Introduction
Mesenchymal tumours are a diverse group of
non-epithelial tumours that originate from connective tissue and
muscle cells, with bladder leiomyomas representing a subtype.
Mesenchymal tumours represent 1-5% of all urinary bladder tumours.
Among these, leiomyomas account for 35% and are the most common
benign mesenchymal tumours in the bladder (1). Bladder leiomyoma is considered rare,
with an incidence rate <0.5% among all types of mesenchymal
bladder tumours (2). To date,
there are only ~250 case reported worldwide (1-3).
Bladder leiomyoma has been reported to be symptomatic more
frequently than asymptomatic at the time of the disease being
clinically suspected, with a proportion of 83 and 16.8 % cases,
respectively (4). Common symptoms
reported by patients include lower urinary tract symptoms,
haematuria, pyuria and acute urinary retention (4). Some patients have also reported
abdominal or back pain which radiates to the left leg (2,4). The
diagnosis of bladder leiomyoma is commonly performed using an
ultrasound, computed tomography (CT) scan, magnetic resonance
imaging (MRI), or cystoscopy (3).
The various symptoms and indistinguishable results from several
imaging techniques render the diagnosis of bladder leiomyoma
challenging.
Given the scarcity of documented cases involving
asymptomatic bladder leiomyomas up until the point of treatment,
the present study describes the case of a middle-aged female
patient who was incidentally diagnosed with asymptomatic bladder
leiomyoma during a routine medical check-up. The present case
report also emphasizes the importance of long-term follow-up and
highlights alternative treatment options for managing bladder
leiomyomas.
Case report
A 55-year-old female patient presented for a routine
medical check-up at Haji Adam Malik General Hospital, Medan,
Sumatera Utara, Indonesia. The overall condition of patient
appeared normal, as determined through a comprehensive physical
examination, complete blood count (CBC), liver function tests,
renal function tests and urinalysis, all of which had values within
the normal reference ranges. The patient denied any changes in
urinary frequency, dysuria, haematuria, or weight loss over the
past year. No issues were reported in bowel movements. The patient
denied a history of smoking, familial bladder tumours, bladder
stones, urinary tract infections, hypertension, diabetes mellitus,
cardiac issues, or previous surgeries.
Laboratory investigations revealed a normal results,
including a complete blood count (haemoglobin, 13.7 g/dl;
leukocytes, 7,310/µl; platelets, 245,000/µl), renal function tests
(urea, 43 mg/dl; creatinine, 0.96 mg/dl), liver function tests
(AST, 29 U/l; ALT, 32 U/l) and urinalysis (clear appearance, pH
6.0, no protein, glucose, or haematuria detected), all within
normal reference ranges. A chest radiography revealed no
abnormalities. An abdominal ultrasonography revealed gallstones and
a mass within the bladder, suspected of a bladder tumour.
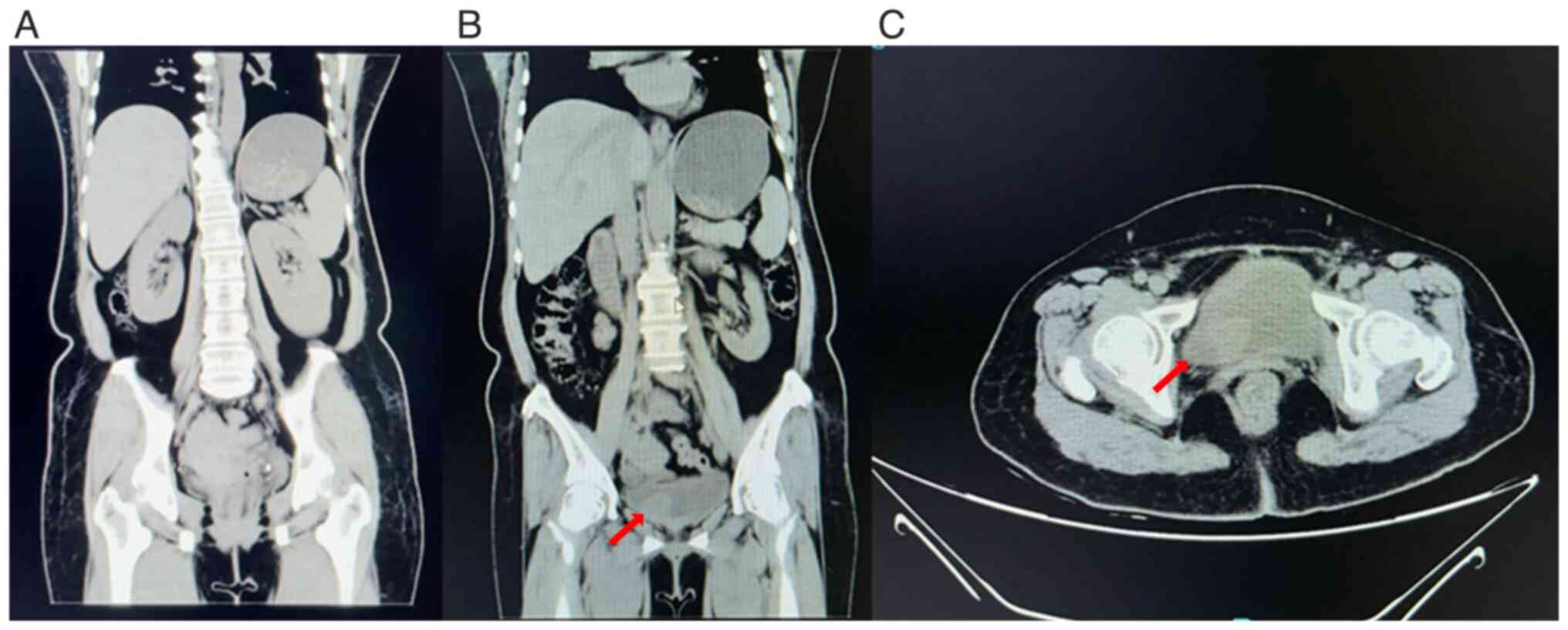
Subsequently, a non-contrast CT scan of the entire abdomen was
performed, which revealed both kidneys to be within normal limits.
An isodense lesion measuring 24x25x21 mm was identified along the
right lateral wall of the bladder (Fig. 1).
The patient was referred to the Department of
Urology at Haji Adam Malik General Hospital, Medan, Sumatera Utara,
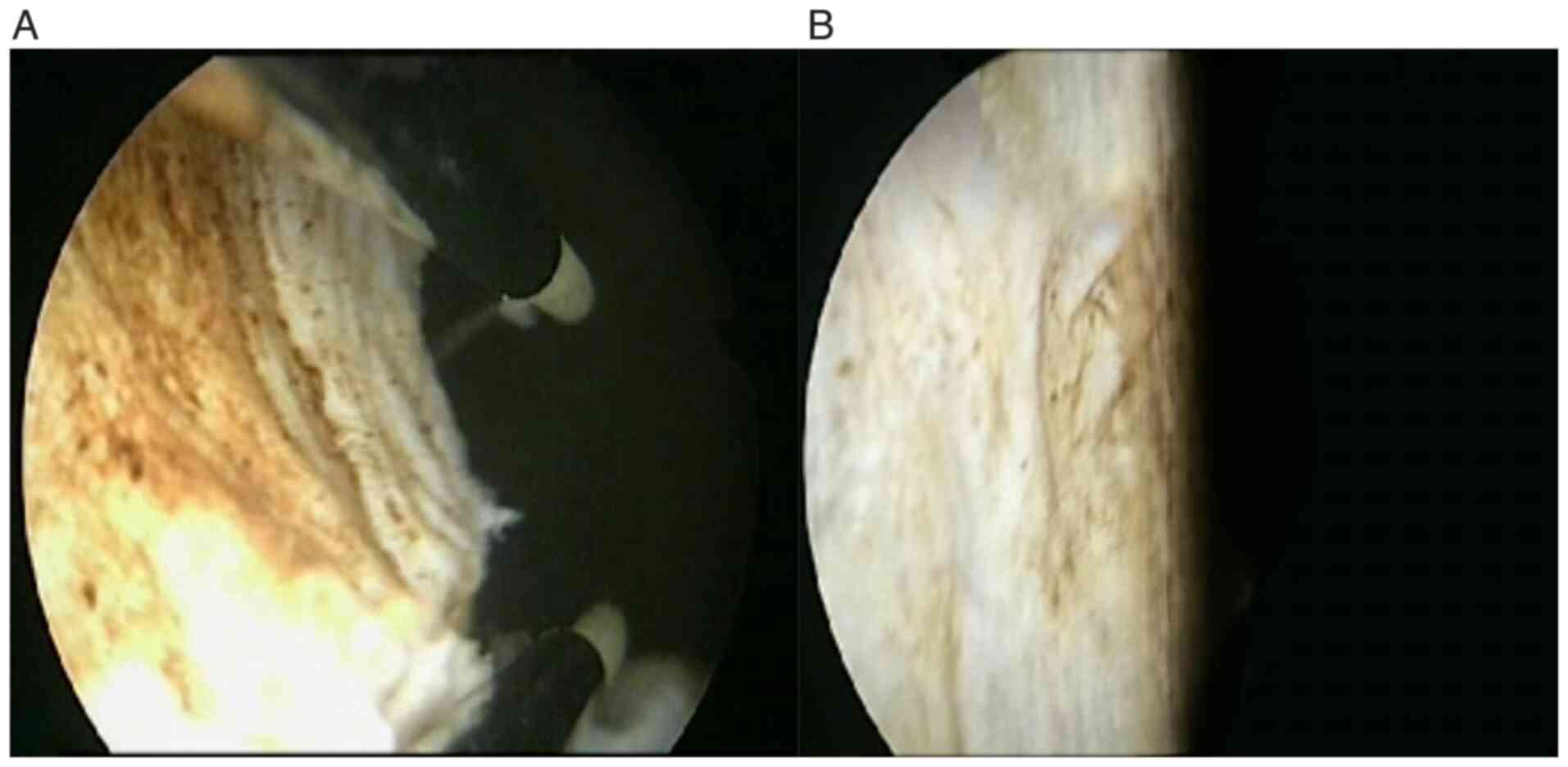
which revealed inflammatory smears in urine cytology. A cystoscopy
was performed, demonstrating non-hyperaemic bladder mucosa, intact
ureteral orifices and no trabeculation, vesiculation, or
diverticula. A mass was observed on the right lateral aspect of the
bladder suspected to be a tumour (Fig.
2). Transurethral resection of the bladder tumour (TURBT) was
then agreed upon. TURBT was preferred in account of the tumour size
being <3 cm, as it is a procedure with a shorter duration, and
is less invasive, therefore improving patient outcomes. No marked
bleeding was encountered during the resection procedure, and the
tumour was completely excised down to its base (Fig. 3).
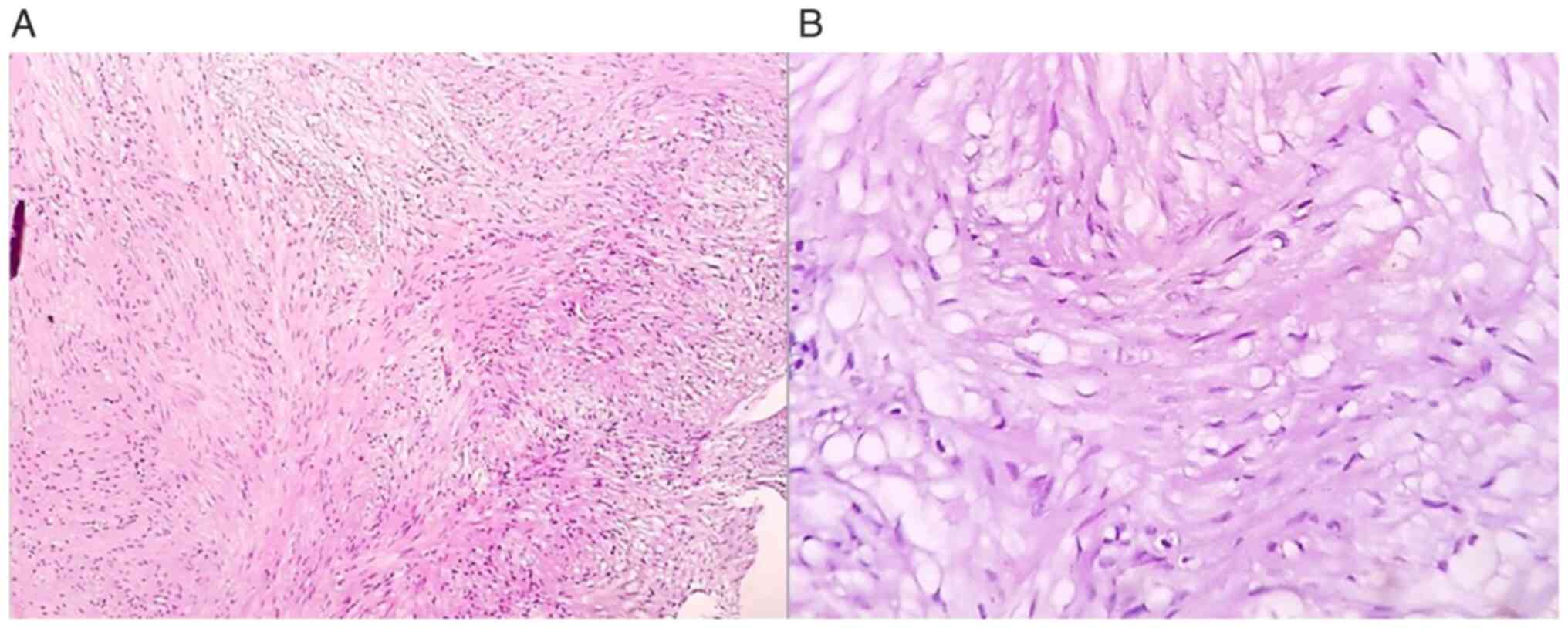
Histopathological analysis of the resected tissue
revealed compact interlacing fascicles of smooth muscle cells
without significant cytological atypia or mitoses, which confirmed
the presence of a bladder leiomyoma (Fig. 4). H&E staining was performed at
the Department of Anatomical Pathology, Haji Adam Malik General
Hospital, Medan, Indonesia. Tissue sections were 4-µm-thick,
formalin-fixed and paraffin-embedded. The specimens were fixed in
10% neutral buffered formalin at room temperature for 24 h.
Haematoxylin and eosin staining was conducted using standard
protocols with commercially available reagents. Haematoxylin
staining utilized Dakewe Biosci Hematoxylin Staining Solution. The
stained slides were examined using a light microscope (Olympus
CX23, Olympus Corporation). The patient was admitted for 2 days
post-operatively without complaints of haematuria or other
complications. The patient was immediately discharged upon
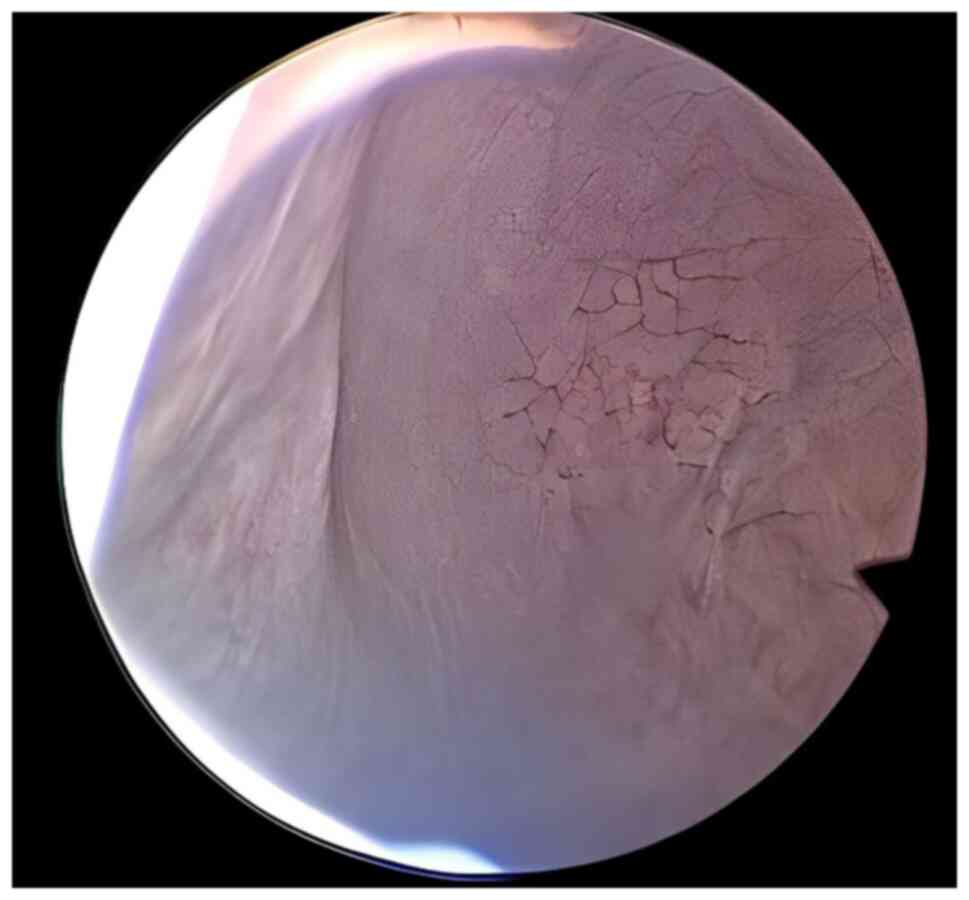
exhibiting no symptoms. Evaluation was carried out using cystoscopy
(Fig. 5) 3 months following TURBT
and revealed that there were tumours in the bladder of the patient;
the patient also did not have any complaints following TURBT.
Discussion
Leiomyoma of the bladder is an infrequent and benign
mesenchymal tumour, accounting for <0.5% of all bladder tumours
(1). Initially, it was considered
to occur in both sexes at a similar rate; however, subsequent
research has revealed that ~70% of cases are found in females. This
tumour primarily affects individuals between 30 and 60 years of
age, and it typically presents with various symptoms, with
obstructive symptoms being the most common (49%), followed by
irritative symptoms (38%) and haematuria (11%) (2). Bladder leiomyomas can be classified
as endovesical, intramural, or extravesical. Among these,
endovesical tumours are the most prevalent and typically manifest
with symptoms such as dysuria, urinary urgency, haematuria, and
occasionally, lower back pain (3).
The aetiology remains unknown as the consequence of its rare
incidence. Tobacco smoking, exposure to substances, such as
arsenic, radiation, any medications such as opium and
chemotherapeutic agents have been reported as significant risk
factors for bladder cancer (5).
However, to the best of our knowledge, there are no reported risk
factors specific to bladder leiomyoma due to its rare incident.
Numerous theories have been put forth in an attempt to elucidate
the origin of leiomyoma as the consequence of its unknown
aetiology. Firstly, Blum's irritative theory posits that chronic
inflammatory factors affecting the bladder wall and detrusor smooth
muscle may be a contributing factor. Secondly, Piegel's
disontogenic theory suggests that these tumours may originate from
embryonic remnants of Muller and Wolffian ducts. Lastly,
Lips-Chutz's theory proposes that leiomyoma development may be
linked to endocrine disturbances, with oestrogen and progesterone
playing pivotal roles in this regard (1).
Bladder leiomyomas often present with atypical
symptoms, leading to misconceptions and misdiagnoses. Numerous case
reports have documented instances where leiomyomas were mistaken
for different conditions, including uterine fibroids (6), ureterocele (7,8),
febrile urinary tract infections (9) and an enlarged prostate gland
(10). However, in a small
percentage of cases, similar to the case presented herein, ~19% of
bladder leiomyomas are incidentally discovered without causing any
noticeable symptoms (2,6).
Typically, patients without symptoms tend to have
tumour sizes measuring ≤3 cm. As highlighted in the study by Erdem
et al (11), a patient
remained asymptomatic until the mass reached 3 cm, underscoring the
close association between the symptoms of bladder leiomyoma and the
location and size of the tumour (11). Przudzik et al (12) documented 3 cases with tumour
diameters <54 mm, most of which were situated away from
anatomical openings. Musayev et al (13) also presented an asymptomatic case
with similar dimensions (20x25x30 mm) and a minimal amount of
surrounding soft tissue, mirroring the characteristics observed in
the case in the present study. This similarity supports the
accurate asymptomatic diagnosis of the case in the present study
(12). Song et al (6) described a case of asymptomatic
leiomyoma characterized by only microhaematuria, suggesting the
importance of obtaining a thorough medical history of the patient
prior to performing any invasive procedures or examinations.
The diagnosis of bladder leiomyomas involves several
diagnostic modalities, such as cystoscopy, ultrasonography, CT
scans, or MRI; however, the definitive confirmation relies on a
histopathological examination (11-13).
Cystoscopy findings can help differentiate between intramural and
endovesical leiomyomas (11). In
terms of diagnostic accuracy for leiomyomas located in the bladder
floor, a comparison among intravenous urography (IVU), voiding
cysto-urethrogram, transabdominal ultrasonography, CT scans and
transvaginal ulstrasound has revealed that transvaginal ulstrasound
provides the most precise information regarding the location of the
mass and its association with neighbouring organs. Nevertheless, it
is worth noting that three-dimensional CT scans and MRI are
preferred over ulstrasound for their enhanced assessment of
delineation planes and the sites of origin (2).
Radiologically, bladder leiomyomas can be mistakenly
identified as various other urinary bladder tumours, cystocele,
ureterocele, uterine fibroids and pelvic masses (7). Macroscopically, leiomyomas exhibit
well-defined borders and thin capsules, presenting as solid masses
with a yellow-coloured sectional surface. Under microscopic
examination, leiomyomas consist of intersecting smooth muscle
fascicles surrounding vascular structures lined with normal
endothelium and arranged as bundles extending in various directions
(1). Histological analysis
typically reveals the absence of necrosis, cellular atypia, or
mitotic activity (8).
MRI, as one of the imaging modalities, is more
sensitive compared to CT scan and ultrasonography (USG) in
distinguishing leiomyoma with leiomyosarcoma and bladder
paraganglioma. Leiomyosarcoma typically presents as large, polypoid
masses, usually near the bladder dome. Distinguishing it from a
bladder leiomyoma can be challenging, as both lesions often exhibit
hypo-intensity on T2-weighted MRI. However, features such as poorly
defined borders, invasion into adjacent structures and necrotic
areas can help differentiate leiomyosarcoma from leiomyoma. Testing
for diffusion restriction also assists in distinguishing bladder
leiomyosarcomas from bladder leiomyomas (4). According to Hu et al (14), quantitative MRI can effectively
differentiate bladder paraganglioma from bladder leiomyoma by
evaluating the signal intensity-ratio on T1-weighted imaging (T1WI)
or the ADC value.
The management of leiomyoma primarily involves
surgical intervention, with the choice of approach contingent upon
factors, such as tumour location, size, and its proximity to the
bladder wall. In the majority of instances, the preferred method is
transurethral (1-3).
Given the benign nature of these lesions, the surgical approach
should be as conservative as possible. Available treatment options
encompass transurethral resection and open surgical procedures like
enucleation or partial cystectomy (1). Similar to the case in the present
study, the majority of cases have been successfully managed through
TURBT (1,2,6,7,9,15).
Nonetheless, in select and exceptional cases, specialized
procedures have been developed, such as vaginal resection for
bladder leiomyoma. Additionally, minimally invasive techniques,
such as laparoscopic cystotomy, robotic extramucosal excision, or
transvesical laparoscopy can also be considered as suitable
alternatives (1,16). Minimally invasive techniques
benefit patients in terms of a shorter duration of hospitalization
compared to open surgery approaches (4).
Regular follow-up appointments are crucial in the
management of leiomyomas, and it is noteworthy that reoperation
rates are relatively low in these cases (12). Previous research has revealed that
follow-ups on reported cases have yielded no indications of
recurrence even up to 20 years post-surgery, or any malignant
transformations (11). Of note, 3
cases of bladder leiomyoma recurrence were reported by Park et
al (17) and Yogeeta et
al (18); 2 patients underwent
repeat TURBT and 1 patient underwent enucleation procedure as
tumour recurrence management. There was no report of complications
related to the procedures in these cases. Incomplete resection was
considered to be the cause of recurrences, considering the fact
that the tumours were located near the urethral orifice, causing
fear of sphincteric or urethral injury (17,18).
Therefore, achieving complete resection has been proven to be an
effective and essential approach to prevent recurrence (6,17,18).
As previously demonstrated, 3-month follow-ups following TURBT
generally show favourable outcomes. In their study, Sodo et
al (19) performed a CT scan,
USG and peak flow measurements for the follow-up of a patient
post-TURBT. At 3 and 9 months, they found negative tumour
recurrence and the peak and average flows were 21 and 10 ml/min,
respectively. The voided volume was 198 ml at 3 months and at 9
months, this increased at 296 ml (19). In the study by Yoshioka et
al (20), a 3 month follow-up
examination of a cystoscope-assisted laparoscopic enucleation of a
large-sized leiomyoma of the urinary bladder revealed no
recurrence. In addition, the studies by He et al (21) and Mitchell et al (22) revealed no recurrence even after at
least 6 months of follow-up. However, in the study by Yucel et
al (23), the patient had left
side and back abdominal pain; thus, a CT scan was performed. The CT
scan revealed a tumour formation of 6x3.5 cm extending from the
left lateral wall to the anterior wall of the bladder. The CT scan
also revealed grade 3 left hydroureteronephrosis. As a result, the
patient underwent reoperation. Therefore, despite the mostly
satisfying outcome, there also a small chance of tumour recurrence
and the need for a reoperation following TURBT (23). This is in line with the case report
conducted by Goktug et al (24), where in patients with bladder
leiomyoma who underwent TURBT, there was no recurrence with
evaluation using cystocopy at 6 months post-operatively.
In conclusion, the present case report highlights
the rarity of bladder leiomyoma, a benign mesenchymal bladder
tumour. The accurate diagnosis of this condition can be
challenging, and it is often mistaken for other urinary bladder
tumours or pelvic masses. Diagnostic modalities, including
cystoscopy and imaging techniques, aid in confirming the diagnosis;
however, a histopathological examination remains the definitive
confirmation method. The preferred treatment approach is usually
transurethral resection, and in a number of cases, this minimally
invasive technique has been successful. The case described herein
underscores the importance of sharing case reports to enhance
understanding of cases with atypical presentations.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
SMW, KAWY and CTM are surgeons, and they contributed
to data acquisition. SMW, KAWY and CTM wrote the initial draft of
the manuscript. SMW provided advice and supervision, and was
involved in the revision of the manuscript. MHW assisted in the
examination of the patient's specimens. SMW, KAWY, CTM and MHW
confirm the authenticity of all the raw data. All authors have read
and approved the final manuscript.
Ethics approval and consent to
participate
Written informed consent for participation in the
present study was obtained from the patient.
Patient consent for publication
Written informed consent for publication for the
present case report and all associated images was obtained from the
patient.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Zachariou A, Filiponi M, Dimitriadis F,
Kaltsas A and Sofikitis N: Transurethral resection of a bladder
trigone leiomyoma: A rare case report. BMC Urol.
20(152)2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Khater N and Sakr G: Bladder leiomyoma:
Presentation, evaluation and treatment. Arab J Urol.
11(54)2013.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Mendes JE, Ferreira AV, Coelho SA and Gil
C: Bladder leiomyoma. Urol Ann. 9:275–277. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Prihadi JC, Hengky A, Lionardi SK and
Haruman SP: Characteristics and outcomes in bladder Leiomyoma
management: A systematic review of case reports and case series
from the past 20 years. BMC Urol. 24(252)2024.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Jubber I, Ong S, Bukavina L, Black PC,
Compérat E, Kamat AM, Kiemeney L, Lawrentschuk N, Lerner SP, Meeks
JJ, et al: Epidemiology of bladder cancer in 2023: A systematic
review of risk factors. Eur Urol. 84:176–190. 2023.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Song J, Song H and Kim YW: Recurrent
atypical leiomyoma in bladder trigone, confused with uterine
fibroids: A case report. World J Clin Cases.
10(10728)2022.PubMed/NCBI View Article : Google Scholar
|
|
7
|
AlAmri N, Abdullah H, AlIbrahim F, Eid K
and AlShehri M: Imaging findings of atypical leiomyoma of urinary
bladder simulating ureterocele. J Surg Case Rep.
2022(rjac256)2022.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Grice P, O'Dowd S, Parkinson R and Bazo A:
Bladder leiomyoma masquerading as a ureterocele. BMJ Case Rep.
14(242866)2021.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Haddad RG and Murshidi MM, Abu Shahin N
and Murshidi MM: Leiomyoma of urinary bladder presenting with
febrile urinary tract infection: A case report. Int J Surg Case
Rep. 27:180–182. 2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Itam S, Elhage O and Khan MS: Large
leiomyoma of the bladder masquerading as an enlarged prostate
gland. BMJ Case Rep. 2016(bcr2015212800)2016.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Erdem H, Yildirim U, Tekin A, Kayikci A,
Uzunlar AK and Sahiner C: Leiomyoma of the urinary bladder in
asymptomatic women. Urol Ann. 4:172–174. 2012.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Przudzik M, Derkaczew M, Łesiów M and
Roslan M: Asymptomatic bladder leiomyoma: A report of three cases
treated with minimal invasive techniques and a review of
literature. Onco Review. 12:59–64. 2022.
|
|
13
|
Musayev J, Bagirov A, Hasanov A and
Mammadov E: An asymptomatic intramural leiomyoma of bladder in male
patient. Austin J Urol. 1(3)2014.
|
|
14
|
Hu X, Wang K, Sun M, Li C, Wang H and Guan
J: Quantitative MRI in distinguishing bladder paraganglioma from
bladder leiomyoma. Abdom Radiol (NY). 48:1051–1061. 2023.PubMed/NCBI View Article : Google Scholar
|
|
15
|
AlHalak R, Alkabbani S, Nasseif H, Oghanna
N and Janahi F: Bladder leiomyoma treated with transurethral
resection of bladder tumor (TURBT): Case report. Int J Surg Case
Rep. 98(107464)2022.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Rey Valzacchi GM, Pavan LI, Bourguignon
GA, Cortez JP, Ubertazzi EP and Saadi JM: Transvesical laparoscopy
for bladder leiomyoma excision: A novel surgical technique. Int
Urogynecol J. 32:2543–2544. 2021.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Park JW, Jeong BC, Seo SI, Jeon SS, Kwon
GY and Lee HM: Leiomyoma of the urinary bladder: A series of nine
cases and review of the literature. Urology. 76:1425–1429.
2010.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Yogeeta F, Malik Z, Rauf SA, Devi M, Tooba
F, Jamalvi SA, Rashid M and Erum H: Recurrent bladder leiomyoma: A
case report. J Med Case Rep. 18(173)2024.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Sodo M, Spirito L, La Rocca R, Bracale U
and Imbimbo C: Partial cystectomy in young male for a urachal tumor
masquerading a bladder leiomyoma. Arch Ital Urol Androl. 91:51–52.
2019.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Yoshioka T, Kawakita M and Kameoka H:
Cystoscope-assisted laparoscopic enucleation of a large progressive
bladder leiomyoma. J Endourol Case Rep. 5:120–123. 2019.PubMed/NCBI View Article : Google Scholar
|
|
21
|
He L, Li S, Zheng C and Wang C: Rare
symptomatic bladder leiomyoma: Case report and literature review. J
Int Med Res. 46:1678–1684. 2018.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Mitchell K, Barnard J and Luchey A:
Locally recurrent leiomyoma of the bladder refractory to visually
complete transurethral resection: An indication for
cystoprostatectomy. Case Rep Urol. 2019(1086575)2019.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Yucel C, Budak S, Kisa E, Celik O and
Kozacioglu Z: The rare togetherness of bladder leiomyoma and
neurofibromatosis. Case Rep Urol. 2018(2302918)2018.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Goktug GH, Ozturk U, Sener NC, Tuygun C,
Bakirtas H and Imamoglu AM: Transurethral resection of a bladder
leiomyoma: A case report. Can Urol Assoc J. 8:E111–E113.
2014.PubMed/NCBI View Article : Google Scholar
|