Tumors that occur at different sites and/or belong
to different histological or morphological groups are considered to
be a multi-primary cancer (1). A
study in 1921 reported that 4.7% of 3,000 patients with malignant
tumors had multiple tumors (2).
Epidemiological studies have reported that the frequency of
multiple primary cancer was 2–17% in 2014 (3–7). Weir
et al (5) reported that
following Surveillance, Epidemiology and End Results guidelines
(8), the incidence of multiple
primary cancer was 19.7% in patients with colon cancer [16.9% as
per International Association of Cancer Registries (IACR)
guidelines (9)] and 21% in those
with lung cancer (19.9% according to the IACR guidelines). The
epidemiological factors contributing to occurrence of multiple
primary cancer include host factors, such as genetic factors,
hormones and tumor history, lifestyle factors, such as smoking and
alcohol consumption, and environmental factors, such as occupation,
pathogen exposure and geographical location (10). Among these, genetic factors have
attracted increasing attention from researchers (3,11–16).
It is estimated that between 5 and 10% of all breast cancer cases
and ~20% of ovarian cancer cases are caused by an inherited
pathogenic variant associated with hereditary breast and ovarian
cancer syndrome (17–21). First- and second-degree relatives
and first cousins have a 12.5–50.0% probability of inheriting the
respective cancer predisposition variants (22,23).
Therefore, timely identification of genetic variants decreases
morbidity and mortality in individuals with inherited cancer risk
and facilitates targeted therapy for patients with cancer (24). Table
I provides a brief overview of germline mutations in patients
with cancer from larger sequencing studies (25–32).
Genetic testing serves as a robust and efficient auxiliary
examination tool that provides information on molecular subtypes
and therapeutic targets and aids in the development of potential
treatment strategies and selection of appropriate drugs (33).
The 5-year survival rate of patients with 27 common
types(including pancreas to testis) of cancer in the UK ranges from
7 to 88% (34). Depending on the
type of combined tumor, survival times vary among patients with
different recurring types of cancer, especially those with
hematological disease (8), who
exhibit rapid progression, high degree of malignancy, difficulty in
treatment and a low survival rate. A number of patients with
multiple primary tumors of hematological disease) carry germline
driver gene mutations (CEBPA OR TP53 and so on) associated with a
poor prognosis (35). Previous
studies (36,37) have shown that a small number of
patients carrying two germline mutations, ERCC excision repair 6,
chromatin remodeling factor (ERCC6) and LYL1 basic
helix-loop-helix family member (LYL1), develop
non-small-cell lung cancer (NSCLC), early T cell precursor acute
lymphoblastic leukemia (ETP-ALL) and SCLC. The present study
describes a patient with ERCC6(+) and LYL1(+)
mutations with triple primary tumors.
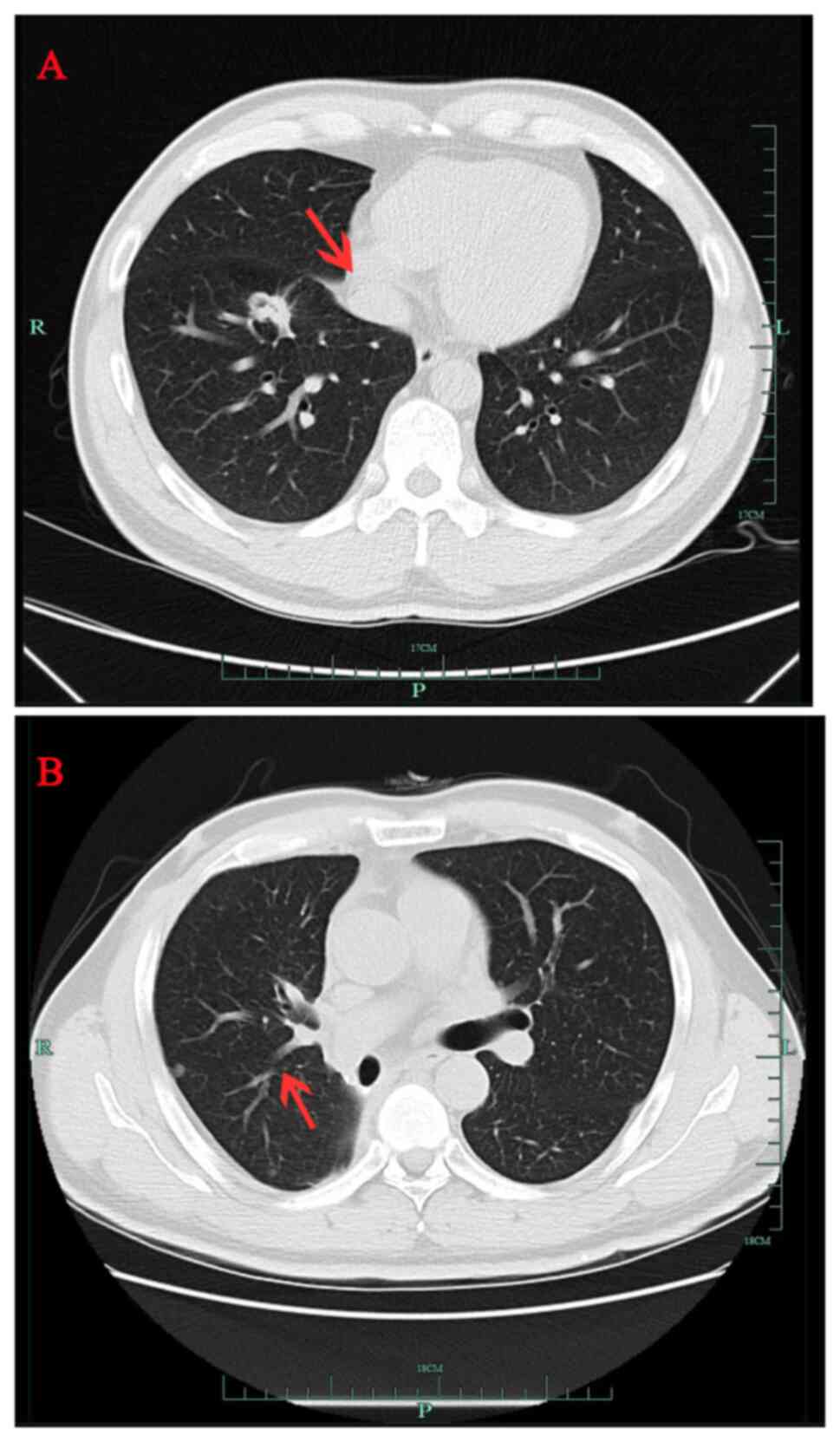
A 40-year-old male patient (healthy and non-smoker)
was found to have a right lower lung space during an annual routine
checkup in September 2016 (Fig. 1A)
at The First Affiliated Hospital Zhejiang University School of
Medicine (Hangzhou, China). The patient's father, who smoked for 40
years, had also been diagnosed with lung cancer but refused genetic
testing. Radical resection of the lower right lung cancer was
performed in October 2016. The pathological diagnosis was
adenocarcinoma of the lower right lung (T1N2M0, stage IIIA)
(38). Postoperative concurrent
chemoradiotherapy included four cycles of pemetrexed + platinum,
with a total radiotherapy dose of 50 Gy in 25 fractions (50 Gy/25
f). In March 2018, routine chest computed tomography (CT) scan
demonstrated a new nodule near the pleura in the middle lobe of the
right lung (Fig. 1B), which
indicated local recurrence of adenocarcinoma. Gefitinib (250 mg,
once daily) was administered orally and the nodules subsequently
disappeared by July 2018, as confirmed by chest CT scan (data not
shown).
In September 2018, at the Tongde Hospital of
Zhejiang Province (Hangzhou, China) for the first presentation, the
patient developed submental lymph node enlargement, which was
diagnosed as ETP-ALL based on lymph node biopsy and bone marrow
tests [CD7(++), CD1α(−), CD8(−), CD5(dim), CD34(+), CD2(+), cyCD3
(weakly positive) and CD4(+). Gefitinib was discontinued and
hyper-cyclophosphamide, vindesine, liposomal doxorubicin and
dexamethasone/methotrexate and cytarabine was initiated (Table II); however, this proved
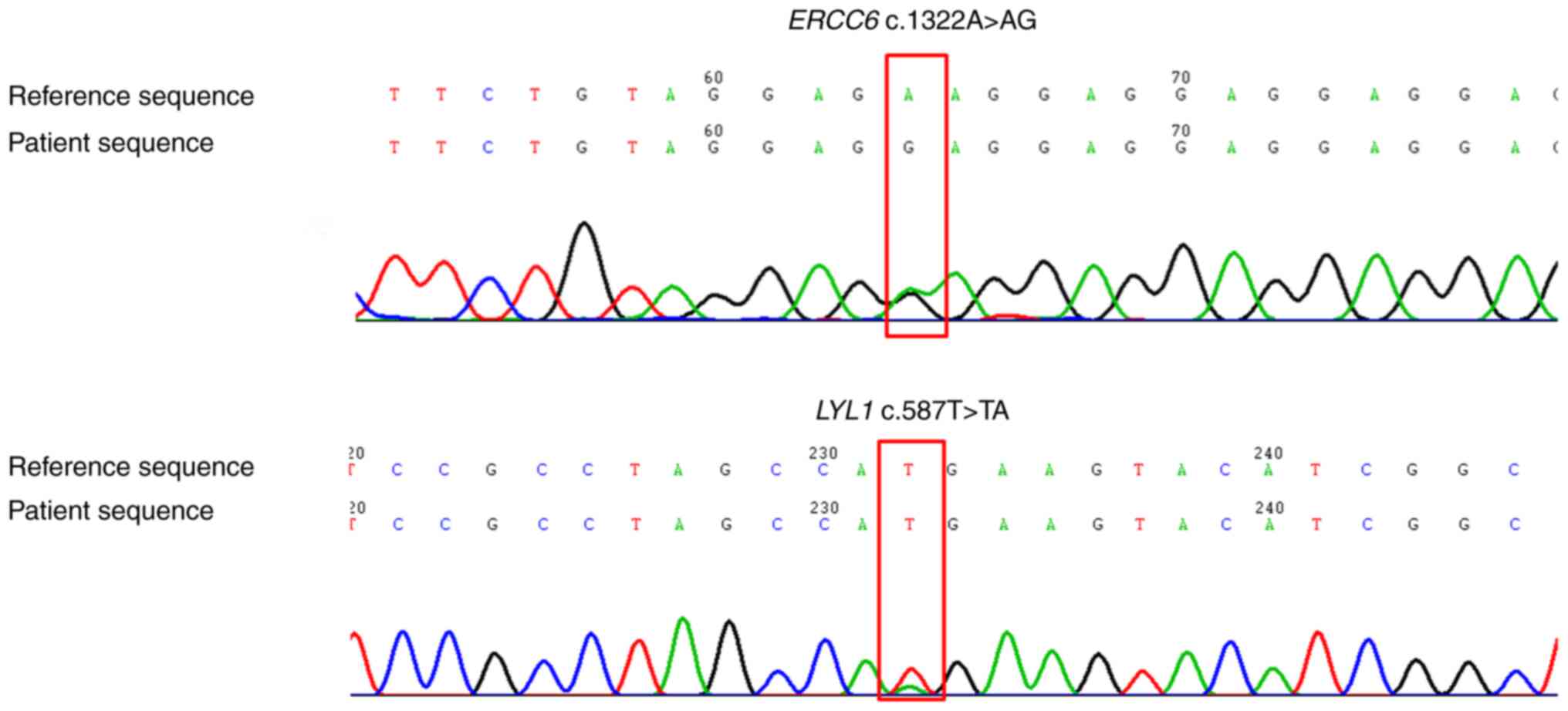
ineffective. Germline gene sequencing of skin tissue demonstrated
ERCC6 variant c.1322A>G and LYL1 variant
c.587T>A (Fig. 2).
The primers were as follows: ERCC6-E5 forward (F),
5′-GAGGAAGATGACGAGGTGGA-3′ and reverse (R),
5′-GGCTGCAGAAATCCAACCTC-3′ and LYL1-E4 F,
5′-CAGACCCATGAGTACACCCA-3′ and R, 5′-CTGACGTCTTCACTGGTCCT-3′. The
high-throughput sequencing was Aligent SureSelect. The method used
to verify the quality/integrity of the processed samples was A 2200
bioanalyzer for genomic DNA or RNA. The type of sequencing was 300
bp for length and paired end for direction of sequencing. The
loading concentration of the final library, including how
concentrations were measured:5 pM for DNA sequencing). i) The
patient received two courses of venetoclax combined with
granulocyte colony-stimulating factor, cytarabine and aclacinomycin
chemotherapy (Table II). February
2019 bone marrow reexamination indicated complete remission (data
not shown).
Modified busulfan-cyclophosphamide pretreatment
(Cytarabine 7.3 g-10d,-9d; busulfan 54 mg q6h8d,-7d,-6d;
cyclophosphamide 3.3 g-5d,-4d; oral semustine 450 mg-3d.
Cytarabine-busulfan and cyclophosphamide intravenous infusion.
Semustine was Oral administration, the purpose of this were to
fully eliminate or suppress the patient's immune system to prevent
graft rejection; reduce the number of tumor cells to a minimum;
remove the patient's hematopoietic stem cells from the bone marrow
niche to provide sufficient space for the engrafted donor
hematopoietic stem cells to support proliferation and
differentiation. ii) was performed in March 2019. Haploidentical
hematopoietic stem cell transplantation was performed following
stem cell donations from the patient's son (March 2019). During
transplantation, anti-thymocyte globulin (ATG; total dose 700 mg),
cyclosporin A and short-course methotrexate(cyclosporin A 75 mg
q12h qd Intravenous infusion; methotrexate 10mg +1d,+3d,+6,+11d,
were Intravenous infusion) were administered on days 1, 3, 5 and 11
following transplantation, to prevent acute graft vs. host disease.
After ATG was administered, leukocyte count (Table III) was monitored. In April 2019,
bone marrow examination showed that the ETP-ALL was in remission,
the short tandem repeat was of the complete donor type and the
right lung lesion was smaller, as observed through CT scan (data
not shown). During the cyclosporin anti-rejection treatment,
routine Positron Emission Tomography-CT examination indicated
multiple small nodules in both lungs, which prompted clinical
consideration of lung adenocarcinoma recurrence. Gefitinib (250 mg,
once daily) targeted therapy was re-administered for 10 months to
alleviate the increase in the number of lung nodules.-we decided to
switch from gefitinib to osimertinib (80 mg/d). The number of
nodules in both lungs decreased following this treatment.
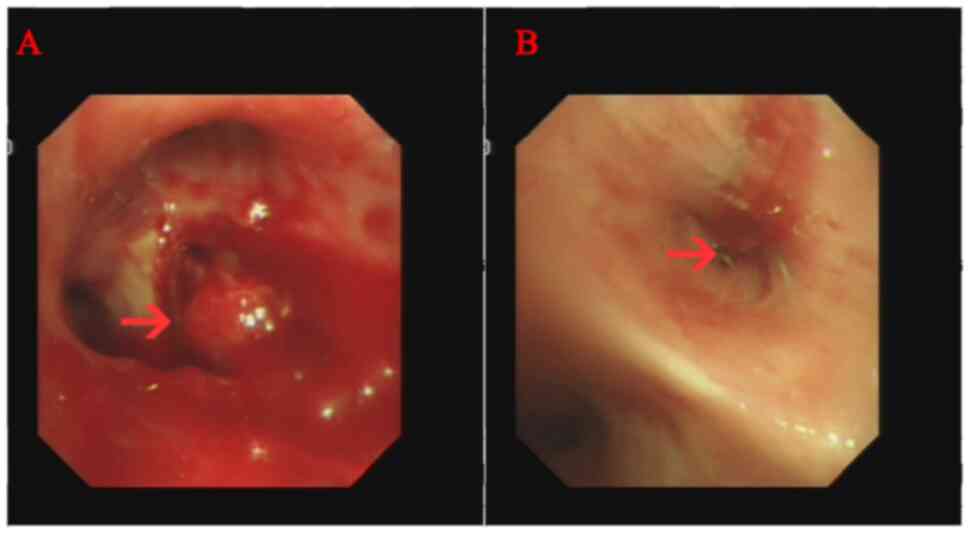
Sudden hemoptysis occurred in November 2020 and a
new obstruction in the lumen was noted following bronchoscopy
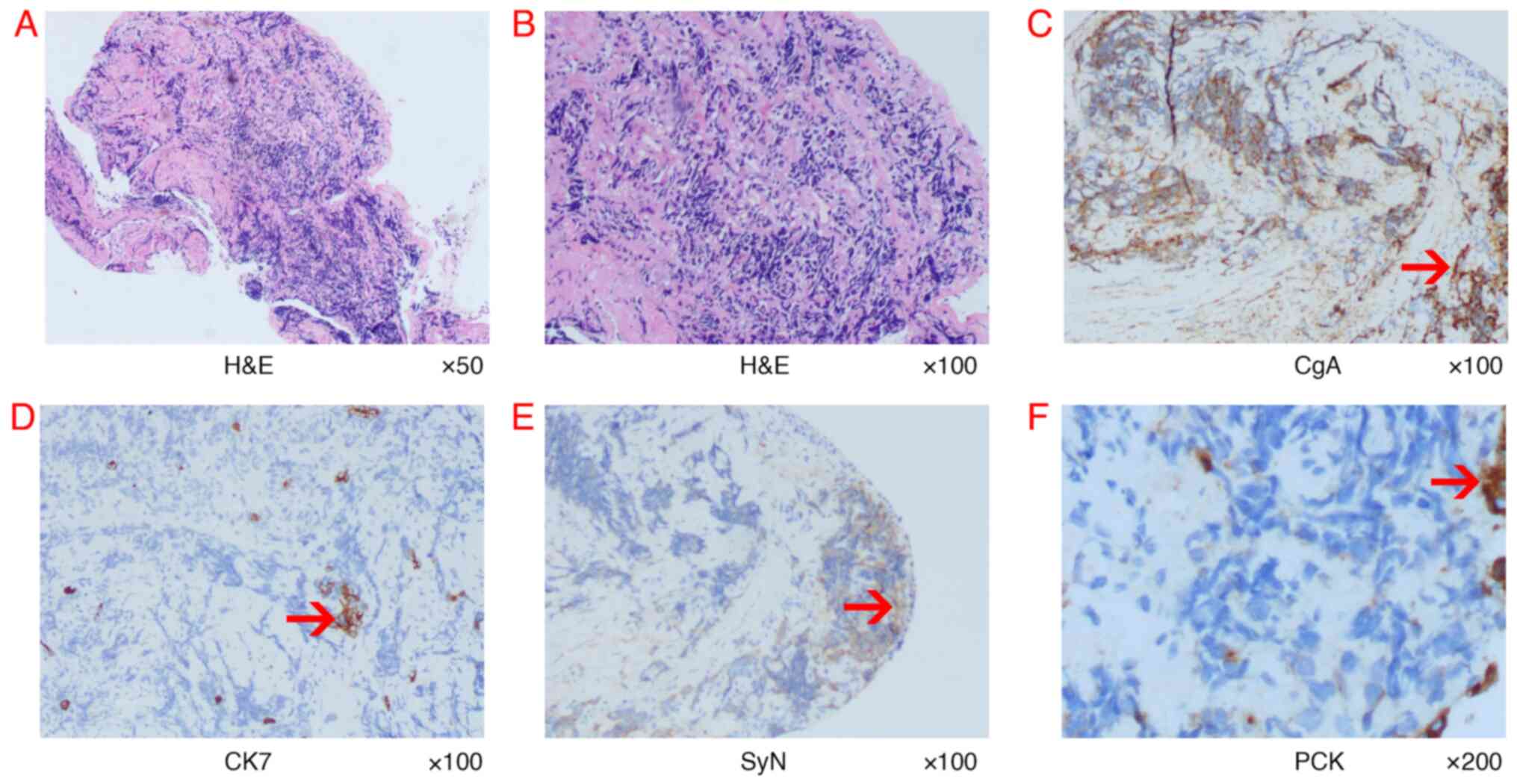
(Fig. 3). Pathological examination
of brush cytology smear under a microscope demonstrated SCLC
(Fig. 4). Immunohistochemistry was
negative for CK7 and positive for pancytokeratin (PCK),
chromogranin A) and SyN(Synaptophysin). A marked decrease in
foreign body count was observed after combining chemoradiotherapy
with osimertinib treatment through chest CT (data not shown). A
timeline of the three types of cancer diagnosed is presented in
Table IV. No metastases in the
skull, bones or gastrointestinal area were observed during
treatment. In August 2022, the patient succumbed to progressive
lung cancer and no autopsy was performed.
Germline gene mutations implicated in development of
multiple primary tumors warrant investigation. Paired tumor
germline genomic analyses have identified at least one pathogenic
or potentially pathogenic germline variant of cancer susceptibility
genes in 8–18% of patients with cancer (39–41).
Oncologists increasingly recommend genetic testing for pathogenic
germline variants in patients with cancer to advise on individual
risk of developing cancer and the likelihood of family members
carrying the same genetic predisposition to cancer (42,43).
For example, inactivating mutations in the cancer suppressor genes
BRCA1 and BRCA2 predict response to drugs, such as
PARP inhibitors docetaxel and cisplatin, and are associated with
increased genetic susceptibility (44).
In addition to driver genes, radiotherapy and
chemotherapy are considered risk factors for recurring types of
cancer (62). In a previous study,
four patients with heterochronous manifestations received
chemotherapy and/or radiation therapy for lung cancer before
developing AML (63). In all four
patients, lung cancer preceded AML by 5–10 years and the patients
died within 2 months of being diagnosed with AML. In the present
case, the patient initially developed NSCLC and ETP-ALL occurred
within 2 years of treatment with pemetrexed combined with cisplatin
chemotherapy and radiotherapy, which progressed rapidly. The
patient harbored the driver genes ERCC6(+) and
LYL1(+), which promoted the occurrence of acute leukemia
following radiotherapy and chemotherapy. Later, owing to the high
degree of malignancy of ETP-ALL, the patient received allogeneic
hematopoietic stem cell transplantation, requiring strong
immunosuppression to prevent rejection. These anti-rejection drugs
act by removing T cells, resulting in T cell exhaustion (42). According to Chan et al
(64), a recurrent SCLC
subpopulation may exist in an immunosuppressed tumor
microenvironment characterized by exhausted CD8+ T cells, as
described by Guo et al (65). Research has shown that the genetic
profile of activated tumor regulatory T cells is associated with a
poor prognosis in lung adenocarcinoma: Chan et al (64) has shown that SCLC exhibits increased
immune isolation and decreased immune infiltration compared with
lung adenocarcinoma. Here, 1.5 years after transplantation, the
patient developed SCLC, which was possibly linked to use of
immunosuppressants such as ATG.
In the present study, the patients father's
long-term smoking may have exposed the patient to tobacco smoke for
numerous years and may represent a carcinogenic exposure factor.
Epidemiological studies of exposure to environmental tobacco smoke,
along with the detection of tobacco-specific carcinogens in blood
and urine of non-smokers in such environments, have indicated that
long-term inhalation of tobacco smoke is a cause of lung cancer
(66,67) Subsequent studies (68–70)
have similarly confirmed that exposure to environmental tobacco
smoke significantly increases risk of lung cancer for
non-smokers.
The National Comprehensive Cancer Network guidelines
recommend genetic screening for breast, ovarian, pancreatic, lung,
colorectal and prostate cancer based on previous studies (71). Genetic screening is performed
according to American College of Medical Genetics and Genomics,
which offers the advantage of early identification of tumors and
effective treatment (72,73). For example (74,75),
positive screening of commonly inherited breast cancer gene
BRCA1/2 mutations can prompt appropriate treatment measures
such as surgery or enhanced monitoring of patients who refuse
surgery. However, screening faces a number of challenges, such as
cost, invasiveness of the procedure. Therefore, in clinical
decision-making, patients should receive information on the
advantages and disadvantages, with their preferences respected.
Management of multiple primary tumors poses
challenges, with implications for overall survival and quality of
life, such as decreasing infections, avoiding transfusions and
shorter hospital stays. Therefore, multidisciplinary collaboration
to develop a personalized treatment plan is essential. In the
present case, when the ETP-ALL diagnosis for the second tumor was
made, multiple multidisciplinary discussions with oncology,
respiratory and radiotherapy departments were conducted regarding
the choice of chemotherapy regimen for ETP-ALL and the decision on
whether to proceed with a transplant. The patient and their family
were also consulted. Finally, a chemotherapy regimen for AML that
combined venetoclax with cytarabine, aclarubicin and G-CSF was
chosen, which achieved complete remission. Subsequently, one
consolidation cycle was administered, followed by a related donor
allogeneic hematopoietic stem cell transplant. Treatment plans for
lung cancer post-transplant due to emergence of the third SCLC
tumor were similarly coordinated with oncology, respiratory and
radiotherapy specialists.
The present study had several strengths, such as
genetic testing of germline genes upon development of a second
tumor, successful management of ETP-ALL with hematopoietic stem
cell transplantation and sustained remission. However, there were
also limitations, which included the absence of sample testing from
the patient's father, inability to verify the genetic pattern and
the need for case reports.
In summary, the present study described a patient
with NSCLC harboring mutations in the germline genes ERCC6
and LYL1 who developed ETP-ALL and SCLC shortly after
remission. Considering the rapid progression of recurring types of
cancer, clinicians should prioritize screening for germline
mutations in patients and their family members to facilitate early
diagnosis, treatment and prognosis assessment.
Not applicable.
The present study was supported by Zhejiang Traditional Chinese
Medicine Administration (grant no. 2021ZQ020) and Key Specialties
of Zhejiang Administration of Traditional Chinese Medicine in the
13th Five-year Plan.
The sequencing data generated in the present study
may be found in the National Centre of Biotechnology database under
accession number PRJNA1146555 or at the following URL: https://dataview.ncbi.nlm.nih.gov/?archive=bioproject.
XFX conceived the study and revised the manuscript.
HFJ interpreted the radiological findings. YXJ and MXH interpreted
the pathological findings. HYW interpreted the genetic findings and
wrote the manuscript. XFX and HYW confirm the authenticity of all
the raw data All authors have read and approved the final
manuscript.
The present study was approved by the Ethics Review
Committee of Tongde Hospital of Zhejiang Province (approval no.
106-JY.2022; Hangzhou, China).
Written informed consent was obtained from the
patient for the publication of this report and any accompanying
images.
The authors declare that they have no competing
interests.
|
1
|
Shah SA, Riaz U, Zahoor I, Jalil A and
Zubair M: Carcinoma multiplex. J Coll Physicians Surg Pak.
23:290–292. 2013.PubMed/NCBI
|
|
2
|
Owen LJ: Multiple malignant neoplasms.
JAMA. 76:1329–1333. 1921. View Article : Google Scholar
|
|
3
|
Coyte A, Morrison DS and McLoone P: Second
primary cancer risk-The impact of applying different definitions of
multiple primaries: Results from a retrospective population-based
cancer registry study. BMC Cancer. 14:1–11. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Buiatti E, Crocetti E, Acciai S, Gafà L,
Falcini F, Milandri C and La Rosa M: Incidence of second primary
cancers in three Italian population-based cancer registries. Eur J
Cancer. 33:1829–1834. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Weir HK, Johnson CJ and Thompson TD: The
effect of multiple primary rules on population-based cancer
survival. Cancer Causes Control. 24:1231–1242. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rosso S, De Angelis R, Ciccolallo L,
Carrani E, Soerjomataram I, Grande E, Zigon G and Brenner H;
Eurocare Working Group, : Multiple tumours in survival estimates.
Eur J Cancer. 45:1080–1094. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Second primary cancers, . Victoria
Karaholios E, English D, Thursfield V and Simpson J:
2009.http://www.cancervic.org.au/downloads/cec/Second-Primary-Cancers.pdfAugust.
2009
|
|
8
|
Tsikitis VL, Wertheim BC and Guerrero MA:
Trends of incidence and survival of gastrointestinal neuroendocrine
tumors in the United States: A seer analysis. J Cancer. 3:2922012.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lynch SM, Heeran AB, Burke C, Lynam-Lennon
N, Eustace AJ, Dean K, Robson T, Rahman A and Marcone S: Precision
oncology, artificial intelligence, and novel therapeutic
advancements in the diagnosis, prevention, and treatment of cancer:
Highlights from the 59th Irish Association for Cancer Research
(IACR) Annual conference. Cancers (Basel). 16:19892024. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Vogt A, Schmid S, Heinimann K, Frick H,
Herrmann C, Cerny T and Omlin A: Multiple primary tumours:
Challenges and approaches, a review. ESMO Open. 2:e0001722017.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wood ME, Vogel V, Ng A, Foxhall L, Goodwin
P and Travis LB: Second malignant neoplasms: Assessment and
strategies for risk reduction. J Clin Oncol. 30:3734–3745. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bajdik CD, Abanto ZU, Spinelli JJ,
Brooks-Wilson A and Gallagher RP: Identifying related cancer types
based on their incidence among people with multiple cancers. Emerg
Themes Epidemiol. 3:172006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Gaskin HS, Hardy RE and Fletcher RL:
Multiple primary malignancies in black patients. J Natl Med Assoc.
73:1065–1068. 1981.PubMed/NCBI
|
|
14
|
Donin N, Filson C, Drakaki A, Tan HJ,
Castillo A, Kwan L, Litwin M and Chamie K: Risk of second primary
malignancies among cancer survivors in the United States, 1992
through 2008. Cancer. 122:3075–3086. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
AIRTUM Working Group, . Italian cancer
figures, report 2010: Cancer prevalence in Italy. Patients living
with cancer, long-term survivors and cured patients = Epidemiol
Prev. 34 (5–6 Suppl 2):S1–S188. 2010.(In English, Italian).
PubMed/NCBI
|
|
16
|
Hauben EI, Arends J, Vandenbroucke JP, van
Asperen CJ, Van Marck E and Hogendoorn PC: Multiple primary
malignancies in osteosarcoma patients. Incidence and predictive
value of osteosarcoma subtype for cancer syndromes related with
osteosarcoma. Eur J Hum Genet. 11:611–618. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hu C, Hart SN, Gnanaolivu R, Huang H, Lee
KY, Na J, Gao C, Lilyquist J, Yadav S, Boddicker NJ, et al: A
population-based study of genes previously implicated in breast
cancer. N Engl J Med. 384:440–451. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Chubb D, Broderick P, Frampton M,
Kinnersley B, Sherborne A, Penegar S, Lloyd A, Ma YP, Dobbins SE
and Houlston RS: Genetic diagnosis of high-penetrance
susceptibility for colorectal cancer (CRC) is achievable for a high
proportion of familial CRC by exome sequencing. J Clin Oncol.
33:426–432. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Walsh T, Casadei S, Lee MK, Pennil CC,
Nord AS, Thornton AM, Roeb W, Agnew KJ, Stray SM, Wickramanayake A,
et al: Mutations in 12 genes for inherited ovarian, fallopian tube,
and peritoneal carcinoma identified by massively parallel
sequencing. Proc Natl Acad Sci USA. 108:18032–18037. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Couch FJ, Nathanson KL and Offit K: Two
decades after BRCA: Setting paradigms in personalized cancer care
and prevention. Science. 343:1466–1470. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Mavaddat N, Peock S, Frost D, Ellis S,
Platte R, Fineberg E, Evans DG, Izatt L, Eeles RA, Adlard J, et al:
Cancer risks for BRCA1 and BRCA2 mutation carriers: Results from
prospective analysis of embrace. J Natl Cancer Inst. 105:812–822.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Greenberg S, Buys SS, Edwards SL, Espinel
W, Fraser A, Gammon A, Hafen B, Herget KA, Kohlmann W, Roundy C, et
al: Population prevalence of individuals meeting criteria for
hereditary breast and ovarian cancer testing. Cancer Med.
8:6789–6798. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Grosse SD, Rogowski WH, Ross LF, Cornel
MC, Dondorp WJ and Khoury MJ: Population screening for genetic
disorders in the 21st century: Evidence, economics, and ethics.
Public Health Genom. 13:106–115. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Schienda J and Stopfer J: Cancer genetic
counseling-current practice and future challenges. Cold Spring Harb
Perspect Med. 10:a0365412020. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Deng M, Chen HH, Zhu X, Luo M, Zhang K, Xu
CJ, Hu KM, Cheng P, Zhou JJ, Zheng S and Chen YD: Prevalence and
clinical outcomes of germline mutations in BRCA1/2 and PALB2 genes
in 2769 unselected breast cancer patients in China. Int J Cancer.
145:1517–1528. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Malkin D, Li FP, Strong LC, Fraumeni JF
Jr, Nelson CE, Kim DH, Kassel J, Gryka MA, Bischoff FZ, Tainsky MA,
et al: Germ line p53 mutations in a familial syndrome of breast
cancer, sarcomas, and other neoplasms. Science. 250:1233–1238.
1990. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Clark SK: Management of genetically
determined colorectal cancer. Surgeon. 17:165–171. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Aghabozorgi AS, Ebrahimi R, Bahiraee A,
Tehrani SS, Nabizadeh F, Setayesh L, Jafarzadeh-Esfehani R, Ferns
GA, Avan A and Rashidi Z: The genetic factors associated with Wnt
signaling pathway in colorectal cancer. Life Sci. 256:1180062020.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Short E and Sampson J: The role of
inherited genetic variants in colorectal polyposis syndromes. Adv
Genet. 103:183–217. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Sekine Y, Iwasaki Y, Hakozaki N, Endo M,
Kamatani Y, Matsuda K, Murakami Y, Sano T, Akamatsu S, Kobayashi T,
et al: Prevalence and risk estimation of cancer-predisposing genes
for upper urinary tract urothelial carcinoma in Japanese. Jpn J
Clin Oncol. 52:1441–1445. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2020. CA Cancer J Clin. 70:7–30. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Baysal BE, Willett-Brozick JE, Lawrence
EC, Drovdlic CM, Savul SA, McLeod DR, Yee HA, Brackmann DE,
Slattery WH III, Myers EN, et al: Prevalence of SDHB, SDHC, and
SDHD germline mutations in clinic patients with head and neck
paragangliomas. J Med Genet. 39:178–183. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Urbina-Jara LK, Rojas-Martinez A,
Martinez-Ledesma E, Aguilar D, Villarreal-Garza C and Ortiz-Lopez
R: Landscape of germline mutations in DNA repair genes for breast
cancer in Latin America: Opportunities for PARP-like inhibitors and
immunotherapy. Genes. 10:7862019. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Cancer survival rates, 2023, .
Nuffieldtrust. https://www.nuffieldtrust.org.uk/resource/cancer-survival-ratesJune
27–2023
|
|
35
|
Zhao Z, Sun K, Yan T, Wei R and Guo W:
Multiple primary tumors: A case report and review of the
literature. BMC Musculoskelet Disord. 21:3942020. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
de Pooter RF, Dias S, Chowdhury M, Bartom
ET, Okoreeh MK, Sigvardsson M and Kee BL: Cutting Edge:
Lymphomyeloid-primed progenitor cell fates are controlled by the
transcription factor tal1. J Immunol. 202:2837–2842. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Ma H, Hu Z, Wang H, Jin G, Wang Y, Sun W,
Chen D, Tian T, Jin L, Wei Q, et al: ERCC6/CSB gene polymorphisms
and lung cancer risk. Cancer Lett. 273:172–176. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Rami-Porta R, Bolejack V, Crowley J, Ball
D, Kim J, Lyons G, Rice T, Suzuki K, Thomas CF Jr, Travis WD, et
al: The lASLC lung cancer staging project: Proposals for the
Revisions of the T Descriptors in the Forthcoming Eighth edition of
the TNM classification for lung cancer. J Thorac Oncol.
10:990–1003. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Mandelker D, Zhang L, Kemel Y, Stadler ZK,
Joseph V, Zehir A, Pradhan N, Arnold A, Walsh MF, Li Y, et al:
Mutation detection in patients with advanced cancer by universal
sequencing of cancer-related genes in tumor and normal DNA vs
guideline-based germline testing. JAMA. 318:825–835. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Zhang J, Walsh MF, Wu G, Edmonson MN,
Gruber TA, Easton J, Hedges D, Ma X, Zhou X, Yergeau DA, et al:
Germline mutations in predisposition genes in pediatric cancer. N
Engl J Med. 373:2336–2346. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Schrader KA, Cheng DT, Joseph V, Prasad M,
Walsh M, Zehir A, Ni A, Thomas T, Benayed R, Ashraf A, et al:
Germline variants in targeted tumor sequencing using matched normal
DNA. JAMA Oncol. 2:104–111. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Domchek SM: Germline genetic testing for
breast cancer: Which patients? What genes? Genet Med. 22:698–700.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Konstantinopoulos PA, Norquist B,
Lacchetti C, Armstrong D, Grisham RN, Goodfellow PJ, Kohn EC,
Levine DA, Liu JF, Lu KH, et al: Germline and somatic tumor testing
in epithelial ovarian cancer: ASCO guideline. J Clin Oncol.
38:1222–1245. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Chakravarty D and Solit DB: Clinical
cancer genomic profiling. Nat Rev Genet. 22:483–501. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Troelstra C, van Gool A, de Wit J,
Vermeulen W, Bootsma D and Hoeijmakers JH: ERCC6, a member of a
subfamily of putative helicases, is involved in Cockayne's syndrome
and preferential repair of active genes. Cell. 71:939–953. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Meira LB, Graham JM Jr, Greenberg CR,
Busch DB, Doughty AT, Ziffer DW, Coleman DM, Savre-Train I and
Friedberg EC: Manitoba aboriginal kindred with original
Cerebro-Oculo-Facio-Skeletal syndrome has a mutation in the
Cockayne syndrome group B (CSB) gene. Am J Hum Genet. 66:1221–1228.
2000. View
Article : Google Scholar : PubMed/NCBI
|
|
47
|
Berndt SI, Platz EA, Fallin MD, Thuita LW,
Hoffman SC and Helzlsouer KJ: Genetic variation in the nucleotide
excision repair pathway and colorectal cancer risk. Cancer
Epidemiol Biomarkers Prev. 15:2263–2269. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Chiu CF, Tsai MH, Tseng HC, Wang CL, Tsai
FJ, Lin CC and Bau DT: A novel single nucleotide polymorphism in
ERCC6 gene is associated with oral cancer susceptibility in
Taiwanese patients. Oral Oncol. 44:582–586. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Lin Z, Zhang X, Tuo J, Guo Y, Green B,
Chan CC, Tan W, Huang Y, Ling W, Kadlubar FF, et al: A variant of
the Cockayne syndrome B gene ERCC6 confers risk of lung cancer. Hum
Mutat. 29:113–122. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Gu J, Zhao H, Dinney CP, Zhu Y, Leibovici
D, Bermejo CE, Grossman HB and Wu X: Nucleotide excision repair
gene polymorphisms and recurrence after treatment for superficial
bladder cancer. Clin Cancer Res. 11:1408–1415. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Ma H, Hu Z, Wang H, Jin G, Wang Y, Sun W,
Chen D, Tian T, Jin L, Wei Q, et al: ERCC6/CSB gene polymorphisms
and lung cancer risk. Cancer Lett. 273:172–176. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Wilson NK, Foster SD, Wang X, Knezevic K,
Schütte J, Kaimakis P, Chilarska PM, Kinston S, Ouwehand WH,
Dzierzak E, et al: Combinatorial transcriptional control in blood
stem/progenitor cells: Genome-wide analysis of ten major
transcriptional regulators. Cell Stem Cell. 7:532–544. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Souroullas GP, Salmon JM, Sablitzky F,
Curtis DJ and Goodell MA: Adult hematopoietic stem and progenitor
cells require either Lyl1 or Scl for survival. Cell Stem Cell.
4:180–186. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Mellentin JD, Smith SD and Cleary ML:
Lyl-1, a novel gene altered by chromosomal translocation in T cell
leukemia, codes for a protein with a helix-loop-helix DNA binding
motif. Cell. 58:77–83. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Meng YS, Khoury H, Dick JE and Minden MD:
Oncogenic potential of the transcription factor LYL1 in acute
myeloblastic leukemia. Leukemia. 19:1941–1947. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Natkunam Y, Zhao S, Mason DY, Chen J,
Taidi B, Jones M, Hammer AS, Hamilton Dutoit S, Lossos IS and Levy
R: The oncoprotein LMO2 is expressed in normal germinal-center B
cells and in human B-cell lymphomas. Blood. 109:1636–1642. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Kwiatkowski N, Zhang T, Rahl PB, Abraham
BJ, Reddy J, Ficarro SB, Dastur A, Amzallag A, Ramaswamy S, Tesar
B, et al: Targeting transcription regulation in cancer with a
covalent CDK7 inhibitor. Nature. 511:616–620. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Sang X, Zhang Y, Fang F, Gao L, Tao Y, Li
X, Zhang Z, Wang J, Tian Y, Li Z, et al: BRD4 Inhibitor GNE-987
exerts anticancer effects by targeting super-enhancer-related gene
LYL1 in acute myeloid leukemia. J Immunol Res. 2022:79124842022.
View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Miyamoto A, Cui X, Naumovski L and Cleary
ML: Helix-loop-helix proteins LYL1 and E2a form heterodimeric
complexes with distinctive DNA-binding properties in hematolymphoid
cells. Mol Cell Biol. 16:2394–2401. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Sanda T, Lawton LN, Barrasa MI, Fan ZP,
Kohlhammer H, Gutierrez A, Ma W, Tatarek J, Ahn Y, Kelliher MA, et
al: Core transcriptional regulatory circuit controlled by the TAL1
complex in human T cell acute lymphoblastic leukemia. Cancer Cell.
22:209–221. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Thoms JAI, Truong P, Subramanian S,
Knezevic K, Harvey G, Huang Y, Seneviratne JA, Carter DR, Joshi S,
Skhinas J, et al: Disruption of a GATA2-TAL1-ERG regulatory circuit
promotes erythroid transition in healthy and leukemic stem cells.
Blood. 138:1441–1455. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Griesinger F, Metz M, Trümper L, Schulz T
and Haase D: Secondary leukaemia after cure for locally advanced
NSCLC: Alkylating type secondary leukaemia after induction therapy
with docetaxel and carboplatin for NSCLC IIIB. Lung Cancer.
44:261–265. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Varadarajan R, Ford L, Sait SNJ, Block AW,
Barcos M, Wallace PK, Ramnath N, Wang ES and Wetzler M:
Metachronous and synchronous presentation of acute myeloid leukemia
and lung cancer. Leuk Res. 33:1208–1211. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Chan JM, Quintanal-Villalonga Á, Gao VR,
Xie Y, Allaj V, Chaudhary O, Masilionis I, Egger J, Chow A, Walle
T, et al: Signatures of plasticity, metastasis, and
immunosuppression in an atlas of human small cell lung cancer.
Cancer Cell. 39:1479–1496. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Guo X, Zhang Y, Zheng L, Zheng C, Song J,
Zhang Q, Kang B, Liu Z, Jin L, Xing R, et al: Global
characterization of T cells in non-small-cell lung cancer by
single-cell sequencing. Nature Med. 24:978–985. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Hackshaw AK, Law MR and Wald NJ: The
accumulated evidence on lung cancer and environmental tobacco
smoke. BMJ. 315:980–988. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Jang HJ, Min HY, Kang YP, Boo HJ, Kim J,
Ahn JH, Oh SH, Jung JH, Park CS, Park JS, et al: Tobacco-induced
hyperglycemia promotes lung cancer progression via cancer
cell-macrophage interaction through paracrine IGF2/IR/NPM1-driven
PD-L1 expression. Nat Commun. 15:49092024. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Zhong L, Goldberg MS, Parent ME and Hanley
JA: Exposure to environmental tobacco smoke and the risk of lung
cancer: A meta-analysis. Lung Cancer. 27:3–18. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Hecht SS: Tobacco smoke carcinogens and
lung cancer. J Natl Cancer Inst. 91:1194–1210. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Adler S, Yip R, Chan H, Cai Q, Zhu Y,
Triphuridet N, Kaufman A, Taioli E, Flores R, Henschke CI, et al:
Comparison of lung cancer aggressiveness in patients who never
smoked compared to those who smoked. Lung Cancer. 171:90–96. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Gradishar WJ, Moran MS, Abraham J,
Abramson V, Aft R, Agnese D, Allison KH, Anderson B, Burstein HJ,
Chew H, et al: NCCN Guidelines® insights: Breast cancer,
version 4. J Natl Compr Canc Netw. 21:594–608. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Parsons MT, de la Hoya M, Richardson ME,
Tudini E, Anderson M, Berkofsky-Fessler W, Caputo SM, Chan RC,
Cline MS, Feng BJ, et al: Evidence-based recommendations for
gene-specific ACMG/AMP variant classification from the ClinGen
ENIGMA BRCA1 and BRCA2 Variant Curation expert panel. Am J Hum
Genet. 111:2044–2058. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Pal T, Agnese D, Daly M, La Spada A,
Litton J, Wick M, Klugman S, Esplin ED and Jarvik GP; Professional
Practice Guidelines Committee, : Points to consider: Is there
evidence to support BRCA1/2 and other inherited breast cancer
genetic testing for all breast cancer patients? A statement of the
American College of Medical Genetics and Genomics (ACMG). Genet
Med. 22:681–685. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Lucas AL, Fu Y, Labiner AJ, Dimaio CJ,
Sethi A and Kastrinos F: Frequent Abnormal pancreas imaging in
patients with pathogenic ATM, BRCA1, BRCA2, and PALB2 breast cancer
susceptibility variants. Clin Gastroenterol Hepatol. 21:2686–2688.
2023. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Narod SA and Giannakeas V: In response to
‘Pregnancy after breast cancer in patients with germline BRCA
mutations’. J Clin Oncol. 38:43522020. View Article : Google Scholar : PubMed/NCBI
|