Introduction
A few decades ago, the primary aim of treatment for
sarcoma arising in the extremities was to save the patient’s life.
Amputation was the standard surgical treatment for musculoskeletal
sarcomas of the extremities. In the 1980s, advances in adjuvant
therapy improved the tumor control and patient survival, advances
in diagnostic imaging allowed more accurate tumor staging and
advances in surgical and reconstructive techniques provided limb
salvage surgery as a safe alternative to amputation. Today, limb
salvage surgery is performed in 70–95% of all patients with bone
and soft tissue sarcoma of the extremities, even if the tumor is
high-grade (1–4).
However, reconstruction of a large bone defect after
resection of a tumor with a wide margin remains a major challenge.
The options for reconstruction after resection of a tumor around
the knee joint include implantation of a prosthesis, osteoarticular
allograft, allograft-prosthesis composite, recycled autologous bone
graft, arthrodesis with intercalary bone grafting or conversion to
a rotationplasty (5). Prosthetic
replacement after resection of a bone tumor around the knee joint
has been demonstrated to provide good function in most cases.
However, unfortunately, prosthesis-related complications still
remain an unresolved problem. Improvement in patient survival has
led to subsequent surgical revisions of the prosthesis as a result
of increases in prosthesis-related complications. These include
periprosthetic infections, aseptic loosening, and wear of the joint
components, dislocations, breakage of the prosthesis and fatigue
fractures. The long-term functional outcome of the affected limbs
depends on these complications. Until now, these are some reports
concerning to the prosthetic limb salvage surgery around the
knee.
The purpose of this study was to evaluate the
clinical and functional results of patients who underwent a limb
salvage surgery for tumors around the knee.
Materials and methods
Between 1982 and 2008, 63 patients underwent limb
salvage surgery. The mean follow-up period was 8.0 years (range,
0.8–28 years) after the initial operation. The patients’ medical
records, surgical reports, radiographs and pathologic records were
retrospectively reviewed (Table I).
Written informed consent was obtained from all of the patients
included in this study.
 | Table IDetails of the patient
characteristics. |
Table I
Details of the patient
characteristics.
| Distal femur (45
patients) | Proximal tibia (18
patients) |
|---|
| Age | 30 (11–79) | 28 (13–68) |
| Gender |
| Male | 25 | 9 |
| Female | 20 | 9 |
| Follow-up periods
(months) | 78.3 (3–340) | 141 (5–305) |
| Diagnosisa |
| OS | 35 | 10 |
| MFH | 1 | 2 |
| Metastasis | 2 | 1 |
| CS | 3 | 0 |
| GCT | 4 | 1 |
| Others | 0 | 4 |
| Surgical
stagingb |
| 3 | 4 | 1 |
| IA | 0 | 1 |
| IIA | 4 | 0 |
| IIB | 34 | 16 |
| III | 3 | 0 |
| Prosthesis |
| Custom made | 3 | 6 |
| Modular | 42 | 12 |
The patient group included 34 males and 29 females,
with a mean age of 29 years (range, 11–79 years) at the initial
treatment. The bone tumors involved the distal femur in 45
patients, the proximal tibia in 14 patients, and the soft tissue
tumors of the proximal lower leg in 4 patients. There were 45
high-grade osteosarcomas (OS), 3 chondrosarcomas, 3 malignant
fibrous histiocytomas (MFH), 5 giant cell tumors (GCT) and other in
7 patients. According to the Enneking staging system (6), one patient was categorized as Stage I,
four patients as IIA, 50 patients as IIB, and three patients as
III. The surgical excisions were performed with wide margins in all
cases. Forty-six patients underwent chemotherapy pre- and
post-operatively. The chemotherapy was performed using a
combination of 2–4 chemotherapeutic drugs, including cisplatin,
doxorubicin, cyclophosphamide, ifosfamide and methotrexate.
Post-operative chemotherapy was started 2–3 weeks after surgery. No
patient underwent radiotherapy.
Surgical methods
The surgical technique involved resection of the
tumor and reconstruction of the knee joint. The biopsy root was
also excised en bloc with a margin of >3-cm in the
malignant lesion. The tumor resection was carried out according to
standard oncologic principles. In all cases, the surgical excision
was performed with a wide margin (5). In the distal femoral tumors, the
median resection length was 16 cm (range, 9–22 cm), and in the
proximal tibia tumors, the median resection length was 14 cm
(range, 11–21 cm).
Special attention was given to cover the prosthesis
completely with muscle tissue. For the distal femur tumors, the
remaining vastus medialis was sutured to the rectus femoris. The
sartorius muscle could be mobilized and rotated anteriorly for
additional closure of the remaining medial soft tissue defect. For
the proximal lower leg tumor, reconstruction of the extensor
mechanism was performed in all patients. The patellar tendon and
anterior capsule were advanced and sutured to the anterior aspect
of the prosthesis using unabsorbent thread. A medial gastrocnemius
transposition flap (GTF) was used in all cases to provide adequate
soft-tissue coverage. In one patient, suturing of the patellar
ligament to the anteriorly transferred fibula was performed, and
this was then followed by covering the prosthesis with a GTF.
Prosthesis
After resection of the tumor, reconstruction was
performed using a prosthesis. Depending on the year the surgery was
performed four types of prostheses were used, which were selected
depending on the tumor location. From 1982 to 1987, a custom-made
prosthesis manufactured by Nemoto-shokai (Tokyo, Japan) was used.
This prosthesis has a restrained hinge and was fixed with cement.
Three Nemoto-shokai custom-made prostheses were used for
reconstruction of distal femurs and six were used for proximal
lower legs. From 1988 to 1997, cementless prostheses, HMRS
(Stryker-Howmedica-Osteonics, Rutherford, NJ), were used for
reconstruction of distal femurs. Thirteen HMRS prostheses were used
for reconstruction of distal femurs. This type of prosthesis is
still being used for the proximal lower leg. In all 12 HMRS
prostheses were used for proximal lower legs during the study
period. The HMRS is a first-generation modular endoprosthetic
system. It features intramedullary, cementless, press-fit stems
supported by external flanges and cortical transfixation screws.
The knee mechanism consists of a simple hinge design. From 1997,
for the reconstruction of the distal femur, 26 patients were
treated using the KLS/PHKIII system (Japan Medical Materials,
Osaka, Japan). The KLS/PHKIII is an original prosthesis in that the
metallic parts are fully made of titanium alloy, and this
prosthesis has a unique semi-rotating hinge joint and was designed
especially for people with the Asian body type/stature (7). Three patients with distal femur tumors
were implanted with other types of modular prostheses in the
1980s.
Assessment and statistical analysis
The oncological results, functional results, and
complications were investigated. A functional evaluation was
performed using the scoring system of the Musculoskeletal Tumor
Society (MSTS) which consists of six parameters (pain, function,
use of walking aids, walking activity, gait and emotional
acceptance) (8). The actuarial data
for the overall survival rate, disease-free survival rate,
prosthesis survival rate and limb salvage rate at the final
follow-up were calculated using a Kaplan-Meier analysis. The
prosthesis survival rate was calculated as the time from the
surgical reconstruction using the prosthesis to revision or
amputation due to prosthetic failure. Prosthetic failure was
defined as replacement of any parts of the prosthetic components,
including minor parts of the prosthesis due to local tumor
recurrence, polyethylene bushing failures, breakage of the
prosthesis and aseptic loosening or infection. Log-rank analyses
were used to determine the factors which influenced the prosthesis
survival rate. The factors included tumor locations, patient ages
(<30 vs. ≥30 years), gender, peroneal palsy vs. non-peroneal
palsy, extension lag (<30º vs. ≥30º) and primary vs. revision
procedures. Mann-Whitney U tests were also used to determine the
factors which correlated with the post-operative results of limb
function. The factors included tumor locations, patient ages
(<30 vs. ≥30 years), gender, perorneal palsy vs. non-peroneal
palsy, extension lag (<30º vs. ≥30º) and primary vs. revision
procedures. Analyses were performed using the Statview 5.0 software
program (SAS Institute, Inc., Cary, NC, USA). A P-value <0.05
was considered to be statistically significant.
Results
Oncological results
At the final follow-up, 36 patients were
continuously disease-free, 8 patients had no evidence of disease,
two patients alive with disease and 17 were patients dead of
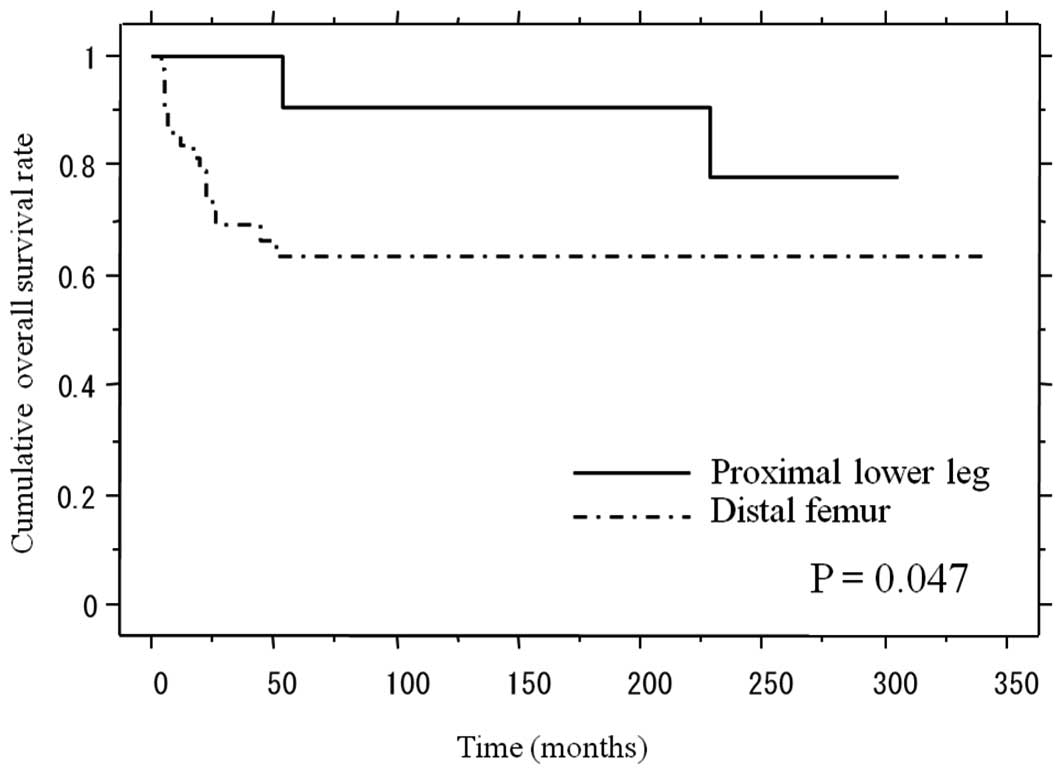
disease. The 5-year overall survival rate was 63.2% in the distal
femur cases and 86.2% in the proximal lower leg cases. The log-rank
test showed that there was a significant difference between the
cumulative survival rates based on the tumor location (P=0.047)
(Fig. 1). The patients with tumors
in their proximal lower legs had a better overall survival rate
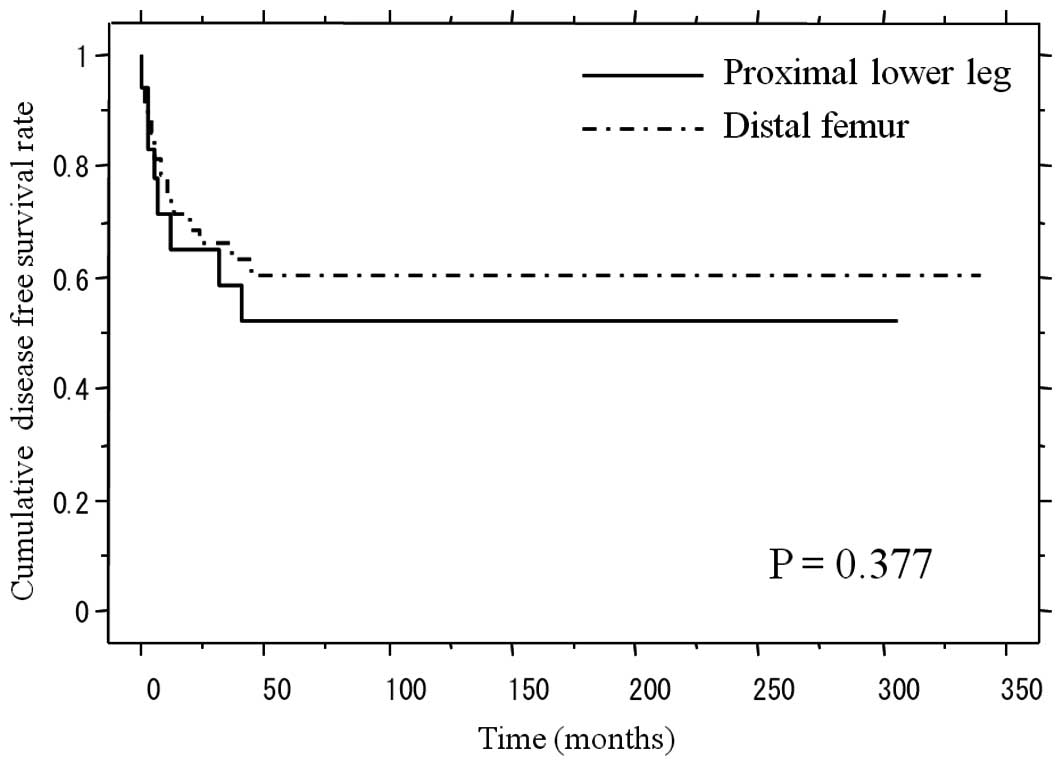
than those with distal femoral tumors. The 5-year disease-free
survival rates were 62.4 and 52.2% in the patients with distal
femur and the proximal leg tumors, respectively (Fig. 2). There were no significant
differences between the disease-free survival rates with regard to
the tumor location (log-rank test, P=0.377).
Prosthetic survival
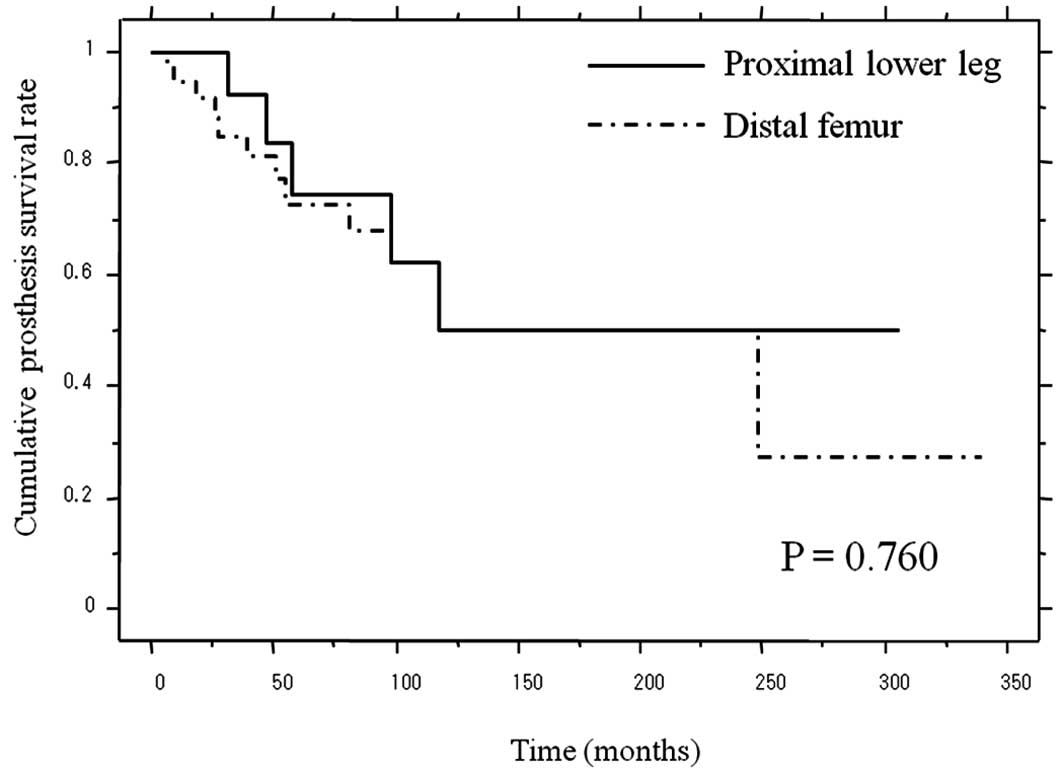
The 5-year prosthetic survival rate was 72.8% in the
distal femur cases and 74.6% in the proximal lower leg cases
(Fig. 3). There were no significant
differences between the prosthesis survival rates based on the
tumor location (log-rank test, P=0.760). During the follow-up
period, no limb amputation was performed. The log-rank test showed
no statistical difference between the prosthetic survival based on
the following factors: patient’s age, tumor location, gender,
presence of peroneal nerve palsy and the presence of extension lag
(Table II).
| Table IIResults of the univariate analysis
showing the factors which affect the 5-year prosthesis survival
rate. |
Table II
Results of the univariate analysis
showing the factors which affect the 5-year prosthesis survival
rate.
| Factors | No. of patients | 5-year prosthesis
survival rate (%) | P-valuea |
|---|
| Tumor location |
| Distal femur | 45 | 72.8 | 0.76 |
| Proximal tibia | 18 | 74.6 | |
| Age (years) |
| <30 | 31 | 75.3 | 0.91 |
| ≥30 | 32 | 70.3 | |
| Gender |
| Male | 34 | 72.1 | 0.88 |
| Female | 29 | 76.0 | |
| Peroneal nerve
palsy |
| Yes | 13 | 83.3 | 0.91 |
| No | 50 | 72.5 | |
| Extension lag |
| <30º | 13 | 73.3 | 0.053 |
| ≥30º | 4 | 0 | |
Functional results
The mean post-operative functional score was 81%
(range, 37–100%). The mean functional score was 81% (range,
37–100%) in the patients with distal femur tumors and 82% (range,
53–97%) in the patients with proximal lower leg tumors (Table III).
| Table IIIResults of the univariate analysis
showing the factors which affect the MSTS score. |
Table III
Results of the univariate analysis
showing the factors which affect the MSTS score.
| Factors | No. of patients | MSTS score | P-valuea |
|---|
| Tumor location |
| Distal femur | 45 | 81 (40–100) | 0.73 |
| Proximal lower
leg | 18 | 82 (53–97) | |
| Age (years) |
| <30 | 31 | 81 (37–100) | 0.85 |
| ≥30 | 32 | 82 (40–100) | |
| Gender |
| Male | 34 | 86 (53–100) | 0.04 |
| Female | 29 | 75 (37–100) | |
| Peroneal nerve
palsy |
| Yes | 13 | 66 (37–97) | 0.01 |
| No | 50 | 85 (60–100) | |
| Extension lag |
| <30º | 13 | 91 (73–100) | <0.01 |
| ≥30º | 4 | 63 (37–73) | |
| Primary | 46 | 82 (37–100) | 0.89 |
| Revision | 17 | 78 (53–97) | |
Regarding the functional results, the Mann-Whitney U
test showed that male patients had significantly better limb
function than female patients (P=0.04). Patients with peroneal
nerve palsy showed significantly worse MSTS scores than those
without peroneal palsy (Mann-Whitney U test, P=0.01). Patients with
extension lag in excess of 30º had a worse MSTS score than those
with less extension lag (P<0.01). The Mann-Whitney U test showed
no significant difference in MSTS scores between primary and
revision surgery (P=0.89).
Complications
A total of 27 of the 63 patients (43%) developed
post-operative complications. Forty-nine post-operative
complications occurred in these 27 patients. The major
complications were peroneal palsy in 13 patients (21%), followed by
loosening in 7 patients (11.1%), breakage of the hinge mechanism in
4 patients (6.3%), breakage of the stem in 4 patients (6.3%),
breakage of a femoral or tibial component in 4 patients (6.3%), a
leg length discrepancy of >2 cm in 4 patients (6.3%), local
recurrence in 4 patients (6.3%), deep infection in 3 patients
(4.8%), skin trouble in 3 patients (4.8%), a periprosthetic
fracture in 2 patients (3.2%), and secondary cancer after
chemotherapy in 1 patient (1.6%) (Table IV).
| Table IVComplications. |
Table IV
Complications.
| Distal femur (45
patients) | Proximal tibia (18
patients) |
|---|
| Prosthesis-related
complications | | |
| Breakage of
prosthesis | 11 | 3 |
| Loosening | 6 | 1 |
| Peroneal nerve
palsy | 5 | 8 |
| Leg length
discrepancy (≥2 cm) | 4 | 0 |
| Recurrence | 3 | 1 |
| Deep infection | 1 | 2 |
| Skin trouble (only
superficial) | 2 | 1 |
| Secondary
cancer | 1 | 0 |
Forty-three operations were eventually required to
treat these complications. For the deep infections, 19 operations
were required, including debridement, primary sutures or coverage
with a skin flap. For the skin troubles, 7 minor operations such as
secondary suturing were performed. For loosening of the prosthesis,
three revision surgeries were required. For the breakage of stems,
4 revision surgeries were performed. Four and 6 surgeries were
performed to repair a breakage of a femoral or tibial component, or
the breakage of a hinge (e.g., breakage of bush or insert),
respectively. Two of the 4 patients with local recurrence underwent
a wide excision of the recurrent tumor preserving the prosthesis,
and one patient exchanged the prosthesis. Another patient with
multiple metastases did not undergo surgery because of a putative
poor prognosis.
In cases of distal femoral reconstruction, 6
prostheses, including 3 modular prostheses and 3 custom-made
prostheses, were implanted before 1987. Breakage of prosthetic
components was observed in 3 of these 6 prostheses (50%). Three
patients had 4 breakages of their prosthesis. One patient
experienced the breakage of a stem. One patient had loosening of a
component. One patient had breakage of the hinge after breakage of
the stem. But since the HMRS or KLS/PHK III were introduced for
reconstruction, the rate of prosthesis breakage was 23% (9 of 39
prostheses). Nine patients had 13 breakages of the prosthesis.
In addition, in the 6 cases of proximal tibial
reconstruction using custom-made prostheses which were implanted
before 1987, breakage of the prosthesis was observed in 2 cases
(33%). One patient had breakage of a tibial component, and the
other patient had loosening of the prosthesis. But since the HMRS
was introduced for reconstruction, the rate of prosthesis breakage
has been 17% (2 of 12 patients). One patient suffered the breakage
of both the bush and tibial components two times, while another
patient had breakage of a tibial component.
Discussion
In this study, the 5-year overall survival rate was
63% in the patients with distal femur tumors and 86% in those with
tumors of the proximal lower leg. The 5-year disease-free survival
rate was 62 and 52% in the subjects with tumors of the distal femur
and the proximal leg, respectively. The 5-year prosthetic survival
rate was 73% in the distal femur and 75% in the proximal lower leg.
The mean functional score according to the scoring system of the
MSTS score was 81% in the patients with distal femur tumors and 82%
in the patients with proximal lower leg tumors. Post-operative
complications occurred in 27 patients (43%), but no limb amputation
was performed.
Both the distal femur and proximal tibia are common
anatomic sites for primary and metastatic bone tumors. These tumors
were traditionally treated with arthrodesis or amputation of the
affected extremity and resulted in unfavorable functional and
psychologic outcomes (9,10). However, the prognosis of the sarcoma
patients has recently improved as a result of a better
understanding of tumor biology, refined chemotherapeutic protocols,
advances in diagnostic imaging and improvements in surgical
techniques. Improvements in the survival of sarcoma patients made
these drawbacks not only more pronounced, but also promoted the
development of new surgical reconstructive procedures which
promised more useful limb function. Simon et al compared the
results of limb-sparing resections to those of amputation in 227
patients with distal femoral osteosarcoma, and concluded that the
limb salvage surgery did not shorten the disease-free interval or
compromise the long-term survival of these patients compared to
amputation (11).
Although amputation still remains one of the
important options for patients whose tumors are too advanced to
obtain a safe margin, amputation has a negative impact on the
patient’s psychological well-being. With regard to arthrodesis, it
is not suitable for many Asian patients, because squatting is
necessary in many components of the Asian lifestyle, such as eating
meals while sitting on the floor. Rotationplasty provides good
local disease control and good function, but the cosmetic outcome
is sometimes not acceptable for patients, especially younger
patients. Harris et al also evaluated the results after
amputation, arthrodesis and endoprosthetic replacement. They found
that only patients with prosthetic reconstruction felt themselves
to be close to the healthy population (12). We therefore have pursued limb
salvage surgery using a prosthesis as the first choice for
resectable malignant tumors occurring around the knee.
In the distal femur, the 3-, 5- and 10-year
prosthesis survival rates were 85, 73 and 68%, respectively. In the
proximal lower leg, the 3-, 5- and 10-year prosthesis survival
rates were 92, 75 and 50%, respectively. In previous studies, the
prosthesis survival of the proximal tibia has been reported to be
lower than that of the distal femur (Table V) (13–21).
Poor soft tissue coverage, difficulties with anchoring the patellar
tendon and possible injuries to the neurovascular system are the
most likely causes for this difference. Horowitz et al
reported that distal femur prostheses showed 75 and 67% survival,
while proximal tibia prostheses showed 54 and 36% survival at 5 and
10 years, thus indicating that there were significant differences
in the prosthetic survival between distal femur and proximal tibia
prostheses (17). Biau et al
reported prosthesis 5- and 10-year survival rates of 85 and 55% in
the distal femur, respectively, while they were 72 and 45% in the
proximal tibia (14). In contrast,
Torbert et al showed no statistically significant
differences in the event-free prosthetic survival rate between the
distal femur and proximal tibia prosthesis (20). Distal femur prostheses showed 90, 84
and 66% survival rate at 3-, 5- and 10-year, respectively, while
proximal tibia prostheses showed 63% survival rates at 3-, 5- and
10-year. Direct comparisons of the present results to other
published reports may be difficult due to the heterogeneity with
respect to the patient population and implant used. In our series,
log-rank testing showed no significant differences between the
prosthetic survival and tumor location. Although the present study
consisted of a relatively small number of patients with proximal
lower leg tumors, there was no aseptic loosening except for one
patient who underwent prosthetic reconstruction before 1987. The
HMRS has a porous-coated stem, and permits bone ingrowth at the
bone/prosthesis junction. Thus, this prosthetic design might reduce
the risk of mechanical failure and loosening, as well as the
improvement of the surgical technique.
| Table VReview of the literature. |
Table V
Review of the literature.
| Tumor location | No. of
patients | Follow-up
(years) | Overall survival
rate (%) | Prosthesis survival
rate (%) | Functional score
(%) | Complications rate
(%) | Revision rate
(%) | Amputation rate
(%) |
|---|
|
|
|---|
| 3-year | 5-year | 10-year | 3-year | 5-year | 10-year |
|---|
| Carty et al
(15) |
| aDF and bPT | 20 | 7.5 | | | | | | | 83 | | | |
| Tunn et al
(21) |
| DF | 41 | 6.5 | | | | | | | 87 | | 31 | |
| PT | 27 | | | | | | | | 77 | | | |
| Myers et al
(19) |
| PT | 194 | | | | | | | | | | 28 | 18 |
| Biau et al
(14) |
| DF and PT | 96 | 5.1 | | | | | 80 | 52 | | 58 | | |
| Torbert et
al (20) |
| DF | 57 | 4.7 | | | | 90 | 84 | 66 | | | | |
| PT | 27 | | | | | 63 | 63 | 63 | | | | |
| Bickels et
al (13) |
| DF | 110 | | | | | | 93 | 88 | | | 14 | 4 |
| Ilyas et al
(18) |
| PT | 15 | 3.5 | | | | | | | 61 | 73 | 0 | 13 |
| Grimer et al
(16) |
| PT | 151 | 6.7 | | | | | | | 77 | | 63% at 10-year | 17 |
| Horowitz et
al (17) |
| DF | 61 | 5.5 | | 75 | 67 | | 59 | 28 | | | | 12% at 5-year |
| PT | 16 | | | 93 | 93 | | 54 | 36 | | | | 22% at 5-year |
| Present report |
| DF | 45 | 8.0 | 69 | 63 | 63 | 81 | 73 | 73 | 81 | 38 | 24 | 0 |
| Proximal lower
leg | 18 | | 100 | 91 | 91 | 84 | 75 | 50 | 82 | 61 | 33 | 0 |
The rate of infection was 4.8% in our series, and
ranged from 2.2–33% in previous studies (13,16,19).
Infections required secondary procedures. But the consequences
nonetheless were noteworthy, with no limb amputation. Infections
are difficult to avoid in prosthetic limb salvage surgery for
numerous reasons: multiple surgeries, resection of large amounts of
tissue, skin sloughing, adjuvant treatments and poor blood supply
to the allograft. Providing adequate soft tissue coverage after
reconstruction is one of the most critical factors for reducing
infection. Grimer et al (16) reported that their initial results
for proximal tibia tumor reconstruction were poor because of the
high infection rate derived from wound breakdown and an infection
rate of 33%. However, this rate later decreased to 12% with the use
of a flap to cover the wound. We therefore recommend the use of a
musculocutaneal flap for this operation, though infection, remains
a common complication in our study.
In our series, the Mann-Whitney U test showed that
male patients had significantly better limb function than female
patients. We speculate that this result could be due to the
residual muscle power in male patients. Patients with peroneal
nerve palsy also showed a significantly worse MSTS score than those
without peroneal palsy. These results suggest that preservation of
the quadriceps femoris muscle and avoidance of peroneal nerve palsy
are critical to maintaining a good limb function.
In summary, prosthetic reconstruction for
musculoskeletal tumors around the knee provides good oncological
and functional results. However, the high complication rate is a
major concern for the prosthetic replacement. Future improvements
of prostheses are very important. With regard to the surgical
techniques, the preservation of the quadriceps femoralis muscle and
avoidance of peroneal nerve palsy are important.
References
|
1
|
Böhm P, Springfeld R and Springer H:
Re-implantation of autoclaved bone segments in musculoskeletal
tumor surgery. Clinical experience in 9 patients followed for 11–84
years and review of the literature. Arch Orthop Trauma Surg.
118:57–65. 1998.PubMed/NCBI
|
|
2
|
Niimi R, Matsumine A, Kusuzaki K, Kuratsu
S, Araki N, Aoki Y, Ueda T, Kudawara I, Myoui A, Ieguchi M, et al:
Usefulness of limb salvage surgery for bone and soft tissue
sarcomas of the distal lower leg. J Cancer Res Clin Oncol.
134:1087–1095. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Veth R, Hoesel R, Pruszczynski M,
Hoogenhout J, Schreuder B and Wobbes T: Limb salvage in
musculoskeletal oncology. Lancet Oncol. 4:343–350. 2003. View Article : Google Scholar
|
|
4
|
Zaretski A, Amir A, Meller I, Leshem D,
Kollender Y, Barnea Y, Bickels J, Shpitzer T, Ad-El D and Gur E:
Free fibula long bone reconstruction in orthopedic oncology: a
surgical algorithm for reconstructive options. Plast Reconstr Surg.
113:1989–2000. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Anract P, Missenard G, Jeanrot C, Dubois V
and Tomeno B: Knee reconstruction with prosthesis and muscle flap
after total arthrectomy. Clin Orthop Relat Res. 384:208–216. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Enneking WF: A system of staging
musculoskeletal neoplasms. Clin Orthop Relat Res. 204:9–24.
1986.PubMed/NCBI
|
|
7
|
Matsumine A, Ueda T, Sugita T, Yazawa Y,
Isu K, Kawai A, Abe S, Yakushiji T, Hiraga H, Sudo A and Uchida A:
Clinical outcomes of the KYOCERA Physio Hinge Total Knee System
Type III after the resection of a bone and soft tissue tumor of the
distal part of the femur. J Surg Oncol. 103:257–263. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Enneking WF, Dunham W, Gebhardt MC,
Malawar M and Pritchard DJ: A system for the functional evaluation
of reconstructive procedures after surgical treatment of tumors of
the musculoskeletal system. Clin Orthop Relat Res. 286:241–246.
1993.PubMed/NCBI
|
|
9
|
Enneking WF and Shirley PD: Resection
arthrodesis for malignant and potentially malignant lesions about
the knee using an intramedullary rod and local bone graft. J Bone
Joint Surg Am. 59:223–235. 1977.PubMed/NCBI
|
|
10
|
Sugarbaker PH, Malawer MM and Baker AR:
Above-knee amputation. Musculoskeletal Surgery for Cancer.
Sugarbaker PH and Malawer MM: Thieme Medical Publishers; New York:
pp. 229–242. 1992
|
|
11
|
Simon MA, Aschliman MA, Thomas N and
Mankin HJ: Limb-salvage treatment versus amputation for
osteosarcoma of the distal end of the femur. J Bone Joint Surg Am.
68:1331–1337. 1986.PubMed/NCBI
|
|
12
|
Harris IE, Leff AR, Gitelis S and Simon M:
Function after amputation, arthrodesis, or arthroplasty for tumors
about the knee. J Bone Joint Surg Am. 72:1477–1483. 1990.PubMed/NCBI
|
|
13
|
Bickels J, Wittig JC, Kollender Y, Henshaw
RM, Kellar-Graney KL, Meller I and Malawer MM: Distal femur
resection with endoprosthetic reconstruction: a long-term followup
study. Clin Orthop Relat Res. 400:225–235. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Biau D, Faure F, Katsahian S, Jeanrot C,
Tomeno B and Anract P: Survival of total knee replacement with a
megaprosthesis after bone tumor resection. J Bone Joint Surg Am.
88:1285–1293. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Carty CP, Dickinson IC, Watts MC, Crawford
RW and Steadman P: Impairment and disability following limb salvage
procedures for bone sarcoma. Knee. 16:405–408. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Grimer RJ, Carter SR, Tillman RM, Sneath
RS, Walker PS, Unwin PS and Shewell PC: Endoprosthetic replacement
of the proximal tibia. J Bone Joint Surg Br. 81:488–494. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Horowitz SM, Glasser DB, Lane JM and
Healey JH: Prosthetic and extremity survivorship after limb salvage
for sarcoma. How long do the reconstructions last? Clin Orthop
Relat Res. 293:280–286. 1993.PubMed/NCBI
|
|
18
|
Ilyas I, Younge D, Pant R and Moreau P:
Limb salvage for proximal tibial tumours using a modular
prosthesis. Int Orthop. 24:208–211. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Myers GJ, Abudu AT, Carter SR, Tillman RM
and Grimer RJ: The long-term results of endoprosthetic replacement
of the proximal tibia for bone tumours. J Bone Joint Surg Br.
89:1632–1637. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Torbert JT, Fox EJ, Hosalkar HS, Ogilvie
CM, Ogilvie CM and Lackman RD: Endoprosthetic reconstructions:
results of long-term followup of 139 patients. Clin Orthop Relat
Res. 438:51–59. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tunn PU, Pomraenke D, Goerling U and
Hohenberger P: Functional outcome after endoprosthetic limb-salvage
therapy of primary bone tumours - a comparative analysis using the
MSTS score, the TESS and the RNL index. Int Orthop. 32:619–625.
2008. View Article : Google Scholar : PubMed/NCBI
|