang Y: MicroRNA-1246 suppresses the metastasis of breast cancer
cells by targeting the DYRK1A/PGRN axis to prevent the
epithelial-mesenchymal transition. Mol Biol Rep. 49:2711–2721.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Rammohan M, Harris E, Bhansali RS, Zhao E,
Li LS and Crispino JD: The chromosome 21 kinase DYRK1A: Emerging
roles in cancer biology and potential as a therapeutic target.
Oncogene. 41:2003–2011. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Li G, Dong T, Yang D, Gao A, Luo J, Yang H
and Wang L: Progranulin promotes lymphangiogenesis through VEGF-C
and is an independent risk factor in human esophageal cancers. Hum
Pathol. 75:116–124. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Wu N, Jia D, Ibrahim AH, Bachurski CJ,
Gronostajski RM and MacPherson D: NFIB overexpression cooperates
with Rb/p53 deletion to promote small cell lung cancer. Oncotarget.
7:57514–57524. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Andreasen S, Persson M, Kiss K, Homøe P,
Heegaard S and Stenman G: Genomic profiling of a combined large
cell neuroendocrine carcinoma of the submandibular gland. Oncol
Rep. 35:2177–2182. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Zhang Q, Cao LY, Cheng SJ, Zhang AM, Jin
XS and Li Y: p53-induced microRNA-1246 inhibits the cell growth of
human hepatocellular carcinoma cells by targeting NFIB. Oncol Rep.
33:1335–1341. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Hirata H, Hinoda Y, Shahryari V, Deng G,
Tanaka Y, Tabatabai ZL and Dahiya R: Correction: Genistein
downregulates onco-miR-1260b and upregulates sFRP1 and Smad4 via
demethylation and histone modification in prostate cancer cells. Br
J Cancer. 119:3882018. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Kim JT, Li J, Jang ER, Gulhati P, Rychahou
PG, Napier DL, Wang C, Weiss HL, Lee EY, Anthony L, et al:
Deregulation of Wnt/β-catenin signaling through genetic or
epigenetic alterations in human neuroendocrine tumors.
Carcinogenesis. 34:953–961. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Kim H, An S, Lee K, Ahn S, Park DY, Kim
JH, Kang DW, Kim MJ, Chang MS, Jung ES, et al: Pancreatic
high-grade neuroendocrine neoplasms in the Korean population: A
multicenter study. Cancer Res Treat. 52:263–276. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Zhou X, You M, Wang F, Wang Z, Gao X, Jing
C, Liu J, Guo M, Li J, Luo A, et al: Multifunctional
graphdiyne-cerium oxide nanozymes facilitate MicroRNA delivery and
attenuate tumor hypoxia for highly efficient radiotherapy of
esophageal cancer. Adv Mater. 33:e21005562021. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Okumura T, Shimada Y, Omura T, Hirano K,
Nagata T and Tsukada K: MicroRNA profiles to predict postoperative
prognosis in patients with small cell carcinoma of the esophagus.
Anticancer Res. 35:719–727. 2015.PubMed/NCBI
|
|
47
|
Latchana N, DiVincenzo MJ, Regan K, Abrams
Z, Zhang X, Jacob NK, Gru AA, Fadda P, Markowitz J, Howard JH and
Carson WE III: Alterations in patient plasma microRNA expression
profiles following resection of metastatic melanoma. J Surg Oncol.
118:501–509. 2018.PubMed/NCBI
|
|
48
|
Yao Y, Ding Y, Bai Y, Zhou Q, Lee H, Li X
and Teng L: Identification of serum circulating MicroRNAs as novel
diagnostic biomarkers of gastric cancer. Front Genet.
11:5915152021. View Article : Google Scholar : PubMed/NCBI
|