Introduction
Primary central nervous system lymphoma (PCNSL) is
an extranodal non-Hodgkin lymphoma that primarily affects the brain
parenchyma, eyes, cranial nerve and meninges. It is an extremely
rare occurrence, accounting for <3% of intracranial tumors in
the US (1,2). PCNSL is primarily composed of diffuse
large B-cell lymphomas of the activated B-cell subtype (3,4), with
a small percentage of these lymphomas being marginal zone B-cell
lymphoma (MZBL). MZBL also includes extranodal MZL of
mucosa-associated lymphoid tissue (MALT) lymphoma, nodal MZL and
splenic MZL (5). MALT lymphoma was
initially thought to arise from gastrointestinal lymphoma, which is
the most common site; however, it can also occur in other sites,
such as the lungs, head and neck, skin, thyroid and breast
(5,6). Meningioma, a common tumor of the
central nervous system, is easy to diagnose because of its unique
imaging features, such as the dural tail sign (7). MALT lymphoma involving meningeal
tissue is uncommon and can be easily confused with meningiomas
clinically. In the present report, the patient had similar imaging
manifestations with meningioma, but was finally diagnosed with MALT
lymphoma based on pathologic findings (Fig. 1). MALT lymphoma is rare in clinical
practice, therefore, the mechanism and treatments were
investigated.
Case report
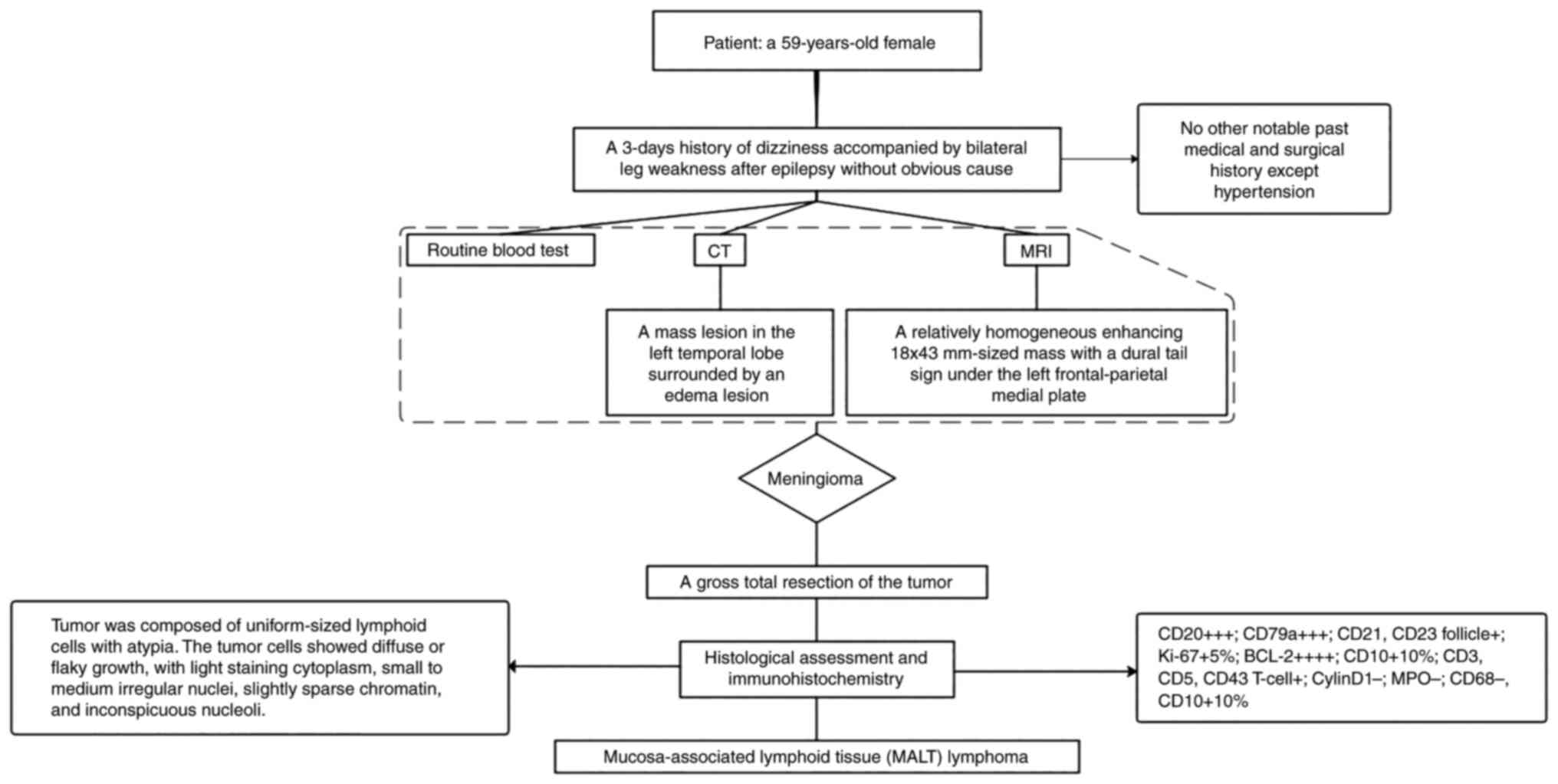
A 59-year-old female with a history of hypertension,
but no other significant medical and surgical history, presented to
The Affiliated Huai'an No. 1 People's Hospital of Nanjing Medical
University (Huai'an, China) with a 3-day history of dizziness
accompanied by bilateral leg weakness after an epileptic seizure
with no apparent cause in November 2015. No abnormalities were
found after neurological examination or routine laboratory tests.
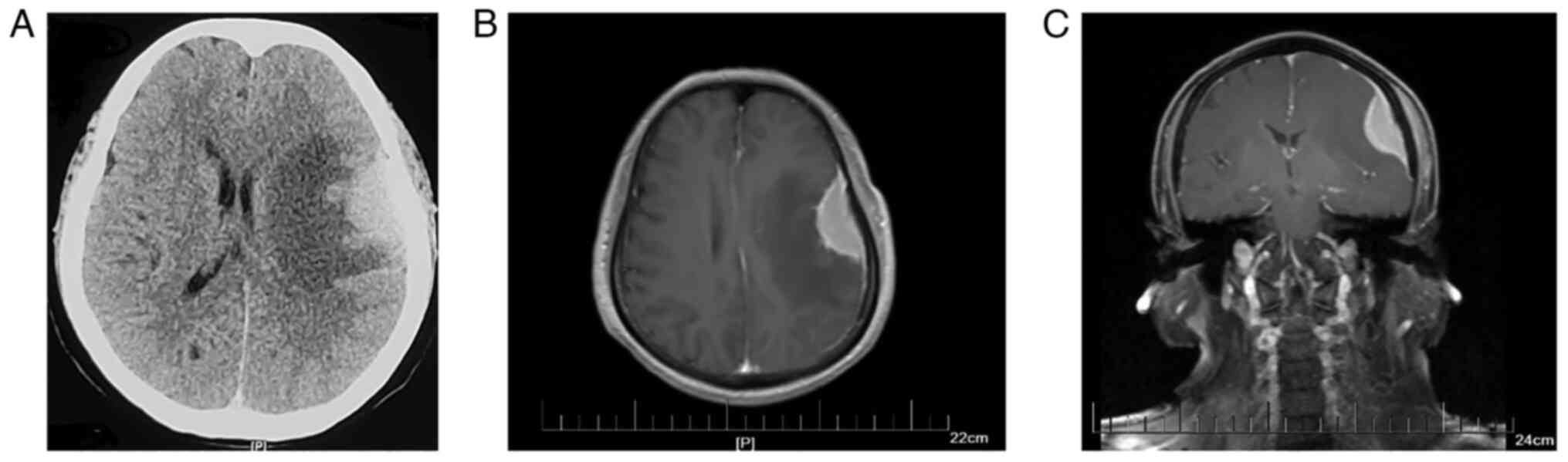
Cranial computerized tomography (CT) revealed a mass lesion in the
left temporal lobe surrounded by an edema lesion (Fig. 2A). Enhanced magnetic resonance
imaging (MRI) showed a relatively homogeneous enhancing mass
measuring 18×43 mm with a dural tail sign under the left
frontal-parietal medial plate, which is a typical imaging
manifestation of meningioma (Fig. 2B
and C). Based on this information, a diagnosis of meningioma
was made on November 11, 2015. The patient subsequently underwent a
gross total resection of the tumor. Intraoperatively, a dark
red-white 4×5×3 cm-sized tumor based on the dura mater was
observed, along with invasion and adhesion of adjacent brain
tissue.
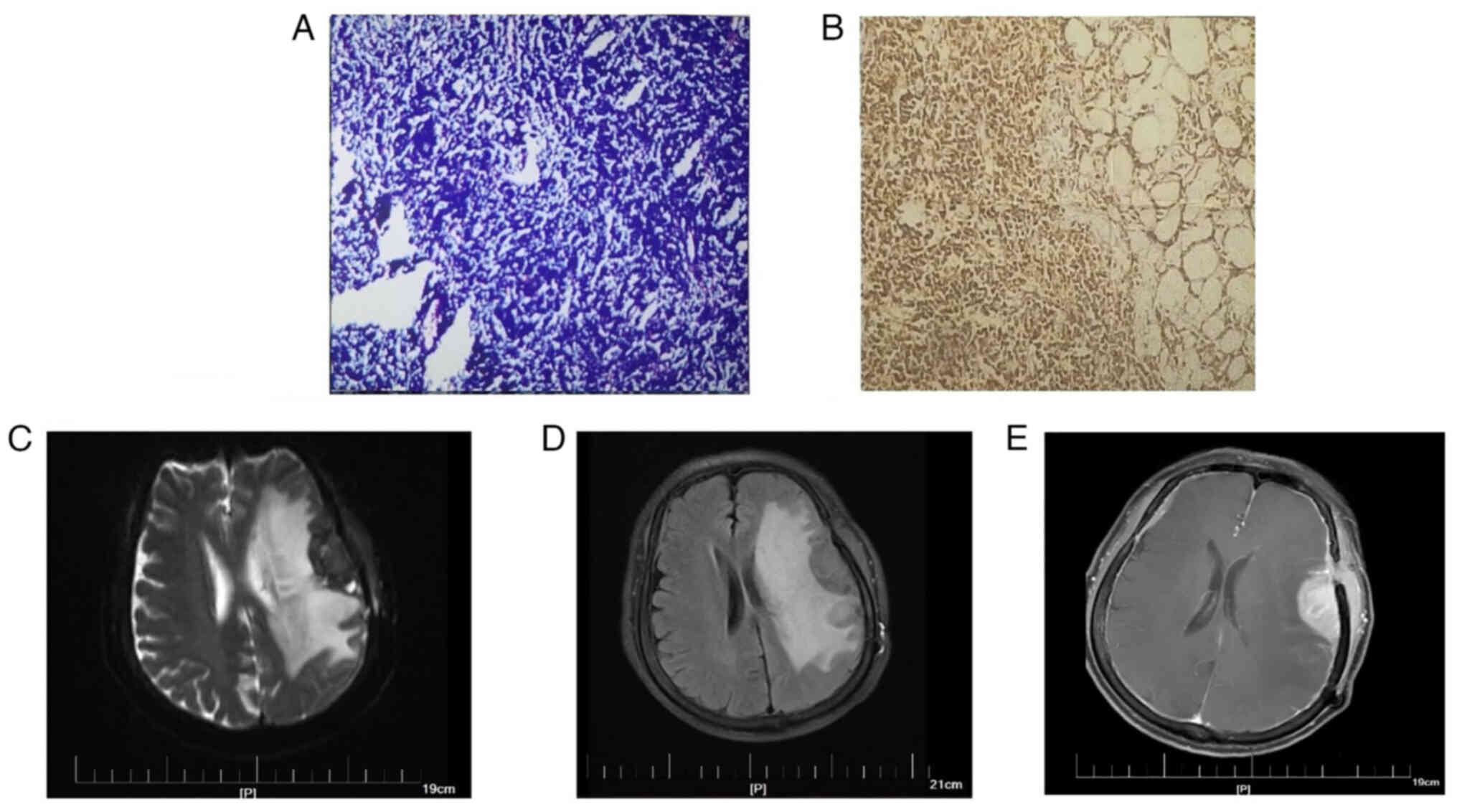
For H&E staining, surgical specimens were fixed
in 10% neutral formalin at room temperature for 24–48 h, and
paraffin-embedded sections were produced (4 µm), stained with
H&E at room temperature for 5 min and analyzed under a light
microscope. Histological assessment of the tumor revealed a diffuse
infiltration containing uniformly sized lymphocytes with atypia
(Fig. 3A), consistent with a
lymphoma diagnosis, as opposed to a meningioma diagnosis.
Generally, most meningiomas are benign, and atypia is rare. The
meningothelial meningioma, the most common subtype, is composed of
polygonal, ill-defined, arachnoid epithelial cells variable in
size, with abundant cytoplasm and large nuclei. The characteristic
structure of meningiomas is the arrangement of cells in concentric
circles of different sizes, with small blood vessels; the vessel
walls can exhibit hyalinization, calcification or psammoma
bodies.
Subsequently, H&E staining and
immunohistochemistry was performed on the patient's tumor tissues.
The primary antibodies used included anti-CD2, anti-CD3, anti-CD5,
anti-CD10, anti-CD20, anti-CD21, anti-CD23, anti-CD43, anti-CD68,
anti-CD79a, anti-Bcl-2, anti-Bcl-6, anti-MPO, anti-Cyclin D1 and
anti-Ki-67 Immunohistochemical findings were as follows:
CD20+++; CD79a+++; CD21+, CD23
follicle+; Ki-67+ 5%; BCL-2++++;
CD10+10%; CD3+, CD5+, CD43
T-cell+; Cyclin D1−; MPO−;
CD68−; and CD10+10% (Fig. 3B shows representative staining for
CD20). The characteristics of small B-cell malignant lymphoma were
consistent with extranodal MZBL of the MALT type.
Based on the immunohistochemical findings and
histological assessment, it was recommended the patient receive
chemotherapy or radiation therapy; however, the patients' economic
situation led to her decision to be discharged from hospital.
Patient follow-up after discharge from hospital continued via
telephone and the internet (messaging) for 2 years, during which
time the patient experienced no discomfort such as dizziness,
headache and weakness. After this 2-year period, the patient began
experiencing these symptoms; however, no abnormalities were found
upon examination. Unfortunately, a cranial enhancing CT performed
in November 2021 revealed a mass lesion in the left temporal lobe,
along with left frontotemporal lobe and basal ganglia edema, which
could not rule out postoperative recurrence; however, the patient
opted out of treatment. The patient developed slurred speech
accompanied by intermittent nausea, vomiting, headache and
dizziness after 2 months, prompting her to re-evaluate treatment.
Given the possibility of lymphoma recurrence, an MRI in January
2022 was performed and subsequently revealed abnormal enhancement
of the left frontotemporal lobe along with surrounding edema and
multiple enhancements of the intracranial meninges (Fig. 3C-E). Furthermore, a PET-CT scan
showed multiple metastases throughout the patient's body. The
patient was transferred to the oncology department for antitumor
therapy after discharge.
Discussion
Primary central nervous system lymphomas are
predominantly aggressive diffuse high-grade B-cell lymphomas of the
large B-cell type. MALT lymphomas arise from B-cells in the MALT
marginal area and are also known as extranodal marginal area B-cell
lymphoma. The majority of MALT lymphomas occur in middle-aged
women, and symptoms include epilepsy, headache and visual
disturbance (8). The cytologic
composition can vary, including small lymphocytic, plasmacytoid and
marginal zone type cells; these may have reactive follicles,
numerous transformed lymphocytes, plasma cells and other
inflammatory cells (9).
Currently, there are a few widely accepted
mechanisms for the formation of MALT lymphomas. In embryology,
meningothelial cells are concentrated in the arachnoid membrane and
dural venous sinuses, similar to epithelial cells in other sites
where MALT lymphoma develops (4,10) In
addition, dural-based MALT may be caused by the implantation
metastasis of undiagnosed or disappearing MALT lymphoma at the
meninges (11). Furthermore, the
role of chronic inflammatory disease, including hepatitis C
(12) and Helicobacter
pylori-associated gastritis cannot be ruled out (8,9,12,13).
Additionally, autoimmune diseases have been reported to be
associated with MALT lymphoma, such as Grave's disease (14), Sjögren syndrome (8,14),
scleroderma (14) and Hashimoto
thyroiditis (9,13). Furthermore, IgG4 expression has been
linked to primary intracranial MZBLs (15,16);
Venkataraman et al (15)
demonstrated this association through a series of retrospective
analyses. A number of cases from the literature have been collated
to further understand the characteristics of MALT lymphomas
(Table I). Historically, the
majority of cases occur in middle-aged women who primarily present
with headaches and seizures, yet other manifestations can include
hearing impairment, numbness, visual impairment and dysphasia,
depending on the location of the tumor.
 | Table I.Summary of patient characteristics
with intracranial extranodal marginal zone B-cell lymphomas. |
Table I.
Summary of patient characteristics
with intracranial extranodal marginal zone B-cell lymphomas.
| First author/s,
year | Case | Age | Sex | Location | Symptoms | Treatment |
Remission/outcome |
Immunohistochemistry | (Refs.) |
|---|
| Rottnek et al,
2004 | 1 | 47 | M | Left tentorial | Seizure, visual field
defects and memory loss | Subtotal excision and
radiation | NED at 8 months | CD20+,
CD79a+, CD43+ and kappa LCR | (9) |
| Kambham et al,
1998 | 2 | 39 | F | Left CP angle
(dura) | Hearing loss and
facial pain/weakness | Subtotal
excision | AWD after 4
years | CD20+,
CD79a+, CD21+ germinal centers and kappa
LCR | (17) |
|
| 3 | 62 | F | Left
parietal-occipital area | Headaches | Radiation | AWD after 6
months | CD20+ and
CD79a+ |
|
| Kumar et al,
1997 | 4 | 40 | F | Right cavernous
sinus | Numbness and visual
field defects | Radiation | NED at 63 months | CD20+,
CD3+ reactive T cells and lambda LCR | (10) |
|
| 5 | 62 | F | Biparietal dural | Seizures | Fludarabine | NED at 22 months | CD20+,
CD3+ reactive T cells and lambda LCR |
|
|
| 6 | 52 | F | Left frontal
dural | Seizures and
numbness |
Radiation/chemotherapy | NED at 9
months | CD20+,
CD3+ reactive T cells and kappa LCR |
|
|
| 7 | 43 | F | Left tentorial | Dizziness,
headaches, blurred vision and numbness | Radiation | NED at 7
months | CD20+,
CD3+ reactive T cells, CD43+ and lambda
LCR |
|
|
| 8 | 57 | F | Left anterior falx
cerebri | Seizures | Radiation | NED at 14
months | CD20+,
CD3+ reactive T cells, CD43+ and
CD23− |
|
| Itoh et al,
2001 | 9 | 28 | F | CP angle | Tinnitus, nausea,
headache and bilateral papilledema | Excision | NED at 2 years | CD20+,
CD10+ (follicular center cells), BCL2+ in
some follicular centers, CD43+ and CD3+ (50%
cells) | (18) |
| Goetz et al,
2002 | 10 | 64 | F | Right
frontoparietal dura | Left hemiparesis
and headache | Excision and
radiation | NED at 3
months |
IgD+/CD20+ small
lymphocytes, IgD−/CD20+ lymphoplasmacytoid
cells, CD20−/CD138+ plasma cells and kappa
LCR | (13) |
| Ferguson et
al, 2010 | 11 | 29 | F | Right frontal
dural | Exophthalmos and
visual loss | Decompression of
the optic nerve, subtotal resection and 30 Gy radiation | NED at 3 years | CD20+,
BCL-6−, kappa LCR and CD5− | (14) |
| Jesionek-Kupnicka
et al, 2013 | 12 | 60 | F | Left
parietooccipital dural | Headache, periodic
cramp of the right face and numbness of the | Excision and
radiotherapy (WS3D 6MV photons) | NED | CD20+,
CD79a+, BCL-2+ (reactive follicles with
germinal centers), CD3−, CD5−,
CD23−, CD10−, BCL-6−, Cyclin
D1−, Ki-67+ (10%), | (4) |
| Kamoshima et
al, 2011 | 13 | 55 | F | Left frontal
dural | Seizures | Subtotal excision
and 40 Gy radiation | NED at 36
months | CD20+,
CD5−, CD23−, CD10−, Cyclin
D1−, CD3+ (some lymphocytes) | (8) |
| Shaia et al,
2010 | 14 | 61 | F | Dura of the right
posterior fossa | Nausea, vomiting
and pain over the top of scalp | Excision and 30 Gy
radiation | NED at 6
months | CD20+,
CD79a+, CD5−, CD10−,
CD23−, CD43− and kappa LCR | (19) |
| Tu et al,
2005 | 15 | 49 | M | Frontal | Seizures | Chemotherapy (MTX
and fludarabine) | NED at 7.6
years | Not available | (20) |
|
| 16 | 48 | F | Dura, tentorium and
falx | Headache and ear
pain | Chemotherapy (MTX
and leucovorin) and radiation | NED at 20
months | Not available |
|
| Lehman et
al, 2002 | 17 | 63 | F | Supratentorial and
infratentorial dural | Seizure | Excision and 36 Gy
radiation | NED | CD20+,
CD45+, CD3+ (small population) and
CD138+ (small population) | (21) |
| Venkataraman et
al, 2011 | 18 | 62 | F | Bilateral
parietal | Unknown | Fludarabine | NED at 22
months | Not available | (15) |
| Villeneuve et
al, 2018 | 19 | 60 | F | Petrous temporal
bone | Vertigo and
unilateral right mixed hearing loss | Chemotherapy
(rituximab and bendamustine) | NED at 2years | CD20+,
CD23+, CD5−, CD10−,
BCL-1− and BCL-2+ | (22) |
| Park et al,
2008 | 20 | 18 | M | Left basal
ganglia | Right-sided central
facial nerve palsy, right-sided weakness, dizziness and
dysarthria | Radiation | NED at 22
months | CD20+,
CD79a+, CD3−, CD5−,
CD10−, BCL-6−, CD23−, MUM1-,
ALK-1−, Cyclin D1−, and negative for kappa
and lambda LCR | (12) |
| Kelley et
al, 2005 | 21 | 53 | M | Right lateral
ventricle | Headache and
seizure | Excision and
chemotherapy (liposomal cytarabine) | NED at 14
months | CD19+,
CD20+, CD45+, CD5−,
CD10− | (23) |
| Jazy et al,
1980 | 22 | 59 | M | Right temporal | Seizures, visual
and hearing impairment | Radiation | NED at 16
months | Not available | (24) |
| Miranda et
al, 1996 | 24 | 51 | F | Right frontal | Major motor
seizure | Excision and
radiation | NED at 14
months | CD19+,
CD20+ and CD22+ | (25) |
| Naberhaus et
al, 1996 | 25 | 48 | F | Right
temporo-parietal | Headaches | Radiation | NED at 36
months |
CD20+ | (26) |
| King et al,
1998 | 26 | 60 | F | Cerebellar vermis
and right fronto-parietooccipital | Seizures and memory
loss | Biopsy and
chemotherapy | Died 3 months later
due to pneumonia | CD45RB+,
CD20+, Cyclin D1 | (27) |
| Hodgson et
al, 1999 | 27 | 57 | F | Right sphenoid
wing | Headache and
mild | Excision
photophobia | NED at 6
months | CD20+,
kappa LCR, BCL-2+ | (28) |
| Freudenstein et
al, 2000 | 28 | 50 | F | Parafalcine and
bilateral convexity dura | Headache and
seizures | Systemic and
intrathecal chemotherapy (MTX) | NED at 36
months | CD20+,
LCA+, Vimentin+, CD3−, IgG light
chain− and IgG heavy chain− | (29) |
| Neidert et
al, 2015 | 29 | 44 | M | Right
fronto-parietal dural | Involuntary muscle
movements on the left-side of his body | Excision and 36 Gy
radiation | NED at 2 years | CD20+,
CD45+, BCL-2+, CD79a+,
EMA−, CD34−, TDT−,
CD99−, Ki-67+ (30%), CD3+,
CD5+, CD10+, CD23+ (small
population) | (30) |
| Pavlou et
al, 2006 | 30 | 73 | F | Left
fronto-parietal | Right arm weakness,
partial seizures and dysphasia | Excision and
chemotherapy (methylpred-nisolone, cytosine and methotrexate,
chlorambucil) | Unknown | CD20+,
CD79+, BCL-2+, CD10−,
BCL-1−, CD5−, MIB-1+ (10%) | (31) |
| Present study | 31 | 59 | F | Left temporal
lobe | Dizziness and
bilateral leg weakness | Excision | AWD after 6
years | CD20+;
CD79a+, CD21+, CD23 follicle+;
Ki-67+ 5%; BCL-2+; CD10+ 10%;
CD3+, CD5+ CD43 T-cell+, Cyclin
D1−, MPO− and CD68- |
|
Clinically, the differential diagnosis of lymphoma
is important; however, due to the dural tail sign, it can be
difficult to distinguish it from meningioma based solely on imaging
and clinical manifestations. Small lymphocytic lymphoma, chronic
lymphocytic leukemia (CLL), lymphoplasmacytic lymphoma (LPL) are
other potential diagnoses that require further histological and
immunophenotypic analysis for confirmation. Notably, MALT lymphomas
express CD20, CD79a and CD38, which can also be seen in LPL
(Table II). In addition, CLL
expresses CD5 and CD23. In the present case, a 59-year-old woman
presented with dizziness and bilateral leg weakness.
Immunophenotypically, the patients' lymphoid cells were positive
for CD20, CD79a, CD21, CD23, BCL-2, CD3, CD5 and CD43, but were
negative for Cylin D1, MPO and CD68. Although the
immunohistochemical findings were similar to follicular lymphomas,
the cells of follicular lymphoma grew nodular and formed obvious
follicular structures at low magnification, which were not observed
in the pathological findings of this tumor. Although the specific
type of lymphoma cannot be confirmed, MALT lymphoma is more likely
based on clinical symptoms, imaging and immunohistochemistry.
However, it is unfortunate that genetic analysis of the lesion was
not performed to verify and validate the diagnosis and treatments.
Additional detection of MYD88, IgM and BRAF would aid in
differentiating between LPL/Waldenstrom's macroglobulinemia,
hairy-cell leukemia and MALT, increasing the accuracy of
diagnosis.
| Table II.Immunohistochemistry of different
types of lymphomaa. |
Table II.
Immunohistochemistry of different
types of lymphomaa.
| Types of
lymphoma |
Immunohistochemistry |
|---|
| MALT lymphoma
(extranodal | CD20+,
CD79a+ and |
| marginal zone
lymphoma) |
CD38+ |
| Lymphoplasmacytic
lymphoma/ | CD20+,
CD79a+ and |
| Waldenstrom
macroglobulinemia |
CD38+/IgM+ |
| Follicular
lymphoma | CD10+
and BCL-2+ |
| Chronic lymphocytic
leukemia | CD5+ and
CD23+ |
| Mantle cell
lymphoma | CD5+,
Cyclin D1−, |
|
| CD10−
and CD23− |
| Lymphoblastic
lymphoma |
TDT+ |
| Lymphomatoid
granulomatosis | EBER in
situ+ |
In conclusion, MALT lymphomas are often confused
with meningioma owing to similarities in imaging and clinical
manifestations; thus, clinicians should not jump to conclusions
when presented with images that resemble meningiomas, especially
containing the dural tail sign. MALT lymphomas are generally
indolent, localized lesions that can be cured through surgical
resection and radiotherapy. Current evidence suggests that
radiotherapy is the most commonly used treatment, and the extent of
the dural lesions and leptomeningeal involvement determine the
radiation field. As molecular genetic changes are tightly
associated with classification, prognosis and treatment of tumors,
additional detection of mutated genes is recommended, so as to more
effectively treat diseases.
Acknowledgements
Not applicable.
Funding
The study was supported by the Key Science and Technology
Project of Jiangsu Commission of Health (grant. no. ZD2021051).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JBR, LYC, SXL and JHR confirm the authenticity of
all the raw data. Study conception and design was performed by LSD
and JBR. Material preparation and data collection were taken by
LYC. Analysis and interpretation of data was performed by SXL.
Follow-up of the patients was performed by JHR. All authors
contributed to manuscript writing. All authors read and approved
the final version of the manuscript.
Ethics approval and consent to
participate
The report has obtained approval from the Ethics
Committee and Institutional Review Board of Huai'an First People's
Hospital (Huai'an, China; approval number: KY-2023-035-01).
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of the case details and any associated
images.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
CLL
|
chronic lymphocytic leukemia
|
|
CT
|
computerized tomography
|
|
LPL
|
lymphoplasmacytic lymphoma
|
|
MALT
|
mucosa-associated lymphoid tissue
|
|
MPO
|
myeloperoxidase
|
|
MRI
|
magnetic resonance imaging
|
|
MZBL
|
marginal zone B-cell lymphoma
|
|
PCNSL
|
primary central nervous system
lymphoma
|
|
PET-CT
|
positron emission tomography
computerized tomography
|
References
|
1
|
Nayak L, Pentsova E and Batchelor TT:
Primary CNS lymphoma and neurologic complications of hematologic
malignancies. Continuum (Minneap Minn). 21:355–372. 2015.PubMed/NCBI
|
|
2
|
Ostrom QT, Gittleman H, Fulop J, Liu M,
Blanda R, Kromer C, Wolinsky Y, Kruchko C and Barnholtz-Sloan JS:
CBTRUS statistical report: Primary brain and central nervous system
tumors diagnosed in the united states in 2008–2012. Neuro Oncol. 17
(Suppl 4):iv1–iv62. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Holdhoff M, Mrugala MM, Grommes C, Kaley
TJ, Swinnen LJ, Perez-Heydrich C and Nayak L: Challenges in the
treatment of newly diagnosed and recurrent primary central nervous
system lymphoma. J Natl Compr Canc Netw. 18:1571–1578. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Jesionek-Kupnicka D, Smolewski P, Kupnicki
P, Pluciennik E, Zawlik I, Papierz W and Kordek R: Primary
extranodal marginal zone B-cell lymphoma of the mucosa-associated
lymphoid tissue type in the central nervous system (MZL CNS)
presented as traumatic subdural hematoma and subarachnoid
bleeding-case report. Clin Neuropathol. 32:384–392. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Olszewski AJ and Castillo JJ: Survival of
patients with marginal zone lymphoma: Analysis of the surveillance,
epidemiology, and end results database. Cancer. 119:629–638. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Weis S and Llenos IC: Primary
leptomeningeal B-cell lymphoma of MALT-type in statu nascendi: A
case report and review of the literature. Clin Neurol Neurosurg.
110:732–738. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Goldbrunner R, Stavrinou P, Jenkinson MD,
Sahm F, Mawrin C, Weber DC, Preusser M, Minniti G, Lund-Johansen M,
Lefranc F, et al: EANO guideline on the diagnosis and management of
meningiomas. Neuro Oncol. 23:1821–1834. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kamoshima Y, Sawamura Y, Sugiyama T,
Yamaguchi S, Houkin K and Kubota K: Primary central nervous system
mucosa-associated lymphoid tissue lymphoma-case report. Neurol Med
Chir (Tokyo). 51:527–530. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Rottnek M, Strauchen J, Moore F and
Morgello S: Primary dural mucosa-associated lymphoid tissue-type
lymphoma: Case report and review of the literature. J Neurooncol.
68:19–23. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kumar S, Kumar D, Kaldjian EP, Bauserman
S, Raffeld M and Jaffe ES: Primary low-grade B-cell lymphoma of the
dura: A mucosa associated lymphoid tissue-type lymphoma. Am J Surg
Pathol. 21:81–87. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Saggioro FP, Colli BO, Paixão-Becker AN,
de Rezende GG, Santos AC and Neder L: Primary low-grade MALT
lymphoma of the dura. Histopathology. 49:323–326. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Park I, Huh J, Kim JH, Lee SW, Ryu MH and
Kang YK: Primary central nervous system marginal zone B-cell
lymphoma of the Basal Ganglia mimicking low-grade glioma: A case
report and review of the literature. Clin Lymphoma Myeloma.
8:305–308. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Goetz P, Lafuente J, Revesz T, Galloway M,
Dogan A and Kitchen N: Primary low-grade B-cell lymphoma of
mucosa-associated lymphoid tissue of the dura mimicking the
presentation of an acute subdural hematoma. Case report and review
of the literature. J Neurosurg. 96:611–614. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ferguson SD, Musleh W, Gurbuxani S,
Shafizadeh SF and Lesniak MS: Intracranial mucosa-associated
lymphoid tissue (MALT) lymphoma. J Clin Neurosci. 17:666–669. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Venkataraman G, Rizzo KA, Chavez JJ,
Streubel B, Raffeld M, Jaffe ES and Pittaluga S: Marginal zone
lymphomas involving meningeal dura: Possible link to IgG4-related
diseases. Mod Pathol. 24:355–366. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ueba T, Okawa M, Abe H, Inoue T, Takano K,
Hayashi H, Nabeshima K and Oshima K: Central nervous system
marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue
type involving the brain and spinal cord parenchyma.
Neuropathology. 33:306–311. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kambham N, Chang Y and Matsushima AY:
Primary low-grade B-cell lymphoma of mucosa-associated lymphoid
tissue (MALT) arising in dura. Clin Neuropathol. 17:311–317.
1998.PubMed/NCBI
|
|
18
|
Itoh T, Shimizu M, Kitami K, Mitsumori K,
Fujita M, Ohnishi A and Nagashima K: Primary extranodal marginal
zone B-cell lymphoma of the mucosa-associated lymphoid tissue type
in the CNS. Neuropathology. 21:174–180. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Shaia J, Kerr PB, Saini A, Roberti F,
Kapil J, Jones R and Aragon-Ching JB: Mucosa-associated lymphoma
tissue of the dura presenting as meningioma. South Med J.
103:950–952. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tu PH, Giannini C, Judkins AR, Schwalb JM,
Burack R, O'Neill BP, Yachnis AT, Burger PC, Scheithauer PW and
Perry A: Clinicopathologic and genetic profile of intracranial
marginal zone lymphoma: A primary low-grade CNS lymphoma that
mimics meningioma. J Clin Oncol. 23:5718–5727. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lehman NL, Horoupian DS, Warnke RA,
Sundram UN, Peterson K and Harsh GR IV: Dural marginal zone
lymphoma with massive amyloid deposition: Rare low-grade primary
central nervous system B-cell lymphoma. Case report. J Neurosurg.
96:368–372. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Villeneuve A, Rubin F and Bonfils P:
Meningeal marginal zone B-cell lymphoma: The meningioma trap. Eur
Ann Otorhinolaryngol Head Neck Dis. 135:131–132. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kelley TW, Prayson RA, Barnett GH, Stevens
GH, Cook JR and His ED: Extranodal marginal zone B-cell lymphoma of
mucosa-associated lymphoid tissue arising in the lateral ventricle.
Leuk Lymphoma. 46:1423–1427. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Jazy FK, Shehata WM, Tew JM, Meyer RL and
Boss HH: Primary intracranial lymphoma of the dura. Arch Neurol.
37:528–529. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Miranda RN, Glantz LK, Myint MA, Levy N,
Jackson CL, Rhodes CH, Glantz MJ and Medeiros LJ: Stage IE
non-Hodgkin's lymphoma involving the dura: A clinicopathologic
study of five cases. Arch Pathol Lab Med. 120:254–260.
1996.PubMed/NCBI
|
|
26
|
Narberhaus B, Buxó J, Pérez de Olaguer J,
Forcadas P, Garcia-Bach M, Aparicio A and Ugarte A: Primary dural
lymphoma. Neurologia (Barcelona, Spain). 11:117–119. 1996.(In
Spanish). PubMed/NCBI
|
|
27
|
King A, Wilson H, Penney C and Michael W:
An unusual case of primary leptomeningeal marginal zone B-cell
lymphoma. Clin Neuropathol. 17:326–329. 1998.PubMed/NCBI
|
|
28
|
Hodgson D, David KM, Powell M, Holton JL
and Pezzella F: Intracranial extracerebral follicular lymphoma
mimicking a sphenoid wing meningioma. J Neurol Neurosurg
Psychiatry. 67:251–252. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Freudenstein D, Bornemann A, Ernemann U,
Boldt R and Duffner F: Intracranial malignant B-cell lymphoma of
the dura. Clin Neuropathol. 19:34–37. 2000.PubMed/NCBI
|
|
30
|
Neidert MC, Leske H, Burkhardt JK, Rushing
EJ and Bozinov O: A 44-year old male with right-sided facial
numbness. Dura-associated extranodal marginal zone B cell lymphoma
(MALT lymphoma). Brain Pathol. 25:113–114. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Pavlou G, Pal D, Bucur S, Chakrabarty A
and van Hille PT: Intracranial non-Hodgkin's MALT lymphoma
mimicking a large convexity meningioma. Acta Neurochir (Wien).
148:791–793; discussion 793. 2006. View Article : Google Scholar : PubMed/NCBI
|