Introduction
Premature rupture of membranes (PROM) and preterm
PROM (PPROM) are common obstetric complications. PPROM is the
rupture of membranes in a pregnant female prior to the onset of
labor, before 37 weeks gestation and PROM occurs after 37 weeks
gestation. The incidence of PPROM is 2.0–3.5% and the incidence of
PROM is 10% (1). In particular,
PPROM can cause neonatal sepsis, pneumonia and neonatal pulmonary
hyaline membrane disease. All these secondary factors can increase
the risk of perinatal fetal mortality.
The current diagnosis of PPROM and PROM is based on
vaginal fluid analysis. However, samples are easily contaminated,
resulting in a high rate of false positives. In addition, there is
too little amniotic fluid in PROM to provide an adequate sample and
this can result in a high false-negative rate. When PROM is
combined with chorioamnionitis (PROM + C), the diagnoses made
according to the C-reactive protein (CRP) levels are not specific
to intrauterine infections and may be influenced by other factors
(1). Therefore, PPROM and PROM
diagnostic procedures, particularly when combined with
chorioamnionitis, are largely limited. The aim of the present study
was to investigate the changes in serum β-human chorionic
gonadotropin (β-hCG) and interleukin-1 (IL-1) levels in PROM
females and compare these with the levels in females with normal
pregnancies. The results indicate that measuring serum β-hCG and
IL-1 levels may provide an alternative diagnostic tool for
determining infection in parturient females.
Materials and methods
Patient information
A total of 100 patients with PROM in the Department
of Obstetrics and Gynecology at the Shenzhen Seventh Peoples
Hospital (Shenzhen, Guangdong, China) were randomly selected for
the prospective study. All the human participants provided written
informed consent prior to the study. The study protocol was
approved by the local Institutional Review Board or Ethics
Committee prior to the study. A total of 56 patients had PROM only.
The average gestational age for this group was 37–41+6
weeks, the patient age range was 20–35 years and the average age
was 25±3.2 years. The remaining 44 patients had PROM + C. Within
this group, the average gestational age was 37–41+6
weeks, the patient age range was 20–35 years and the average age
was 26±2.8 years. Simultaneously, 50 females with normal
pregnancies were chosen as the control group. The average
gestational age was 37±41+6 weeks, the patient age range
was 20–34 years and the average age was 24±3.4 years. Females with
any other obstetric complications were excluded from the study.
Blood analysis
A total of 3 ml venous blood was drawn from all the
patients ~1 h before delivery. The blood samples were centrifuged
for 15 min at 4,929 × g to separate the serum. A chemiluminescence
assay (Roche Diagnostics, Madison, WI, USA) was used to determine
the β-hCG levels. The reagent was used according to the
manufacturer’s instructions (Randox Life Science, Crumlin, UK) and
chemiluminescence was measured using a Cobas 6000 analyzer (Roche
Diagnostics, Madison, WI, USA).
A turbidity test (Zhongguo, Shanghai, China) was
used to provide a preliminary diagnosis of chorioamnionitis and to
determine the serum CRP levels. The test was performed according to
the manufacturer’s instructions. ELISA (Shanghai Yisha Biological
Technology Co., Ltd., Shanghai, China) was used to detect serum
IL-1 levels. The results were measured using an auto-analyzer (Gold
Innovative Materials Co., Ltd., Anhui, China).
Placenta and fetal membrane tissues
Following the delivery of the placenta, a membrane
sample that was 5 cm from the membrane breach of each patient was
obtained. Each sample size was ~5×5 cm. Two placenta tissue samples
that were ~2×2 cm in size were also obtained from each patient. One
sample was from the placental edge and the other was collected from
the center of the placenta. All the samples were fixed with 10%
formalin prior to pathological analyses.
PROM and chorioamnionitis diagnoses
PROM was diagnosed using standard procedures
(2). Briefly, the patient was
diagnosed with PROM if any of the following clinical criteria were
observed upon pelvic examination with a sterile speculum: Amniotic
fluid leaving or pooling behind the cervix, the fluid had a pH
>6.5 and a vaginal posterior fornix smear exhibited a fern-like
appearance under the microscope when dried.
The patients were diagnosed with chorioamnionitis
using standard clinical and histopathological procedures (3). The clinical diagnoses were made
according to malodorous amniotic fluid or vaginal discharge,
maternal fever, uterine tenderness, increased white blood cell
count and serum CRP levels >8 mg/l.
Histopathological diagnoses were generated and
staged according to the following criteria: Stage I, minor
neutrophil invasion without significant chorionic fibrin deposition
of chorionic plate or limited to the decidual layer; stage II,
significant neutrophil invasion extended to chorionic tissues and
fetal blood vessels, but not the amniotic membrane; and stage III,
extensive neutrophil invasion of the decidual, chorionic and
amniotic membrane. Neutrophils covering the surface of the amniotic
membrane indicated sepsis in the amniotic cavity. The patients were
assigned a level based on neutrophil count: Level 1, <10
neutrophils; level II, 11–30 neutrophils; and level III, >30
neutrophils per field of view at high magnification (3). These observations indicated the
severity of chorioamnionitis. The association between β-hCG levels
and the severity of chorioamnionitis was not investigated in the
study.
Statistical analysis
SPSS 17.0 software (SPSS, Inc., Chicago, IL, USA)
was used to perform statistical analyses. Independent sample
t-tests were used to analyze the patient characteristics. Receiver
operating characteristic (ROC) curve construction was used for
diagnostic test evaluation. Enumeration data was analyzed using the
χ2 test. P<0.05 was considered to indicate a
statistically significant difference.
Results
Statistical analyses of patient
parameters
Statistical analyses were performed for all the
patient parameters between the control, PROM and PROM + C groups.
There were no statistical differences between parity, gestational
age and patient age for the three study groups (P>0.05). The
patient characteristics are summarized in Table I.
 | Table IPatient characteristics. |
Table I
Patient characteristics.
| Group | Parity, n | Average age,
years | Average gestational
age, weeks |
|---|
|
|---|
| 1 | 2 | 3 |
|---|
| Control | 34 | 14 | 2 | 24±3.4 |
39+2±1+1 |
| PROM | 38 | 15 | 3 | 25±3.2 |
38+6±1+4 |
| PROM + C | 32 | 11 | 1 | 26±2.8 |
38+4±1+3 |
To determine if there were any differences in serum
β-hCG, CRP and IL-1 levels between the control and PROM groups, the
blood samples that were obtained from all the patients ~1 h before
delivery were analyzed. The serum β-hCG levels were higher in the
PROM compared to the control group (18,636.96±14,379.10 vs.
7,557.86±2,922.06 IU/l; P<0.05). There were no significant
differences in serum CRP and IL-1 levels between the two groups
(P>0.05; Table II).
| Table IIComparative blood analyses between the
control and PROM groups. |
Table II
Comparative blood analyses between the
control and PROM groups.
| Group | β-hCG, IU/l | CRP, mg/l | IL-1, ng/ml |
|---|
| Control |
7,557.86±2,922.06 | 6.08±1.70 | 0.12±0.04 |
| PROM |
18,636.96±14,379.10 | 6.76±1.75 | 0.13±0.03 |
| P-value | <0.05 | 0.65 | 0.54 |
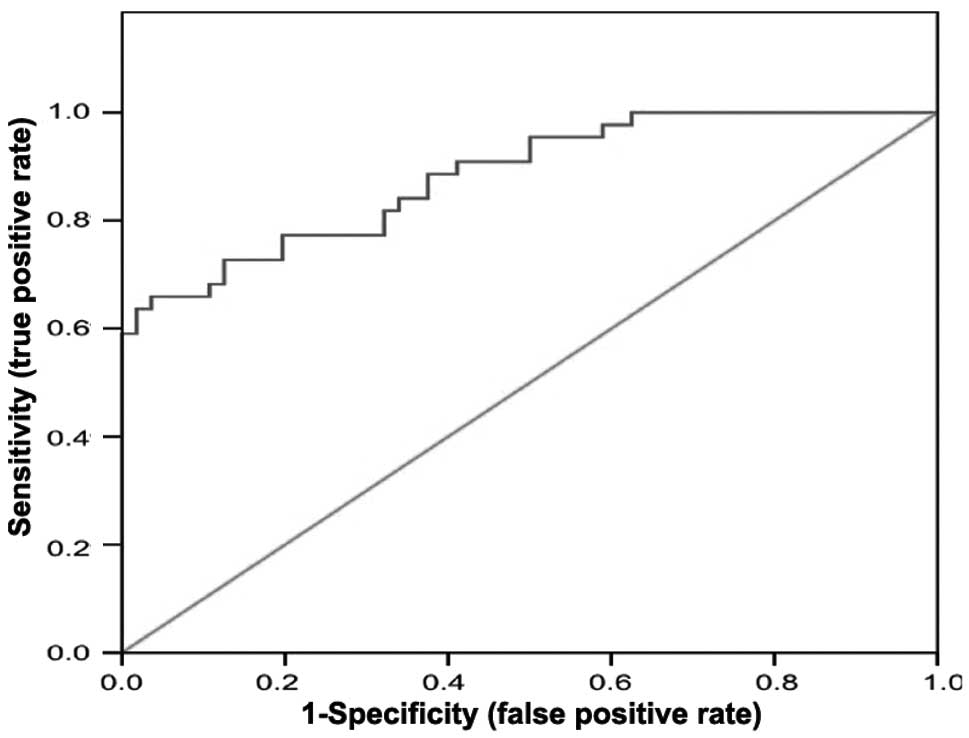
An ROC curve was constructed to test the diagnostic
value of measuring serum β-hCG levels between patients in the
control and PROM groups. The area under the ROC curve was 0.80
(Fig. 1). Therefore, serum β-hCG
levels have a clinical value in diagnosing PROM. According to the
ROC curve coordinates, when serum β-hCG levels were ≥8,382.50 IU/l,
the sensitivity of diagnosing PROM with this measurement was 71%
and the specificity was 76%.
Serum levels of β-hCG, CRP and IL-1
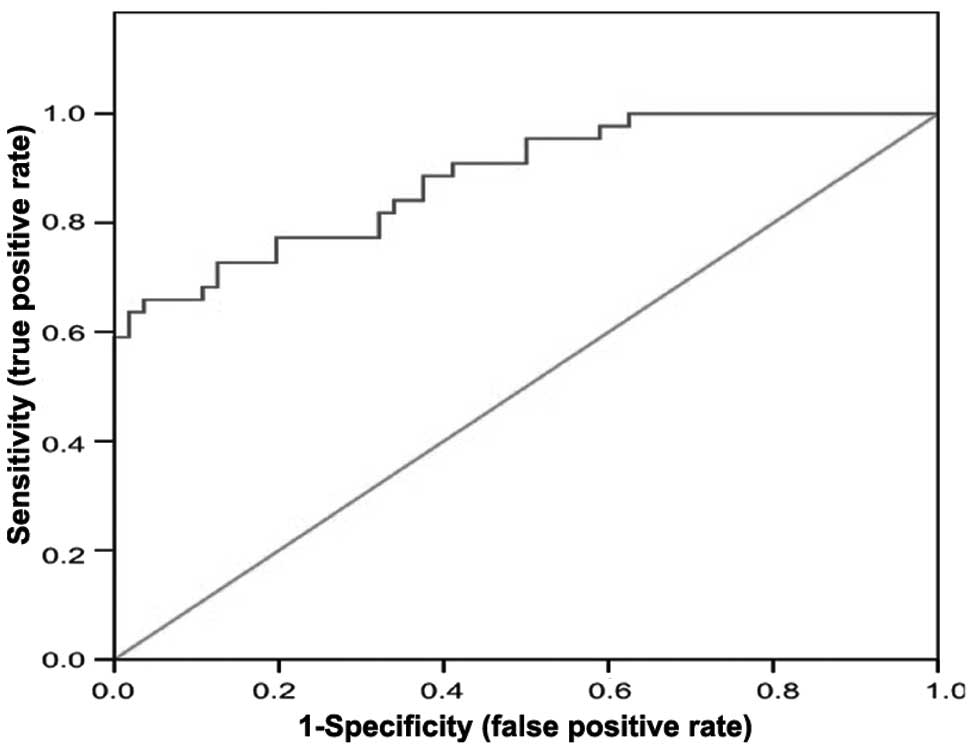
Whether there were any differences in serum β-hCG,
CRP and IL-1 levels between the PROM and PROM + C groups was also
investigated (Table III). The
PROM + C serum β-hCG levels were higher compared to the PROM group
(50,310.34±22,874.82 IU/l and 18,636.96±14,379.10 IU/l,
respectively; P<0.05). The area under the ROC curve constructed
for the serum β-hCG levels in these two groups was 0.87 (Fig. 2). Therefore, the measurement of
serum β-hCG levels has clinical value in distinguishing between
PROM and PROM + C. According to the ROC coordinates, when serum
β-hCG levels were ≥23,900.50 IU/l, the sensitivity of diagnosing
PROM + C with this measurement was 77.5% and the specificity was
78.6%.
| Table IIIComparative blood analyses between the
PROM and PROM + C groups. |
Table III
Comparative blood analyses between the
PROM and PROM + C groups.
| Group | β-hCG, IU/l | CRP, mg/l | IL-1, ng/ml |
|---|
| PROM |
18,636.96±14,379.10 | 6.76±1.75 | 0.13±0.03 |
| PROM + C |
50,310.34±22,874.82 | 17.27±7.18 | 0.58±0.05 |
| P-value | <0.05 | <0.05 | <0.05 |
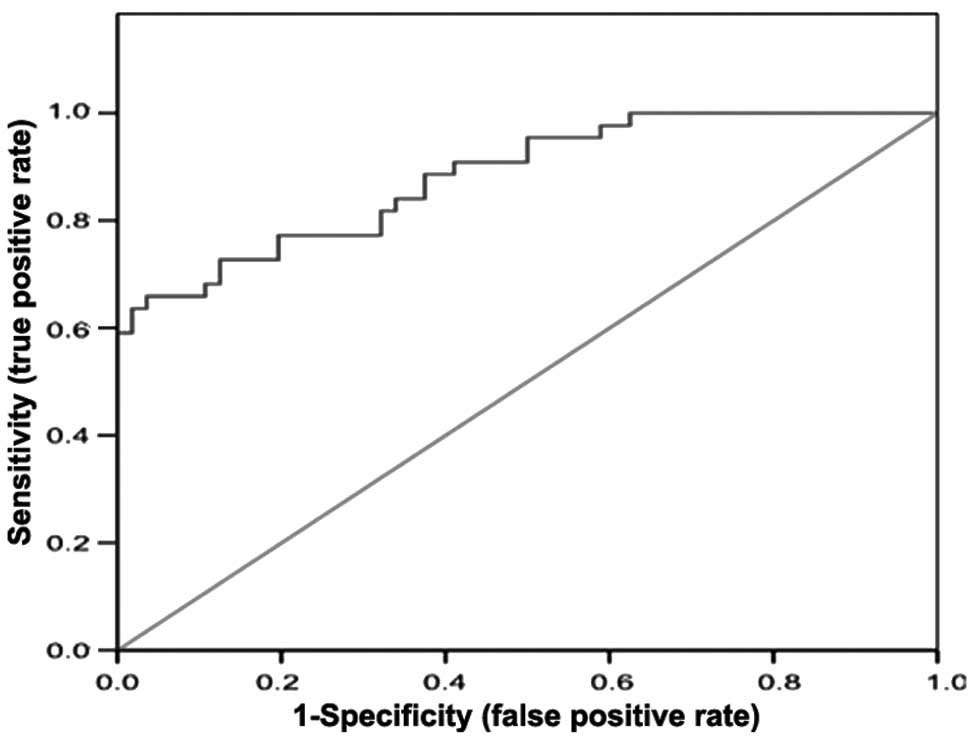
The differences in the serum CRP and IL-1 levels
between the PROM and PROM + C groups were also statistically
significant (P<0.05). The serum CRP levels for the PROM and PROM
+ C groups were 6.76±1.75 and 17.27±7.18 mg/l, respectively. The
serum IL-1 levels for the PROM and PROM + C groups were 0.13±0.03
and 0.58±0.05 ng/ml, respectively (Table III). According to ROC curve
analyses, serum IL-1 levels can distinguish between patients with
PROM alone and patients with PROM + C. The ROC curve coordinates
show that when serum IL-1 levels are ≥0.38 ng/ml, the sensitivity
of diagnosing PROM + C is 76.5% and the specificity is 72.6%
(Fig. 3). This was compared to the
sensitivity of diagnosing PROM + C according to serum CRP levels
(81.3%) and the specificity was (70.2%). These diagnostic serum-CRP
values of sensitivity and specificity were also compared to those
of serum β-hCG values. CRP sensitivity was higher than that of
β-hCG, however, the specificity was lower. Using the χ2
test, it was determined that the differences between these two
indices had no statistical significance (P>0.05).
The study aimed to determine if a combination of two
blood analysis indices could be used to improve the sensitivity and
specificity of diagnosing patients with PROM + C. The clinical
value of combining serum β-hCG and IL-1 level measurements to
diagnose PROM + C was evaluated. The results show that combining
these two indices had no statistical significance (P>0.05;
Table IV).
| Table IVEvaluation of combined serum β-hCG and IL-1 ROC indices in the
diagnosis of PROM + C. |
Table IV
Evaluation of combined serum β-hCG and IL-1 ROC indices in the
diagnosis of PROM + C.
| Index | Sensitivity, % | Specificity, % | Positive predictive
value, % | Negative predictive
value, % |
|---|
| β-hCG, ≥23,900.50 IU/l | 77.5 | 78.6 | 80.1 | 79.3 |
| IL-1, ≥0.38
ng/ml | 76.5 | 72.6 | 78.3 | 77.6 |
| β-hCG + IL-1 | 77.8 | 79.7 | 81.1 | 78.6 |
Discussion
In recent years, much progress has been made in
elucidating the multiple factors that contribute to PROM. These
include structural changes in the amniotic membrane, infection and
immunology (4). Among them,
infectious factors are a primary cause. Numerous pregnant females
sustain infections prior and subsequent to amniotic membrane
rupture and a number of these infections are asymptomatic.
Therefore, it is important to diagnose PROM + C to improve maternal
and fetal outcomes. The conventional diagnosis of PROM combines
patient history, speculum examination, measuring vaginal fluid pH
with nitrazine paper and the cervical smear fern test (5). However, these tests are often
subjective and have high false-positive rates due to vaginal
contamination with blood, urine or semen (6). Non-invasive diagnostic tests include
the detection of α-fetoprotein, prolactin, insulin-like growth
factor-binding protein-1 (IGFBP-1), placental α microglobulin-1
(PAMG-1) and β-hCG in vaginal fluids (7,8).
Bedside strip tests for IGFBP-1 and PAMG-1 are the most commonly
used and most accurate assays, but a gold standard non-invasive
diagnostic test for PROM does not yet exist (9).
In the current study, an alternative diagnostic test
is reported for PROM in the detection of serum β-hCG levels. The
levels were significantly higher in patients with PROM and PROM +
C, compared to females with normal pregnancies. When evaluated with
an ROC curve, the data demonstrate that this application has
clinical diagnostic value, as the sensitivity of diagnosing PROM is
71% and the specificity is 76%.
The serum β-hCG levels rise quickly from conception
until 8–10 weeks gestation. At 4 months gestation, serum β-hCG
levels progressively decline until delivery. As measuring serum
β-hCG levels is relatively clear, this measurement alone or in
combination with another diagnostic test, may be useful in
diagnosing difficult cases of PROM. Conversely, the differences in
serum CRP and IL-1 levels were not statistically significant in
differentiating between patients with or without PROM. Therefore,
these should not be considered as alternative diagnostic indices
for PROM.
Early diagnosis of PROM + C is pivotal in improving
prognoses. Currently, chorioamnionitis diagnoses are performed by
measuring CRP levels and by histopathology. Also, IL-6 is the most
studied candidate and several studies have reached different
conclusions. A study by Kopyra et al (10) indicated that detecting IL-6 levels
is more efficient than detecting CRP levels for diagnosing PROM + C
and determining the severity of neonatal infection. However, Tita
and Andrews (11) have shown that
IL-6 plays a limited role in intrauterine infection and another
study has shown that measuring serum IL-6 levels may be helpful in
predicting subclinical chorioamnionitis (12).
The present study aimed to determine whether
measuring serum β-hCG levels could be used as an alternative
approach to differentiate between patients with PROM or PROM + C.
The data show that the serum β-hCG levels were significantly higher
in patients with PROM + C, when compared to patients that only had
PROM. In addition, ROC curves indicated that this index has value
as a clinical diagnostic tool (area under the curve >0.5). The
sensitivity of diagnosing PROM + C with serum β-hCG levels was
77.5% and the specificity was 78.6%. Although the data indicate
that this diagnostic index is no more efficient than measuring CRP
levels, the serum β-hCG levels are pregnancy-specific, whereas the
CRP levels are not. In addition, Smith et al (13) have concluded that the detection of
CRP levels alone cannot predict chorioamnionitis with
certainty.
The study performed by Li (14) supports our hypothesis that serum
β-hCG levels have a higher value in predicting chorioamnionitis
compared to CRP levels. However, the pathophysiological mechanism
in which serum β-hCG levels increase during infection has not yet
been elucidated. When patients with PROM become infected, villous
interstitial inflammatory cell infiltration and placental tissue
injury occurs. This can lead to intrauterine hypoxia and cause
reactive trophoblastic cell hyperplasia. This may result in
increased synthesis and release of β-hCG (14). Another possibility is that
intrauterine infection induces inflammatory cells to release more
cytokines, such as IL-6 (15). In
turn, circulating cytokines may induce trophoblast cells to produce
more β-hCG. The severity of chorioamnionitis, as determined by
histopathological grading, may be associated with increased β-hCG
levels.
IL-1 is a cytokine that is primarily produced by
monocytes. Using radiation immunology technology, our previous
study found that the IL-1 receptor is highly expressed in the nerve
fibers of the rat hippocampus, brain cortex, bulbus olfactorius,
cerebellum choroid plexus, hypothalamus, corpus striatum and
medulla oblongata (1). IL-1 is
produced earlier than other host defense proteins and has a higher
sensitivity and specificity. In the present study, serum IL-1
levels were significantly higher in patients with PROM + C when
compared to patients with PROM only. Notably, a previous study
demonstrated that the IL-1 levels in amniotic fluid are higher
during pregnancy and IL-1 levels may be linked to an increased risk
of PROM (16). In addition, a study
by Puchner et al (17)
demonstrated that the IL-1β levels in amniotic fluid are positively
associated with preterm delivery. For every unit increase in IL-1β,
females are 7.2 times more likely to deliver preterm.
The present study demonstrates that the serum β-hCG
and IL-1 levels are potential biomarkers for diagnosing PROM + C.
The serum β-hCG levels may also be able to diagnose patients that
only have PROM. β-hCG is a pregnancy-specific hormone, therefore it
has an advantage in diagnosing PROM and PROM + C. In addition,
blood samples are easy to obtain and analyses are cost effective.
Using β-hCG, it may be possible to dynamically monitor PROM and
detect chorioamnionitis at an early stage. The IL-1 response is
rapid and inflammation-specific, adding to its value as a clinical
diagnostic tool. Measuring the IL-1 levels is also cost effective.
However, the use of these indices for diagnosing PROM + C resulted
in a sensitivity and specificity <80%. Sensitivity and
specificity must be improved prior to combining serum β-hCG and
IL-1 levels for use as an effective diagnostic tool. However, serum
β-hCG and IL-1 may be powerful diagnostic tools for PROM + C when
evaluated in parallel with other factors. Therefore, further
studies are required to investigate this possibility.
References
|
1
|
Le J: Obstetrics and Gynecology. 7th
edition. Beijing People’s Medical Publishing House; Beijing: pp.
137–138. 2008
|
|
2
|
Falagas ME, Avgeri SG, Matthaiou DK,
Dimopoulos G and Siempos II: Short- versus long-duration
antimicrobial treatment for exacerbations of chronic bronchitis: a
meta-analysis. J Antimicrob Chemother. 62:442–450. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chen ZN: Pathology of Obstetrics and
Gynecology Shanghai Medical. University Press; Shanghai: pp.
343–344. 1996
|
|
4
|
Malak TM, Ockleford CD, Bell SC, et al:
Confocal immunofluorescence localization of collagen types I, III,
IV, VI and their ulrtastructural organization in term human fetal
membranes. Placenta. 14:385–406. 1993. View Article : Google Scholar
|
|
5
|
Casey ML and MacDonald PC: Interstitial
collagen synthesis and processing in human amnion: a property of
the mesenchynal cells. Biol Reprod. 55:1253–1260. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Menon R and Fortunato SJ: The role of
matrix degrading enzymes and apoptosis in rupture of membranes. J
Soc Gynecol Investig. 11:427–437. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Carranza Lira S, Negrete López M,
Quinzaños Fresnedo C and Leaños Miranda A: Usefulness of the
qualitative detection of hCG in cervicovaginal lavage for the
diagnosis of premature rupture of membranes. Ginecol Obstet Mex.
77:142–146. 2009.(In Spanish).
|
|
8
|
Knapik D and Olejek A: Analysis of
cervicovaginal fluid in the diagnosis of premature rupture of
membranes. Ginekol Pol. 82:50–55. 2011.(In Polish).
|
|
9
|
van der Ham DP, van Teeffelen AS and Mol
BW: Prelabour rupture of membranes: overview of diagnostic methods.
Curr Opin Obstet Gynecol. 24:408–412. 2012.PubMed/NCBI
|
|
10
|
Kopyra P, Seremak-Mrozikiewicz A and Drews
K: Usefulness of PCT, IL-6, CRP measurement in the prediction of
intraamniotic infection and newborn status in pregnant women with
premature rupture of membranes. Ginekol Pol. 81:336–341. 2010.(In
Polish).
|
|
11
|
Tita AT and Andrews WW: Diagnosis and
management of clinical chorioamnionitis. Clin Perinatol.
37:339–354. 2010. View Article : Google Scholar
|
|
12
|
Hou LT, Zhou YW and Liu CF: Monitoring the
significance of serum CRP and IL-1 in preterm premature rupture of
membranes pregnant women. Chin J Mater Child Heal Care.
5:1777–1778. 2008.
|
|
13
|
Smith EJ, Muller CL, Sartorius JA, White
DR and Maslow AS: C-reactive protein as a predictor of
chorioamnionitis. J Am Osteopath Assoc. 112:660–664.
2012.PubMed/NCBI
|
|
14
|
Li HX: Comparing serum β-hCG and CRP
levels in predicting intrauterine infection and prognosis. Chin J
Hosp Infect. 22:2016–2018. 2012.
|
|
15
|
Yu L and Chen JH: The relationship among
CRP, preterm premature rupture of membranes and subclinical
chorionic amnionitis. J Pract Med Tech. 15:2889–2890. 2008.
|
|
16
|
Bitner A and Kalinka J: IL-β, IL-6
promoter, TNF-α promoter and IL-1RA gene polymorphisms and the risk
of preterm delivery due to preterm premature rupture of membranes
in a population of Polish women. Arch Med Sci. 6:552–557. 2010.
|
|
17
|
Puchner K, Iavazzo C, Gourgiotis D, et al:
Mid-trimester amniotic fluid interleukins (IL-1β, IL-10 and IL-18)
as possible predictors of preterm delivery. In Vivo. 25:141–148.
2011.
|