Introduction
Struma ovarii (SO) is a unique monodermal teratoma
that is defined as having thyroid tissue accounting for >50% of
teratoma components (1). It is
estimated that 2–5% of ovarian teratomas and <1% of all ovarian
tumors can be classified as SO (2).
Malignant transformation of SO, namely malignant struma ovarii
(MSO), is an extremely rare entity that is observed in ~5% of the
cases (3). Management of MSO
remains controversial due to its rarity (4). Conservative surgery with personalized
radioiodine therapy (RAI), aggressive treatment combined with
comprehensive staging surgery with total thyroidectomy (TT), and
RAI regardless of the presence of metastatic diseases, have been
proposed in previous studies (5–7). The
feasibility of fertility preservation and the survival outcomes
have also been evaluated, but the risk factors are inconsistent
(8).
Although patients with MSO suffer a significantly
increased risk of primary thyroid cancer in the neck, to the best
of our knowledge, there are currently only a small number of cases
documented in the literature (9).
The current study presents a case of MSO coexisting with primary
cervical papillary thyroid cancer (PTC) to further investigate the
clinical characteristics, treatment options and survival outcomes
of this particularly rare entity.
Case report
A 44-year-old woman was admitted to Peking Union
Medical College Hospital (Beijing, China) in September 2019 due to
an ovarian mass first identified ~3 years ago. An ultrasound
examination revealed a 7.1×4.7-cm solid-cystic mass in the left
adnexal area, with plentiful blood signals identified by color
Doppler imaging (Fig. 1A). A 3-cm
anterior uterine myoma was also noted. Routine thyroid
ultrasonography showed a 0.5-cm solid nodule in the right lobe near
the isthmus, which was potentially malignant (Thyroid Imaging
Reporting and Data System grade 4c) (10). Multiple cervical lymph nodes
measuring 1.1–1.3 cm, located at right region VI, were detected.
Another notable finding was an elevated serum CA125 level (67 U/ml;
normal range, 0–35 U/ml). The patient was euthyroid and the serum
thyroglobulin (TG) level was also within the normal range (23.1
ng/ml; normal range, 1.4–78 ng/ml).
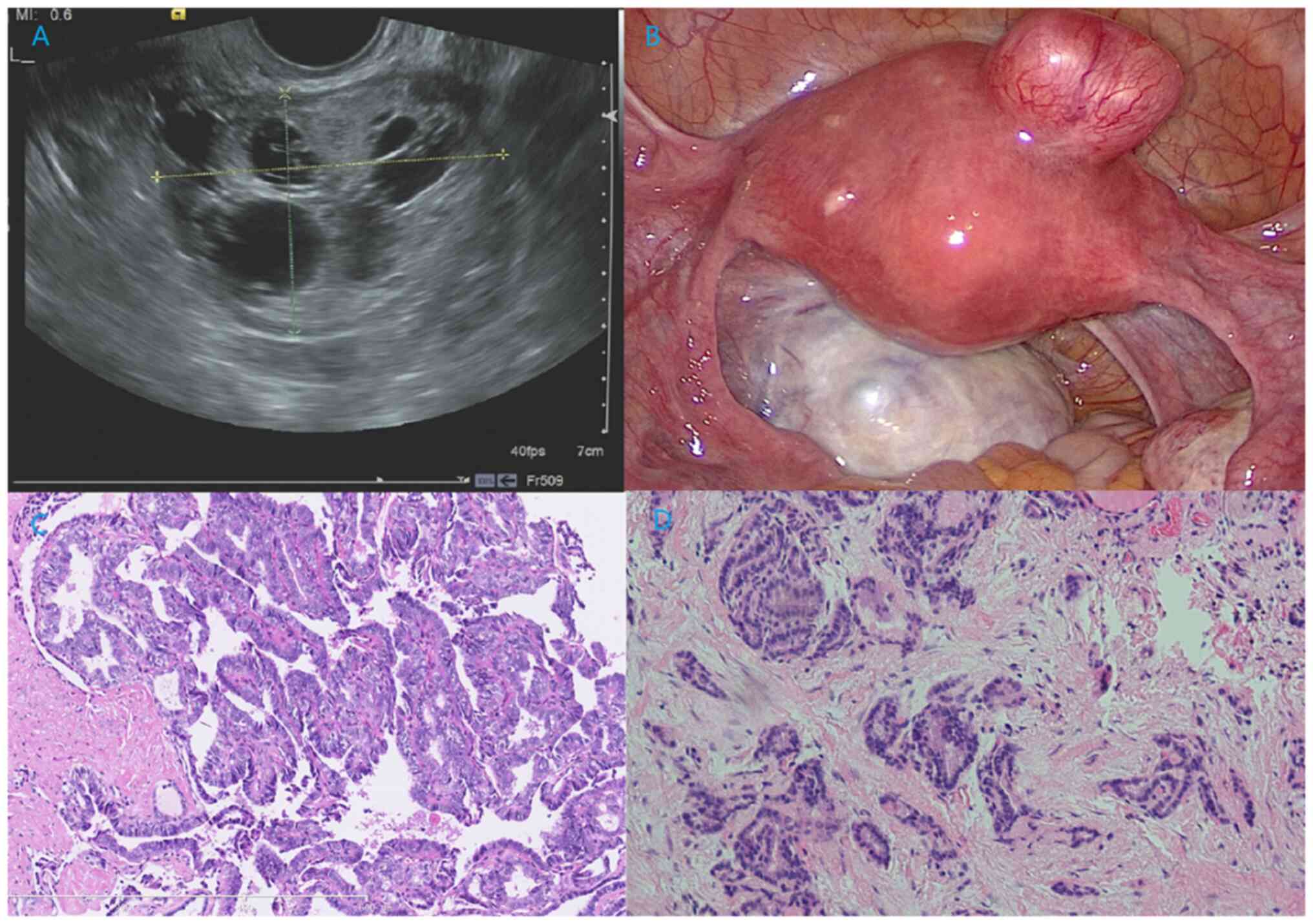 | Figure 1.Ultrasound and pathologic image of
this patient. (A) Ultrasound of the ovarian mass revealed a round,
multilocular, solid-cystic shape. Several round, echoless regions
could be noted, which was similar to a palette. (B) Intraoperative
exploration showed a 6-cm solid-cystic left ovarian mass with
plentiful vascularization, and a 3-cm myoma was also noted in the
anterior uterine wall. (C) Pathological analysis of MSO showed PTC
arising in SO. Papillary structures lined by one or more layers of
tumor cells were observed. The tumor cells were crowded, in round
or oval nuclei shapes, and the nuclei of some neoplastic cells were
enlarged, clear, ‘ground glass opacity (unclear nuclei) and
overlapping (H&E staining; ×100 magnification). (D)
Pathological analysis of primary thyroid cancer in the neck
demonstrating non-typical papillary structures (H&E staining;
×100 magnification). H&E, hematoxylin and eosin. |
An exploratory laparoscopy was conducted, showing a
6-cm solid-cystic left ovarian mass with plentiful vascularization,
and a 3-cm myoma was also noted in the anterior uterine wall
(Fig. 1B). No positive findings
were detected on the right ovary or in the abdominopelvic cavity.
An ovarian cystectomy and myomectomy were conducted. The pathology
(10% formalin solution, 20°C for 30 min; 10 µm; HE stain, 20°C for
30 min; light microscope) of the ovarian mass showed struma ovarii
with focal PTC (3 mm; Fig. 1C).
Papillary structures lined by one or more layers of tumor cells
were observed, and the nuclei of some neoplastic cells were
enlarged, clear, ‘ground glass opacity (unclear nuclei)’ and
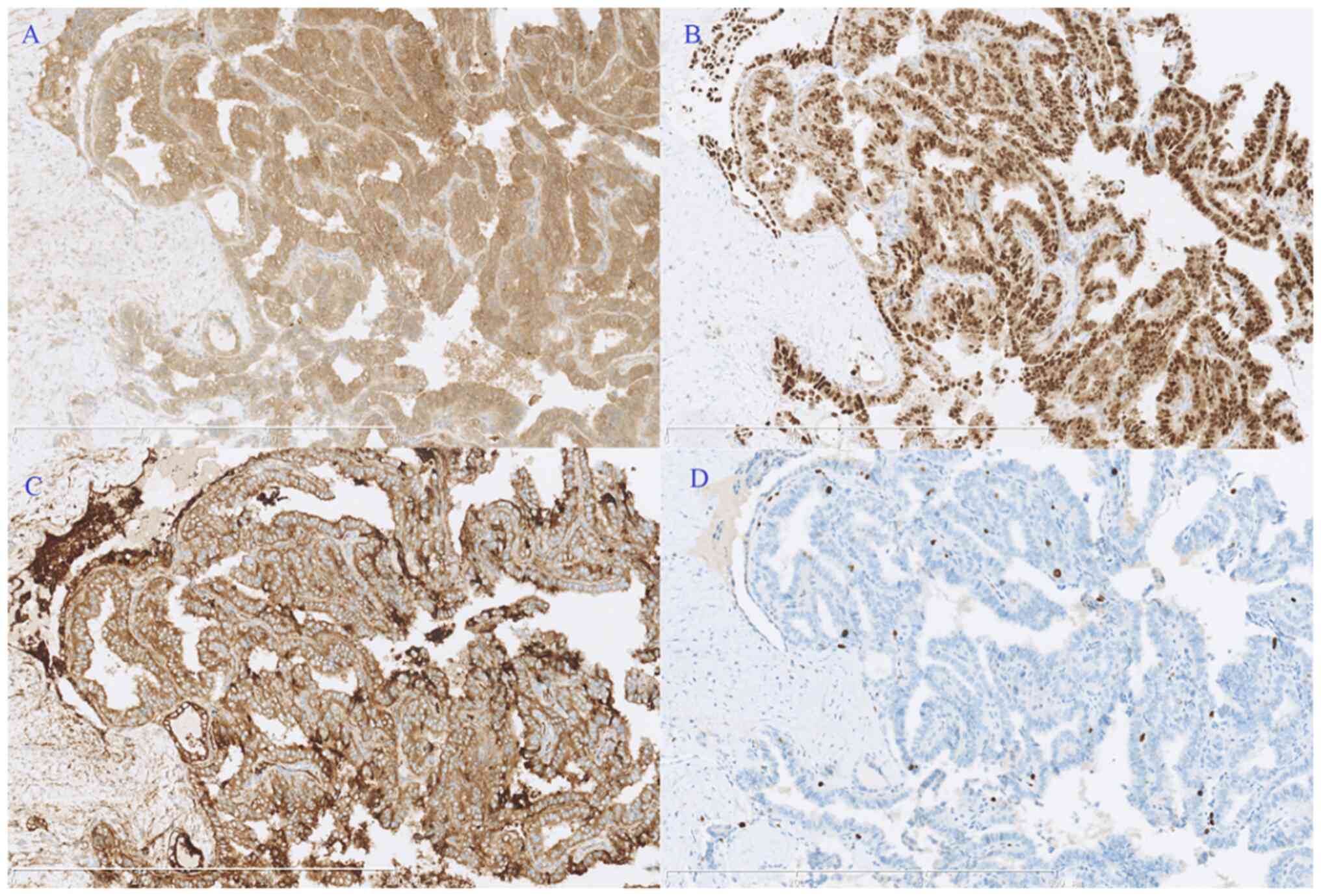
overlapping. Immunohistochemical staining demonstrated positive
expression of calretinin thyroxin and thyroid transcription
factor-1, with a Ki-67 index of 5% (Fig. 2). A unilateral salpingo-oophorectomy
(USO) was performed 2 weeks later based on this result. No tumor
cells were found upon peritoneal washing and no residual tumor
could be identified in the second surgical pathological analysis.
Approximately 2 months later, the patient underwent a TT, and the
frozen section of the right lobe nodule revealed papillary growth
with enlarged, ground glass opacity features of the tumor cells,
confirming the diagnosis of a PTC. Therefore, a right zone VI
cervical lymph node resection (ipsilateral central node dissection)
was performed, but the pathological results showed chronic
inflammation. The final pathology showed follicular-variant PTC (5
mm) without capsular involvement or vascular invasion, and no
extrathyroidal extension (Fig. 1D).
Postoperative contrast enhanced computed tomography scans of the
neck, thorax, abdomen and pelvic cavity, and whole-body iodine
scans showed no residual lesions. Therefore, the stage of thyroid
cancer in the neck was pT1aN0M0 (AJCC TNM staging system for
thyroid cancer) (11).
The patient recovered uneventfully and the serum TG
level rapidly decreased to an undetectable level (<1.4 ng/ml)
postoperatively. No further adjuvant therapy was conducted, and a
combination of TG and CA125 assessment, and imaging examinations
(cervical and pelvic ultrasonography), were performed at 3–6 month
intervals for follow-up. To date, no evidence of MSO or cervical
thyroid cancer has been detected for >4 years.
Literature review
A comprehensive literature review was performed in
PubMed (pubmed.ncbi.nlm.nih.gov/), Web of Science (https://www.webofscience.com/wos/), Scopus
(https://www.scopus.com/) database using the
following keywords: ‘malignant struma ovarii’; ‘metastatic
malignant struma ovarii’; ‘malignant ovarian teratoma’; ‘thyroid
carcinoma arising in struma ovarii’; ‘struma ovarii’. The present
study also evaluated references cited by these articles. Only
articles in English published between 1960 and 2023 were examined.
The other 13 known cases of MSO coexisting with primary thyroid
cancer in the neck that had detailed clinical characteristics,
treatment information and results of follow-up were identified and
summarized (Table SI) (12–24).
Several cases of MSO with thyroid cancer in the neck without
follow-up outcomes were excluded (25,26).
Benign struma ovarii, or MSO without coexisted with thyroid cancer
in the neck, or patients without documented clear clinical
characteristics, treatment, and outcomes were also excluded.
The median age of the patients was 44.0 years
(range, 30–78 years) and the condition mostly occurred in those
individuals aged in their 40s. PTC was the most common pathological
subtype in both MSO and thyroid cancer. Only two cases of FTC in
MSO were noted, but none had FTC in the neck in this group. The
pelvic surgery at initial treatment included USO, bilateral
salpingo-oophorectomy (BSO), hysterectomy with BSO and
comprehensive staging surgery without fertility-sparing. A total of
9 patients also received RAI at varied doses (28.3–179 mCi).
Although two patients relapsed in the group who received surgery
alone during follow-up, they were both cured by RAI at recurrence
(12,22). One of these patients also received
repeated surgery.
The median follow-up time was 2 years, 11 patients
remain alive with NED (12–14,16–22,24)
and one was alive with the disease (23). Only 1 patient died of another
disease (15).
Discussion
The risk of the coexistence of thyroid cancer in the
neck is significantly increased in patients with MSO, compared with
common population (4). In several
large cohort studies, the incidence of cervical thyroid cancer in
patients with MSO was 2.6–8.8% (4–6), while
the highest incidence of thyroid cancer in the neck was ~10 cases
per 10,0000 person-years (27).
Researchers have proposed that this may be attributed to more
rigorous thyroid screening and ‘field cancerization’ in patients
with MSO (6,17). Leong et al (17) found that the two malignancies may be
independent in existence, but the early genomic instability may
explain these multifocal carcinogeneses. Poli et al
(28) identified similar
histomorphological and molecular features in thyroid components of
MSO (such as BRAF, RAS and KIT mutations) and primary thyroid
cancer in a series of 6 patients, and a review of 48 cases reported
molecular profiles. In primary thyroid cancer, some specific gene
mutations, including BRAFV600E, and telomerase reverse
transcriptase promoter mutations are significantly associated with
the prognosis (29). Hence, routine
thyroid imaging examinations should be recommended in patients with
MSO, and gene detection methods for thyroid cancer are also
encouraged.
Patients with MSO usually have satisfactory survival
outcomes (9). In 2015, Goffredo
et al (4) found the 5-, 10-
and 20-year overall survival (OS) rate in these patients was 96.7,
94.3 and 84.9%, respectively (4).
Even in patients with metastatic MSO, the outcomes remained
promising with 5-, 10- and 15-year OS rates of 89.3, 82.4 and
65.9%, respectively, in a large cohort of 79 patients (6). Furthermore, patients with MSO confined
to the ovary were found to have better outcomes, with a 5- and
20-year disease-specific survival (DSS) rate of 95.3 and 88.7%,
respectively (5). These findings
are also consistent with other similar case reports and systematic
reviews that revealed inexact 5-year OS rate >90% (30,31).
Therefore, it has always been controversial whether conservative or
aggressive treatment should be administered in patients with
MSO.
Most of these patients underwent aggressive
management with pelvic and thyroid surgery, and TT followed by RAI,
while 4 patients received surgery alone. However, according to the
European Society for Medical Oncology guidelines for thyroid cancer
(32), only 3 patients needed RAI
after TT, if MSO confined to the ovary was not considered as an
indication for RAI. Marti et al (14) suggested that pelvic surgery alone
may be enough for MSO confined to the ovary, as the 25-year
cumulative recurrence rate was only 7.5%. Our previous study found
that the benefit of RAI was unclear in terms of lowering the
recurrence (94.4 and 60.1% with and without RAI, respectively) and
DSS (95.3%) rates in a cohort of 125 patients with MSO confined to
the ovary (5). Furthermore,
although 2 patients had a relapse in the present literature review,
including 1 patient who should have received initial RAI due to
metastatic disease but did not, they were both successfully cured
by RAI with or without repeat surgery. This suggested that some
patients might not need RAI at initial treatment but that they were
being given it, possibly leading to overtreatment.
At present, most patients with MSO are administered
RAI based on the risk stratifications of primary thyroid cancer
(9). For example, Yassa et
al (33) suggested that
patients with tumors >2 cm in diameter, disease outside the
ovaries or aggressive histological features should be considered
for postoperative RAI therapy. However, directly applying the risk
stratifications of primary thyroid cancer to MSO may not be
suitable and lacks evidence from large cohorts, which would
inevitably result in most patients being given RAI (13). The size of the ovarian mass can
easily be much larger than the thyroid nodules, and the mass size
does not equal the carcinoma size in MSO (6). The cancer components are mostly very
small focal struma components, and measuring tumor size in a
situation where cancer and teratomatous components blend would be
extremely difficult. Furthermore, studies found that no potential
risk factors were identified in MSO confined to the ovary, while
age >55 years and International Federation of Gynecology and
Obstetrics stage (34) IV were
prognostic factors in metastatic MSO in large cohorts, but the mass
size, presence of ascites, surgical options and pathological
subtypes were not (5,6,9).
In the literature review cohort of patients with MSO
coexisting with primary thyroid cancer, no patients died of the
disease, confirming the excellent survival outcomes in this
subgroup and that coexistence with primary thyroid cancer does not
seem to be a risk factor. Therefore, the risk stratifications of
these two synchronous malignancies may be better determined
independently. Reserving TT for patients with MSO with suspected
primary thyroid cancer or for those planning to receive RAI may be
more reasonable. Whether the patients receive RAI therapy should be
determined by the risk stratification of both the cervical thyroid
cancer and the MSO (5,6,9,14).
Namely, personalized RAI may be preferred in MSO confined to the
ovary while RAI is recommended in patients with metastatic MSO
(5,6).
Previously, several studies with large sample sizes
have fully discussed the significance of conservative surgery
(5,6,9). Given
the fact that MSO is greatly different from common epithelial
ovarian carcinoma in terms of biological behavior and survival
outcome, less aggressive surgery should also be advocated. In
patients with MSO confined to the ovary or metastatic MSO, more
aggressive surgery did not significantly improve the survival
outcomes (5,6). The current case received USO without
adjuvant therapy but showed NED for >4 years, again supporting
the conservative surgical option.
Due to the extremely rare nature of MSO, more
evidence of practical risk stratifications and application of RAI
should be gathered to determine in which circumstance and doses RAI
should be applied. Survival outcomes from long-term close follow-up
should also be further investigated.
In conclusion, the prognosis of patients with MSO
confined to the ovary with synchronous primary thyroid cancer in
the neck is satisfactory, and USO with personalized RAI therapy may
be a preferred treatment option balancing the quality of life and
therapeutic effect. Whether RAI is administered should be based on
the risk group of cervical thyroid cancer in this population.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The present study was supported by the National High-Level
Hospital Clinical Research Funding (grant no. 2022-PUMCH-B-083) and
the Chinese Academy of Medical Sciences Innovation Fund for Medical
Sciences (grant no. 2022-I2M-C&T-B-023).
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
SL wrote the manuscript and participated in study
conceptualization. RH completed the pathological analysis and
participated in the literature review. JY conceived the study
design and modified the manuscript. All authors have read and
approved the manuscript. SL, RP and JY confirm the authenticity of
all the raw data.
Ethics approval and consent to
participate
This retrospective study was approved by the Ethics
Committee of Peking Union Medical College Hospital (approval no.
S-K1198). Written informed consent to participate in the study was
obtained from the patient.
Patient consent for publication
Written informed consent for publication of clinical
details and/or clinical images was obtained from the patient.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
MSO
|
malignant struma ovarii
|
|
PTC
|
papillary thyroid cancer
|
|
RAI
|
radioiodine therapy
|
|
USO
|
unilateral salpingo-oophorectomy
|
References
|
1
|
Devaney K, Snyder R, Norris HJ and
Tavassoli FA: Proliferative and histologically malignant struma
ovarii: A clinicopathologic study of 54 cases. Int J Gynecol
Pathol. 12:333–343. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Outwater EK, Siegelman ES and Hunt JL:
Ovarian teratomas: Tumor types and imaging characteristics.
Radiographics. 21:475–490. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hanby A and Walker C: Pathology and
genetics: Tumours of the breast and female genital organs. WHO
classification of tumours series-volume IV. Lyon, France: IARC
Press. Breast Cancer Res. 6:1332004. View
Article : Google Scholar
|
|
4
|
Goffredo P, Sawka AM, Pura J, Adam MA,
Roman SA and Sosa JA: Malignant struma ovarii: A population-level
analysis of a large series of 68 patients. Thyroid. 25:211–215.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Li S, Yang T, Xiang Y, Li X, Zhang L and
Deng S: Clinical characteristics and survival outcomes of malignant
struma ovarii confined to the ovary. BMC Cancer. 21:3832021.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Li S, Yang T, Li X, Zhang L, Shi H, Cheng
N and Lang J: FIGO stage IV and age over 55 years as prognostic
predicators in patients with metastatic malignant struma ovarii.
Front Oncol. 10:5849172020. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shrimali RK, Shaikh G and Reed NS:
Malignant struma ovarii: The west of Scotland experience and review
of literature with focus on postoperative management. J Med Imaging
Radiat Oncol. 56:478–482. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shaco-Levy R, Peng RY, Snyder MJ, Osmond
GW, Veras E, Bean SM, Bentley RC and Robboy SJ: Malignant struma
ovarii: A blinded study of 86 cases assessing which histologic
features correlate with aggressive clinical behavior. Arch Pathol
Lab Med. 136:172–178. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Li S, Kong S, Wang X, Zhang X, Yin M and
Yang J: Survival outcomes and prognostic predictors in patients
with malignant struma ovarii. Front Med (Lausanne). 8:7746912021.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tessler FN, Middleton WD, Grant EG, Hoang
JK, Berland LL, Teefey SA, Cronan JJ, Beland MD, Desser TS, Frates
MC, et al: ACR thyroid imaging, reporting and data system
(TI-RADS): White paper of the ACR TI-RADS committee. J Am Coll
Radiol. 14:587–595. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Amin MB, Greene FL, Edge SB, Compton CC,
Gershenwald JE, Brookland RK, Meyer L, Gress DM, Byrd DR and
Winchester DP: The eighth edition AJCC cancer staging manual:
Continuing to build a bridge from a population-based to a more
‘personalized’ approach to cancer staging. CA Cancer J Clin.
67:93–99. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dardik RB, Dardik M, Westra W and Montz
FJ: Malignant struma ovarii: Two case reports and a review of the
literature. Gynecol Oncol. 73:447–451. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Janszen EW, van Doorn HC, Ewing PC, de
Krijger RR, de Wilt JH, Kam BL and de Herder WW: Malignant struma
ovarii: Good response after thyroidectomy and I ablation therapy.
Clin Med Oncol. 2:147–152. 2008.PubMed/NCBI
|
|
14
|
Marti JL, Clark VE, Harper H, Chhieng DC,
Sosa JA and Roman SA: Optimal surgical management of
well-differentiated thyroid cancer arising in struma ovarii: A
series of 4 patients and a review of 53 reported cases. Thyroid.
22:400–406. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Leite I, Cunha TM, Figueiredo JP and Félix
A: Papillary carcinoma arising in struma ovarii versus ovarian
metastasis from primary thyroid carcinoma: A case report and review
of the literature. J Radiol Case Rep. 7:24–33. 2013.PubMed/NCBI
|
|
16
|
Krishnamurthy A, Ramshankar V,
Vaidyalingam V and Majhi U: Synchronous papillary carcinoma thyroid
with malignant struma ovarii: A management dilemma. Indian J Nucl
Med. 28:243–245. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Leong A, Roche PJ, Paliouras M, Rochon L,
Trifiro M and Tamilia M: Coexistence of malignant struma ovarii and
cervical papillary thyroid carcinoma. J Clin Endocrinol Metab.
98:4599–4605. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Brusca N, Del Duca SC, Salvatori R,
D'Agostini A, Cannas P, Santaguida MG, Virili C, Bianchi L, Gargano
L and Centanni M: A case report of thyroid carcinoma confined to
ovary and concurrently occult in the thyroid: Is conservative
treatment always advised? Int J Endocrinol Metab.
13:e182202015.PubMed/NCBI
|
|
19
|
Ma D, Guseva NV, Dahmoush L and Robinson
RA: Struma ovarii with malignant transformation and germline KIT
mutation: A case report with review of the literature. Int J
Gynecol Pathol. 35:442–447. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Middelbeek RJW, O'Neill BT, Nishino M and
Pallotta JA: Concurrent intrathyroidal thyroid cancer and thyroid
cancer in struma ovarii: A case report and literature review. J
Endocr Soc. 1:396–400. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Gomes-Lima CJ, Nikiforov YE, Lee W and
Burman KD: Synchronous independent papillary thyroid carcinomas in
struma ovarii and the thyroid gland with different RAS mutations. J
Endocr Soc. 2:944–948. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tzelepis EG, Barengolts E, Garzon S,
Shulan J and Eisenberg Y: Unusual case of malignant struma ovarii
and cervical thyroid cancer preceded by ovarian teratoma: Case
report and review of the literature. Case Rep Endocrinol.
2019:79641262019.PubMed/NCBI
|
|
23
|
Donato S, Simões H and Leite V: Malignant
struma ovarii with concurrent thyroid cancer: Outcomes during and
after pregnancy. Eur Thyroid J. 10:523–527. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Seo GT, Minkowitz J, Kapustin DA, Fan J,
Minkowitz G, Minkowitz M, Dowling E, Matloob A, Asti D, Dhar M, et
al: Synchronous thyroid cancer and malignant struma ovarii:
Concordant mutations and microRNA profile, discordant loss of
heterozygosity loci. Diagn Pathol. 18:472023. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Boyd JC, Williams BA, Rigby MH, Kieser K,
Offman S, Shirsat H, Trites JRB, Taylor SM and Hart RD: Malignant
Struma ovarii in a 30-year old nulliparous patient. Thyroid Res.
10:32017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lim ST, Jeong HJ, Chung MJ, Yim CY and
Sohn MH: Malignant struma ovarii demonstrated on post-therapy
radioiodine scan after total thyroidectomy for papillary thyroid
cancer. Clin Nucl Med. 33:429–431. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kitahara CM and Sosa JA: The changing
incidence of thyroid cancer. Nat Rev Endocrinol. 12:646–653. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Poli R, Scatolini M, Grosso E, Maletta F,
Gallo M, Liscia D, Nelva A, Cesario F, Forte G, Metovic J, et al:
Malignant struma ovarii: Next-generation sequencing of six cases
revealed Nras, Braf, and Jak3 mutations. Endocrine. 71:216–224.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Moon S, Song YS, Kim YA, Lim JA, Cho SW,
Moon JH, Hahn S, Park DJ and Park YJ: Effects of coexistent BRAF
V600E and TERT promoter mutations on poor clinical
outcomes in papillary thyroid cancer: A meta-analysis. Thyroid.
27:651–660. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Siegel MR, Wolsky RJ, Alvarez EA and
Mengesha BM: Struma ovarii with atypical features and synchronous
primary thyroid cancer: A case report and review of the literature.
Arch Gynecol Obstet. 300:1693–1707. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ayhan S, Kilic F, Ersak B, Aytekin O, Akar
S, Turkmen O, Akgul G, Toyran A, Turan T and Kimyon Comert G:
Malignant struma ovarii: From case to analysis. J Obstet Gynaecol
Res. 47:3339–3351. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Filetti S, Durante C, Hartl D, Leboulleux
S, Locati LD, Newbold K, Papotti MG, Berruti A, ESMO Guidelines
Committee and Electronic address: simpleclinicalguidelines@esmo.org:
Thyroid cancer: ESMO clinical practice guidelines for diagnosis,
treatment and follow-up. Ann Oncol. 30:1856–1883. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Yassa L, Sadow P and Marqusee E: Malignant
struma ovarii. Nat Clin Pract Endocrinol Metab. 4:469–472. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Prat J: FIGO's staging classification for
cancer of the ovary, fallopian tube, and peritoneum: abridged
republication. J Gynecol Oncol. 26:87–89. 2015. View Article : Google Scholar : PubMed/NCBI
|