Introduction
Bisphosphonates are potent inhibitors of osteoclast
activity and are used in patients with bone metastases due to
malignant diseases or osteoporosis. Depending on the molecular
structure, bisphosphonates can be separated into first, second and
third generation bisphosphonates. The first generation
bisphosphonates are non-nitrogen-containing, and the second and
third generation bisphosphonates are nitrogen-containing
bisphosphonates. The difference between second and third generation
bisphosphonates is that the third generation bisphosphonates have
substitutes at the nitrogen segment of the molecule.
Through two different mechanisms impacting cell
functions, nitrogen-containing and non-nitrogen-containing
bisphosphonates cause osteoclast cell death. Whereas
non-nitrogen-containing bisphosphonates are built into the
phosphate chain of adenosine triphosphate, nitrogen-containing
bisphosphonates inhibit farnesyl pyrophosphate synthase (1).
The side-effects of bisphosphonates can be
categorized into four major groups: Acute phase reactions,
gastro-intestinal side-effects, effects on the kidneys and
bisphosphonate-associated osteonecrosis of the jaws (BP-ONJ)
(2). These necroses are usually
associated with the higher potent nitrogen-bisphosphonates
(3).
According to the American Association of Oral and
Maxillofacial Surgeons, BP-ONJ is defined as enorally exposed
necrotic bone existing for >8 weeks, with previous or current
bisphosphonate treatment and no radiation of the head and neck area
(4).
In the majority of the patients, a further trigger
factor in the development of BP-ONJ in addition to the
bisphosphonate treatment is often described, such as previous
extractions, periodontal diseases, pressure denture sores or
surgical procedures (4,5).
Since the etiopathology of BP-ONJ is not
definitively known, several theories regarding the development of
BP-ONJ are being discussed, which are as follows (6). i) The most common theory describes
reduced bone remodeling due to bisphosphonate-induced osteoclast
inhibition and accumulation of microfractures (7). ii) Another theory stresses the
anti-angiogenic effect of bisphosphonates resulting in the
development of avascular osteonecrosis of the jaws. The negative
influence of bisphosphonates on endothelial cells is supported by
the negative effect on the number of circulating endothelial cells
(8,9). iii) Bisphosphonates also have a
negative effect on bone covered by soft tissues; this bone is more
likely to be exposed (10,11).
All these effects have a negative impact on wound
healing and could partially contribute to the development of
BP-ONJ. In vitro studies support the negative impact of
bisphosphonates on osteoblasts, fibroblasts and endothelial cells
(9,11).
Depending on the prognosis of the underlying disease
and the stage of BP-ONJ, several therapy options are carried out.
The therapeutic options include mouth rinses, antibiotics,
debridements, sequestrectomies, partial resections and continuity
resections (4). However, the
recurrence rate of BP-ONJ in treated patients is extremely high
(4). A previous method used is the
ablation of osteonecrotic sites by Er:YAG laser (12). A further supportive option in the
treatment of these patients may be the application of low-level
laser therapy (LLLT). A positive effect on the proliferation rate
of fibroblasts (13) and
osteoblasts (14), and the
acceleration of bone formation (15) has previously been described.
To evaluate the influence of the effect of LLLT on
bisphosphonate-incubated cells involved in wound healing, an in
vitro study was performed to investigate the possible positive
effect of LLLT on cell viability. The aim of the present study was
to investigate the influence of LLLT on cell viability and on the
potential to decrease the negative effects of bisphosphonates on
cells.
Materials and methods
Cell culture
Human umbilical cord vein endothelial cells (HUVEC),
human gingival fibroblasts (HGF) (Lonza Group AG, Basel,
Switzerland), human osteogenic cells (HHOB-c; PromoCell GmbH,
Heidelberg, Germany) and human oral keratinocytes (HOK; Provitro,
Heidelberg, Germany) were examined. The cells were cultured in an
incubator with 5% CO2 at 37̊C. Cells were passaged at
regular intervals depending on their growth characteristics using
0.25% trypsin (Biochrom GmbH, Berlin, Germany).
HOKs were cultured in keratinocyte growth medium,
(Provitro GmbH, Berlin, Germany). The medium contained fibroblast
growth factor (FGF), epidermal growth factor (EGF),
Ca2+<0,1 mmol/l and insulin, but without bovine
pituitary extract and hydrocortisone.
HGFs were grown in stroma cell growth medium (Lonza
Group AG) with 1% penicillin-streptomycin-neomycin antibiotic
mixture (PSN), 10% FCS and 500 ng basic FGF in 500 ml medium.
HUVECs were cultured in an endothelial basal medium
supplemented with 1 µg/ml hydrocortisone, 12 µg/ml bovine brain
extract, 50 µg/ml gentamicin, 50 ng/ml amphotericin-B, 10 ng/mL EGF
and 10% FCS until the third passage.
Osteogenic cells were cultivated in a solution
composed of Dulbecco's modified Eagle's medium with 1% PSN, 1%
L-glutamine and 10% FCS.
Bisphosphonates
Due to the results of a previous study (16), the cells were incubated with 50 µmol
of clodronate, ibandronate, pamidronate or zoledronate for 24 h
prior to the cell viability test.
Laser irradiation
The cells were irradiated via a diode laser with 280
mW, at 670 nm for 60 sec (Periowave; Ondine Biopharma Corp.,
Toronto, Canada). During irradiation the laser tip was placed in
the medium.
Experimental group
The cells were transferred into 24-well dishes for
irradiation and bisphosphonate incubation. For each cell line, six
different experiments were performed. The first group was the
control group with no irradiation or bisphosphonate treatment. The
second group underwent irradiation only. The third group had no
irradiation but underwent bisphosphonate treatment. The cells in
group four were irradiated shortly following incubation with
bisphosphonates. The cells in group five were treated vice versa to
group four. For the last group, the medium was mixed with
bisphosphonates and irradiated prior to placing the osteoblasts
into the medium (Fig. 1).
MTT-test
To examine the cell viability of all four cell
lines, a 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium
bromide colorimetric assay (MTT M5655; Sigma-Aldrich Produktions
GmbH, Steinheim, Germany) was performed. Tetrazolium bromide is
fermented to formazan by viable cells. Formazan can be measured
photometrically following cell lysis at 550 nm. The experiments
were performed six times for each of the groups as specified
above.
Statistical analysis
Continuous variables are expressed as mean ±
standard error of mean. Comparisons between groups were analyzed by
analysis of variance (ANOVA; post hoc test: Tukey). The software
SPSS 16.0 for Windows (SPSS, Inc., Chicago, IL, USA) was used for
calculations. P<0.05 was considered to indicate a statistically
significant difference.
Results
ANOVA
For each cell type, the four ANOVAs conducted (one
for each bisphosphonate tested) showed significant differences
among the control and experimental groups. Each ANOVA yielded a
P-value of <0.001.
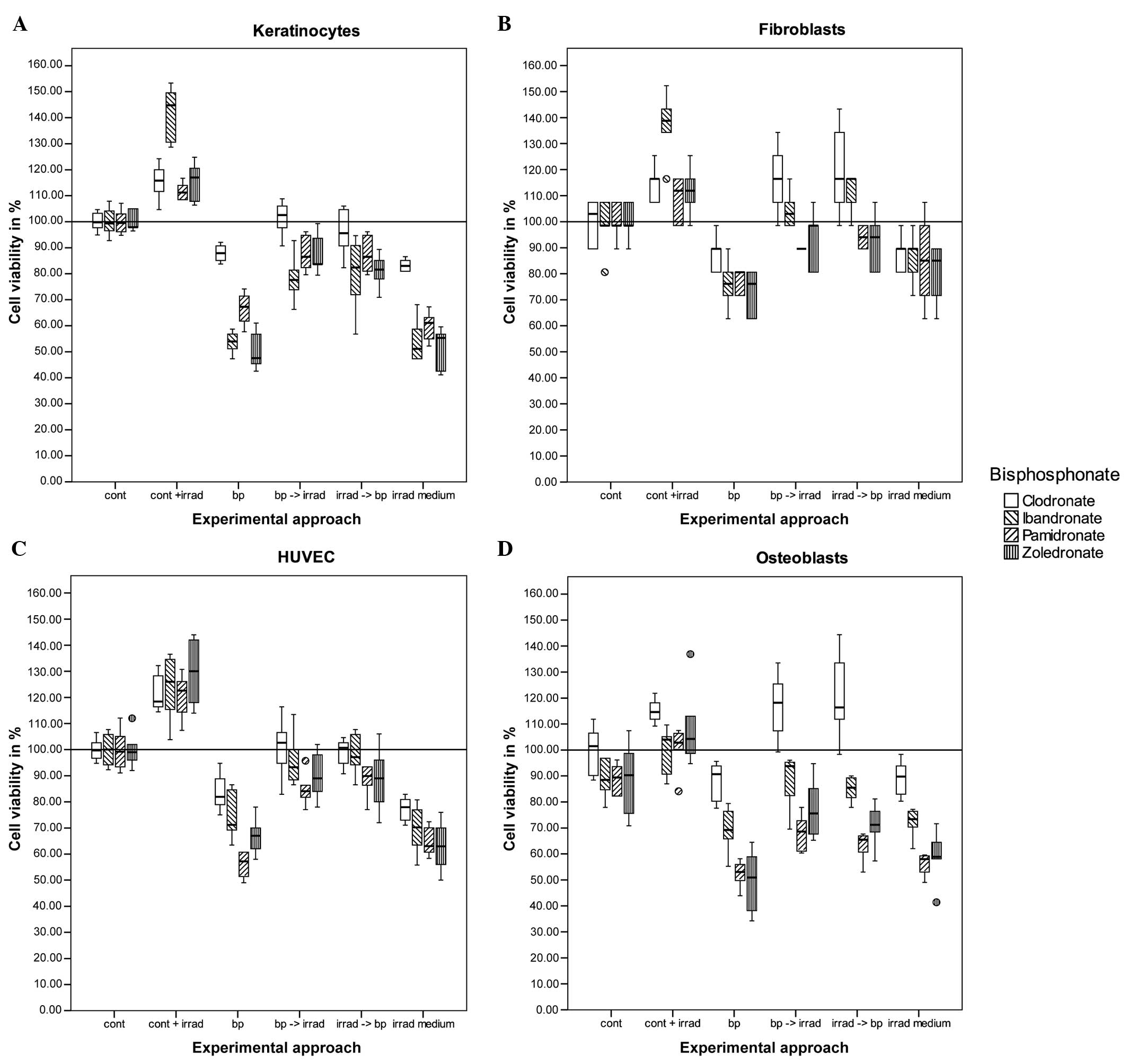
Keratinocytes
The exclusive irradiation of keratinocytes increased
cell viability significantly as compared to the control group
(P=0.015). Cells that were only treated with bisphosphonates had
reduced cell viability: Clodronate, P=0.027; and ibandronate,
pamidronate and zoledronate, P<0.001. There were no significant
differences in the two approaches of combining irradiation and
bisphosphonate treatment in different orders. The differences
between the cells incubated with bisphosphonate and the cells that
were additionally irradiated were significant for all the groups
(P<0.001), except for one experimental approach in the
clodronate group. In this group, the sequence of irradiation
followed by bisphosphonate treatment had no significant difference
(P=0.285), but in the reverse sequence the P-value was 0.010. For
all the other approaches, the P-values were ≤0.001. There was no
significant difference between the cells incubated with
bisphosphonates and the cells that were grown in
bisphosphonate-containing medium that was irradiated (Fig. 1A).
Fibroblasts
Although the viability was increased following laser
stimulation, there was no significant difference between the
control cells and the cells with laser stimulation in three out of
four tests. A significant difference was only obtained in the
experiments using ibandronate (P<0.001). The addition of 50 µmol
bisphosphonate reduced the viability significantly for ibandronate
(P=0.001), pamidronate (P=0.004) and zoledronate (P<0.001), but
not for clodronate (P=0.336). There was no significant difference
between the sequence of bisphosphonate treatment and laser
treatment, but there was a significant difference between the cells
incubated with bisphosphonates only and the cells that were
additionally irradiated. P-values for clodronate and ibandronate
were <0.001, and for pamidronate a P-value of 0.093, compared to
the cells incubated with bisphosphonates first and irradiated
subsequently. The cells treated with pamidronate in the reverse
order (irradiation first) had a P-value of 0.039. The cells treated
with zoledronate had a significance difference with P=0.001 for the
two approaches. The analysis of the cells with irradiation of the
cell-free bisphosphonate-containing medium revealed no differences
compared to the experimental approach with the incubation of cells
with bisphosphonates only [P-values ranging between P=0.349
(ibandronate) and P=1.000 (clodronate)] (Fig. 1B).
HUVEC
The treatment consisting exclusively of radiation
and bisphosphonates revealed significant changes in cell viability.
Irradiation increased the viability, with P-values between
P<0.001 and P=0.002, and bisphosphonate treatment decreased the
viability, with P-values between P<0.001 and P=0.004. The
combination of irradiation and bisphosphonate treatment increased
cell viability significantly, independent of order with P-values
between P<0.001 and P=0.008. There was no difference between the
cells treated with bisphosphonates and the cells treated with
irradiated medium [P-values between P=0.251 (pamidronate) and
P=0.981 (zoledronate)] (Fig.
1C).
Osteoblasts
Low-level laser application increased the viability
of cells, but was significant only in the experimental approach
with pamidronate (P=0.026), and had a significant tendency with
zoledronate (P=0.076). Adding bisphosphonates reduced the cell
viability in the ibandronate (P=0.002), pamidronate and
zoldedronat-treated assays (P<0.001). Osteoblasts treated with
clodronate had no significant reduction in cell viability. The
sequence of irradiation and bisphosphonate treatment did not result
in significant differences for any of the cell lines. However, the
additional irradiation of the cells treated with bisphosphonates
increased the cell viability in all the cases, with P-values
ranging from P<0.001 (clodronate) to P=0.046 (pamidronate and
zoledronate). There was no significant difference between the cells
treated with bisphosphonates only and the cells receiving the
bisphosphonate medium that had been irradiated, with P-values
ranging between P=0.761 (zoledronate) and P=1.000 (clodronate)
(Fig. 1D).
Discussion
The development of BP-ONJ may be initiated due to
several reasons. In addition to the influence of bisphosphonate on
several cell lines of the oral cavity (11), further factors are frequently
described, including previous tooth extractions, the presence of
periodontal disease, pressure denture sores or dental surgical
procedures (3,5). Guidelines regarding BP-ONJ have been
published worldwide (4,16–18).
In addition to treatment recommendations, the prevention of BP-ONJ
is emphasized, as successful treatment is difficult due to high
recurrence rates.
Frequent recommendations to prevent BP-ONJ include
introducing the patient to dental treatment prior to bisphosphonate
therapy, with the aim to establish or maintain good oral hygiene.
In patients already receiving bisphosphonates, where possible,
discontinuing bisphosphonate treatment when a dental surgical
procedure is necessary is also being investigated, as well as
maintaining good oral hygiene. The CTX-level (c terminal
telopeptide of collagen) as a marker for the risk of developing a
BP-ONJ has been discussed previously (19,20).
The treatment of BP-ONJ ranges from mouth rinses to resection of
the affected area.
The positive effect of low-level laser therapy on
cell growth of different cells of the oral cavity is well known
(13–15) and used in surgery to accelerate
wound repair (21). Explanations
for this effect are an increased mitotic activity or changes in
collagen synthesis (13). The
negative impact of bisphosphonates on different cell lines has been
described previously (11). Certain
case series have reported the application of laser biostimulation
in the treatment of patients with BP-ONJ and reviewed the benefit
for patients undergoing this treatment (22,23).
In the present study, the influence of laser
stimulation on keratinocytes, fibroblasts, HUVEC and osteoblasts
has been analyzed, which are the cells that are negatively
influenced by bisphosphonates. The negative impact on all these
cells may contribute to the development of BP-ONJ. The results
revealed a positive effect of low-level laser stimulation on
keratinocytes and endothelial cells, and a negative effect of
bisphosphonates on all the tested cell lines. The laser stimulation
of bisphosphonate-treated cells increased cell viability in all
cell lines, particularly for fibroblasts treated with clodronate,
which had even higher levels compared to the control group. The
radiation of the bisphosphonate-containing cell medium did not
change the cell viability of the different cell lines compared to
the experiment approach of cells incubated with bisphosphonate
only. An interference of irradiation with bisphosphonate can be
excluded, so that the effect is based on the influence of the
irradiation on the cells.
In conclusion, these data support the idea of using
low-level laser stimulation as a supportive therapy in patients
receiving bisphosphonates to avoid BP-ONJ development and in
patients being treated due to BP-ONJ.
Acknowledgements
The authors would like to thank Katherine Joyce
(MSE) for the statistical and language assistance. Dr Christian
Walter (MD, DDS, PhD) received speaker's fees from Roche (Basel,
Switzerland) and financial help for another research project from
Novartis.
References
|
1
|
Fleisch H: Bisphosphonates in
osteoporosis. Eur Spine J. 12:S142–S146. 2003. View Article : Google Scholar
|
|
2
|
Diel IJ, Bergner R and Grötz KA: Adverse
effects of bisphosphonates: current issues. J Support Oncol.
5:475–482. 2007.PubMed/NCBI
|
|
3
|
Walter C, Grötz KA, Kunkel M and Al-Nawas
B: Prevalence of bisphosphonate associated osteonecrosis of the jaw
within the field of osteonecrosis. Support Care Cancer. 15:197–202.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ruggiero SL, Dodson TB, Assael LA,
Landesberg R, Marx RE and Mehrotra BAmerican Association of Oral
and Maxillofacial Surgeons: American Association of Oral and
Maxillofacial Surgeons position paper on bisphosphonate-related
osteonecrosis of the jaws-2009 update. J Oral Maxillofac Surg.
67:2–12. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Walter C, Al-Nawas B, Grötz KA, Thomas C,
Thüroff JW, Zinser V, Gamm H, Beck J and Wagner W: Prevalence and
risk factors of bisphosphonate-associated osteonecrosis of the jaw
in prostate cancer patients with advanced disease treated with
zoledronate. Eur Urol. 54:1066–1072. 2008. View Article : Google Scholar
|
|
6
|
Allen MR and Burr DB: The pathogenesis of
bisphosphonate-related osteonecrosis of the jaw: so many
hypotheses, so few data. J Oral Maxillofac Surg. 67 (Suppl
5):S61–S70. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mashiba T, Hirano T, Turner CH, Forwood
MR, Johnston CC and Burr DB: Suppressed bone turnover by
bisphosphonates increases microdamage accumulation and reduces some
biomechanical properties in dog rib. J Bone Miner Res. 15:613–620.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fournier P, Boissier S, Filleur S,
Guglielmi J, Cabon F, Colombel M and Clézardin P: Bisphosphonates
inhibit angiogenesis in vitro and testosterone-stimulated vascular
regrowth in the ventral prostate in castrated rats. Cancer Res.
62:6538–6544. 2002.PubMed/NCBI
|
|
9
|
Ziebart T, Pabst A, Klein MO, Kämmerer P,
Gauss L, Brüllmann D, Al-Nawas B and Walter C: Bisphosphonates:
restrictions for vasculogenesis and angiogenesis: inhibition of
cell function of endothelial progenitor cells and mature
endothelial cells in vitro. Clin Oral Investig. 15:105–111. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Landesberg R, Cozin M, Cremers S, Woo V,
Kousteni S, Sinha S, Garrett-Sinha L and Raghavan S: Inhibition of
oral mucosal cell wound healing by bisphosphonates. J Oral
Maxillofac Surg. 66:839–847. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Walter C, Klein MO, Pabst A, Al-Nawas B,
Duschner H and Ziebart T: Influence of bisphosphonates on
endothelial cells, fibroblasts, and osteogenic cells. Clin Oral
Investig. 14:35–41. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Stübinger S, Dissmann JP, Pinho NC,
Saldamli B, Seitz O and Sader R: A preliminary report about
treatment of bisphosphonate related osteonecrosis of the jaw with
Er:YAG laser ablation. Lasers Surg Med. 41:26–30. 2009.PubMed/NCBI
|
|
13
|
Pereira AN, Eduardo Cde P, Matson E and
Marques MM: Effect of low-power laser irradiation on cell growth
and procollagen synthesis of cultured fibroblasts. Lasers Surg Med.
31:263–267. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Fujihara NA, Hiraki KR and Marques MM:
Irradiation at 780 nm increases proliferation rate of osteoblasts
independently of dexamethasone presence. Lasers Surg Med.
38:332–336. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ninomiya T, Miyamoto Y, Ito T, Yamashita
A, Wakita M and Nishisaka T: High-intensity pulsed laser
irradiation accelerates bone formation in metaphyseal trabecular
bone in rat femur. J Bone Miner Metab. 21:67–73. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Khan AA, Sándor GK, Dore E, Morrison AD,
Alsahli M, Amin F, Peters E, Hanley DA, Chaudry SR, Dempster DW,
Glorieux FH, Neville AJ, Talwar RM, Clokie CM, Al Mardini M, Paul
T, Khosla S, Josse RG, Sutherland S, Lam DK, Carmichael RP, Blanas
N, Kendler D, Petak S, St-Marie LG, Brown J, Evans AW, Rios L and
Compston JECanadian Association of Oral and Maxillofacial Surgeons:
Canadian consensus practice guidelines for bisphosphonate
associated osteonecrosis of the jaw. J Rheumatol. 35:1391–1397.
2008.PubMed/NCBI
|
|
17
|
Grötz KA and Kreusch T: Zahnärztliche
Betreuung von Patienten unter/nach Bisphosphonat-Medikation. DZZ.
60:102006.(In German).
|
|
18
|
Bagán J, Blade J, Cozar JM, Constela M,
García Sanz R, Gómez Veiga F, Lahuerta JJ, Lluch A, Massuti B,
Morote J, San Miguel JF and Solsona E: Recommendations for the
prevention, diagnosis, and treatment of osteonecrosis of the jaw
(ONJ) in cancer patients treated with bisphosphonates. Med Oral
Patol Oral Cir Bucal. 12:E336–E340. 2007.
|
|
19
|
Marx RE, Cillo JE Jr..Ulloa JJ: Oral
bisphosphonate-induced osteonecrosis: risk factors, prediction of
risk using serum CTX testing, prevention, and treatment. J Oral
Maxillofac Surg. 65:2397–2410. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bagan JV, Jimenez Y, Gomez D, Sirera R,
Poveda R and Scully C: Collagen telopeptide (serum CTX) and its
relationship with the size and number of lesions in osteonecrosis
of the jaws in cancer patients on intravenous bisphosphonates. Oral
Oncol. 44:1088–1089. 2008. View Article : Google Scholar
|
|
21
|
Pinheiro Al, Cavalcanti ET, Pinheiro TI,
Alves MJ and Manzi CT: Low-level laser therapy in the management of
disorders of the maxillofacial region. J Clin Laser Med Surg.
15:181–183. 1997.PubMed/NCBI
|
|
22
|
Merigo E, Manfredi M, Meleti M, Guidotti
R, Ripasarti A, Zanzucchi E, D'Aleo P, Corradi D, Corcione L,
Sesenna E, Ferrari S, Poli T, Bonaninil M and Vescovi P: Bone
necrosis of the jaws associated with bisphosphonate treatment: a
report of twenty-nine cases. Acta Biomed. 77:109–117.
2006.PubMed/NCBI
|
|
23
|
Vescovi P, Merigo E, Manfredi M, Meleti M,
Fornaini C, Bonanini M, Rocca JP and Nammour S: Nd:YAG laser
biostimulation in the treatment of bisphosphonate-associated
osteonecrosis of the jaw: clinical experience in 28 cases. Photomed
Laser Surg. 26:37–46. 2008. View Article : Google Scholar
|