Introduction
Coronary artery calcification (CAC) is a basic
pathological change in coronary atherosclerotic heart disease and
often indicates further morbidities (1,2). Currently,
the most common method of assessment of calcification is multislice
computed tomography, and calcification is calculated by using
methods such as Agatston, quality and volume integrals. The
parathyroid hormone (PTH) is a linear peptide comprising 84 amino
acids secreted by parathyroid lord cells, which are mainly
implicated in the regulation of calcium phosphorus metabolism.
Previous studies have shown that PTH induces high blood pressure
and myocardial hypertrophy, is closely associated with heart
failure and can even predict the occurrence of coronary heart
disease (3–6). In recent years, the association between
PTH and CAC has become a research hotspot. The results of previous
studies suggested that PTH levels were not associated with the
baseline CAC score (CACS), but with CAC progression (7–11). All of
the patients included in these studies suffered from kidney failure
with or without hemodialysis. However, whether PTH levels are
positively correlated with CAC in patients without renal failure
has remained elusive. The purpose of the present study was to
investigate the correlation between serum PTH levels and CAC in
patients without renal failure, as well as independent risk factors
of CACS.
Materials and methods
Patients
A total of 225 consecutive patients who underwent
coronary CTA examination at the 101th Hospital of the People's
Liberation Army (PLA) (Wuxi, China) between December 2013 and
February 2015 were retrospectively evaluated. After excluding
patients with acute myocardial infarction, heart valve disease,
heart failure, a glomerular filtration rate <60 ml/min or
transaminase levels three times higher than the upper limit of the
99% reference range, malignant tumors, systemic infection, or
autoimmune or connective tissue disease, 157 patients were
enrolled. Heart failure was diagnosed according to the Chinese
heart failure diagnosis and treatment guidelines from 2014
(12).
The Medical Ethics Committee of The 101th Hospital
of the PLA approved the present retrospective study (protocol no.
20150052). Each patient signed a consent form agreeing to the
storage of their information in the hospital's database and use for
scientific studies.
Experimental methods
Patient data regarding hypertension, diabetes,
hyperlipidemia, as well as history of smoking and alcohol
consumption were collected and patients were stratified according
to their positive or negative status. The body mass index (BMI) was
calculated by dividing weight by the square of the height.
A total of 3 ml venous blood had been taken from
each patient in the fasting state and subjected to laboratory
analysis. Total cholesterol (TC), electrolytes, triglycerides
(TGs), C-reactive protein (CRP), creatinine, high-density
lipoprotein cholesterol (HDL-C), low-density lipoprotein
cholesterol (LDL-C) and fasting blood glucose (FBG) levels were
measured with an automatic biochemical analyzer (AU5800; Olympus,
Tokyo, Japan). Serum PTH levels were measured using a
chemiluminescence method (PTH ELISA kit; GETEIN Co., Nanjing,
China). The glomerular filtration rate (GFR) was calculated by
using the equation: GFR (ml/min × 73 m−2) = [140 - age
(years)] × weight (Kg)/0.818 × creatinine concentration (µmol/l).
For women, the resulting value was multiplied by 0.85.
For coronary computed tomography (CT) scanning, the
Toshiba 320 row spiral CT scanner (Toshiba, Tokyo, Japan) was used.
The CACS was calculated by using a Toshiba vital 6.2 workstation
(Toshiba, Tokyo, Japan) according to the Agatston integral
(13), which was operated by a
technician. Patients with CACS>0 were assigned to the CAC
group.
Heart Doppler examination was performed by cardiac
ultrasonography using an ultrasonographic diagnostic instrument
(vivid E9; GE Healthcare, Little Chalfont, UK), through which
degenerative heart valve disease was diagnosed.
Statistical analysis
All statistical analyses were performed by using
SPSS 15.0 (SPSS, Inc., Chicago, IL, USA). Continuous variables were
presented as the mean ± standard deviation, and analysis of
variance and least significant difference tests were applied to
compare differences between groups. Categorical variables were
presented as percentages and determined by using the χ2
test. The Pearson rank order was used to analyze the correlations.
A receiver operating characteristic (ROC) curve was drawn to
determine the predictive value of PTH for CAC. The best cut-off PTH
level to predict CAC was determined by using PTH values that
provide the maximum sum of sensitivity and specificity. Indicators
including gender, age, smoking status, diabetes, hypertension,
hyperlipidemia, BMI, GFR, levels of serum calcium, serum
phosphorus, calcium-phosphorus product (CPP), serum magnesium, PTH,
TC, LDL-C, TG, HDL-C and CRP were assessed using the logistic
regression analysis model with the response variable Be binary
class in order to determine independent factors correlated with
CAC, presented as odds ratio (OR) and 95% confidence interval (CI).
P<0.05 was considered to indicate a statistically significant
difference.
Results
Patient data
The present study included 68 patients with CAC,
comprising 41 men and 27 women, with a mean CACS of 402.49±666.3
and serum PTH levels of 48.70±21.39 pg/ml (range, 20.40–123 pg/ml;
normal, 14–72 pg/ml), and 89 patients without CAC, including 49 men
and 40 women, with a mean serum PTH level of 31.98±16.03 pg/ml
(12.00–86.90 pg/ml). The two groups displayed statistically
significant differences in terms of age, PTH levels, GFR and blood
phosphorus level, smoking status and frequency of coronary heart
disease (P<0.05). However, no significant differences were
observed in BMI, calcium, magnesium, CPP, cholesterol, FBG and CRP
levels, as well as gender, hypertension, diabetes, hyperlipidemia
and alcohol use (P>0.05).
In addition, the 157 patients were further
stratified based on the CACS as follows: CACS≤100 (n=118 patients)
and CACS>100 (n=39). The two groups only significantly differed
in terms of age, PTH levels, GFR and the frequency of coronary
heart disease (P<0.05) (Tables I
and II).
 | Table I.Gender and disease constitution in
patients with and without calcification. |
Table I.
Gender and disease constitution in
patients with and without calcification.
| Parameter | No calcification
group (n=89) | Calcification group
(n=68) | χ2 | P-value | CACS≤100 (n=118) | CACS>100
(n=39) | χ2 | P-value |
|---|
| Males, n (%) | 49 (55.06) | 41 (60.29) | 0.432 | 0.511 | 67 (56.78) | 23 (58.97) | 0.058 | 0.810 |
| CAD, n (%) | 23 (25.84) | 56 (82.35) | 49.241 | < 0.001 | 44 (37.29) | 35 (89.74) | 32.263 | 0.000 |
| Hypertension, n
(%) | 60 (67.42) | 54 (79.41) | 2.789 | 0.095 | 85 (72.03) | 29 (74.36) | 0.080 | 0.778 |
| Diabetes, n (%) | 12 (13.48) | 14 (20.59) | 1.408 | 0.235 | 16 (13.56) | 10 (25.64) | 3.096 | 0.078 |
| Hyperlipaemia, n
(%) | 17 (19.10) | 10 (14.71) | 0.523 | 0.470 | 22 (18.64) | 5 (12.82) | 0.698 | 0.403 |
| Smoking, n (%) | 17 (19.10) | 24 (35.29) | 5.239 | 0.022 | 28 (23.73) | 13 (33.33) | 1.401 | 0.236 |
| Alcohol, n (%) | 2 (2.25) | 7 (10.29) | 3.250 | 0.071 | 7 (5.93) | 2 (5.13) | 0.035 | 0.851 |
| Cardiomyopaty, n
(%) | 0 (0) | 0 (0) | – | – | 0 (0) | 0 (0) | – | – |
| Atrial fibrillation,
n (%) | 5 (5.62) | 2 (2.94) | 0.172 | 0.678 | 7 (5.93) | 0 (0) | 1.229 | 0.268 |
| Table II.Clinical and biochemical parameters of
patients with and without calcification. |
Table II.
Clinical and biochemical parameters of
patients with and without calcification.
| Parameter | No calcification
group (n=89) | Calcification group
(n=68) | t-value | P-value | CACS≤100
(n=118) | CACS>100
(n=39) | t-value | P-value |
|---|
| Age (years) | 59.82±11.50 | 68.38±10.05 | 4.879 | < 0.001 | 60.94±11.01 | 71.36±10.09 | 5.228 | <0.001 |
| BMI
(kg/m2) | 24.86±3.28 | 23.94±3.39 | 1.725 | 0.087 | 24.65±3.28 | 23.91±3.54 | 1.203 | 0.231 |
| PTH (pg/ml) | 31.98±16.03 | 48.70±21.39 | 5.391 | < 0.001 | 35.87±19.68 | 49.37±18.76 | 3.755 | <0.001 |
| GFR
(ml/min/1.73m2) | 102.16±29.54 | 84.49±22.47 | 4.108 | < 0.001 | 98.97±28.43 | 80.99±22.15 | 3.603 | <0.001 |
| Ca (mmol/l) | 2.28±0.13 | 2.28±0.15 | 0.088 | 0.930 | 2.28±0.13 | 2.27±0.15 | 0.725 | 0.470 |
| Mg (mmol/l) | 0.81±0.09 | 0.82±0.08 | 0.043 | 0.966 | 0.81±0.09 | 0.83±0.09 | 1.264 | 0.208 |
| P (mmol/l) | 1.12±0.16 | 1.07±0.18 | 2.095 | 0.038 | 1.11±0.17 | 1.06±0.18 | 1.715 | 0.088 |
| CPP
(mmol2/l2) | 2.57±0.42 | 2.43±0.44 | 1.971 | 0.050 | 2.54±0.42 | 2.40±0.46 | 1.755 | 0.081 |
| FBG (mmol/l) | 5.36±1.35 | 5.54±1.40 | 0.828 | 0.409 | 5.41±1.35 | 5.54±1.44 | 0.524 | 0.601 |
| TC (mmol/l) | 4.26±0.90 | 4.11±0.91 | 1.019 | 0.310 | 4.21±0.88 | 4.17±0.99 | 0.201 | 0.841 |
| TG (mmol/l) | 1.81±1.26 | 1.60±1.41 | 0.962 | 0.338 | 1.74±1.15 | 1.65±1.77 | 0.393 | 0.695 |
| HDL-C (mmol/l) | 1.23±0.29 | 1.18±0.26 | 1.145 | 0.254 | 1.22±0.29 | 1.19±0.25 | 0.586 | 0.559 |
| LDL-C (mmol/l) | 2.05±0.67 | 2.04±0.69 | 0.080 | 0.936 | 2.04±0.66 | 2.06±0.74 | 0.103 | 0.918 |
| CRP (mg/l) | 3.07±7.05 | 7.07±18.81 | 1.668 | 0.099 | 4.51±14.60 | 5.68±9.88 | 0.467 | 0.641 |
Correlation of PTH levels and calcium score as well
as metabolic measures. The results of the Pearson correlation
analysis showed that among all of the patients included in the
present study, the PTH levels were positively correlated with the
CACS (r=0.288, P<0.001), while they were negatively correlated
with the GFR, phosphorus levels and CPP (r=−0.207, P=0.011;
r=−0.231, P=0.005; and r=−0.225, P=0.006, respectively). However,
in the calcification group, no significant correlation was observed
in this respect (r=0.186, P=0.130; Tables III and IV).
| Table III.Correlation analysis for parathyroid
hormone and biological metabolic parameters. |
Table III.
Correlation analysis for parathyroid
hormone and biological metabolic parameters.
| Parameter | r-value | P-value |
|---|
| GFR | −0.207 | 0.011 |
| Calcium | 0.023 | 0.778 |
| Magnesium | 0.006 | 0.945 |
| Inorganic
phosphate | −0.231 | 0.005 |
| CPP | −0.225 | 0.006 |
| FBG | 0.139 | 0.092 |
| TC | 0.011 | 0.892 |
| TG | −0.029 | 0.726 |
| HDL-C | 0.051 | 0.538 |
| LDL-C | −0.032 | 0.702 |
| CRP | −0.033 | 0.690 |
| Table IV.Correlation analysis for parathyroid
hormone and calcification scores. |
Table IV.
Correlation analysis for parathyroid
hormone and calcification scores.
| Group | r-value | P-value |
|---|
| Calcification + no
calcification | 0.288 | <0.001 |
| Calcification | 0.186 | 0.130 |
Serum PTH levels in patients with CACS≤10 (n=98)
were significantly lower than those in patients with 10<CACS≤100
(n=20) and CACS>100 (n=39) (P<0.001 for each). However, no
significant differences were observed in PTH levels between
patients with 10<CACS≤100 and CACS>100 (P=0.626) (Table V).
| Table V.Parathyroid hormone levels in
patients with three degrees of CAC. |
Table V.
Parathyroid hormone levels in
patients with three degrees of CAC.
|
|
| 95% CI for mean
difference |
|---|
|
|
|
|
|---|
| Groups | P-value | Lower | Upper |
|---|
| CACS≤10 and
10<CACS<100 | <0.001 | −28.19 | −10.28 |
| CACS≤10 and
CACS>100 | <0.001 | −23.66 | −9.85 |
| 10<CACS≤100 and
CACS>100 | 0.626 | −7.56 | 12.52 |
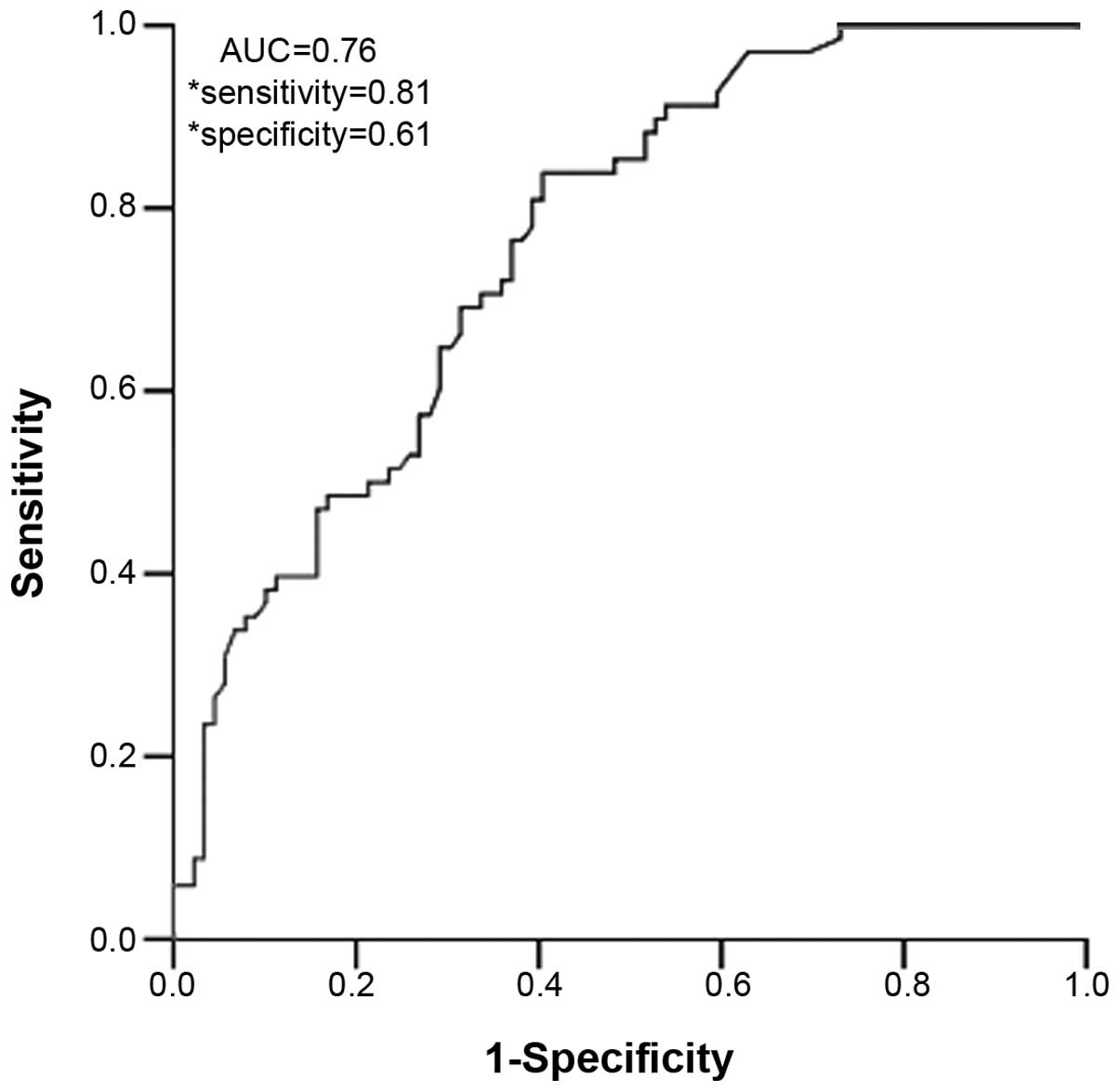
Predictive value of PTH for CAC. The ROC curve
revealed that PTH levels of ≥31.05 pg/ml are optimal for the
prediction of CAC, with a sensitivity of 80.88%, a specificity of
60.67% and an area under the curve of 0.76 (P<0.001; Fig. 1).
Independent predictors of CAC. The results of the
logistic regression analysis model with the response variable Be
binary class showed that PTH levels (OR=1.050; 95% CI, 1.050–1.074;
P<0.001) and smoking (OR=2.513; 95% CI, 2.513–5.731; P=0.029)
were predictors of CAC and that the GFR (OR=0.975, 95% CI
0.961–0.991; P=0.002) was negatively associated with CAC
(P<0.05; Table VI). None of the
other factors assessed had any predictive value regarding CAC
(P>0.05). Overall, the results supported the significance of PTH
levels in terms of prediction of CAC.
| Table VI.Binary logistic regression analysis
of independent predictors for coronary artery calcification. |
Table VI.
Binary logistic regression analysis
of independent predictors for coronary artery calcification.
| Indicators | B | Wald | P-value | OR | 95% CI |
|---|
| PTH | 0.049 | 18.231 | <0.001 | 1.050 | 1.027–1.074 |
| Smoking | 0.921 | 4.795 | 0.029 | 2.513 | 1.102–5.731 |
| GFR | −0.025 | 9.972 | 0.002 | 0.975 | 0.961–0.991 |
Discussion
CAC arises from calcium salt deposition via
atheromatous plaque rupture and hemorrhage-induced composite
patches. Previous studies have confirmed that hypertension,
diabetes, gender, age and other cardiovascular risk factors are
involved in the formation of CAC (14). The results of the present study showed
that the mean age and smoking status of the patients in the CAC
group were significantly higher than those in the non-calcification
group, which was consistent with the results of previous studies
(15,16). While in the CAC group, the number of
patients with high blood pressure and diabetes, and the proportion
of men were higher than those in the group without calcification,
the difference did not reach statistical significance, possibly due
to factors such as the small overall sample size and the fact that
the number of patients without calcification was higher than that
of patients with calcification.
The degree of CAC can predict the extent of coronary
artery stenosis, affect the therapeutic efficacy of coronary artery
intervention and predict the incidence of cardiovascular events,
regardless of whether patients had clinical symptoms (17,18).
Therefore, an accurate prediction of the degree of CAC is
significant in clinical practice. In addition to the most commonly
used imaging techniques at present, laboratory indexes, including
lipoprotein(a), endothelin 1 and bone morphogenetic protein 2
levels, are also associated with calcification and may be utilized
to assess the degree of CAC (19–21). To
date, the association between serum calcium, phosphorus, CPP and
CAC has been most widely discussed in previous studies (22,23);
however, the conclusions are not consistent. The presence of
cardiovascular risk factors may affect the results of these
studies. According to the present consensus, calcification is
considered as the result of calcium phosphorus metabolism
disorders, transformation of vascular endothelial cells to
osteoblasts and calcium balance disorders (24). PTH mainly regulates calcium phosphorus
metabolism and vice versa, suggesting a feedback loop-like
association between PTH and calcification.
In fact, the results of a previous study indicated
that serum PTH levels were able to predict coronary heart disease
in subjects with calcium levels within the normal range (6). Hyperparathyroidism impairs coronary
microcirculation and PTH was shown to be independently correlated
with abnormal coronary flow reserve (25). Furthermore, several studies have
pointed out the important effect of PTH overexpression on
cardiovascular disease, including carotid artery, abdominal aortic
and valvular calcifications, as well as CAC (26–30), while
most of these studies focused on patients with renal failure, which
is known to induce secondary hyperparathyroidism. However, the
results of previous studies are inconsistent with regard to whether
renal insufficiency is associated with CAC. Ix et al
(31) reported that the association
between mild-to-moderate renal insufficiency and CAC was not
statistically significant after adjusting cardiovascular risk
factors, while Fox et al (32)
concluded the opposite. Certain studies have argued that the
correlation only existed in patients >70 years of age or with
stage 3–5 chronic kidney disease (33,34).
Furthermore, it remains elusive whether renal failure influences
the association of PTH levels and CAC. In the present study, in
order to avoid interference, patients with GFR <60 ml/min were
excluded, and PTH remained an independent predictor of CAC after
including multiple cardiovascular risk factors; furthermore PTH
levels were positively correlated with the CACS in all patients.
However, in the calcification group, PTH levels did not show an
increasing trend corresponding with the increase in the calcium
score, which was different from the results of previous studies
(11,23). The small sample size of the
calcification group may be one of the reasons for this
observation.
All of the abovementioned results indicated that PTH
is independently correlated with CAC, irrespective of renal failure
being present. Moreover, PTH is easy to detect at low cost,
representing advantages over other biomarkers.
The limitations of the present study include, but
are not limited to the following points: Patients with heart
failure and heart valve disease were excluded; however, the
presence of peripheral artery calcification was not known. Calcium
metabolism is not only determined by the level of PTH, but vitamin
D also has a marked impact on it; however, the levels of vitamin
D-associated factors were not available in the present
retrospective study. Further limitations of the present study
included small sample size and number of parameters available; in
addition only a preliminarily analysis of the correlation between
PTH levels and CAC was performed. Therefore, the results of the
present study only indicated an association, and further studies
are therefore required to clarify the detailed mechanisms of the
impact of PTH on CAC.
In conclusion, the present study revealed that the
serum PTH levels correlated with CAC and may thus be used as a
reliable predictor of CAC in patients without renal failure;
however, it remains to be determined whether PTH is an independent
predictor of CAC.
Acknowledgements
The present study was supported by the National
Natural Science Fund of China (no. 81371657).
References
|
1
|
Shang CL, Wang Y, Bai J and Chen C: Effect
of moderate-severe calcified coronary lesions on immediate outcome
of percutaneous coronary intervention. Chin J Geriatr Heart Brain
Vessel Dis. 4:357–360. 2013.
|
|
2
|
Budoff MJ, Shaw LJ, Liu ST, Weinstein SR,
Mosler TP, Tseng PH, Flores FR, Callister TQ, Raggi P and Berman
DS: Long-term prognosis associated with coronary calcification:
Observations from a registry of 25,253 patients. J Am Coll Cardiol.
49:1860–1870. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Demir M, Günay T, Özmen G and Melek M:
Relationship between vitamin D deficiency and nondipper
hypertension. Clin Exp Hypertens. 35:45–49. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cha H, Jeong HJ, Jang SP, Kim JY, Yang DK,
Oh JG and Park WJ: Parathyroid hormone accelerates decompensation
following left ventricular hypertrophy. Exp Mol Med. 42:61–68.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sugimoto T, Dohi K, Onishi K, Watanabe K,
Sato Y, Sugiura E, Nakamori S, Nakajima H, Nakamura M and Ito M:
Interrelationship between haemodynamic state and serum intact
parathyroid hormone levels in patients with chronic heart failure.
Heart. 99:111–115. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kamycheva E, Sundsfjord J and Jorde R:
Serum parathyroid hormone levels predict coronary heart disease:
The Tromsø Study. Eur J Cardiovasc Prev Rehabil. 11:69–74. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Oka M, Ohtake T, Mochida Y, Ishioka K,
Maesato K, Moriya H, Hidaka S and Kobayashi S: Correlation of
coronary artery calcification with pre-hemodialysis bicarbonate
levels in patients on hemodialysis. Ther Apher Dial. 16:267–271.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ohtake T, Kobayashi S, Oka M, Furuya R,
Iwagami M, Tsutsumi D, Mochida Y, Maesato K, Ishioka K, Moriya H,
et al: Lanthanum carbonate delays progression of coronary artery
calcification compared with calcium-based phosphate binders in
patients on hemodialysis: A pilot study. J Cardiovasc Pharmacol
Ther. 18:439–446. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Iyer H, Abraham G, Reddy YN, Pandurangi
UM, Kalaichelvan U, Gomathi SB, Mathew M and Santhosham R: Risk
factors of chronic kidney disease influencing cardiac
calcification. Saudi J Kidney Dis Transpl. 24:1189–1194. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Daniel WT, Weber C, Bailey JA, Raggi P and
Sharma J: Prospective analysis of coronary calcium in patients on
dialysis undergoing a near-total parathyroidectomy. Surgery.
154:1315–1321. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Malluche HH, Blomquist G, Monier-Faugere
MC, Cantor TL and Davenport DL: High parathyroid hormone level and
osteoporosis predict progression of coronary artery calcification
in patients on dialysis. J Am Soc Nephrol. 26:2534–2544. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chinese Society of Cardiology of Chinese
Medical Association; Editorial Board of Chinese Journal of
Cardiology, . Chinese guidelines for the diagnosis and treatment of
heart failure 2014. Zhonghua Xin Xue Guan Bing Za Zhi. 42:98–122.
2014.(In Chinese). PubMed/NCBI
|
|
13
|
Agatston AS, Janowitz WR, Hildner FJ,
Zusmer NR, Viamonte M Jr and Detrano R: Quantification of coronary
artery calcium using ultrafast computed tomography. J Am Coll
Cardiol. 15:827–832. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bild DE, Detrano R, Peterson D, Guerci A,
Liu K, Shahar E, Ouyang P, Jackson S and Saad MF: Ethnic
differences in coronary calcification: The multi-ethnic study of
atherosclerosis (MESA). Circulation. 111:1313–1320. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hoffmann U, Massaro JM, Fox CS, Manders E
and O'Donnell CJ: Defining normal distributions of coronary artery
calcium in women and men (from the Framingham Heart Study). Am J
Cardiol. 102:1136–1141. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Loria CM, Liu K, Lewis CE, Hulley SB,
Sidney S, Schreiner PJ, Williams OD, Bild DE and Detrano R: Early
adult risk factor levels and subsequent coronary artery
calcification: The CARDIA Study. J Am Coll Cardiol. 49:2013–2020.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mosseri M, Satler LF, Pichard AD and
Waksman R: Impact of vessel calcification on outcomes after
coronary stenting. Cardiovasc Revasc Med. 6:147–153. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sharma RK, Sharma RK, Voelker DJ, Singh
VN, Pahuja D, Nash T and Reddy HK: Cardiac risk stratification:
Role of the coronary calcium score. Vasc Health Risk Manag.
6:603–611. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Greif M, Arnoldt T, von Ziegler F,
Ruemmler J, Becker C, Wakili R, D'Anastasi M, Schenzle J, Leber AW
and Becker A: Lipoprotein (a) is independently correlated with
coronary artery calcification. Eur J Intern Med. 24:75–79. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ping Q, Li Y, Jia Y, et al: Correlationg
between endothelin-1 and coronary artery calcification. Chin J
Geriatr Heart Brain Vessel Dis. 15:916–919. 2013.
|
|
21
|
Csiszar A, Smith KE, Koller A, Kaley G,
Edwards JG and Ungvari Z: Regulation of bone morphogenetic
protein-2 expression in endothelial cells: Role of nuclear
factor-kappaB activation by tumor necrosis factor-alpha,
H2O2, and high intravascular pressure.
Circulation. 111:2364–2372. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Block GA, Klassen PS, Lazarus JM, Ofsthun
N, Lowrie EG and Chertow GM: Mineral metabolism, mortality, and
morbidity in maintenance hemodialysis. J Am Soc Nephrol.
15:2208–2218. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Shin S, Kim KJ, Chang HJ, Cho I, Kim YJ,
Choi BW, Rhee Y, Lim SK, Yang WI, Shim CY, et al: Impact of serum
calcium and phosphate on coronary atherosclerosis detected by
cardiac computed tomography. Eur Heart J. 33:2873–2881. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Qiao H, Wu Y and Zeng H: Progress of
coronary artery calcification. Adv Cardiovasc Dis. 31:715–718.
2010.
|
|
25
|
Osto E, Fallo F, Pelizzo MR, Maddalozzo A,
Sorgato N, Corbetti F, Montisci R, Famoso G, Bellu R, Lüscher TF,
et al: Coronary microvascular dysfunction induced by primary
hyperparathyroidism is restored after parathyroidectomy.
Circulation. 126:1031–1039. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Klarić D, Klarić V and Kristić I: Cardiac
valves calcifications in dialysis patients. Acta Med Croatica.
65(Suppl 3): 11–13. 2011.(In Croatian).
|
|
27
|
Choi HS, Kim SH, Rhee Y, Cho MA, Lee EJ
and Lim SK: Serum parathyroid hormone is associated with carotid
intima-media thickness in postmenopausal women. Int J Clin Pract.
62:1352–1357. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Buizert PJ, van Schoor NM, Simsek S, Lips
P, Heijboer AC, den Heijer M, Deeg DJ and Eekhoff EM: PTH: A new
target in arteriosclerosis? J Clin Endocrinol Metab.
98:E1583–E1590. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Nuzzo V, Tauchmanovà L, Fonderico F,
Trotta R, Fittipaldi MR, Fontana D, Rossi R, Lombardi G, Trimarco B
and Lupoli G: Increased intima-media thickness of the carotid
artery wall, normal blood pressure profile and normal left
ventricular mass in subjects with primary hyperparathyroidism. Eur
J Endocrinol. 147:453–459. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Reis JP, von Mühlen D, Michos ED, Miller
ER III, Appel LJ, Araneta MR and Barrett-Connor E: Serum vitamin D,
parathyroid hormone levels, and carotid atherosclerosis.
Atherosclerosis. 207:585–590. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ix JH, Katz R, Kestenbaum B, Fried LF,
Kramer H, Stehman-Breen C and Shlipak MG: Association of mild to
moderate kidney dysfunction and coronary calcification. J Am Soc
Nephrol. 19:579–585. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Fox CS, Larson MG, Keyes MJ, Levy D,
Clouse ME, Culleton B and O'Donnell CJ: Kidney function is
inversely associated with coronary artery calcification in men and
women free of cardiovascular disease: The Framingham Heart Study.
Kidney Int. 66:2017–2021. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kramer H, Toto R, Peshock R, Cooper R and
Victor R: Association between chronic kidney disease and coronary
artery calcification: The Dallas Heart Study. J Am Soc Nephrol.
16:507–513. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
El Barzouhi A, Elias-Smale S, Dehghan A,
Vliegenthart-Proença R, Oudkerk M, Hofman A and Witteman JC: Renal
function is related to severity of coronary artery calcification in
elderly persons: The Rotterdam study. PLoS One. 6:e167382011.
View Article : Google Scholar : PubMed/NCBI
|