Introduction
T-lymphoblastic lymphoma (T-LBL) is a rare subtype
of non-Hodgkin lymphoma (NHL), accounting for ~2% of all cases of
NHL (1–4). T-LBL has a high incidence in children,
in which it constitutes approximately one-third of NHL cases; it is
also more prevalent in men than in women, and is typically a highly
aggressive lymphoma with extremely poor therapeutic efficacy. It
advances rapidly, is characterized by extensive lesions and is
often accompanied by mediastinal masses and central nervous system
(CNS) infiltration. Patients with T-LBL predominantly present with
multiple lymph node involvement or mediastinal masses, but rarely
exhibit bone marrow invasion. Local compression symptoms may occur
and are often associated with tumor cells originating from the
thymus. The disease may also invade the pleura and pericardium,
causing serous cavity effusion.
Metagenomic next-generation sequencing (mNGS) can be
used for the unbiased sequencing of human and microbial nucleic
acids in clinical specimens. It has the advantages of being a
hypothesis-free diagnostic approach, requiring no culturing and
having a short turn-around time. It has been widely used in the
diagnosis and treatment of infectious diseases, and its sensitivity
is significantly higher than that of the traditional culture method
(61.0% vs. 19.5%) (5). The
metagenomic sequencing of body fluids has enabled previously
undiagnosed tumors to be identified via the detection of human
chromosome copy number variations (CNVs), and may facilitate the
early diagnosis of tumors and promote the timely and evidence-based
treatment of patients (6).
The present case report describes a case of
abdominal pain, chest tightness and shortness of breath in an
8-year-old boy. When the patient was admitted following multiple
serous cavity effusions, the imaging and clinical presentation and
routine blood biochemistry were similar those seen in infectious
diseases such as tuberculosis, leading to a delayed diagnosis.
However, a diagnosis was ultimately made based on analysis of the
serous cavity fluid using mNGS. The test excluded microbial
infection while simultaneously detecting chromosomal abnormalities
that conformed to the chromosomal characteristics of a malignant
neoplasm. Flow cytometric immunophenotyping of the pleural effusion
revealed that the neoplasm was T-LBL.
Case report
In August 2022, an 8-year-old male child was
admitted to Huishui County Lianjiang Hospital having experienced
abdominal pain for 6 days accompanied by chest tightness and
shortness of breath for >5 days. Chest digital radiography and
computed tomography (CT) were performed in the local hospital,
which indicated a large amount of left pleural effusion,
compression atelectasis and pericardial effusion in the left lung.
The patient was treated with an anti-infection regimen and a closed
chest drainage procedure following local hospitalization. Following
recurrence of the left pleural effusion, the patient was
transferred to Guizhou Provincial People's Hospital (Guiyang,
China) 3 days later. Physical examination revealed rapid breathing,
an increased heart rate, the inability to lie supine, jugular vein
irritation, a positive hepatic jugular vein reflux sign,
unobstructed left chest drainage, and bloody and turbid effusion.
The thorax was normal, without sternal percussion pain or a
subcutaneous twisting sensation when touched; however, slight
widening of the left intercostal space was observed. The
respiratory activity of the left lower lung was diminished and the
speech pattern of the patient was weak and irregular. In addition,
the percussive sound of the left lung was tympanic and its
breathing sound was significantly deeper than that of the right
lung, which exhibited a light percussive tone and deep breathing
sound. Low-pitched and distant heart sounds in the chest were heard
through a stethoscope. The ribs displayed no tenderness upon
palpation. The clinicians suggested that pericardiocentesis should
be performed immediately after cardiac tamponade; therefore, the
left closed chest drainage system was preserved. The main
laboratory findings are shown in Tables
I and II.
 | Table I.Examinations during
hospitalization. |
Table I.
Examinations during
hospitalization.
|
|
Number of
days after hospitalization |
|---|
|
|
|
|---|
| Testsa | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
|---|
| Routine blood
tests |
|
|
|
|
|
|
|
|
|
|
|
|
|
| WBC
(×109) | 14.34 | 12.4 | - | - | - | 15.66 | - | - | 13.14 | - | - | - | - |
| N% | 67.6 | 62.8 | - | - | - | 77.4 | - | - | 61.7 | - | - | - | - |
| Blood
biochemistry |
|
|
|
|
|
|
|
|
|
|
|
|
|
| CRP
(mg/l) | 46.41 | 17.96 | 14.23 | - | - | 2.62 | - | - | 0.68 | - | - | - | - |
| PCT
(ng/ml) | - | 0.21 | 0.2 | - | - | - | - | - | - | - | - | - | - |
|
Lactate | 604 | 589 | 387 | - | - | 399 | - | - | 333 | - | - | - | - |
|
dehydrogenase (U/l) |
|
|
|
|
|
|
|
|
|
|
|
|
|
| Uric acid
(µmol/l) | 500 | 331 | - | - | - | 151 | - | - | 160 | - | - | - | - |
|
α-hydroxybutyrate | 525 | 466 | 329 | - | - | 324 | - | - | 260 | - | - | - | - |
|
dehydrogenase (U/l) |
|
|
|
|
|
|
|
|
|
|
|
|
|
| Blood tumor
markers |
|
|
|
|
|
|
|
|
|
|
|
|
|
| NSE
(µg/l) | - | - | 35 | - | - | - | - | - | - | 24.1 | - | - | - |
| CA125
(U/ml) | - | - | 161 | - | - | - | - | - | - | 104 | - | - | - |
| Serous cavity
edema |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Thoracic closed | No | No | 200, | No | No | 250, | 350, | 200, | 125, | 200, | 50, | 225, | 275, |
| drain
(ml) |
|
| light |
|
| blood | blood | bloody | yellow | light | light | light | light |
|
|
|
| blood |
|
|
|
|
|
| yellow | yellow | yellow | yellow |
|
Pericardial drainage | No | No | 145, | 270, | 205, | 70, | 75, | 60, | 40, | 20, | 30, | No | No |
|
(ml) |
|
| blood | blood | blood | blood | bloody | bloody | yellow | light | light |
|
|
|
|
|
|
|
|
|
|
|
|
| yellow | yellow |
|
|
| Effusion, routine
and biochemicalb |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pigment | - | Red | - | - | - | Red | - | - | - | - | - | - | - |
|
Clearness | - | Cloudy | - | - | - | Lightly | - | - | - | - | - | - | - |
|
|
|
|
|
|
| cloudy |
|
|
|
|
|
|
|
|
Mucin | - | Positive | - | - | - | Positive | - | - | - | - | - | - | - |
| TCS
(×106/l) | - | 58,250 | - | - | - | 63,600 | - | - | - | - | - | - | - |
| ADA
(U/l) | - | 153 | - | - | - | 24.1 | - | - | - | - | - | - | - |
|
Chlorine (mmol/l) | - | 109.1 | - | - | - | 111.3 | - | - | - | - | - | - | - |
| Glucose
(mmol/l) | - | 5.75 | - | - | - | 8.34 | - | - | - | - | - | - | - |
|
Lactate | - | 873 | - | - | - | 312 | - | - | - | - | - | - | - |
|
dehydrogenase (U/l) |
|
|
|
|
|
|
|
|
|
|
|
|
|
| Etiology |
|
|
|
|
|
|
|
|
|
|
|
|
|
| Eaton's
reagent | - | 1:80+ | - | - | - | - | - | - | - | - | 1:160+ | - | - |
| Maximum temperature
(°C) | 36.7 | 36.3 | 38.6 | 38.9 | 36.7 | 36.8 | 36.9 | 36.8 | 36.9 | 38.7 | 36.9 | 36.8 | 36.9 |
| Maximum heart rate
(beats/min) | 133 | 124 | 157 | 151 | 124 | 134 | 98 | 89 | 93 | 89 | 94 | 85 | 85 |
| Table II.General results. |
Table II.
General results.
| Examinations | Findings |
|---|
| Blood
biochemistry | Blood ammonia,
blood lactate and B-type natriuretic peptide negative; renal
function, coagulation function, electrolytes, blood glucose, liver
function and myocardial enzyme normal |
| Blood tumor
markers | Carbohydrate
antigen 19-9, α-fetoprotein, carcinoembryonic antigen and ferrotin
normal |
| Etiology | Three tuberculosis
tests, T-SPOT, resist O, respiratory pathogen tests (A and B
influenza virus, adenovirus, respiratory syncytial virus,
mycoplasma and rhinovirus), Epstein-Barr virus antibody and DNA
tests, preoperative infectious diseases screen, pericardial
effusion smear and culture, pleural effusion smears and the culture
all negative |
| Rheumatic immunity
and connective tissue | Thyroid function,
complement C3 and C4, rheumatoid factor, erythrocyte sedimentation
rate, lymphocyte immunity somatotype and anti-neutrophil
cytoplasmic antibodies all negative. Antinuclear antibody profiles
for anti-nRNP/Sm and anti-Sm weakly positive |
| Imaging | High resolution
lung CT revealed inflammation and exudate in both lungs, although
mainly in the left lung, and regional compression, expansion and
pulmonary insufficiency after drainage of the left pleural
effusion; left main bronchus stenosis; blurred fat space and
unclear layers in the mediastinum; large accumulation of
pericardial effusion. Abdominal CT revealed no obvious
abnormality |
| Heart
ultrasound | Large amount of
pericardial effusion. Left ventricular systolic function
measurement normal |
Following admission, the child had a recurrent fever
with a highest recorded temperature of 38.9°C. Blood CRP was
elevated and the white blood cell count was higher than the normal
range.. Routine blood tests indicated that the percentage of
neutrophils was elevated. The pericardial and pleural effusion was
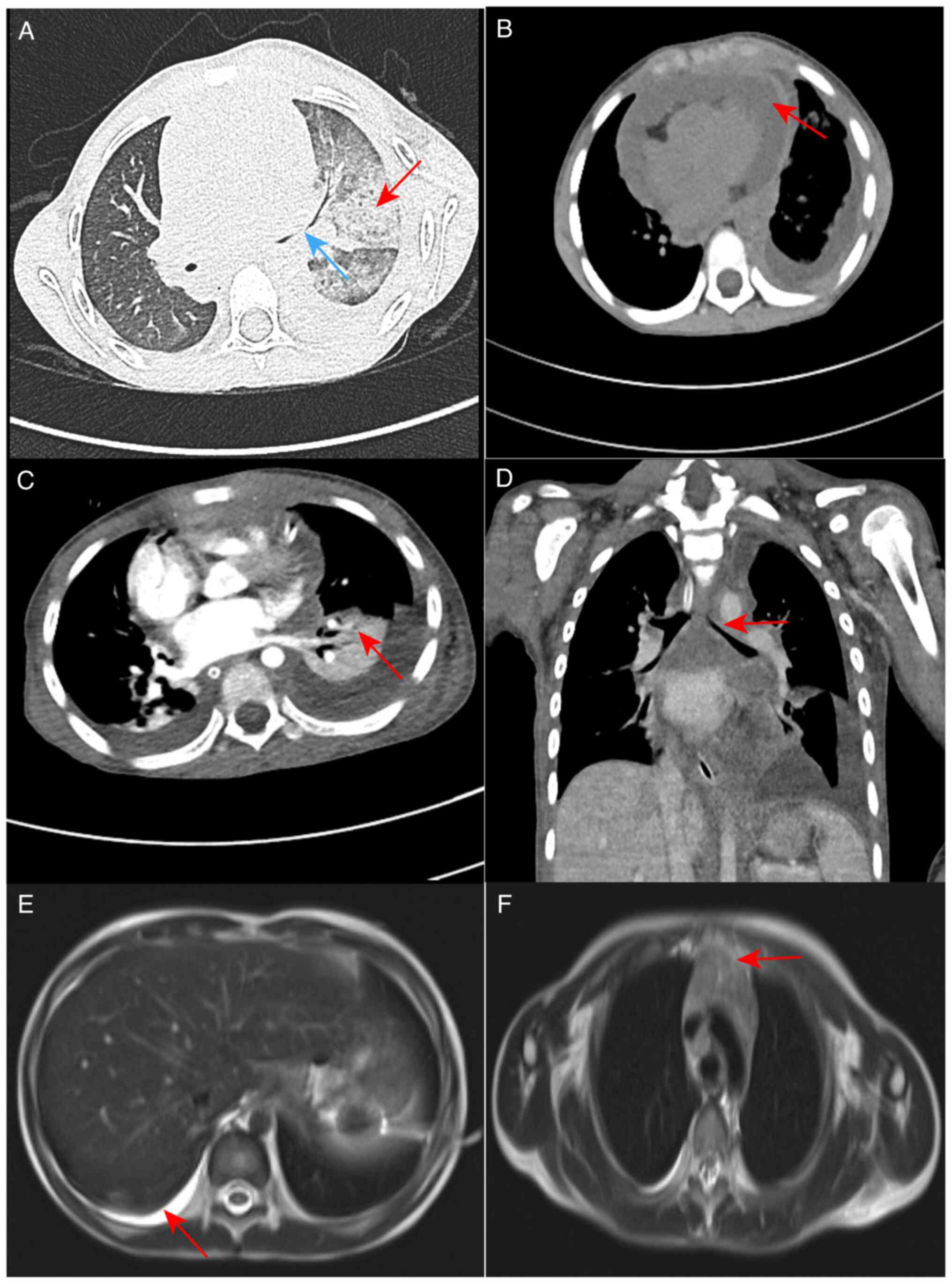
identified as an exudate. A high-resolution CT scan of the lungs
(Fig. 1A) revealed multiple
exudation sites and inflammation in both lungs. This was more
severe in the left lung, with partial compression and expansion of
the left lower lobe, left main bronchial stenosis, blurred
mediastinal borders and a large amount of fluid accumulated in the
pericardium (Fig. 1B). This was
attributed to severe necrotizing pneumonia with the possibility of
infectious disease.
Initial treatment
After admission, the left closed chest drainage
system was retained and remained unobstructed. Due to signs of a
large amount of pericardial effusion, pericardiocentesis was
performed and immediately followed by ultrasound monitoring.
Pleural reaction and heart failure occurred during the puncture,
and the patient was endotracheally intubated for mechanical
ventilation. Anti-infection treatment was cefoperazone sulbactam
(75 mg/kg/dose via intravenous infusion pump once every 8 h)
combined with azithromycin (10 mg/kg/dose via intravenous infusion
pump once daily). Anti-inflammatory treatment was performed with
methylprednisolone sodium succinate (1–2 mg/kg/dose), milrinone
(0.5 µg/kg/min) and dobutamine (5 µg/kg/min) for cardiac
stimulation. Myocardial nutrition was administered using sodium
fructose diphosphate. After these treatments, no fever was observed
and the abdominal pain, chest pain and shortness of breath were
markedly ameliorated. The endotracheal intubation and ventilator
were successfully withdrawn and the patient was able to breathe
stably using a nasal catheter. After 11 days of treatment, the
volume of pericardial drainage fluid gradually decreased and the
color of the fluid changed from bloody to pale yellow. The
condition of the patient improved following the anti-infection
treatment, which supported the diagnosis of an infectious disease.
However, the fluid volume obtained by closed-chest drainage was not
notably reduced, the daily diverted flow increased (200–350 ml),
and the color of the fluid changed from bloody to light yellow.
mNGS testing
The routine diagnostic tests were negative after
admission. However, large volumes of pericardial and pleural
effusions continued to be generated following the anti-infection
treatment. To clarify the cause of this, pericardial drainage fluid
was collected for mNGS testing and no pathogens were detected.
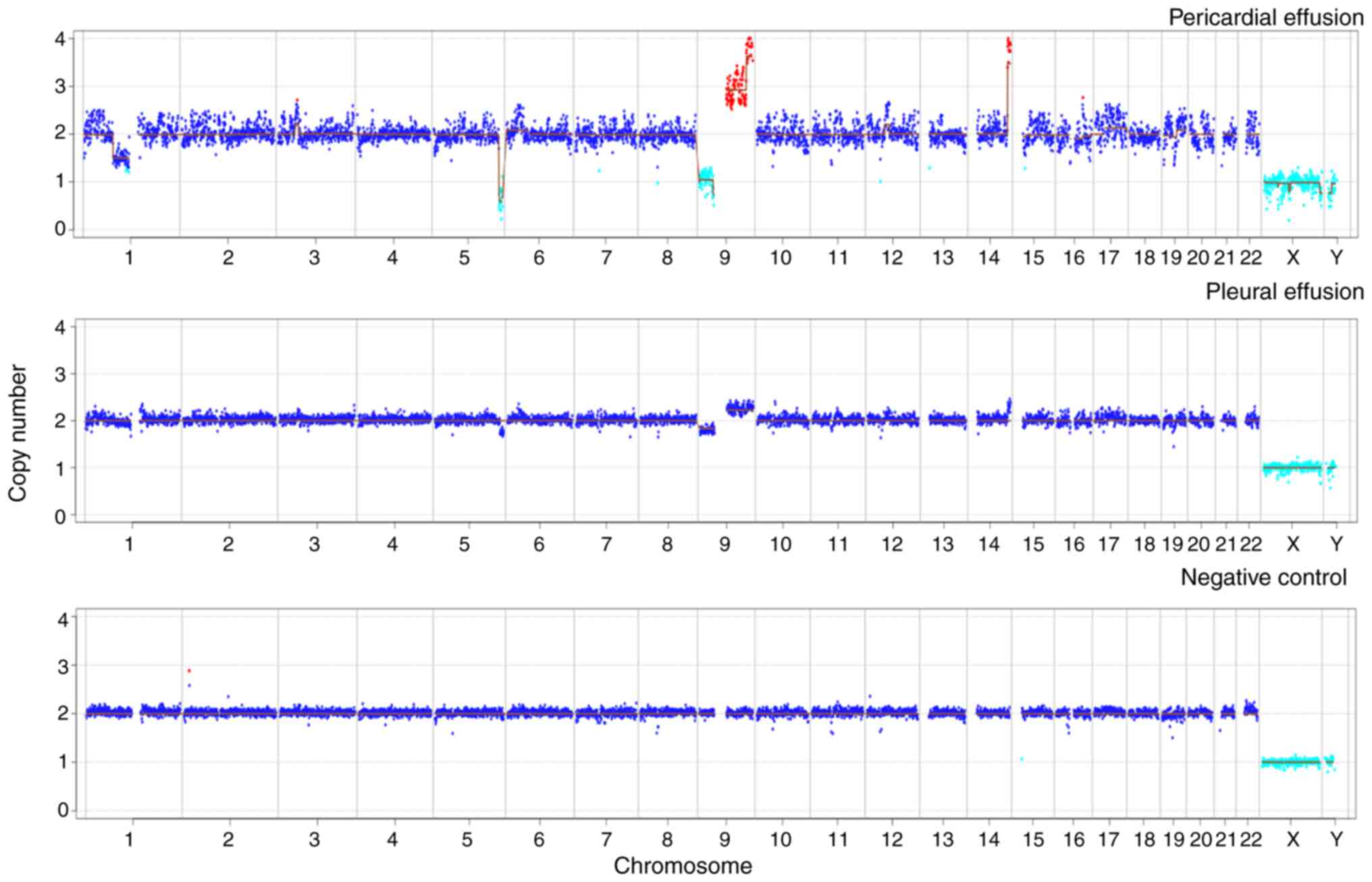
However, mNGS was also used perform a CNV analysis of the host
chromosome (Data S1). Following
normalization of the data and comparison with data from a healthy
individual with no known genetic disease, abnormalities
(duplications and deletions) were identified in chromosomes 1, 6,
9, 12, 16, 17 and 19. The deletion of large segments (>10
megabase pairs), which may have occurred due to chromosomal
instability, suggested that the patient may have a tumor. The
temperature of the patient was normal, and although the volume of
pericardial fluid drainage gradually decreased following
anti-infection treatment, the volume of thoracic drainage fluid
remained copious. Magnetic resonance imaging (MRI) examination of
the mediastinum indicated that the thymus was enlarged and its
signal was not uniform. Due to the pleural and pericardial
effusion, the left pleura appeared to be slightly thickened, and no
obvious space-occupying lesions were observed. To further
investigate the cause of the pleural effusion, mNGS was applied to
the pleural drainage fluid. The results revealed the presence of
Escherichia coli (sequence reads, 19; relative abundance,
11.18%). The CNV analysis of the pleural drainage also revealed
abnormalities, with chromosomal variant sites similar to those
found in the pericardial drainage fluid (Fig. 2). Notably, numerous expansions and
deletions were detected among the CNVs in chromosome 9, which
indicated the presence of tumor DNA in this body fluid. It must be
noted that the variation sites in the two types of drainage fluid
were not exactly the same. This is likely due to tumor nucleic acid
fragments varying in different body fluids; in general, the closer
the fluid is to the lesion, the higher the concentration of tumor
nucleic acid fragments (7).
Therefore, it was inferred that the tumor was located in the
mediastinum.
Follow-up and outcomes
After admission, testing for autoantibodies revealed
no abnormalities. No cancer cells were observed during the
cytological examination of the pericardial drainage fluid (Fig. 3A) and thoracic drainage fluid
(Fig. 3B). Furthermore,
cytomorphological examination revealed no abnormal cell hyperplasia
in the bone marrow. Flow cytology immunophenotyping of the pleural
effusion was performed (Data S1).
Gated on the CD45/side scatter dot plot, the abnormal cell
population was visible in the original cell distribution area,
comprising ~58% of the nuclear cells, which were positive for the
expression of CD3, CD4, CD5, CD7, CD10, CD38, CD58, T-cell receptor
γ/δ, cytoplasmic CD3 and terminal deoxynucleotidyl transferase. No
juvenile lymphocytes were detected in the peripheral blood. Myeloid
proliferation was observed to be significantly inhibited. According
to the World Health Organization National Comprehensive Cancer
Network (NCCN) Clinical Practice Guidelines for Oncology (second
edition, 2015) (8), the patient's
flow cytometric results were consistent with a T-LBL
immunophenotype (Fig. 3C). The
patient was diagnosed with acute T-LBL with intermediate risk and
transferred to the pediatric hematology department for further
specialist treatment. Following transfer, pre-chemotherapy
examinations were conducted and the treatment plan was determined.
This was communicated to the patient's family, who provided
informed consent. The treatment strategy adopted was in accordance
with the guidelines for the intermediate-risk disease as described
in the Pediatric Acute Lymphoblastic Leukemia Diagnosis and
Treatment Guidelines (2020 edition) (9). It included the CVDLD regimen,
comprising prednisone, dexamethasone, vindesine, daunorubicin,
cyclophosphamide and intramuscular pemaspartase as follows:
prednisone tablets (60 mg/m2/day orally on days 1–7);
dexamethasone (6–8 mg/m2/day orally or intravenously on
days 8–28, reduced for 7 days); vindesine (3 mg/m2/day
intravenously on days 8, 15, 22 and 29); daunorubicin (30
mg/m2/day for 1 h on days 8, 15, 22 and 29;
cyclophosphamide (1 g/m2 by intravenous drip on day 8);
and intramuscular pemaspartase injection (2,500 U/m2/day
on days 9 and 23, twice in total). Remission was observed.
Evaluation of the bone marrow cells revealed that on day 15 of the
CVDLD-induced remission, the cell morphology was M1, but the bone
marrow minimal residual disease (MRD) was <3.4%, leading to an
adjustment of the risk group to high risk. By day 33 of CVDLD
treatment, the morphology of bone marrow cells exhibited a complete
response, and the bone marrow MRD was <0.01%. The patient
continued to be evaluated, and eventually achieved a complete
response following two rounds of early intensive therapy with CAML
(10) [Cytoxan, 750–1000
mg/m2/day, once a day, intravenously; cytosine
arabinoside, 75–100 mg/m2/day, for 7–8 days, 1–2 times a
day, intravenously; 6-mercaptopurine, 50–75 mg/m2/day,
for 7–14 days, orally on an empty stomach. Pegaspargase (CAML
regimen) 2,000-2,500 U/m2/day, on day 2, once,
intramuscularly; or home DXM on top of CAML 8 mg/m2/day
orally, days 1–7]. Next, the child began the consolidation protocol
according to treatment guidelines.
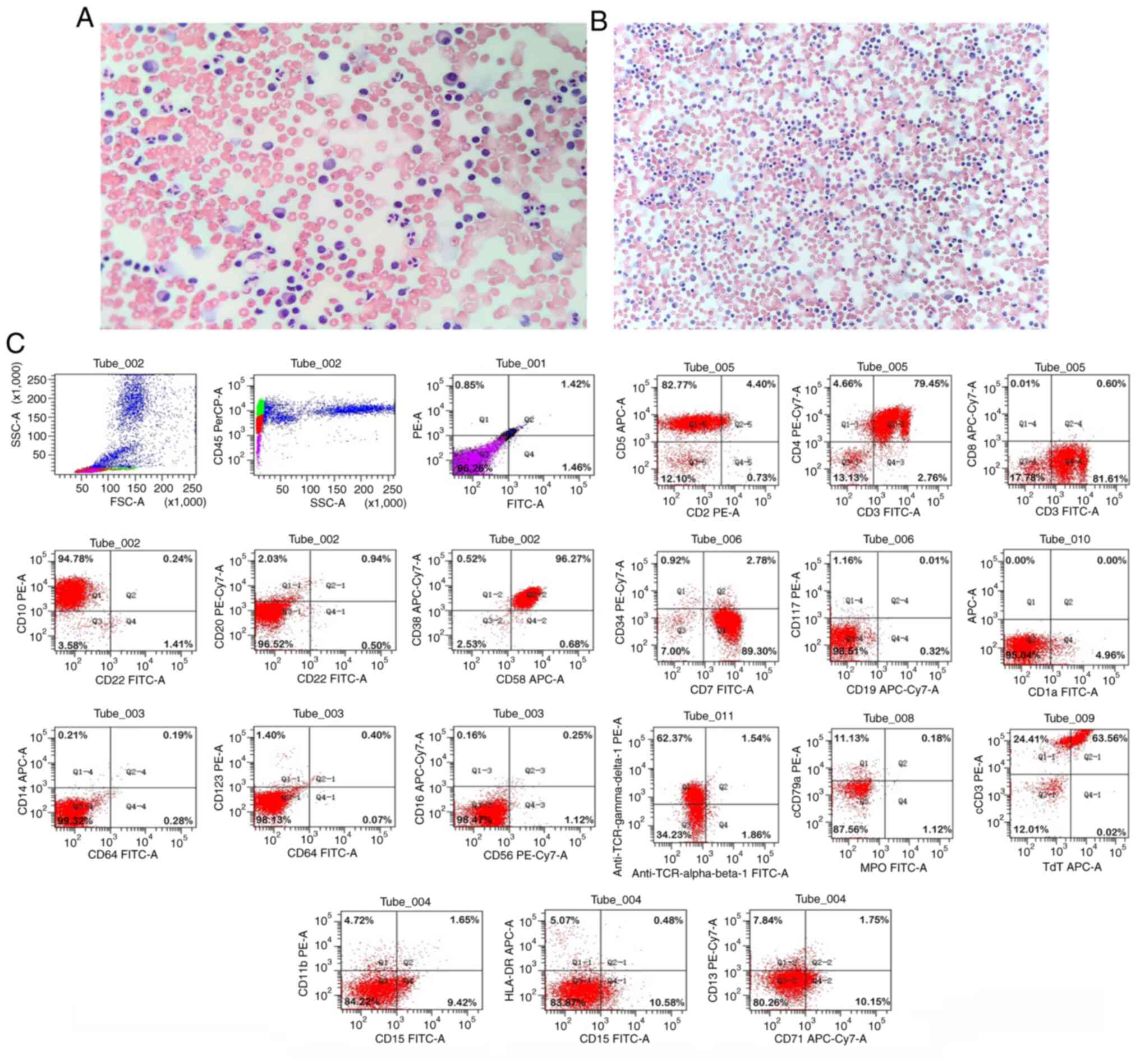 | Figure 3.Papanicolaou staining and flow
cytometry results for the present case. Papanicolaou staining
revealed no heterotypic cells in the (A) pericardial drainage fluid
(magnification, ×200) and (B) thoracic drainage fluid
(magnification, ×100). (C) Gate analysis on the CD45/SSC dot plot
showed an abnormal cell population in the original cell
distribution region, comprising ~58% of the nuclear cells, with
positive expression of CD3, CD4, CD5, CD7, CD10, CD38, CD58, TCR
γ/δ, cCD3 and TdT. Myeloid proliferation was significantly
inhibited. SSC, side scatter; TCR, T-cell receptor; cCD3,
cytoplasmic CD3; TdT, terminal deoxynucleotidyl transferase. |
Discussion
The present report describes a pediatric patient
with T-LBL who presented with abdominal pain, chest tightness and
shortness of breath and was initially diagnosed with multiple
serous effusions. Laboratory tests and imaging findings, including
negative results for tumor markers and serous effusion cells,
normal blood tests and response to repeated anti-infection
treatment indicated an infection. However, multiple CNVs in the
host chromosome were detected by mNGS, suggesting the possibility
of a tumor. Flow cytological immunotyping of the pleural effusion
finally confirmed the diagnosis of T-ALL/LBL. T-cell lymphomas
mainly present as LBL with a small number presenting as ALL.
T-ALL/LBL commonly affects older children, with a median onset age
of 9–12 years. Clinical symptoms include an anterior mediastinal
mass, airway compression symptoms, dysphagia and venous
obstruction. Lymph node lesions are common, particularly in the
neck, supraclavicular and axilla regions, while ~50% of cases have
bone marrow involvement. CNS metastases occur in ~15% of cases,
with meningeal lesions occurring more frequently than parenchymal
lesions (11).
Multiple serous body cavity effusion is a frequently
occurring disease, which comprises the simultaneous presence of
effusion in two or more of the serosal cavities, which comprise the
pericardial, thoracic and abdominal cavities. Due to the complex
etiology of multiple serous body cavity effusions and the
heterogeneous clinical manifestations, diagnosis is challenging.
Moreover, the differentiation of malignant and nonmalignant
effusions is important for the subsequent treatment and prognostic
evaluation of this disease. Multiple serous body cavity effusion
can occur as an isolated disease or in association with a wide
spectrum of systemic diseases. A previous study conducted an
etiological analysis of 241 patients with multiple serous body
cavity effusions, of which 11.6% had an unknown etiology (12). The most common cause of these
effusions in patients with clear etiology was malignancy (32.8%),
followed by autoimmune diseases (13.3%), tuberculosis (8.3%),
cirrhosis (7.9%) and cardiac insufficiency (6.2%). In another study
in which 92 patients with multiple serous body cavity effusions
were analyzed, 38% of cases had unknown etiology, and the most
common diagnosis in patients with clear etiology was malignancy
(30.4%), followed by infectious diseases (15.2%) and autoimmune
diseases (13.0%) (13).
In the relevant auxiliary examination of the present
case, the results of autoimmunity-associated tests were negative
and did not support an autoimmune disease. Etiological examination
revealed that the adenosine deaminase (ADA) levels in the
pericardial effusion were markedly increased, and the measurement
of ADA activity in serous cavity effusions has been shown to have
high specificity and sensitivity in the diagnosis of tuberculous
infection (14). However, in the
present case the ADA levels in the pleural effusion were normal,
and the results of tuberculosis and T-SPOT. TB assays were normal.
These negative results did not support the involvement of
tuberculosis. The mNGS sequencing results for the pleural effusion
suggested that a nosocomial Escherichia coli infection must
be considered. The blood mycoplasma antibody titer of the child was
elevated (1:160), but his mycoplasma nucleic acid test was negative
and therefore not supportive of a recent infection. The negative
pathogen detection results did not support an infectious disease as
the cause of the effusions. No secondary or tertiary blood
reduction was evident and no original naive T cells were detected.
The carbohydrate antigen 19-9, α-fetoprotein, carcinoembryonic
antigen and ferritin results were normal. The chest CT scan and
enhancement did not reveal any space-occupying lesions. Mediastinal
MRI scan and enhancement also did not indicate any organic lesions,
but instead suggested enlargement of the mediastinum and small
hilum lymph nodes. T-LBL is known to present a mediastinal mass in
60–70% of cases, often with shortness of breath, due to superior
vena cava compression or pericardial and/or pleural effusion
(15). Tests and procedures used to
diagnose T-cell blastic lymphoma include bone marrow biopsy,
immunohistochemistry, flow cytometry, polymerase chain reaction
testing and the fluorescence in situ hybridization testing
of major chromosomal translocations. Furthermore, in certain cases,
MRI and positron emission tomography-CT can facilitate the
diagnostic examination. In the diagnosis and treatment of the
present child, based on the rarity of T-LBL, the nonspecific
diagnosis of malignancy by the cytological examination of multiple
serous body cavity effusions, and the low positivity rate of
carcinoembryonic antigen, numerous tests did not support the
diagnosis of cancer, which easily resulted in a misdiagnosis.
mNGS has been used increasingly widely in the clinic
in recent years, and has gradually emerged as an important method
for the detection of pathogens in infectious diseases. When
pathogenic microorganisms are detected in a patient sample, a large
number of host nucleic acids are also present; therefore, the host
nucleic acid must be filtered. A number of studies have assisted in
the diagnosis of lymphoma (16),
meningeal carcinoma (17) and
squamous cell lung carcinoma (18)
via the analysis of CNVs in the host chromosome. Cancer cells are
characterized by structural variation during division, as
chromosomal instability is common in tumors (19). A CNV is a change in the copy number
of one or more genes, and CNVs are an important component of the
genetic variation involved in the development of multiple types of
cancers. CNVs are present in ~90% of solid tumors (20), but the sensitivity for their
detection is low (21). CNVs caused
by tumors appear as duplications or deletions of large fragments or
entire chromosomes, so the large CNVs (>10 M) encompassing
several chromosomes were unlikely to be false-positives (6). In the present case, several host
chromosomes in the pericardial effusion were found to contain
abnormalities, although in lower quantities than would be expected
in a patient with congenital chromosomal abnormalities (18). This allowed a diagnosis of genetic
chromosomal changes to be excluded. The chromosomal examination of
multiple serous cavity effusions is considered to be beneficial for
the diagnosis of benign and malignant diseases (22). mNGS is able to detect many types of
pathogens in one test, including low levels of pathogens, and is
useful for detecting coinfections (23). However, it also presents false
positives and can be difficult to interpret. It is also
expensive.
As a novel method for the clinical detection of
infectious pathogens, mNGS can analyze human CNVs or aneuploidy in
addition to providing data on pathogenic microbes. Even though the
detection of chromosomal CNVs using mNGS cannot provide a
definitive cancer diagnosis, following the exclusion of infection
it can provide an early warning of a clinical tumor diagnosis and
improve the likelihood of tumor detection. In the present study,
mNGS performed on human body fluids suggested the presence of a
tumor. It may serve as a reference case for the analysis of
pathogens and chromosomal CNVs in the detection of pediatric
T-LBL.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available in the Sequence Read Archive
[https://www.ncbi.nlm.nih.gov/sra/?term=PRJNA901203].
Authors' contributions
LQM is the primary physician who performed the
diagnosis and treatment of the patient. JJ and JS collected and
analyzed clinical and sequencing data. ZMY processed images, and
collected and collated data. LQM, DH and LYL wrote the manuscript.
DH and LYL conceived and designed the study. LQM, DH and LLY
confirm the authenticity of all the raw data. All authors have read
and approved the final version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the legal
guardian of the patient for the publication of any potentially
identifiable images or data in this article.
Competing interests
LYL and ZMY are employees of Hangzhou Matridx
Biotechnology Co., Ltd. The other authors declare that they have no
competing interests.
References
|
1
|
Cortelazzo S, Ponzoni M, Ferreri AJ and
Hoelzer D: Lymphoblastic lymphoma. Crit Rev Oncol Hematol.
79:330–343. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Park HS, McIntosh L, Braschi-Amirfarzan M,
Shinagare AB and Krajewski KM: T-cell non-hodgkin lymphomas:
spectrum of disease and the role of imaging in the management of
common subtypes. Korean J Radiol. 18:71–83. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Swerdlow SH, Campo E, Pileri SA, Harris
NL, Stein H, Siebert R, Advani R, Ghielmini M, Salles GA, Zelenetz
AD and Jaffe ES: The 2016 revision of the World Health Organization
classification of lymphoid neoplasms. Blood. 127:2375–2390. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Vose J, Armitage J and Weisenburger D:
International peripheral T-cell and natural killer/T-cell lymphoma
study: Pathology findings and clinical outcomes. J Clin Oncol.
26:4124–4130. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hogan CA, Yang S, Garner OB, Green DA,
Gomez CA, Dien Bard J, Pinsky BA and Banaei N: Clinical impact of
metagenomic next-generation sequencing of plasma cell-free DNA for
the diagnosis of infectious diseases: A multicenter retrospective
cohort study. Clin Infect Dis. 72:239–245. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gu W, Talevich E, Hsu E, Qi Z, Urisman A,
Federman S, Gopez A, Arevalo S, Gottschall M, Liao L, et al:
Detection of cryptogenic malignancies from metagenomic whole genome
sequencing of body fluids. Genome Med. 13:982021. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tivey A, Church M, Rothwell D, Dive C and
Cook N: Circulating tumour DNA-looking beyond the blood. Nat Rev
Clin Oncol. 19:600–612. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Alvarnas JC, Brown PA, Aoun P, Ballen KK,
Barta SK, Borate U, Boyer MW, Burke PW, Cassaday R, Castro JE, et
al: Acute Lymphoblastic Leukemia, Version 2.2015. J Natl Compr Canc
Netw. 13:1240–1279. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tianyou Wang XS, Zhang Y, Tang J, Jin L,
Yang J, Duan Y, Zhou C, Gao Z and Qu X: Childhood lymphoblastic
lymphoma treatment standard (2019 update). National Health
Commission of the PRC. 716:10–29. 2019.(In Chinese).
|
|
10
|
Koprivnikar J, McCloskey J and Faderl S:
Safety, efficacy, and clinical utility of asparaginase in the
treatment of adult patients with acute lymphoblastic leukemia. Onco
Targets Ther. 10:1413–1422. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhang HL, Bai ZY, Zhang MX and Xi YF:
Advances in molecular genetics of acute T lymphoblastic
lymphoma/leukemia. Zhonghua Bing Li Xue Za Zhi. 49:870–873.
2020.(In Chinese). PubMed/NCBI
|
|
12
|
Zhang Hong CB: Clinical analysis of 241
cases with multiserosal cavity effusion. J Clin Int Med.
20:644–646. 2003.
|
|
13
|
Losada I, González-Moreno J, Roda N,
Ventayol L, Borjas Y, Domínguez FJ, Fernández-Baca V,
García-Gasalla M and Payeras A: Polyserositis: A diagnostic
challenge. Intern Med J. 48:982–987. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Li Jiao ZY, Qu Yi and Mu Zhi:
Evidence-based evaluation of the diagnostic value of adenosine
deaminase in tuberculous serosal cavity effusion. Chin J
Evidence-Based Med. 10:495–498. 2010.
|
|
15
|
Portell CA and Sweetenham JW: Adult
lymphoblastic lymphoma. Cancer J. 18:432–438. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Liu K, Gao Y, Han J, Han X, Shi Y, Liu C
and Li J: Diffuse large B-cell lymphoma of the mandible diagnosed
by metagenomic sequencing: A case report. Front Med (Lausanne).
8:7525232021. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mohammad NS, Nazli R, Zafar H and Fatima
S: Effects of lipid based multiple micronutrients supplement on the
birth outcome of underweight pre-eclamptic women: A randomized
clinical trial. Pak J Med Sci. 38:219–226. 2022.PubMed/NCBI
|
|
18
|
Wei P, Gao Y, Zhang J, Lin J, Liu H, Chen
K, Lin W, Wang X, Wang C and Liu C: Diagnosis of lung squamous cell
carcinoma based on metagenomic next-generation sequencing. BMC Pulm
Med. 22:1082022. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Shlien A and Malkin D: Copy number
variations and cancer. Genome Med. 1:622009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Taylor AM, Shih J, Ha G, Gao GF, Zhang X,
Berger AC, Schumacher SE, Wang C, Hu H, Liu J, et al: Genomic and
functional approaches to understanding cancer aneuploidy. Cancer
Cell. 33:676–689.e3. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Guo Y, Li H, Chen H, Li Z, Ding W, Wang J,
Yin Y, Jin L, Sun S, Jing C and Wang H: Metagenomic next-generation
sequencing to identify pathogens and cancer in lung biopsy tissue.
EBioMedicine. 73:1036392021. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zheng D, Zeng L, Gu H and Guan X: Clinical
studies of cell chromosomal detection in the diagnosis of malignant
multiserosal cavity effusion. Chin J Clinicians (Electronic
Edition). 3:602–607. 2009.
|
|
23
|
Yan L, Sun W, Lu Z and Fan L: Metagenomic
next-generation sequencing (mNGS) in cerebrospinal fluid for rapid
diagnosis of Tuberculosis meningitis in HIV-negative population.
Int J Infect Dis. 96:270–275. 2020. View Article : Google Scholar : PubMed/NCBI
|