Introduction
Metabolic syndrome is one of the most important
illnesses of the recent century (1).
It is a set of symptoms, namely hypertension, dyslipidemia,
dysglycemia and abdominal obesity, which occur secondary to insulin
resistance (2). Its prevalence is
20.2% in the United States (3), 30%
in Brazil (4) and 10.7% in South
Korea (5). A meta-analysis on a
sample of 74,440 Iranians stated that its prevalence in Iran is
34.7% (6).
Metabolic syndrome increases the risk of chronic
illnesses, particularly cardiovascular disease (7). People with metabolic syndrome are at
twice the risk of developing cardiovascular disease, three times
the risk of developing ischemic stroke (8), and five times the risk of developing
diabetes mellitus (9). Furthermore,
those with metabolic syndrome are prone to developing
osteoarthritis, certain types of cancer, with increased disability
and mortality risks (10). Metabolic
syndrome imposes heavy costs on healthcare systems (1).
The pathogenesis of metabolic syndrome remains
unclear. It involves a variety of contributing factors, including
lifestyle, environmental and genetic factors (11), stress (12), sex (13), number of parities (14), and shift work (15). Certain studies have reported a higher
risk of metabolic syndrome among women (14) and shift workers (15). Shift work is defined as working night
shifts between 6:00 p.m. to 07:00 a.m. It can negatively affect
circadian rhythm, and thereby, cause alterations in the secretion
of hormones, such as growth hormone, melatonin, cortisol, leptin
and ghrelin (16,17). Alterations to these hormones may
affect body metabolism, reduce glucose tolerance and increase
insulin resistance (18,19). A study on 2,089 hospital staff in
South Korea concluded that shift work significantly increases the
risk of metabolic syndrome (20).
However, certain studies reported an insignificant association with
metabolic syndrome (21,22), weight gain (23) and serum lipid levels (24).
In Iran, women are primarily employed in service
jobs (25), particularly in hospitals
(26), welfare centers (27) and nursing homes, whereby shift work is
typically encountered (28). Around
two thirds of employed women in Iran are of reproductive age
(25), and thus, experience pregnancy
and childbirth during their employment (29). Besides shift work, parity and the
number of parities can increase the risk of metabolic syndrome
among these women due to parity-associated increased abdominal
circumference (14) and increased
insulin resistance (30). Therefore,
female shift workers with more children appear to be at greater
risk of developing metabolic syndrome. Previous studies in Iran
investigating the association between shift work and metabolic
syndrome have been performed on industrial workers (24) and drivers (7). However, to the best of our knowledge, no
study has yet evaluated the prevalence of metabolic syndrome among
Iranian female shift workers, particularly those who are married
and are of reproductive age. The current study aimed to evaluate
the association between shift work with metabolic syndrome during
reproductive age.
Materials and methods
Patients
The present multi-center cross-sectional
correlational study was performed between September 2017 and May
2018 in three central cities located in Mazandaran, Iran (Amol,
Babol and Ghaemshahr). Participants were female shift and day
workers purposively selected from hospitals, welfare and
rehabilitation centers, nursing homes, and textile and sewing
mills. Participants were recruited if they were between 18 and 45
years old, married and had >2 years of work experience. The
exclusion criteria maintained were voluntary withdrawal from the
study or incompletion of the study, and having cardiovascular
disease, diabetes mellitus, or hypertension (with a blood pressure
of >140/90 mmHg) at the beginning of work.
For sample size calculation, the prevalence of
metabolic syndrome was considered to be at most 25% based on
results from two previous studies (31,32).
Accordingly, with a confidence level of 95% and an estimation error
of 6%, the sample size was estimated to be 200 participants/group.
Yet, considering an attrition rate of 5%, 419 women were
selected.
Assessment of demographical,
occupational and medical characteristics
A questionnaire was used to assess participant
demographical, occupational and reproductive characteristics.
Demographical characteristics included age, educational level,
place of residence and family income. Occupational characteristics
were work schedule (shift work or day work), work experience,
number of working hours/month, organizational position, workload
and occupational stress. Workload was assessed using a question
answered on a five-point Likert scale from ‘light’ to ‘heavy’,
while occupational stress was assessed using a question answered on
a five-point Likert scale from ‘very low’ to ‘very high’.
Reproductive characteristics assessed in the present study were
number of parities and route of delivery.
Assessment of health-associated
behaviors
Participant health-associated behaviors were
assessed through questions regarding cigarette smoking (yes/no),
alcohol consumption (yes/no), sleep quantity and quality, and
physical activity. The questions for sleep quantity and quality
assessment were, ‘How many hours do you sleep a day, on average?’
and ‘Is your current sleep adequate to fulfil your need for sleep?’
(yes/no), respectively. For physical activity assessment,
participants were asked if they walked ≥30 min thrice weekly. ‘Yes’
and ‘No’ responses to this question were respectively interpreted
as physically active and physically inactive.
Anthropometric measures
An analogue weight scale (MW84; EmsiG GmbH Co.,
Hamburg, Germany) and a wall-mounted plastic tape were used to
respectively measure weight and height in upright position without
shoes and with minimum possible clothes. Waist circumference (WC)
was also measured in the midway between the lowest rib edge and the
iliac crest.
Blood pressure
Blood pressure (BP) was measured using an analogue
sphygmomanometer (EmsiG GmbH Co.) from the right arm in the sitting
position, and following a 15-min rest.
Biomarkers
Biomarkers assessed in the current study were
triglyceride (TG), high-density lipoprotein (HDL) and fasting blood
sugar (FBS). Accordingly, a 5-mm blood sample was taken from each
participant at 07:00-09:00 a.m. following a night time fasting
period of 12-14 h. Subsequently, biochemical analysis was performed
in a laboratory of a hospital affiliated to Babol University of
Medical Sciences, Babol, Iran. All laboratory analyses were
performed by a laboratory technician, using an identical kit (Pars
Azmoon kit, Pars Azmoon Inc., Tehran, Iran), and one biochemistry
analyzer (Sapphire 800; Audit Diagnostics, Cork, Ireland).
Furthermore, blood sampling and anthropometric and blood pressure
measurements were performed by one person.
Diagnostic criteria for metabolic
syndrome
According to the National Cholesterol Education
Program Adult Treatment Panel III guidelines (33), participants were diagnosed with
metabolic syndrome if they simultaneously met three of the
following five criteria: i) Hypertension as determined by a BP
>130/85 mmHg or taking blood pressure medications; ii) high
serum TG level (>150 mg/dl); iii) high FBS (>110 mg/dl); iv)
low serum HDL level (<50 mg/dl); and v) abdominal obesity as
determined by a WC of >88 cm.
Shift work assessment
Participants were divided into two main groups based
on the work schedules, day workers and shift workers. Participants
who did morning or evening shifts and never did night shift were
considered as day workers. Shift workers included participants who
had rotational work. Shift workers were those participants who
worked 3 shifts of 8 h (morning, evening and night shifts) or who
worked two shifts of 8 h and one of 12 h or who worked 2 shifts of
12 h.
Statistical data analysis
The data were analyzed using SPSS (version 16.0;
SPSS, Inc., Chicago, IL, USA). Shift worker and day worker
participants were compared with each other respecting their
demographical, occupational, and reproductive characteristics and
health-associated behaviors using the independent-sample t,
Chi-square and the Fisher's exact tests. Furthermore, logistic
regression analysis was performed to determine the effect of shift
work on the odds of metabolic syndrome following adjustments for
the effects of potential confounders. For regression analysis, the
variable number of sleeping hours was dichotomized as ‘<6 h’ and
‘>6 h’. P<0.05 was considered to indicate a statistically
significant difference.
Results
Participants' demographical,
occupational and reproductive characteristics
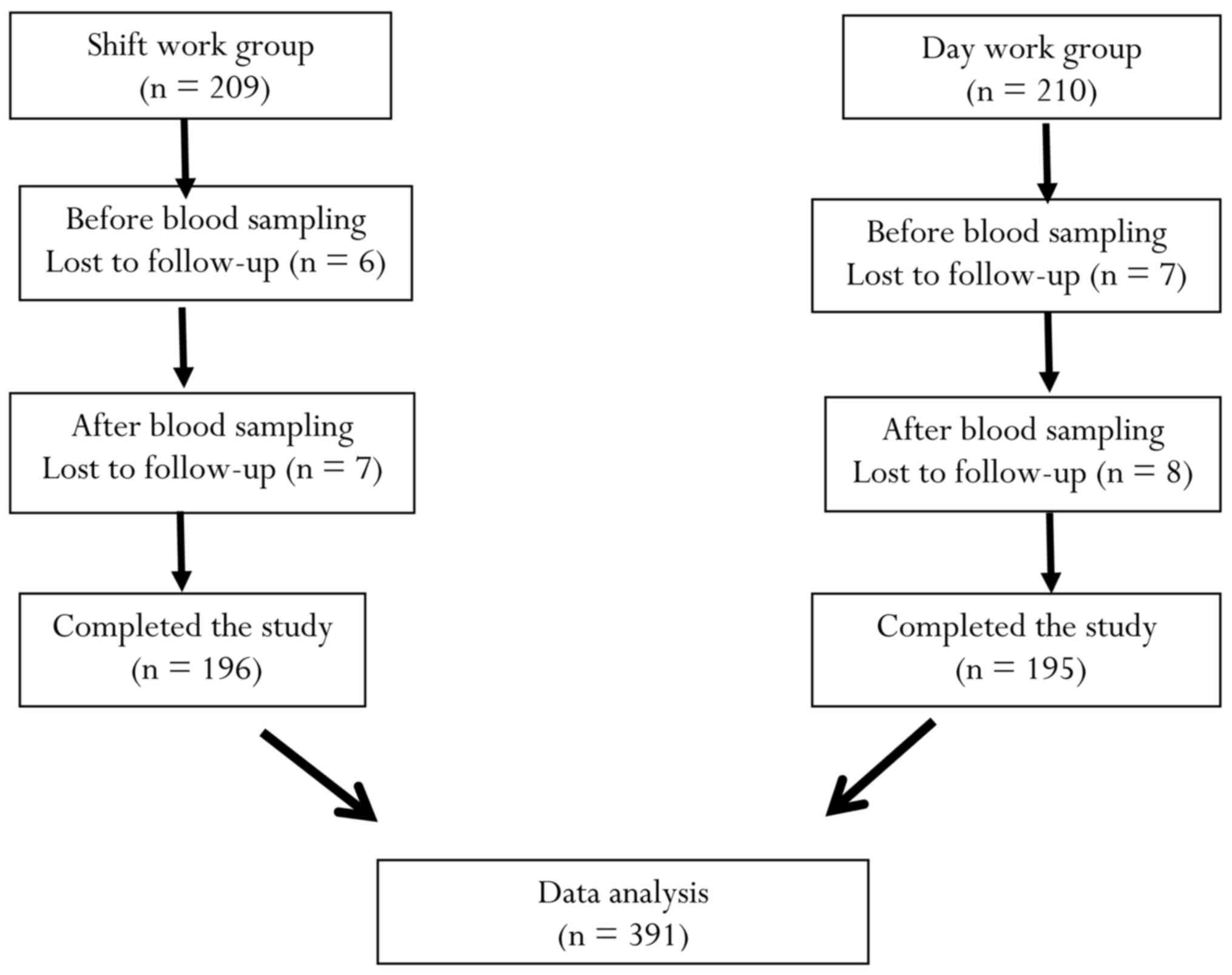
Among the 419 women recruited to the study, 28 were
excluded due to voluntary withdrawal or study incompletion.
Consequently, statistical data analysis was performed on the data
collected from 391 participants (Fig.
1). A total of 196 shift workers and 195 day workers were
included. Those who were excluded from the study did not
significantly differ from participants respecting their
demographical, occupational and reproductive characteristics
(P>0.05).
The mean age and work experience of participants
were 36.12±5.21 and 12.38±5.92 years, respectively, and there was
no statistically significant difference between shift workers and
day workers in terms of age and work experience. Shift workers had
significantly higher levels of Monthly work (h) compared with day
workers. (P<0.001; 192.61±23.33 vs. 179.12±18.76).
The majority of participants held university degrees
(73%), resided in urban areas (84%), were a healthcare provider
(70%), had a heavy workload with high levels of occupational stress
(60%), and had given birth through a caesarean section (70%).
Approximately 50% of women had one child (49.5%). Shift workers had
significantly higher levels of occupational stress compared with
day workers (P=0.02) and participants with more parities had
significantly greater WC measures (P<0.001).
Participants' health-associated
behaviors
One third of participants (33.3%) were physically
active, 2% of them smoked cigarettes and none reported alcohol
consumption. Furthermore, 48% of participants reported having
inadequate sleep. Sleep adequacy among shift workers was
significantly reduced compared with day workers (P=0.006; Table I). In addition, the length of sleep in
a 24-h period among shift workers was significantly shorter
compared with day workers (P<0.001).
 | Table IParticipants' demographical,
occupational and reproductive characteristics. |
Table I
Participants' demographical,
occupational and reproductive characteristics.
|
Characteristics | Total N (%) | Shift workers N
(%) | Day workers N
(%) | P-value |
|---|
| Age (years) | | | | 0.26a |
|
20-29 | 46 (11.8) | 27 (13.8) | 19 (9.7) | |
|
30-39 | 222 (55.9) | 113 (57.9) | 109 (55.9) | |
|
40-45 | 122 (31.3) | 55 (28.2) | 67 (34.4) | |
| Educational
level | | | | 0.82a |
|
Bachelor's | 287 (8.73) | 146 (75.3) | 141 (72.3) | |
|
Diploma | 72 (18.5) | 34 (17.5) | 38 (19.5) | |
|
Incomplete
secondary | 87 (13.3) | 14 (4.2) | 16 (8.2) | |
| Place of
residence | | | | 0.20a |
|
Urban
areas | 61 (15.7) | 35 (18.0) | 26 (13.3) | |
|
Rural
areas | 328 (84.3) | 159 (82.0) | 169 (86.7) | |
| Family income | | | | 0.036a |
|
Sufficient | 149 (40.38) | 63 (32.5) | 86 (44.3) | |
|
Moderately
sufficient | 179 (46.1) | 95 (49.0) | 84 (43.3) | |
|
Insufficient | 60 (15.5) | 36 (18.6) | 24 (12.4) | |
| Body mass index
(kg/m2) | | | | 0.27a |
|
<18.5 | 2 (0.5) | 2 (0.6) | 0 (0.0) | |
|
18.5-25 | 131 (33.5) | 69 (35.2) | 62 (31.8) | |
|
25-30 | 176 (45.0) | 81 (41.3) | 95 (48.7) | |
|
>30 | 82 (21.0) | 44 (22.4) | 38 (19.5) | |
| Number of
parities | | | | 0.64a |
|
1 | 185 (49.6) | 91 (48.4) | 94 (50.8) | |
|
≥2 | 188 (50.4) | 97 (51.6) | 91 (49.2) | |
| Route of
delivery | | | | 0.46a |
|
Normal
vaginal delivery | 109 (29.8) | 50 (27.0) | 59 (32.6) | |
|
Cesarean
section | 234 (63.9) | 122 (65.9) | 112 (61.9) | |
|
Both (in
different deliveries) | 23 (6.3) | 13 (7.0) | 10 (5.5) | |
| Physical
activity | | | | 0.057a |
|
Inactive | 143 (38.3) | 61 (33.3) | 82 (43.2) | |
|
Active | 230 (61.7) | 122 (66.7) | 108 (56.8) | |
| Cigarette
smoking | | | | 0.68b |
|
Yes | 5 (1.3) | 2 (1.0) | 3 (1.5) | |
|
No | 611 (98.1) | 125 (97.7) | 477 (98.1) | |
| Sleep adequacy
(h/day) | | | | 0.006a |
|
Inadequate | 180 (48.0) | 103 (55.1) | 77 (41.0) | |
|
Adequate | 195 (52.0) | 84 (44.9) | 111 (59.0) | |
| Employment
status | | | | 0.17a |
|
Healthcare
provider | 273 (70.7) | 136 (69.4) | 137 (72.1) | |
|
Mother aid
or nurse aid | 61 (15.7) | 38 (19.4) | 23 (12.1) | |
|
Laborer | 34 (8.8) | 15 (7.7) | 19 (10.0) | |
|
Service
worker | 18 (4.7) | 7 (3.6) | 11 (5.8) | |
| Workload | | | | 0.14a |
|
Low to
moderate | 151 (39.6) | 67 (35.3) | 84 (44.0) | |
|
Heavy | 161 (42.3) | 83 (43.7) | 78 (40.8) | |
|
Very
heavy | 69 (18.1) | 40 (21.1) | 29 (15.2) | |
| Occupational
stress | | | | 0.002a |
|
Very
high | 66 (17.3) | 43 (22.6) | 23 (12.0) | |
|
High | 138 (36.1) | 74 (38.9) | 64 (33.3) | |
|
Low to
moderate | 178 (46.6) | 73 (38.4) | 105 (54.7) | |
Association between shift work and
metabolic syndrome
The total prevalence of metabolic syndrome was
16.3%. The rate among shift workers and day workers was 17.3 and
14.9%, respectively, with no statistically significant
between-group difference (P=0.50; Table
II). The most prevalent components of metabolic syndrome among
participants were low serum HDL level (88%) and abdominal obesity
(73%). The prevalence of low serum HDL level among shift workers
was significantly increased compared with day workers (P=0.019).
However, they did not significantly differ from each other
respecting the other components of metabolic syndrome, including
hypertension, dysglycemia, abdominal obesity and
hypertriglyceridemia (P>0.05; Table
II).
| Table IIPrevalence of metabolic syndrome and
its components among shift and day workers. |
Table II
Prevalence of metabolic syndrome and
its components among shift and day workers.
| Metabolic syndrome
and its components | Total N (%) | Shift workers N
(%) | Day workers N
(%) |
P-valuea |
|---|
| BP (mmHg) | | | | 0.29 |
|
<130/85 | 377 (96.2) | 186 (94.9) | 190 (97.4) | |
|
≥130/85 | 15 (3.8) | 10 (5.1) | 5 (2.6) | |
| FBS (Mg/dl) | | | | 0.47 |
|
<110 | 384(98) | 191 (97.4) | 192 (98.5) | |
|
≥110 | 8(2) | 5 (2.6) | 3 (1.5) | |
| WC (cm) | | | | 0.42 |
|
<88 | 105 (26.8) | 49 (25.0) | 56 (28.7) | |
|
≥88 | 287 (73.2) | 147 (75.0) | 139 (71.3) | |
| HDL (Mg/dl) | | | | 0.019 |
|
<50 | 47 (12.0) | 16 (8.2) | 31 (15.9) | |
|
≥50 | 345 (88.0) | 180 (91.8) | 164 (84.1) | |
| TG (Mg/dl) | | | | 0.73 |
|
<150 | 314 (80.1) | 159 (81.1) | 155 (79.5) | |
|
≥150 | 78 (19.9) | 37 (18.9) | 40 (20.5) | |
| Metabolic
syndrome | | | | 0.50 |
|
Yes | 64 (16.3) | 34 (17.3) | 29 (14.9) | |
|
No | 328 (83.7) | 162 (82.7) | 166 (85.1) | |
Logistic regression analysis was used to determine
the odds of metabolic syndrome in relation to shift work. Following
adjustment for the effects of potential demographical, occupational
and medical confounders, the results of the logistic regression
analysis demonstrated that the odds of metabolic syndrome among
shift workers was nearly two times greater compared with day
workers (odds ratio, 1.83; 95% confidence interval, 0.088-3.79;
P=0.10; Table III).
| Table IIIRegression analysis for the
prediction of metabolic syndrome affliction based on work schedule
(shift or day work) adjusted for confounders. |
Table III
Regression analysis for the
prediction of metabolic syndrome affliction based on work schedule
(shift or day work) adjusted for confounders.
| Work schedule | Unadjusted OR (95%
CI) | Model 2 OR (95%
CI) | Model 3 OR (95%
CI) | Model 4 OR (95%
CI) | Model 5OR (95%
CI) |
|---|
| Day workers | 1 (Reference) | 1 (Reference) | 1 (Reference) | 1 (Reference) | 1 (Reference) |
| Shift workers | 1.20
(0.7-2.06) | 1.22
(0.71-2.11) | 1.21
(0.69-2.12) | 1.24
(0.77-2.54) | 1.83
(0.88-3.79) |
Discussion
The present study evaluated the association between
shift work and metabolic syndrome among women of reproductive age.
The results revealed that the prevalence of metabolic syndrome
among shift worker participants was 16.3%. However, two previous
studies reported that this rate was 22.4% among healthcare workers
in Iran (32) and 19.8% among
patients in a primary healthcare setting in Germany (34). This contradiction may be due the fact
that the present study was performed on women aged 18-45 years,
while the two previous studies were performed on people from
different age groups. Age is a significant risk factor for
metabolic syndrome (35), a previous
study on 3,024 Iranian women reported that the prevalence of
metabolic syndrome was 20% among women aged 25-34 years and 72%
among women aged 55-64 years (35).
Th present study findings also demonstrated that
shift work doubled the risk of metabolic syndrome. Previous studies
in Iran (7,32) and Italy (36) have reported the same finding. A
probable explanation for the higher risk of metabolic syndrome
among female shift workers in the current study may be their lower
serum HDL level compared to their day worker counterparts. This is
in line with the findings of two earlier studies (8,37). The
results of a meta-analysis on 74,440 Iranians also revealed that
low serum HDL level was the most common predisposing factor for
metabolic syndrome (39). Another
study on Iranian physicians reported that >50% of participants
exhibited low serum HDL levels (40).
Similarly, a study on Egyptian nurses reported that the level of
serum HDL among nurse day worker was twice that of nurse shift
workers (38). Lower levels of serum
HDL among shift workers may be due to circadian disorders (41). Circadian rhythm causes variations in
lipid metabolism (41), whereby
periodical alterations in cholesterol and triglycerides over a 24-h
period are 31.6 for and 38.5%, respectively (16). Accordingly, shift work may result in
dyslipidemia through altering circadian rhythm and
sleep-wakefulness cycle (40).
Although, a previous study indicated no significant association
between serum HDL level and shift work (17).
The present study also demonstrated that sleep
quantity and quality among shift workers were significantly less
compared with that of day workers, and the majority of shift
workers reported that they have inadequate sleep. Sleep has a
mediating role in the association between shift work and metabolic
syndrome (42). This role is probably
due to the negative effects of disturbed sleep among shift workers
on circadian rhythm, subsequent alterations in the metabolism of
serum lipids and endogenous glucose, and effects on glucose
tolerance (42).
The findings in the current study also indicated
that a third of participants regularly performed physical activity.
Furthermore, the rate of regular physical activity among shift
workers was considerably less compared with their day worker
counterparts. Similarly, a study on a group of Iranian nurses
reported that poor physical activity status' due to their multiple
parental and spousal responsibilities, and inadequate time for
engagement in physical activity (43). Regular physical activity can reduce
the risk of metabolic syndrome through reducing WC and body mass
index (44).
None of the participants in the current study
reported alcohol consumption and the majority (98%) did not smoke.
Two earlier studies in Iran also reported the same findings
(7,45). Unlike the high prevalence of low serum
HDL level and abdominal obesity in the present study, only a
limited number of participants (<4%) suffered from hypertension
and diabetes mellitus. These low rates of hypertension and diabetes
mellitus in the present study are attributable to the fact that all
participants were female and <45. Compared with men, women
>50 years are less likely to develop hypertension (46).
Due to time and financial limitations, the current
study was performed using a cross-sectional design. Future studies
are recommended to use cohort designs to provide more reliable data
on the association between shift work and metabolic syndrome.
Additionally, only a third of participants were mother aid, nurse
aid, labourer or service workers. The low number of these workers
in this study was associated with the limited number of welfare and
rehabilitation centers, nursing homes, and industrial female shift
workers in the area.
The results of the current study revealed that shift
work is associated with greater risk of metabolic syndrome among
women of reproductive age. Therefore, metabolic syndrome screening
programs should be essential for female shift workers. In addition,
the present study suggests that the most important components of
metabolic syndrome are low serum HDL level and abdominal obesity,
probably due to the limited physical activity intake and high
occupational stress of female shift workers. Strategies, including
awareness raising, dietary educations, and provision of physical
activity facilities at the workplace may reduce the risk of
metabolic syndrome among female shift workers, and improve their
health status during the reproductive age.
Acknowledgements
The authors would like to thank Mr. Mohammad Ghasemi
(laboratory technician, Shahid Beheshti Hospital, Babol, Iran) who
helped collect the study data.
Funding
The present study was funded by the Health Research
Institute in Babol University of Medical Sciences (grant no.
9542537).
Authors' contributions
MN, AT, MH, AH, AE, FG, FN, BH and MF contributed in
the design of the study. MN and FH performed measurements of
biomarkers. MN, AT, MH prepared analyzed the data and the first
draft of the manuscript. MN, AT, AE, FG, FN, BH and MF reviewed the
manuscript and provided comments. All authors approved the final
version of the manuscript.
Availability of data and materials
All the datasets generated and analyzed in the
present study are included in this published manuscript.
Ethics approval and consent to
participate
The Ethics Committee of Babol University of Medical
Sciences, Babol, Iran, approved this study (approval no.
MUBABOL.HRI.REC.1395.58). Written informed consent was obtained
from all participants and they were given the right to voluntarily
withdraw from the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
McCullough AJ: Epidemiology of the
metabolic syndrome in the USA. J Dig Dis. 12:333–340.
2011.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Kawabe Y, Nakamura Y, Kikuchi S, Murakami
Y, Tanaka T, Takebayashi T, Okayama A, Miura K, Okamura T and
Ueshima H: Relationship between shift work and clustering of the
metabolic syndrome diagnostic components. J Atheroscler Thromb.
21:703–711. 2014.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Davila EP, Florez H, Fleming LE, Lee DJ,
Goodman E, LeBlanc WG, Caban-Martinez AJ, Arheart KL, McCollister
KE, Christ SL, et al: Prevalence of the metabolic syndrome among
U.S. workers. Diabetes Care. 33:2390–2395. 2010.PubMed/NCBI View Article : Google Scholar
|
|
4
|
de Carvalho Vidigal F, Bressan J, Babio N
and Salas-Salvadó J: Prevalence of metabolic syndrome in Brazilian
adults: A systematic review. BMC Public Health.
13(1198)2013.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Yu KH, Yi YH, Kim YJ, Cho BM, Lee SY, Lee
JG, Jeong DW and Ji SY: Shift work is associated with metabolic
syndrome in young female Korean workers. Korean J Fam Med.
38:51–56. 2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Dalvand S, Bakhshi E, Zarei M, Asl MT and
Ghanei R: Prevalence of Metabolic Syndrome in Iran: A systematic
review and meta-analysis. MSNJ. 5:1–14. 2017.
|
|
7
|
Mohebbi I, Shateri K and Seyedmohammadzad
M: The relationship between working schedule patterns and the
markers of the metabolic syndrome: Comparison of shift workers with
day workers. Int J Occup Med Environ Health. 25:383–391.
2012.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Guize L, Pannier B, Thomas F, Bean K, Jégo
B and Benetos A: Recent advances in metabolic syndrome and
cardiovascular disease. Arch Cardiovasc Dis. 101:577–583.
2008.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Ginsberg HN and MacCallum PR: The obesity,
metabolic syndrome, and type 2 diabetes mellitus pandemic: Part I.
Increased cardiovascular disease risk and the importance of
atherogenic dyslipidemia in persons with the metabolic syndrome and
type 2 diabetes mellitus. J Cardiometab Syndr. 4:113–119.
2009.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Bolton MM: Sounding the alarm about
metabolic syndrome. Nursing. 40:34–40; quiz 40-41. 2010.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Cai H, Huang J, Xu G, Yang Z, Liu M, Mi Y,
Liu W, Wang H and Qian D: Prevalence and determinants of metabolic
syndrome among women in Chinese rural areas. PLoS One.
7(e36936)2012.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Chandola T, Brunner E and Marmot M:
Chronic stress at work and the metabolic syndrome: Prospective
study. BMJ. 332:521–525. 2006.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Kaur J: A comprehensive review on
metabolic syndrome. Cardiol Res Pract. 2014(943162)2014.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Lye MS, Ahmadi N, Khor GL, Hassan STBS,
Hanachi P and Delavar AM: Parity and metabolic syndrome in
middle-aged Iranian women: A cross-sectional study. Casp J Reprod
Med. 1:19–24. 2015.
|
|
15
|
Ye HH, Jeong JU, Jeon MJ and Sakong J: The
association between shift work and the metabolic syndrome in female
workers. Ann Occup Environ Med. 25(33)2013.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Boivin DB and Boudreau P: Impacts of shift
work on sleep and circadian rhythms. Pathol Biol (Paris).
62:292–301. 2014.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Kim TW, Jeong JH and Hong SC: The impact
of sleep and circadian disturbance on hormones and metabolism. Int
J Endocrinol. 2015(591729)2015.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Morris CJ, Purvis TE, Hu K and Scheer FA:
Circadian misalignment increases cardiovascular disease risk
factors in humans. Proc Natl Acad Sci USA. 113:E1402–E1411.
2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Scheer FA, Hilton MF, Mantzoros CS and
Shea SA: Adverse metabolic and cardiovascular consequences of
circadian misalignment. Proc Natl Acad Sci USA. 106:4453–4458.
2009.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Oh JI and Yim HW: Association between
rotating night shift work and metabolic syndrome in Korean workers:
Differences between 8-hour and 12-hour rotating shift work. Ind
Health. 56:40–48. 2018.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Karlsson BH, Knutsson AK, Lindahl BO and
Alfredsson LS: Metabolic disturbances in male workers with rotating
three-shift work. Results of the WOLF study. Int Arch Occup Environ
Health. 76:424–430. 2003.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Puttonen S, Viitasalo K and Härmä M: The
relationship between current and former shift work and the
metabolic syndrome. Scand J Work Environ Health. 38:343–348.
2012.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Nazri SM, Tengku MA and Winn T: The
association of shift work and hypertension among male factory
workers in Kota Bharu, Kelantan, Malaysia. Southeast Asian J Trop
Med Public Health. 39:176–183. 2008.PubMed/NCBI
|
|
24
|
Akbari H, Mirzaei R, Nasrabadi T and
Gholami-Fesharaki M: Evaluation of the effect of shift work on
serum cholesterol and triglyceride levels. Iran Red Crescent Med J.
17(e18723)2015.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Firouzbakht M, Nikpour M and Tirgar A: The
study of impact of employment on gestational age and weight of
newborn. Iran J Health Sci. 3:9–14. 2015. View Article : Google Scholar
|
|
26
|
Heydarikhayat N, Mohammadinia N,
Sharifipour H and Almasy A: Assessing frequency and causes of
verbal abuse against the clinical staff. Q J Nurs Manage. 1:70–78.
2012.
|
|
27
|
Tavafi N, Hatami-Zadeh N, Kazem-Nezhad A
and Jazayeri A: Organizational stressors and related stress
intensities in Tehran's comprehensive rehabilitation centers: From
the employees' point of view. jrehab. 7:30–34. 2007.
|
|
28
|
Rajaratnam SM, Howard ME and Grunstein RR:
Sleep loss and circadian disruption in shift work: Health burden
and management. Med J Aust. 199:S11–S15. 2013.PubMed/NCBI
|
|
29
|
Nikpour M, Tirgar A, Ebadi A, Ghaffari F,
Firouzbakht M and Hajiahmadi M: Development and psychometric
evaluation of a women shift workers' reproductive health
questionnaire: Study protocol for a sequential exploratory
mixed-method study. Reprod Health. 15(22)2018.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Sourinejad H, Niyati S and Moghaddam
Banaen L: The metabolic syndrome and its components in
mid-pregnancy in Tehran. J Urmia Nurs Midwifery Fac. 14:465–473.
2016.
|
|
31
|
Amiri A and Hakimi A: The study of
prevalence of metabolic syndrome among nurses of Shahid Mohammadi
Hospital of Bandar Abbas city, Iran. jcnm. 6:1–8. 2017.
|
|
32
|
Niazi E, Saraei M, Aminian O and Izadi N:
Frequency of metabolic syndrome and its associated factors in
health care workers. Diabetes Metab Syndr. 13:338–342.
2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Expert Panel on Detection Evaluation and
Treatment of High Blood Cholesterol in Adults: Executive summary of
the third report of the National Cholesterol Education Program
(NCEP) expert panel on detection, evaluation, and treatment of high
blood cholesterol in adults (Adult Treatment Panel III). JAMA.
285:2486–2497. 2001.
|
|
34
|
Moebus S, Hanisch JU, Aidelsburger P,
Bramlage P, Wasem J and Jöckel K-H: Impact of 4 different
definitions used for the assessment of the prevalence of the
Metabolic Syndrome in primary healthcare: The German Metabolic and
Cardiovascular Risk Project (GEMCAS). Cardiovasc Diabetol.
6(22)2007.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Delavari A, Forouzanfar MH, Alikhani S,
Sharifian A and Kelishadi R: First nationwide study of the
prevalence of the metabolic syndrome and optimal cutoff points of
waist circumference in the Middle East: The national survey of risk
factors for noncommunicable diseases of Iran. Diabetes Care.
32:1092–1097. 2009.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Pietroiusti A, Neri A, Somma G, Coppeta L,
Iavicoli I, Bergamaschi A and Magrini A: Incidence of metabolic
syndrome among night-shift healthcare workers. Occup Environ Med.
67:54–57. 2010.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Karlsson B, Knutsson A and Lindahl B: Is
there an association between shift work and having a metabolic
syndrome? Results from a population based study of 27,485 people.
Occup Environ Med. 58:747–752. 2001.PubMed/NCBI
|
|
38
|
Gadallah M, Hakim SA, Mohsen A and Eldin
WS: Association of rotating night shift with lipid profile among
nurses in an Egyptian tertiary university hospital. East Mediterr
Health J. 23:295–302. 2017.PubMed/NCBI
|
|
39
|
Daneshpour M, Mehrabi Y, Hedayati M,
Houshmand M and Azizi F: A multivariate study of metabolic syndrome
risk factors, using factor analysis: Tehran Lipid and Glucose
Study. IJEM. 8:139–146. 2006.
|
|
40
|
Chiti H, Shakibi E, Soltani Z,
Mazloomzadeh S and Mousavinasab S: Prevalence of metabolic syndrome
and cardiovascular risk factors among physicians of Zanjan city.
ZUMS J. 24:10–20. 2016.
|
|
41
|
Rivera-Coll A, Fuentes-Arderiu X and
Díez-Noguera A: Circadian rhythmic variations in serum
concentrations of clinically important lipids. Clin Chem.
40:1549–1553. 1994.PubMed/NCBI
|
|
42
|
Kim JY, Yadav D, Ahn SV, Koh SB, Park JT,
Yoon J, Yoo BS and Lee SH: A prospective study of total sleep
duration and incident metabolic syndrome: The ARIRANG study. Sleep
Med. 16:1511–1515. 2015.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Kalroozi F, Pishgooie S, Taheriyan A,
Khayat S and Faraz R: Health-promoting behaviours and related
factors among nurses in selected military hospitals. Journal of
Faculty of Nursing, AJA university of Medical Sciences. 1:73–80.
2015.
|
|
44
|
Monteiro CA, Conde WL, Lu B and Popkin BM:
Obesity and inequities in health in the developing world. Int J
Obes Relat Metab Disord. 28:1181–1186. 2004.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Fotouhi A, Khabazkhoob M, Hashemi H and
Mohammad K: The prevalence of cigarette smoking in residents of
Tehran. Arch Iran Med. 12:358–364. 2009.PubMed/NCBI
|
|
46
|
Everett B and Zajacova A: Gender
differences in hypertension and hypertension awareness among young
adults. Biodemogr Soc Biol. 61:1–17. 2015.PubMed/NCBI View Article : Google Scholar
|