Colorectal cancer is the third most common type of
cancer in the world and the second leading cause of
cancer-associated death in the United States (1,2).
According to the global cancer statistics in 2020, there were
>1.9 million new cases of colorectal cancer, among which rectal
cancer accounted for 30–50%, and 935,000 associated deaths
(3,4). Approximately half of rectal cancer
diagnoses are of locally advanced rectal cancer (LARC), which is
difficult to treat and has a poor prognosis (5). According to the Tumor-Node-Metastasis
classification (6,7), LARC is defined as patients with
cT3-cT4 or N+ (stage II or III) rectal cancer without
distant metastasis (8).
Neoadjuvant chemoradiotherapy (NCRT) followed by total mesorectal
excision (TME) after 6–10 weeks is the preferred treatment for LARC
(9,10). NCRT can decrease the tumor size and
tumor stage, block tumor invasion, and improve resection during
surgery and the probability of sphincter preservation, thus
increasing the local control rate and the survival rate of the
patient (10–13).
Identifying biomarkers that predict the response to
NCRT is a constant challenge. Numerous studies have proposed
biomarkers that could predict response to NCRT in patients with
LARC, such as tumor stage, tumor regression grade, tumor markers
(carcinoembryonic antigen), circulating tumor-derived DNA, DNA
methylation level and cancer related-inflammatory markers; however,
their accuracy is not perfect (14–17).
As LARC has great heterogeneity in proteins, genes, cells and
tissues (18), it is difficult to
capture its heterogeneity by using examinations such as
pathological biopsy, colonoscopy and hematology (19–21).
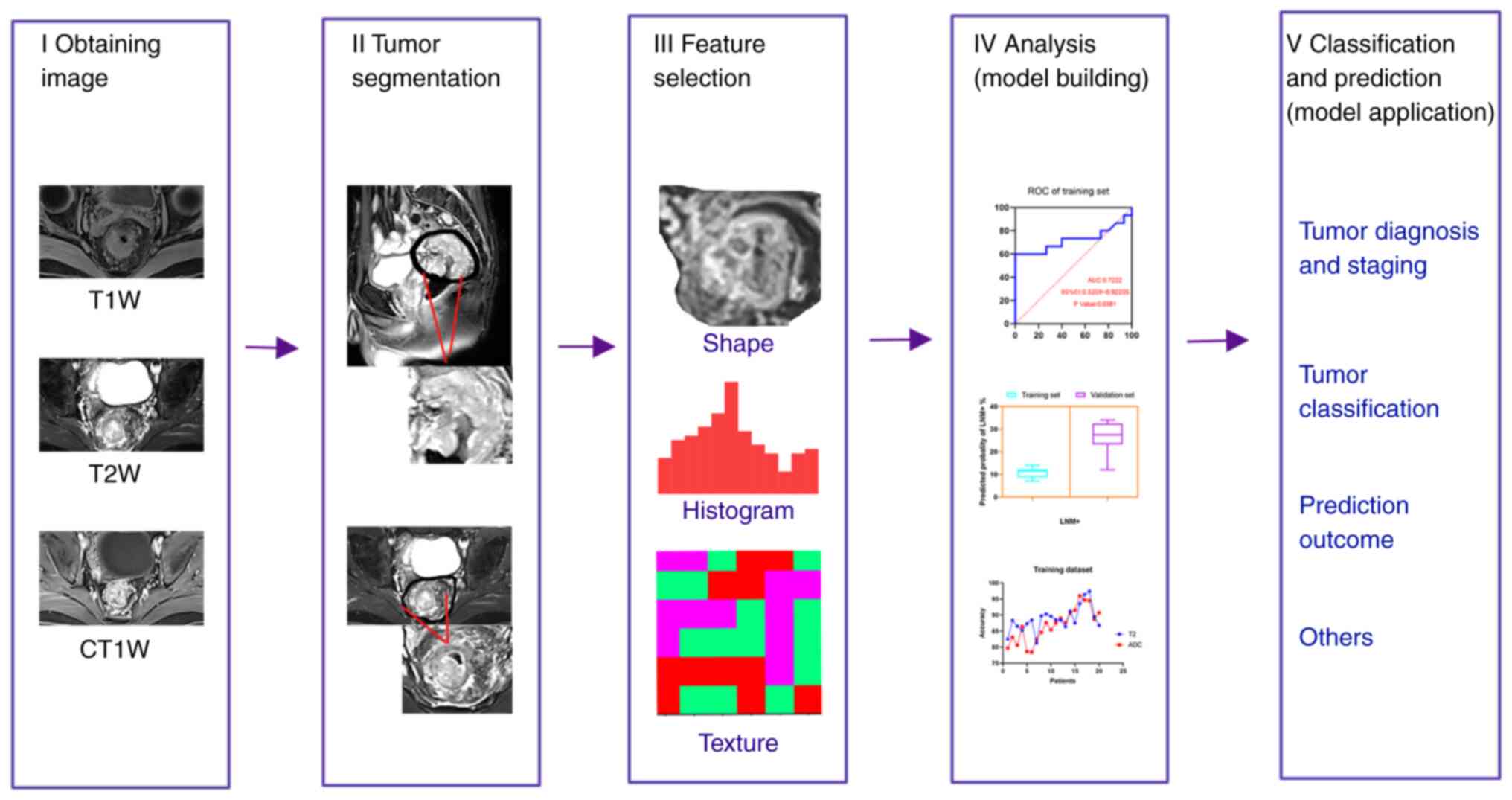
By contrast, as a new non-invasive imaging technology, radiomics
transforms medical imaging into high-dimensional data that can be
mined to reveal a large number of quantitative features, including
texture, grayscales, wavelet and fractal, and combines quantitative
features with clinical features, protein genome information and
other information (22,23). With its advantages, such as being
easy to operate, a low cost and a high efficiency in capturing the
heterogeneity of tumors, it can be used for tumor diagnosis,
staging, prognosis and predicting treatment response (24–27);
it also has great potential to be an imaging biomarker for
predicting the response to NCRT and determining the prognosis.
In recent years, there has been an increase in the
amount of research into MRI-based radiomics in LARC. In the present
review, based on existing research, the workflow of radiomics will
first be introduced, and then the research into MRI-based radiomics
for predicting the response of patients with LARC to NCRT, and
their prognosis, will be summarized. Lastly, the challenges and
development trends of MRI-based radiomics will be discussed.
Imaging examination is an important medical
technique, which is mainly used to assist clinical decision-making
in clinical practice (36). With
the rapid development of medical technology, imaging examination
has gradually evolved from a clinical diagnostic tool to a powerful
tool for personalized medicine (37). The most common imaging examinations
for the diagnosis and staging of rectal cancer include CT, MRI,
positron emission tomography (PET)/CT and ultrasound endoscopy
(38). CT is able to show the
structural characteristics of tumors, and is often used in
dosimetry research and tumor staging of rectal cancer radiotherapy
(39). However, it also has some
shortcomings, such as the inability to describe the function of
solid tumors, limited T staging of early rectal cancer, high
radiation and low contrast (40,41).
PET/CT is mainly used to evaluate the metabolic activity of tumors,
which are usually more active than normal tissue (42). In addition, it is used for tumor
diagnosis, staging and assessment of metastasis in rectal cancer;
however, its spatial resolution is low, thus tumor T staging is
limited. At the same time, PET/CT not only has a high price, high
radiation toxicity and relatively complicated usability, but it is
also difficult to describe and analyze the features of its lesions
in radiomics research (40,43).
By contrast, MRI has high resolution for soft tissue, and has the
advantages of being radiation-free, multi-orientational,
multi-parameter and delineating the tumor boundary clearly
(44,45). MRI is considered as the standard
for the evaluation and staging of rectal cancer, and has wide
application value in LARC (38,46,47).
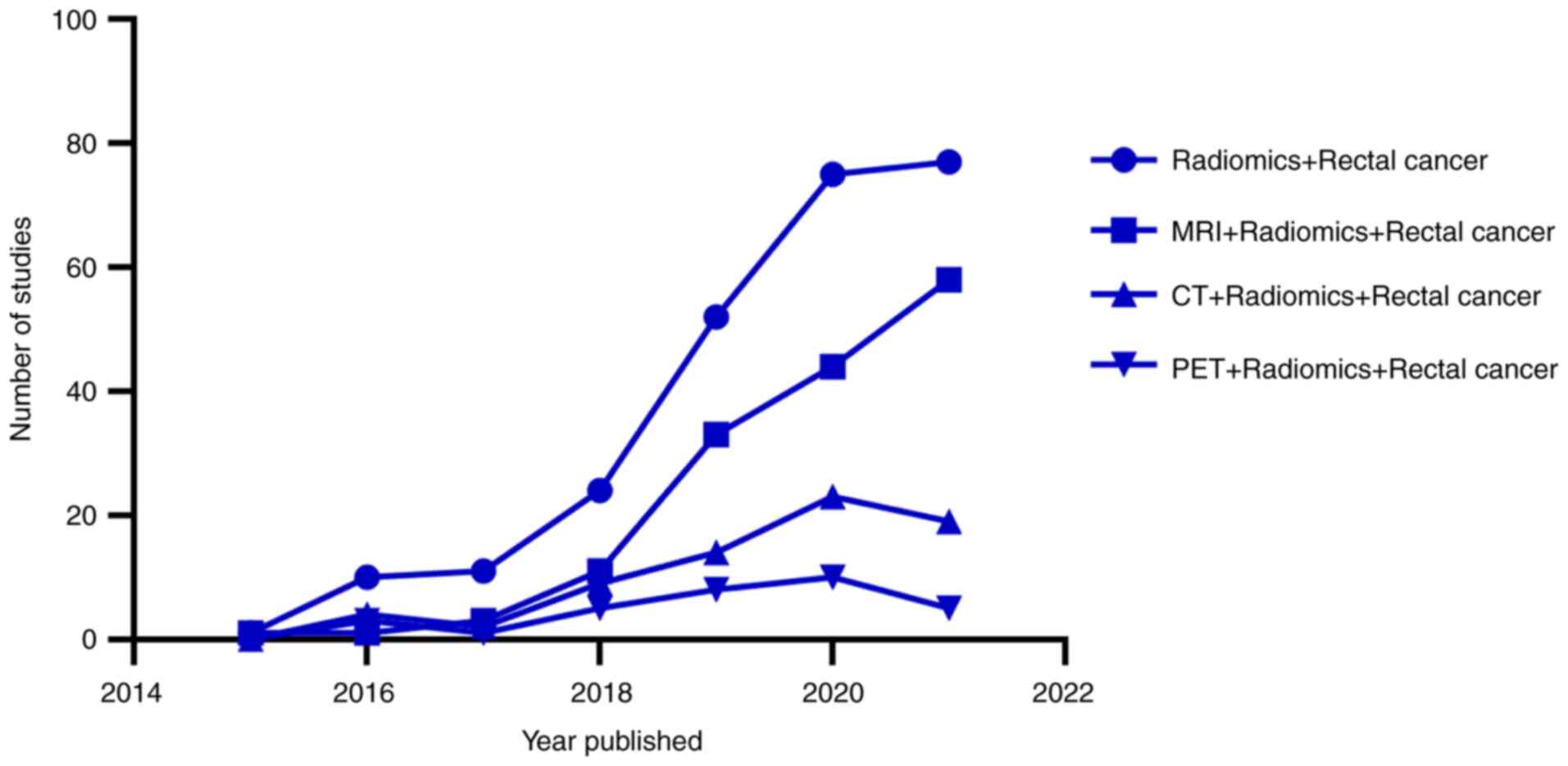
In recent years, the research into radiomics in rectal cancer has
increased year on year, and there is more research into
radiomics-based on MRI than that based on CT or PET/CT. This
indicates that radiomics-based on MRI is of great research
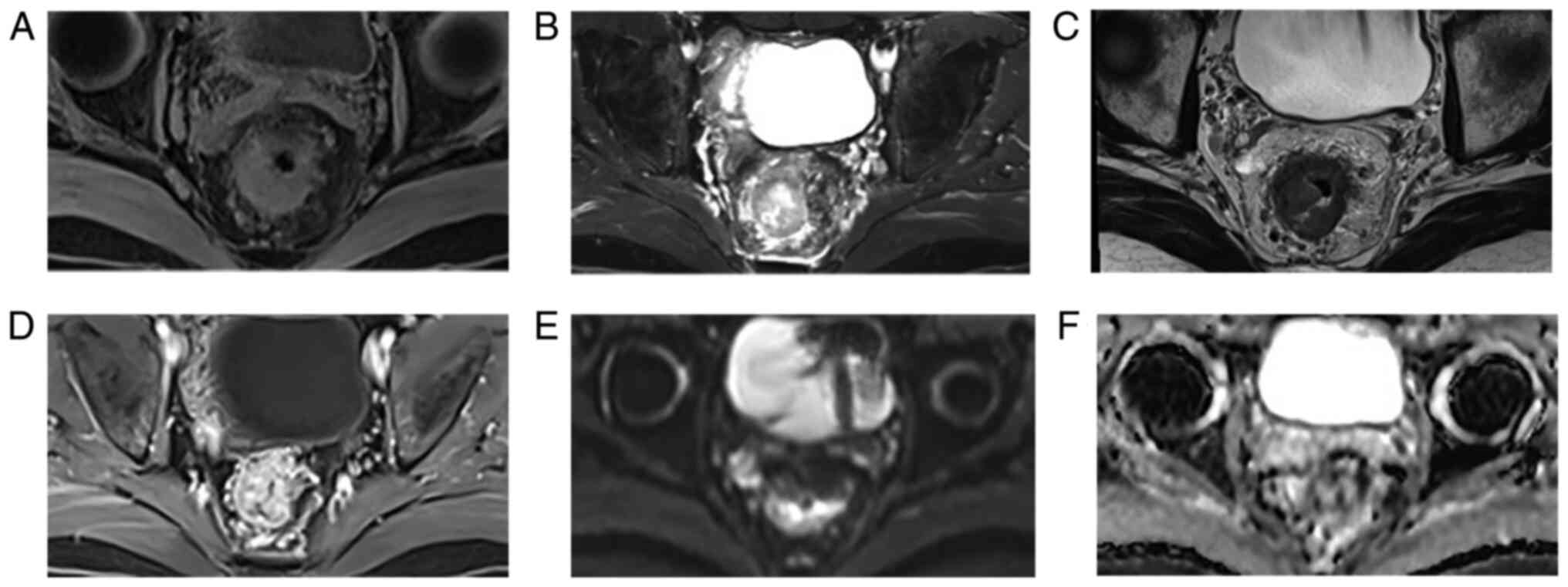
significance and has potential in rectal cancer (Fig. 2). MRI has multi-parameter
characteristics, which can be divided into morphological and
functional parameters. Morphological parameters include T1-weighted
imaging (T1WI) and T2-weighted imaging (T2WI), while functional
parameters include diffusion-weighted imaging and enhanced
scanning. The most commonly used examination parameter (sequence)
is T2WI, with an accuracy of 65–94% for T staging and 35–75% for N
staging in rectal cancer (32,48)
(Fig. 3). Morphological imaging is
beneficial to provide detailed information of rectal cancer and its
surrounding structures. Functional imaging distinguishes residual
tumors from fibrosis (49). The
information provided by the various imaging methods is different.
Combining different imaging features can improve the prediction
efficiency of the model. MRI radiomics, as an imaging biomarker,
can predict the response of patients with rectal cancer to NCRT and
the prognosis of the tumor from numerous aspects, including
pathological complete response (PCR) determination, lymph node
status, KRAS status, tumor-stroma ratio and tumor heterogeneity
(31,50–52).
The following is an analysis from the three aspects: PCR
determination, lymph node status and KRAS status (Table I). Data for the present study,
including Table I, was obtained by
searching the Pubmed (http://www.ncbi.nlm.nih.gov), WebofScience (http://www.webofscience.com) and Metstroge (https://www.metstr.com) databases from mainly the last
6 years (with a few studies prior to 2015). The key words used
include radiomics and locally advanced rectal cancer rectal cancer,
NCRT, MRI, CT, PET, PCR, lymph nodes, Kras, challenges, limitations
and prospects. Approximately >300 studies were searched, and
>100 studies were finally cited.
The curative effect of NCRT on LARC is notable;
however, the individual response to treatment varies, from a PCR to
almost no tumor regression, while some patients have tumor
progression (53). In total, ~20%
of the patients can attain a PCR (54), and a PCR is equivalent to no
residual tumor cells (55–57). Patients with a PCR are able to
receive ‘waiting or watching’ treatment, which is a non-surgical
treatment strategy used for patients to obtain complete clinical
remission (58,59). If PCR can be predicted prior to
surgery, personalized medicine can be used. A large number of
studies have shown that MRI radiomics is effective in predicting
the tumor response of LARC following NCRT. Yi et al
(50) used T2WI radiomics,
combining imaging features with clinical pathological
characteristics to construct a prediction model. The results showed
good diagnostic accuracy in predicting a PCR, a good response and
tumor degradation in patients with LARC who had progressed to NCRT,
and the area under curve values were 0.908, 0.902 and 0.930,
respectively. Dinapoli et al (60) analyzed the radiomics of 221
patients from three different centers and concluded that the MRI
radiomics model could predict the probability of a PCR in patients
with LARC using pre-treatment imaging. The study also established
external verification (performed with patients from two other
institutions) to further improve the credibility of its model. In
addition, Li et al (61)
completed MRI prior to and following NCRT, and analyzed the images
in parallel. By comparing the changes in the images during
treatment, seven radiomics features were extracted. The prediction
model could effectively predict a PCR following NCRT. It could be
concluded that MRI prior to and following NCRT is an important
source of radiomics data. At the same time, the radiomics model
also predicted patients who were unresponsive or low in response to
treatment. This was beneficial as the treatment plan could be
adjusted in clinical practice, unnecessary toxicity of radiotherapy
and chemotherapy could be avoided, and the economic burden for the
patients could be reduced. Zhou et al (62) analyzed the multi-parameter MRI in
425 patients with LARC prior to NCRT. It was concluded that the
features of multi-parameter MRI prior to treatment could
effectively predict patients who were non-response to NCRT.
Therefore, MRI-based radiomics, whether multi-parameter or
single-sequence MRI radiomics, is of great significance in
evaluating PCR and unresponsiveness following NCRT. This could
provide an improved basis for personalized treatment.
Most treatment responses following NCRT are
evaluated by observing the primary tumor; however, lymph nodes can
also be evaluated, as NCRT can cause heterogeneous response of the
lymph nodes (63). NCRT can cause
certain changes in the lymph nodes, such as changes in their
morphology, size, number and texture. In addition, the response of
the lymph nodes to NCRT varies, ranging from a large number of
residual cancer cells to a completely fibrotic response (the
surrounding normal cells continue to proliferate to repair the
damage caused by radiotherapy and chemotherapy, which specifically
means that there are no residual tumor cells). Therefore, it can be
complicated to interpret the prognostic impact of the lymph nodes
following NCRT due to the changes in the lymph nodes (64). A large number of previous studies
have shown that the positive mesenteric lymph nodes are the main
cause of the local recurrence and distant spread of rectal cancer
(51,65–67).
TME is significantly effective for local tumor control; however,
there are numerous complications, such as sexual dysfunction, poor
urination and infection (68–70).
Therefore, organ preservation strategies, such as watchful waiting
and local excision following NCRT, are particularly important in
preserving organ function and improving the quality of life of the
patients (71,72). It is worth noting that the status
of the lymph nodes following NCRT is an important indicator of
organ preservation strategies (63,73).
Hence, assessing the status of the lymph nodes following NCRT is of
great significance in assessing treatment response, predicting
prognosis and improving the quality of life of patients.
In the past, clinicians often used the size of the
lymph nodes to estimate which lymph nodes could have metastases and
which could be free of metastatic foci (74), to assess the volume reduction rate
prior to and following treatment to evaluate lymph node metastasis
(75), or to predict the status of
the lymph nodes using clinicopathological factors (76); however, precise prediction accuracy
has not been achieved. In recent years, with the development of
artificial intelligence and big data, radiomics studies have become
increasingly popular in the clinic. A large number of studies have
shown that radiomics can effectively predict the status of the
lymph nodes and provide a basis for clinical decision-making. For
example, Zhou et al (72)
predicted the status of the lymph nodes following NCRT using a
multi-parameter MRI radiomics model. The joint model of
multi-parameter MRI radiomics features and tumor staging was
obtained. The receiver operating characteristic curve was 0.818 and
the negative predictive value was 93.7% in the validation cohort,
which was higher than that in the single imaging model. In
particular, the combined model had high accuracy in evaluating the
lymph node status in patients with MRI T1-2 tumors following NCRT,
and its negative predictive value was as high as 100%. Song and Yin
(77) found that the low energy of
sagittal fat inhibition T2WI, and the high information correlation
and short-run low gray-level emphasis of oblique T2WI, were
independent predictors of lymph node invasion of rectal cancer.
These have a certain value in judging preoperative lymph node
invasion.
In summary, MRI-based radiomics has the advantage of
being non-invasive and easy to use, with a high prediction accuracy
and no need to visualize features (tumor shape, edge and size). MRI
also has a good ability to identify lymph nodes, which has great
potential in predicting the lymph node status of patients with LARC
following NCRT. However, there are relatively few studies based on
this aspect at present, which requires the support of big data and
multi-center research. This presents an opportunity for future
scientific research.
A large number of studies have reported that the
KRAS mutation is a good biomarker to predict the resistance and
prognosis of metastatic rectal cancer with anti-epidermal growth
factor receptor monoclonal antibody therapy (78,79).
The KRAS gene is a murine sarcomatoid virus oncogene that belongs
to the RAS gene family and has been associated with the development
of human tumors. The KRAS mutation is the most common gene mutation
in colorectal cancer. Between 30 and 40% of patients with
colorectal cancer carry the KRAS mutation (80). In LARC, the KRAS mutation has been
associated with tumor invasion and metastasis, insensitivity to
epidermal growth factor inhibitor and low overall survival time
(81,82). Certain patients with LARC have low
sensitivity to NCRT, and have side effects to radiotherapy and
chemotherapy, such as trisomy, radiation proctitis and sexual
dysfunction. Early in vitro experiments have proved that
cell lines with the KRAS mutation are more prone to radiation
resistance and mediate the radiation resistance of cells via the
EGFR/PI3K/AKT pathway (83,84).
At present, there are numerous studies investigating the
association between the KRAS mutation and treatment response
following NCRT. For example, Zhou et al (82) retrospectively analyzed 1,886
patients with LARC, and found that the KRAS mutation was not
associated with low PCR rate and tumor degradation following
neoadjuvant treatment of LARC; however, the KRAS mutation was
associated with low survival rate following NCRT, suggesting a poor
prognosis. In another study, Peng et al (85) retrospectively analyzed 70 patients
with LARC who received NCRT prior to surgery at the Cancer Center
of Sun Yat-Sen University (Guangzhou, China). It was concluded that
the 3-year disease-free survival rate and the 3-year overall
survival rate were lower in patients with the KRAS mutation gene
than in patients who did not have the mutation. In addition, the
response to preoperative radiotherapy and chemotherapy was worse in
patients with the KRAS mutation compared with that in patients who
did not have the mutation. Therefore, the detection of the KRAS
mutation is of great importance for clinicians to predict the
response to NCRT and determine the prognosis.
At present, the methods for detecting the KRAS
mutation are mainly based on tumor biopsy specimens or surgical
resection specimens, and are performed following surgery. This has
several disadvantages, including invasiveness, complexity and high
cost, and the quality of the specimens may not be guaranteed. If
the gene mutation could be detected by radiomics prior to surgery,
it would save on medical resources, relieve the distress of the
patients and more importantly, provide effective prognostic
indicators. Different molecular subtypes of rectal cancer often
have different morphological features (86). In recent years, various MRI
sequences (i.e. diffusion-weighted MRI, routine MRI, dynamic
contrast-enhanced MRI and MR spectroscopy) have been used to
evaluate the biological characteristics of the tumor and predict
KRAS status (87–89). In particular, radiomics analysis
based on MRI has become a hot topic, as it is a non-invasive method
and can be used to evaluate the heterogeneity within the tumor,
which is difficult to determine using the naked eye (90). Zhang et al (31) established a radiomics model using
MRI prior to NCRT and extracted the image feature X.LL_scaled_std,
which has high predictive performance in predicting the KRAS
mutation prior to NCRT in patients with LARC. Similarly, Oh et
al (91) also confirmed that
T2WI radiomics has high predictive performance for preoperative
KRAS status of rectal cancer. Therefore, MRI-based radiomics
features could effectively predict KRAS mutation prior to NCRT in
patients with LARC, and could be used to evaluate treatment
response and determine prognosis. However, this still requires
further verification using a large multicenter cohort and
prospective trials. If applied to clinical decision-making, it will
avoid the side effects of radiotherapy and chemotherapy, and
provide a non-invasive treatment for targeted therapy.
Current research provides clinical prospects
regarding radiomics; however, there are still certain shortcomings.
Firstly, due to the complexity of establishing the workflow of
radiomics, the image acquisition and protocols of the different
institutions vary. In addition, there are also differences among
various scanning instruments, including in the standardization of
the signal intensity and how the image data should be shared from
different medical institutions, which requires resolving. Secondly,
most radiomics features are extracted from the maximum
cross-sectional area of the tumor, rather than the whole tumor.
This information may not be representative of all the tumor
information. Thirdly, the ROI is mainly determined manually, which
is time-consuming and laborious, and depends on the experience of
the examiner, resulting in the reduction of repeatability.
Fourthly, a large number of radiomics models have poor
reproducibility, are mostly retrospective studies and lack
independent external verification. Finally, there is still a lack
of large sample, multi-center and prospective studies (26,50,92–96).
If the aforementioned problems can be solved, it
will lay a solid foundation for the realization of personalized
medicine. Until now, most studies have only used single-modality
imaging methods, such as CT, MRI and PET. It has been reported that
a multi-modality radiomics model has higher prediction efficiency
compared with that for a single-modality radiomics model. Li et
al (97) combined the two
imaging modalities of CT and MRI to establish a radiomics model,
while comparing it with separate CT or MRI models. It was concluded
that the multi-modality radiomics model was more accurate in
predicting the treatment response to NCRT. In another study
combining 18F-fluorodeoxyglucose PET and MRI radiomics,
the combined model had higher predictive value in predicting the
NCRT response in patients with LARC compared with that for the MRI
model alone (98). There are also
reports showing that the multi-parameter MRI radiomics model had
higher accuracy compared with that of the single-sequence
radiohistology model. In a study using a multi-parameter MRI (T1WI,
T2WI, diffusion-weighted and contrast-enhanced T1WI) radiomics
model, a multi-parameter prediction model and four single-sequence
prediction models were established. It was concluded that the
multi-parameter prediction model had more potential in predicting
unresponsive patients following NCRT in patients with LARC
(62). The studies by Cui et
al (54,99) also showed similar results. In
addition, the multi-parameter MRI radiomics model had more
potential in predicting the response to NCRT in patients with LARC.
It has also been reported that a multi-regional radiomics model
could improve the predictive effectiveness of the model. Liu et
al (100) combined
multi-regional (tumor and mesorectum) MRI radiomics features with
clinical data to build a model, which effectively improved the rate
of predicting lymph node metastasis in rectal cancer.
In recent years, a new artificial intelligence
method, known as deep learning, has also emerged. Deep learning is
a machine learning algorithm characterized by a neural network,
which can be used in image classification, object detection,
computer vision, speech recognition and natural language
processing. Compared with radiomics, it does not require image
segmentation and intermediate feature extraction (101). Deep learning has been applied to
numerous aspects of medical image analysis, such as image
acquisition, image rectification and image classification (102). In the future, if radiomics can be
combined with deep learning or machine learning methods to build a
higher performance model, they may create a new field of
personalized imaging medicine (102–104). At the same time, if a powerful
and easy to use software was developed to obtain the ROI of the
tumor, and semi-automatic or even full-automatic segmentation could
be used, it would also save on medical resources.
In summary, radiomics provides new ideas and
valuable data for clinical practice. MRI-based radiomics can
predict the response and prognosis in patients with LARC to NCRT
using PCR determination, the lymph node status and the KRAS
mutation status. However, there are still some limitations and
challenges in its application in clinical practice. In the future,
analyses from multi-parameter, multi-modality and multi-regional
radiomics may lead to improvements in the results. Radiomics may
also be combined with machine learning methods, such as deep
learning, to improve the predictive value. With the development of
technology and medicine, radiomics has great potential as an
imaging biomarker for predicting treatment response and determining
prognosis, and could be used to assist clinical
decision-making.
Not applicable.
This study was supported by the Sichuan Science and Technology
Program (grant no. 2021YFG0320 and 2020YJ0446).
Not applicable.
BT and JL designed the study and revised the
manuscript. SZ and MY performed the literature research, analyzed
the data, and drafted and wrote the final version of the
manuscript. DC and PL participated in the conception of the study.
All the authors read and approved the final manuscript. Data
authentication is not applicable.
This study has been approved by the Ethics Committee
of Sichuan Cancer Hospital (Chengdu, China; approval no.
SCCHEC-02-2020-008).
The authors declare that they have no competing
interests.
|
1
|
Gabriel E, Ostapoff K, Attwood K,
Al-Sukhni E, Boland P and Nurkin S: Disparities in the age-related
rates of colorectal cancer in the United States. Am Surg.
83:640–647. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Glynne-Jones R, Wyrwicz L, Tiret E, Brown
G, Rödel C, Cervantes A and Arnold D; ESMO Guidelines Committee, :
Rectal cancer: ESMO clinical practice guidelines for diagnosis,
treatment and follow-up. Ann Oncol. 28 (Suppl_4):iv22–iv40. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Siegel RL, Miller KD, Goding Sauer A,
Fedewa SA, Butterly LF, Anderson JC, Cercek A, Smith RA and Jemal
A: Colorectal cancer statistics, 2020. CA Cancer J Clin.
70:145–164. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ferlay J, Colombet M, Soerjomataram I,
Dyba T, Randi G, Bettio M, Gavin A, Visser O and Bray F: Cancer
incidence and mortality patterns in Europe: Estimates for 40
countries and 25 major cancers in 2018. Eur J Cancer. 103:356–387.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bigness A, Imanirad I, Sahin IH, Xie H,
Frakes J, Hoffe S, Laskowitz D and Felder S: Locally advanced
rectal adenocarcinoma: Treatment sequences, intensification, and
rectal organ preservation. CA Cancer J Clin. 71:198–208. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wei J, Huang R, Guo S, Zhang X, Xi S, Wang
Q, Chang H, Wang X, Xiao W, Zeng Z and Gao Y: ypTNM category
combined with AJCC tumor regression grade for screening patients
with the worst prognosis after neoadjuvant chemoradiation therapy
for locally advanced rectal cancer. Cancer Manag Res. 10:5219–5225.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Edge SB and Compton CC: The American Joint
Committee on Cancer: The 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cercek A, Roxburgh CSD, Strombom P, Smith
JJ, Temple LKF, Nash GM, Guillem JG, Paty PB, Yaeger R, Stadler ZK,
et al: Adoption of total neoadjuvant therapy for locally advanced
rectal cancer. JAMA Oncol. 4:e1800712018. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Conroy T, Bosset JF, Etienne PL, Rio E,
François É, Mesgouez-Nebout N, Vendrely V, Artignan X, Bouché O,
Gargot D, et al: Neoadjuvant chemotherapy with FOLFIRINOX and
preoperative chemoradiotherapy for patients with locally advanced
rectal cancer (UNICANCER-PRODIGE 23): A multicentre, randomised,
open-label, phase 3 trial. Lancet Oncol. 22:702–715. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Li Y, Wang J, Ma XW, Tan L, Yan Y, Xue C,
Hui B, Liu R, Ma H and Ren J: A Review of neoadjuvant
chemoradiotherapy for locally advanced rectal cancer. Int J Biol
Sci. 12:1022–1031. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cunningham D, Atkin W, Lenz HJ, Lynch HT,
Minsky B, Nordlinger B and Starling N: Colorectal cancer. Lancet.
375:1030–1047. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Roh MS, Colangelo LH, O'Connell MJ,
Yothers G, Deutsch M, Allegra CJ, Kahlenberg MS, Baez-Diaz L,
Ursiny CS, Petrelli NJ and Wolmark N: Preoperative multimodality
therapy improves disease-free survival in patients with carcinoma
of the rectum: NSABP R-03. J Clin Oncol. 27:5124–5130. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sun Z, Adam MA, Kim J, Turner MC, Fisher
DA, Choudhury KR, Czito BG, Migaly J and Mantyh CR: Association
between neoadjuvant chemoradiation and survival for patients with
locally advanced rectal cancer. Colorectal Dis. 19:1058–1066. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Park IJ, You YN, Agarwal A, Skibber JM,
Rodriguez-Bigas MA, Eng C, Feig BW, Das P, Krishnan S, Crane CH, et
al: Neoadjuvant treatment response as an early response indicator
for patients with rectal cancer. J Clin Oncol. 30:1770–1776. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ravenda P, Gregato G, Rotundo M, Frassoni
S, Dell'Acqua V, Trovato C, Petz W, Rafaniello Raviele P, Bagnardi
V, Bertolini F, et al: Predictive value of circulating
tumor-derived DNA (ctDNA) in patients with locally advanced rectal
cancer (LARC) treated with neoadjuvant chemoradiotherapy (CT-RT):
Preliminary results. Ann Oncol. 29:V852018. View Article : Google Scholar
|
|
16
|
do Canto LM, Barros-Filho MC, Rainho CA,
Marinho D, Kupper BEC, Begnami MDFS, Scapulatempo-Neto C, Havelund
BM, Lindebjerg J, Marchi FA, et al: Comprehensive Analysis of DNA
methylation and prediction of response to Neoadjuvanttherapy in
locally advanced rectal cancer. Cancers (Basel). 12:30792020.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Timudom K, Akaraviputh T,
Chinswangwatanakul V, Pongpaibul A, Korpraphong P, Petsuksiri J,
Ithimakin S and Trakarnsanga A: Predictive significance of cancer
related-inflammatory markers in locally advanced rectal cancer.
World J Gastrointest Surg. 12:390–396. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Vuijk FA, van de Water C, Lent-van Vliet
S, van der Valk MJM, Simmer F, van de Velde CJH, Vahrmeijer AL,
Nagtegaal ID and Hilling DE: Intra-Tumoral genomic heterogeneity in
rectal cancer: Mutational status is dependent on preoperative
biopsy depth and location. Cancers (Basel). 13:22712021. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Davnall F, Yip CS, Ljungqvist G, Selmi M,
Ng F, Sanghera B, Ganeshan B, Miles KA, Cook GJ and Goh V:
Assessment of tumor heterogeneity: An emerging imaging tool for
clinical practice? Insights Imaging. 3:573–589. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Greenbaum A, Martin DR, Bocklage T, Lee
JH, Ness SA and Rajput A: Tumor heterogeneity as a predictor of
response to neoadjuvant chemotherapy in locally advanced rectal
cancer. Clin Colorectal Cancer. 18:102–109. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bundschuh RA, Dinges J, Neumann L,
Seyfried M, Zsótér N, Papp L, Rosenberg R, Becker K, Astner ST,
Henninger M, et al: Textural parameters of tumor heterogeneity in
18F-FDG PET/CT for therapy response assessment and
prognosis in patients with locally advanced rectal cancer. J Nucl
Med. 55:891–897. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lambin P, Rios-Velazquez E, Leijenaar R,
Carvalho S, van Stiphout RG, Granton P, Zegers CM, Gillies R,
Boellard R, Dekker A and Aerts HJ: Radiomics: Extracting more
information from medical images using advanced feature analysis.
Eur J Cancer. 48:441–446. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Aerts HJ, Velazquez ER, Leijenaar RT,
Parmar C, Grossmann P, Carvalho S, Bussink J, Monshouwer R,
Haibe-Kains B, Rietveld D, et al: Decoding tumour phenotype by
noninvasive imaging using a quantitative radiomics approach. Nat
Commun. 5:40062014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gillies RJ, Kinahan PE and Hricak H:
Radiomics: Images are more than pictures, they are data. Radiology.
278:563–577. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kiessling F: The changing face of cancer
diagnosis: From computational image analysis to systems biology.
Eur Radiol. 28:3160–3164. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lambin P, Leijenaar RTH, Deist TM,
Peerlings J, de Jong EEC, van Timmeren J, Sanduleanu S, Larue RTHM,
Even AJG, Jochems A, et al: Radiomics: The bridge between medical
imaging and personalized medicine. Nat Rev Clin Oncol. 14:749–762.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bi WL, Hosny A, Schabath MB, Giger ML,
Birkbak NJ, Mehrtash A, Allison T, Arnaout O, Abbosh C, Dunn IF, et
al: Artificial intelligence in cancer imaging: Clinical challenges
and applications. CA Cancer J Clin. 69:127–157. 2019.PubMed/NCBI
|
|
28
|
Larue RT, Defraene G, De Ruysscher D,
Lambin P and van Elmpt W: Quantitative radiomics studies for tissue
characterization: A review of technology and methodological
procedures. Br J Radiol. 90:201606652017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Liang C, Cheng Z, Huang Y, He L, Chen X,
Ma Z, Huang X, Liang C and Liu Z: An MRI-based radiomics classifier
for preoperative prediction of Ki-67 status in breast cancer. Acad
Radiol. 25:1111–1117. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Bulens P, Couwenberg A, Intven M,
Debucquoy A, Vandecaveye V, Van Cutsem E, D'Hoore A, Wolthuis A,
Mukherjee P, Gevaert O and Haustermans K: Predicting the tumor
response to chemoradiotherapy for rectal cancer: Model development
and external validation using MRI radiomics. Radiother Oncol.
142:246–252. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Zhang Z, Shen L, Wang Y, Wang J, Zhang H,
Xia F, Wan J and Zhang Z: MRI Radiomics signature as a potential
biomarker for predicting KRAS status in locally advanced rectal
cancer patients. Front Oncol. 11:6140522021. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Petresc B, Lebovici A, Caraiani C, Feier
DS, Graur F and Buruian MM: Pre-treatment T2-WI based radiomics
features for prediction of locally advanced rectal cancer
non-response to Neoadjuvant chemoradiotherapy: A preliminary study.
Cancers (Basel). 12:18942020. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Chen Q, Xia T, Zhang M, Xia N, Liu J and
Yang Y: Radiomics in stroke neuroimaging: Techniques, applications,
and challenges. Aging Dis. 12:143–154. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Fornacon-Wood I, Faivre-Finn C, O'Connor
JPB and Price GJ: Radiomics as a personalized medicine tool in lung
cancer: Separating the hope from the hype. Lung Cancer.
146:197–208. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Gardin I, Gregoire V, Gibon D, Kirisli H,
Pasquier D, Thariat J and Vera P: Radiomics: Principles and
radiotherapy applications. Crit Rev Oncol Hematol. 138:44–50. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Bogowicz M, Vuong D, Huellner MW, Pavic M,
Andratschke N, Gabrys HS, Guckenberger M and Tanadini-Lang S: CT
radiomics and PET radiomics: Ready for clinical implementation? Q J
Nucl Med Mol Imaging. 63:355–370. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Hood L and Friend SH: Predictive,
personalized, preventive, participatory (P4) cancer medicine. Nat
Rev Clin Oncol. 8:184–187. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Pickhardt PJ: Recent developments in
colorectal imaging. Curr Opin Gastroenterol. 31:76–80. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Rutegard MK, Batsman M, Axelsson J,
Brynolfsson P, Brännström F, Rutegård J, Ljuslinder I, Blomqvist L,
Palmqvist R, Rutegård M and Riklund K: PET/MRI and PET/CT hybrid
imaging of rectal cancer-description and initial observations from
the RECTOPET (REctal Cancer trial on PET/MRI/CT) study. Cancer
Imaging. 19:522019. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Raman SP, Chen Y and Fishman EK: Evolution
of imaging in rectal cancer: Multimodality imaging with MDCT, MRI,
and PET. J Gastrointest Oncol. 6:172–184. 2015.PubMed/NCBI
|
|
41
|
Gal O, Feldman D, Mari A, Baker FA, Hebron
D and Kopelman Y: Computerized tomography criteria as a tool for
simplifying the assessment of locally advanced rectal cancer. J
Gastrointest Cancer. 51:130–134. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Rymer B, Curtis NJ, Siddiqui MR and Chand
M: FDG PET/CT can assess the response of locally advanced rectal
cancer to Neoadjuvant chemoradiotherapy: Evidence from
meta-analysis and systematic review. Clin Nucl Med. 41:371–375.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Avallone A, Aloj L, Pecori B, Caracò C, De
Stefano A, Tatangelo F, Silvestro L, Granata V, Bianco F, Romano C,
et al: 18F-FDG PET/CT is an early predictor of
pathologic tumor response and survival after preoperative
radiochemotherapy with bevacizumab in high-risk locally advanced
rectal cancer. J Nucl Med. 60:1560–1568. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Schmidt G: Importance of whole body MRI
for staging of colorectal cancer. Radiologe. 52:537–544. 2012.(In
German). View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Georgiou PA, Tekkis PP, Constantinides VA,
Patel U, Goldin RD, Darzi AW, John Nicholls R and Brown G:
Diagnostic accuracy and value of magnetic resonance imaging (MRI)
in planning exenterative pelvic surgery for advanced colorectal
cancer. Eur J Cancer. 49:72–81. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Jhaveri KS and Hosseini-Nik H: MRI of
rectal cancer: An overview and update on recent advances. AJR Am J
Roentgenol. 205:W42–W55. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Klessen C, Rogalla P and Taupitz M: Local
staging of rectal cancer: The current role of MRI. Eur Radiol.
17:379–389. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Attenberger UI, Pilz LR, Morelli JN,
Hausmann D, Doyon F, Hofheinz R, Kienle P, Post S, Michaely HJ,
Schoenberg SO and Dinter DJ: Multi-parametric MRI of rectal
cancer-do quantitative functional MR measurements correlate with
radiologic and pathologic tumor stages? Eur J Radiol. 83:1036–1043.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Xu Q, Xu Y, Sun H, Jiang T, Xie S, Ooi BY
and Ding Y: MRI evaluation of complete response of locally advanced
rectal cancer after Neoadjuvant therapy: Current status and future
trends. Cancer Manag Res. 13:4317–4328. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Yi X, Pei Q, Zhang Y, Zhu H, Wang Z, Chen
C, Li Q, Long X, Tan F, Zhou Z, et al: MRI-Based radiomics predicts
tumor response to neoadjuvant chemoradiotherapy in locally advanced
rectal cancer. Front Oncol. 9:5522019. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Mirbagheri N, Kumar B, Deb S, Poh BR, Dark
JG, Leow CC and Teoh WM: Lymph node status as a prognostic
indicator after preoperative Neoadjuvant chemoradiotherapy of
rectal cancer. Colorectal Dis. 16:O339–O346. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Cai C, Hu T, Gong J, Huang D, Liu F, Fu C
and Tong T: Multiparametric MRI-based radiomics signature for
preoperative estimation of tumor-stroma ratio in rectal cancer. Eur
Radiol. 31:3326–3335. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
De Cecco CN, Ganeshan B, Ciolina M, Rengo
M, Meinel FG, Musio D, De Felice F, Raffetto N, Tombolini V and
Laghi A: Texture analysis as imaging biomarker of tumoral response
to Neoadjuvant chemoradiotherapy in rectal cancer patients studied
with 3-T magnetic resonance. Invest Radiol. 50:239–245. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Cui Y, Yang W, Ren J, Li D, Du X, Zhang J
and Yang X: Prognostic value of multiparametric MRI-based radiomics
model: Potential role for chemotherapeutic benefits in locally
advanced rectal cancer. Radiother Oncol. 154:161–169. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Kapiteijn E, Marijnen CA, Nagtegaal ID,
Putter H, Steup WH, Wiggers T, Rutten HJ, Pahlman L, Glimelius B,
van Krieken JH, et al: Preoperative radiotherapy combined with
total mesorectal excision for resectable rectal cancer. N Engl J
Med. 345:638–646. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Chetty R, Gill P, Govender D, Bateman A,
Chang HJ, Deshpande V, Driman D, Gomez M, Greywoode G, Jaynes E, et
al: International study group on rectal cancer regression grading:
Interobserver variability with commonly used regression grading
systems. Hum Pathol. 43:1917–1923. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Bahadoer RR, Dijkstra EA, van Etten B,
Marijnen CAM, Putter H, Kranenbarg EM, Roodvoets AGH, Nagtegaal ID,
Beets-Tan RGH, Blomqvist LK, et al: Short-course radiotherapy
followed by chemotherapy before total mesorectal excision (TME)
versus preoperative chemoradiotherapy, TME, and optional adjuvant
chemotherapy in locally advanced rectal cancer (RAPIDO): A
randomised, open-label, phase 3 trial. Lancet Oncol. 22:29–42.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Smith JJ, Strombom P, Chow OS, Roxburgh
CS, Lynn P, Eaton A, Widmar M, Ganesh K, Yaeger R, Cercek A, et al:
Assessment of a watch-and-wait strategy for rectal cancer in
patients with a complete response after Neoadjuvant therapy. JAMA
Oncol. 5:e1858962019. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Maas M, Nelemans PJ, Valentini V, Das P,
Rödel C, Kuo LJ, Calvo FA, García-Aguilar J, Glynne-Jones R,
Haustermans K, et al: Long-term outcome in patients with a
pathological complete response after chemoradiation for rectal
cancer: A pooled analysis of individual patient data. Lancet Oncol.
11:835–844. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Dinapoli N, Barbaro B, Gatta R, Chiloiro
G, Casà C, Masciocchi C, Damiani A, Boldrini L, Gambacorta MA,
Dezio M, et al: Magnetic resonance, vendor-independent, intensity
histogram analysis predicting pathologic complete response after
radiochemotherapy of rectal cancer. Int J Radiat Oncol Biol Phys.
102:765–774. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Li Y, Liu W, Pei Q, Zhao L, Güngör C, Zhu
H, Song X, Li C, Zhou Z, Xu Y, et al: Predicting pathological
complete response by comparing MRI-based radiomics pre- and
postneoadjuvant radiotherapy for locally advanced rectal cancer.
Cancer Med. 8:7244–7252. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Zhou X, Yi Y, Liu Z, Cao W, Lai B, Sun K,
Li L, Zhou Z, Feng Y and Tian J: Radiomics-Based pretherapeutic
prediction of non-response to Neoadjuvant therapy in locally
advanced rectal cancer. Ann Surg Oncol. 26:1676–1684. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Sun Y, Wu X, Lin H, Lu X, Huang Y and Chi
P: Lymph node regression to neoadjuvant chemoradiotherapy in
patients with locally advanced rectal cancer: Prognostic
implication and a predictive model. J Gastrointest Surg.
25:1019–1028. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Okada K, Sadahiro S, Suzuki T, Tanaka A,
Saito G, Kamijo A, Akiba T and Kawada S: Effects of
chemoradiotherapy on lymph nodes in patients with rectal
adenocarcinoma: Evaluation of numbers and sizes of retrieved lymph
nodes inside and outside the radiation field. Anticancer Res.
34:4195–4200. 2014.PubMed/NCBI
|
|
65
|
Lee SH, Lee JL, Kim CW, Lee HI, Yu CS and
Kim JC: Oncologic significance of para-aortic lymph node and
inferior mesenteric lymph node metastasis in sigmoid and rectal
adenocarcinoma. Eur J Surg Oncol. 43:2076–2083. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Kang J, Hur H, Min BS, Kim NK and Lee KY:
Prognostic impact of inferior mesenteric artery lymph node
metastasis in colorectal cancer. Ann Surg Oncol. 18:704–710. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Mei SW, Liu Z, Wang Z, Pei W, Wei FZ, Chen
JN, Wang ZJ, Shen HY, Li J, Zhao FQ, et al: Impact factors of lymph
node retrieval on survival in locally advanced rectal cancer with
neoadjuvant therapy. World J Clin Cases. 8:6229–6242. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Sartori CA, Sartori A, Vigna S, Occhipinti
R and Baiocchi GL: Urinary and sexual disorders after laparoscopic
TME for rectal cancer in males. J Gastrointest Surg. 15:637–643.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Herzog T, Belyaev O, Chromik AM, Weyhe D,
Mueller CA, Munding J, Tannapfel A, Uhl W and Seelig MH: TME
quality in rectal cancer surgery. Eur J Med Res. 15:292–296. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Veenhof AA, Brosens R, Engel AF, van der
Peet DL and Cuesta MA: Risk factors and management of presacral
abscess following total mesorectal excision for rectal cancer. Dig
Surg. 26:317–321. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Yuval JB, Thompson HM and Garcia-Aguilar
J: Organ preservation in rectal cancer. J Gastrointest Surg.
24:1880–1888. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Zhou X, Yi Y, Liu Z, Zhou Z, Lai B, Sun K,
Li L, Huang L, Feng Y, Cao W and Tian J: Radiomics-based
preoperative prediction of lymph node status following neoadjuvant
therapy in locally advanced rectal cancer. Front Oncol. 10:6042020.
View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Marijnen CA: Organ preservation in rectal
cancer: Have all questions been answered? Lancet Oncol. 16:e13–e22.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Langman G, Patel A and Bowley DM: Size and
distribution of lymph nodes in rectal cancer resection specimens.
Dis Colon Rectum. 58:406–414. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Yuan Y, Pu H, Chen GW, Chen XL, Liu YS,
Liu H, Wang K and Li H: Diffusion-weighted MR volume and apparent
diffusion coefficient for discriminating lymph node metastases and
good response after chemoradiation therapy in locally advanced
rectal cancer. Eur Radiol. 31:200–211. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Newton AD, Li J, Jeganathan AN, Mahmoud
NN, Epstein AJ and Paulson EC: A nomogram to predict lymph node
positivity following Neoadjuvant chemoradiation in locally advanced
rectal cancer. Dis Colon Rectum. 59:710–717. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Song L and Yin J: Application of texture
analysis based on sagittal fat-suppression and oblique axial
T2-Weighted magnetic resonance imaging to identify lymph node
invasion status of rectal cancer. Front Oncol. 10:13642020.
View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Lievre A, Bachet JB, Boige V, Cayre A, Le
Corre D, Buc E, Ychou M, Bouché O, Landi B, Louvet C, et al: KRAS
mutations as an independent prognostic factor in patients with
advanced colorectal cancer treated with cetuximab. J Clin Oncol.
26:374–379. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Sorich MJ, Wiese MD, Rowland A,
Kichenadasse G, McKinnon RA and Karapetis CS: Extended RAS
mutations and anti-EGFR monoclonal antibody survival benefit in
metastatic colorectal cancer: A meta-analysis of randomized,
controlled trials. Ann Oncol. 26:13–21. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
George B and Kopetz S: Predictive and
prognostic markers in colorectal cancer. Curr Oncol Rep.
13:206–215. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Dai D, Wang Y, Zhu L, Jin H and Wang X:
Prognostic value of KRAS mutation status in colorectal cancer
patients: A population-based competing risk analysis. Peerj.
8:e91492020. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Zhou P, Goffredo P, Ginader T, Thompson D,
Hrabe J, Gribovskaja-Rupp I, Kapadia M and Hassan I: Impact of KRAS
status on tumor response and survival after Neoadjuvant treatment
of locally advanced rectal cancer. J Surg Oncol. 123:278–285. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Gupta AK, Bakanauskas VJ, Cerniglia GJ,
Cheng Y, Bernhard EJ, Muschel RJ and McKenna WG: The Ras radiation
resistance pathway. Cancer Res. 61:4278–4282. 2001.PubMed/NCBI
|
|
84
|
Toulany M, Dittmann K, Kruger M, Baumann M
and Rodemann HP: Radioresistance of K-Ras mutated human tumor cells
is mediated through EGFR-dependent activation of PI3K-AKT pathway.
Radiother Oncol. 76:143–150. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Peng J, Lin J, Qiu M, Zhao Y, Deng Y, Shao
J, Ding P, Zhang H, Wan D, Lu Z and Pan Z: Oncogene mutation
profile predicts tumor regression and survival in locally advanced
rectal cancer patients treated with preoperative chemoradiotherapy
and radical surgery. Tumour Biol. 39:10104283177096382017.
View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Coppede F, Lopomo A, Spisni R and Migliore
L: Genetic and epigenetic biomarkers for diagnosis, prognosis and
treatment of colorectal cancer. World J Gastroenterol. 20:943–956.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Xu Y, Xu Q, Sun H, Liu T, Shi K and Wang
W: Could IVIM and ADC help in predicting the KRAS status in
patients with rectal cancer? Eur Radiol. 28:3059–3065. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Yeo DM, Oh SN, Choi MH, Lee SH, Lee MA and
Jung SE: Histogram analysis of perfusion parameters from dynamic
contrast-enhanced MR imaging with tumor characteristics and
therapeutic response in locally advanced rectal cancer. Biomed Resm
Int. 2018:37243932018.PubMed/NCBI
|
|
89
|
Meng X, Xia W, Xie P, Zhang R, Li W, Wang
M, Xiong F, Liu Y, Fan X, Xie Y, et al: Preoperative radiomic
signature based on multiparametric magnetic resonance imaging for
noninvasive evaluation of biological characteristics in rectal
cancer. Eur Radiol. 29:3200–3209. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Xu Y, Xu Q, Ma Y, Duan J, Zhang H, Liu T,
Li L, Sun H, Shi K, Xie S and Wang W: Characterizing MRI features
of rectal cancers with different KRAS status. BMC Cancer.
19:11112019. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Oh JE, Kim MJ, Lee J, Hur BY, Kim B, Kim
DY, Baek JY, Chang HJ, Park SC, Oh JH, et al: Magnetic
resonance-based texture analysis differentiating KRAS mutation
status in rectal cancer. Cancer Res Treat. 52:51–59. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Chiloiro G, Rodriguez-Carnero P, Lenkowicz
J, Casà C, Masciocchi C, Boldrini L, Cusumano D, Dinapoli N,
Meldolesi E, Carano D, et al: Delta radiomics can predict distant
metastasis in locally advanced rectal cancer: The challenge to
personalize the cure. Front Oncol. 10:5950122020. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Liu Z, Wang S, Dong D, Wei J, Fang C, Zhou
X, Sun K, Li L, Li B, Wang M and Tian J: The applications of
radiomics in precision diagnosis and treatment of oncology:
Opportunities and challenges. Theranostics. 9:1303–1322. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Mayerhoefer ME, Szomolanyi P, Jirak D,
Materka A and Trattnig S: Effects of MRI acquisition parameter
variations and protocol heterogeneity on the results of texture
analysis and pattern discrimination: An application-oriented study.
Med Phys. 36:1236–1243. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Collewet G, Strzelecki M and Mariette F:
Influence of MRI acquisition protocols and image intensity
normalization methods on texture classification. Magn Reson
Imaging. 22:81–91. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Daye D, Tabari A, Kim H, Chang K, Kamran
SC, Hong TS, Kalpathy-Cramer J and Gee MS: Quantitative tumor
heterogeneity MRI profiling improves machine learning-based
prognostication in patients with metastatic colon cancer. Eur
Radiol. 31:5759–5767. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Li ZY, Wang XD, Li M, Liu XJ, Ye Z, Song
B, Yuan F, Yuan Y, Xia CC, Zhang X and Li Q: Multi-modal radiomics
model to predict treatment response to neoadjuvant chemotherapy for
locally advanced rectal cancer. World J Gastroenterol.
26:2388–2402. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Giannini V, Mazzetti S, Bertotto I,
Chiarenza C, Cauda S, Delmastro E, Bracco C, Di Dia A, Leone F,
Medico E, et al: Predicting locally advanced rectal cancer response
to neoadjuvant therapy with 18F-FDG PET and MRI
radiomics features. Eur J Nucl Med Mol Imaging. 46:878–888. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Cui Y, Yang X, Shi Z, Yang Z, Du X, Zhao Z
and Cheng X: Radiomics analysis of multiparametric MRI for
prediction of pathological complete response to neoadjuvant
chemoradiotherapy in locally advanced rectal cancer. Eur Radiol.
29:1211–1220. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Liu X, Yang Q, Zhang C, Sun J, He K, Xie
Y, Zhang Y, Fu Y and Zhang H: Multiregional-Based magnetic
resonance imaging radiomics combined with clinical data improves
efficacy in predicting lymph node metastasis of rectal cancer.
Front Oncol. 10:5857672021. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Chartrand G, Cheng PM, Vorontsov E,
Drozdzal M, Turcotte S, Pal CJ, Kadoury S and Tang A: Deep
learning: A primer for radiologists. Radiographics. 37:2113–2131.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Parekh VS and Jacobs MA: Deep learning and
radiomics in precision medicine. Expert Rev Precis Med Drug Dev.
4:59–72. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Shi L, Zhang Y, Nie K, Sun X, Niu T, Yue
N, Kwong T, Chang P, Chow D, Chen JH and Su MY: Machine learning
for prediction of chemoradiation therapy response in rectal cancer
using pre-treatment and mid-radiation multi-parametric MRI. Magn
Reson Imaging. 61:33–40. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Zhu HT, Zhang XY, Shi YJ, Li XT and Sun
YS: A deep learning model to predict the response to neoadjuvant
chemoradiotherapy by the pretreatment apparent diffusion
coefficient images of locally advanced rectal cancer. Front Oncol.
10:5743372020. View Article : Google Scholar : PubMed/NCBIPubMed/NCBI
|