Introduction
Endothelial progenitor cells (EPCs) play an
important role in endogenous vascular reparation, and modulate the
clinical course of coronary artery disease (1). EPCs have been shown to mobilize from
the bone marrow into the circulation and home to sites of vascular
injury. They are then incorporated into foci of neovascularization,
thereby improving tissue recovery and blood flow in the setting of
tissue ischemia and endothelial damage (2,3).
Endothelial denudation and endovascular laceration due to rigid
stent struts and high-pressure balloon inflations initiate an
intensive local inflammatory response and disturb local vascular
function. Vascular injury may also produce abnormal neointimal
hyperplasia resulting in clinical or sub-clinical in-stent
restenosis as well as acute stent thrombosis, a potentially
catastrophic complication of coronary stenting. It has been
suggested that variations in EPCs in response to vascular injury
caused by stenting may affect short-term (acute stent thrombosis)
and long-term (restenosis) outcomes of percutaneous coronary
intervention (PCI) (4–7). EPC counts following coronary stenting
may potentially serve as a predictor for the risk stratification of
therapeutic coronary interventions.
EPCs can be identified by the expression of surface
markers, such as cluster of differentiation (CD)34 and kinase
domain receptor (KDR), the latter of which is the extracellular
domain of vascular endothelial growth factor receptor-2 (VEGFR-2).
CD133 is highly expressed on immature EPCs, but is lost when they
differentiate into mature endothelial cells (8). Immature EPCs can therefore be
distinguished by the expression of CD133.
Thomas et al (9) and Lee et al (10) have observed transient changes of
CD34+/KDR+ EPCs in patients 4–6 h post-PCI,
in non-diabetic and diabetic populations. Previous studies have
reported heterogeneous changes of EPC counts following PCI
procedures (11–13). However, these studies have not
addressed the pattern of recruitment or mobilization of mature and
immature EPCs following PCI. The sequential quantitation and
characterization of EPCs following coronary stenting may provide
new evidence to explain the endothelial recovery and the impact on
patient prognosis.
The present study aimed to measure the sequential
changes of mature and immature EPCs in the peripheral blood of
patients with exertional angina pectoris prior and subsequent to a
PCI procedure. Furthermore, the associations between the extent of
EPC motivation and a variety of clinical factors were studied,
particularly the association with the degree of endothelial injury
during PCI as represented by stent area plus inflating pressure. To
exclude confounding factors, such as the homing of EPCs secondary
to necrotic myocardium or the presence of other inflammatory
substances, strict inclusion criteria for the study population were
applied.
Materials and methods
Study population
Patients who underwent elective and successful PCI
treatment between October 2011 and September 2012 were screened for
the present study. The inclusion criteria were: i) Presence of
typical effort angina; ii) feasibility of complete
revascularization of clinically significant stenoses by PCI; and
iii) age ≤70 years. Exclusion criteria included: i) Age >70
years; ii) familial hyperlipidemia; iii) the presence of acute or
chronic inflammatory disease, ischemic cerebral and peripheral
arterial diseases, recent surgery or trauma; iv) acute coronary
syndrome (including unstable angina and acute myocardial
infarction); v) abnormal hepatic function at least 1 month prior to
PCI; vi) patients whose coronary angiography showed coronary artery
flow less than thrombolysis in myocardial infarction (TIMI) grade
3, dissection or thrombosis; vii) patients with PCI-associated
acute myocardial infarction, acute stent thrombosis, left
ventricular ejection fraction (LVEF) ≤50%; and viii) prior PCI or
coronary artery bypass graft surgery.
Patients who met the inclusion criteria and only
underwent angiography were enrolled as controls. Informed consent
was obtained from all patients. The study was approved by the
Committee for Human Research in Tianjin Chest Hospital (Heping,
China).
Percutaneous coronary angioplasty and
adjunctive drugs
According to the study protocol, all patients
without contraindications were pre-treated with 300 mg aspirin and
300 mg clopidogrel for the first day prior to PCI. Following PCI,
the anti-platelet regime was 300 mg aspirin daily for 1 month, then
100 mg daily indefinitely, and 75 mg clopidogrel daily for 12
months. Other medications such as β-blockers, statins and
angiotensin-converting enzyme inhibitors (ACEIs) were continued as
required. All patients received a standard dose of unfractionated
heparin (100 U/kg) prior to the angioplasty procedure.
Blood samples and cardiac progenitor
cell flow cytometry
Peripheral blood samples (2 ml) were collected
following diagnostic angiography (baseline level) and immediately
subsequent to the end of the PCI process (this was defined as the 1
h time-point, despite the actual time being <1 h from the first
balloon dilatation). Subsequently, blood samples were obtained for
time-points 3, 5, 7 and 24 h from the first balloon dilation. Blood
samples of angiography patients were collected pre-procedure and 7
and 24 h post-procedure in the control group. The blood samples for
stem cell assessment were stored at room temperature and analyzed
within 20 min. To 100 µl peripheral blood was added 10 µl
fluorescent anti-human CD34+ antibody (BD Biosciences,
San Jose, CA, USA), 10 µl anti-human KDR-PE (BD Biosciences), 5 µl
APC-conjugated anti-CD133 (Miltenyi Biotec GmbH, Bergisch Gladbach,
Germany) or fluorescent isotype-identical antibody controls. After
undiluted samples were stained with antibodies for 30 min in the
dark, erythrocytes were lysed using a lysing solution (BD
Biosciences), and samples were centrifuged at 200 × g for 10 min.
The mononuclear cell population, which includes EPCs, was isolated
from the whole blood forward and side scatter profile in a
FACSCalibur flow cytometer (BD Biosciences), then analyzed with Cell
Quest™ software (BD Biosciences). The method of EPC quantification
was consistent with published standard practices and
recommendations (14,15). Classic EPCs are described as
CD34+/KDR+, the mature EPC subpopulation was
considered as CD133−/CD34+/KDR+
and immature or naive EPCs as
CD133+/CD34+/KDR+. Immature
CD34+ and KDR+ cells were marked as
CD133+/CD34+ and
CD133+/KDR+. Counts of the different types of
EPC were reported as cells per 200,000 total events. The
measurements were performed by one operator who was blinded to the
status of the patients. To assess the reproducibility of the
results, circulating EPCs were measured twice in the first 5
consecutive patients from two blood samples drawn 1 day prior to
PCI.
The stent was assumed to be cylindrical following
its deployment from the stent-balloon. The surface area of the
stent (perimeter × length) in contact with the vascular endothelium
and the maximum stent inflation pressure were taken to be
representative of the severity of endothelial damage.
Quantitative parameters of coronary
angiography and angioplasty
Analysis of coronary angiograms was performed prior
to (baseline level) and subsequent to PCI by two independent
cardiologists from Tianjin Chest Hospital. Vessels with diameters
>2.25 mm were treated. Procedural success of the PCI was defined
as a decrease in diameter stenosis ≥50% and/or a residual narrowing
of <30% diameter stenosis.
Quantitative parameters for
endothelial injury
Mechanical trauma induced by high-pressure inflation
and rigid stent struts inevitably results in endothelial denudation
and endovascular laceration. In the present study, the stent
surface area was used to quantify the amount of endothelium damaged
by the stenting procedure. The stent-inflation pressure was also
used to estimate the extent of the endothelial trauma caused by the
PCI procedure. In order to evaluate the vascular damage during PCI,
the product of the stent surface area and the stent-inflation
pressure was determined and regarded as a global injury integral.
The present study focused predominantly on the correlation between
the extent of endothelial injury and the alterations of
CD34+/KDR+ and
CD133−/CD34+/KDR+ EPCs measured at
baseline and 24 h post-PCI.
Statistical analysis
Data are presented as mean ± standard deviation for
continuous variables or frequency percentages for categorical
variables. Kolmogorov-Smirnov testing was applied to assess
normality of distribution for continuous variables. Student's
paired t-tests were performed to compare the serial changes in cell
counts with baseline or the lowest value following a percutaneous
transluminal coronary angioplasty procedure. P<0.05 was
considered to indicate a statistically significant difference. The
correlations of changed magnitude of EPCs and trauma parameters
(stent surface area/global injury integral) were explored by
partial correlation. Analyses and error bars were performed with
the SPSS statistical software package (version 18.0; SPSS Inc.,
Chicago, IL, USA).
Results
Patient characteristics and progenitor
count
The 66 patients fulfilling the inclusion/exclusion
criteria were enrolled in the PCI group and samples were taken from
them at 6 time-points. Another 17 patients who only underwent
angiography were distributed into a control group with samples
taken at 3 time-points: Baseline, and 7 and 24 h post-angiography.
A total of 61 patients (92.4%) had a single vessel treated and 5
patients (7.6%) had 2 vessels treated with a mean stent surface
area of 335.59±234.99 mm2 per patient. Clinical
characteristics of the two groups are shown in Table I. There was no significant difference
between the two groups with the exception of diabetic incidence,
angiographic characteristics and family history of coronary heart
disease.
 | Table I.Comparison of clinical
characteristics between the two groups. |
Table I.
Comparison of clinical
characteristics between the two groups.
| Clinical
parameter | PCI group,
n=66 | Control group,
n=17 | P-value |
|---|
| Basic clinical
characteristics |
|
|
|
| Age,
years | 59.54±9.06 | 57.32±6.30 | NS |
| Male
(%) | 49 (74.2) | 11 (68.7) | NS |
| BMI,
kg/m2 | 24.6±3.4 | 23.9±2.8 | NS |
|
Hypertension (%) | 35 (53) | 7 (43.8) | NS |
| ACEI or
ARB treatment (%) | 29 (43.9) | 7 (43.8) | NS |
|
Diabetes (%) | 24 (36.4) | 2 (11.8) | <0.05 |
| Current
smoker (%) | 20 (30.3) | 4 (23.5) | NS |
| Family
history of coronary disease (%) | 5 (31.3) | 2 (5.9) | <0.05 |
|
Single-vessel disease (%) | 36 (54.5) | 5 (31.2) | <0.05 |
|
Two-vessel disease (%) | 16 (24.2) | 2 (12.5) | <0.05 |
|
Three-vessel disease (%) | 14 (18.75) | 1 (6.25) | <0.05 |
| Statin
therapy prior to PCI (%) | 66 (100) | 17 (100) | NS |
| Laboratory
characteristics |
|
|
|
| Plasma
low density cholesterol, mmol/l | 2.54±0.81 | 2.21±0.32 | NS |
| Hs-CRP,
mg/l | 1.55±2.83 | 0.62±0.78 | NS |
| White
cell count (x109/l) | 6.63±1.35 | 6.39±1.23 | NS |
|
Lymphocyte count
(x109/l) | 1.62±0.44 | 1.64±0.31 | NS |
|
Monocyte count
(x109/l) | 0.50±0.4 | 0.51±0.32 | – |
| Maximum
value of CKMB pre-PCI, U/l | 22 | 19 | – |
| Minimum
value of CKMB post-PCI or CAG, U/l | 19 | 20 | – |
| Maximum
value of troponin I pre-PCI, ng/ml |
0.9 |
0.81 | – |
| Minimum
value of troponin I post-PCI or CAG, ng/ml |
0.9 |
0.21 | – |
| Procedural
details |
|
|
|
|
Drug-eluting stent (%) | 66 (100) | – |
|
| Stent
surface per subject, 2πR × length, mm2 | 335.59±234.99 | – |
|
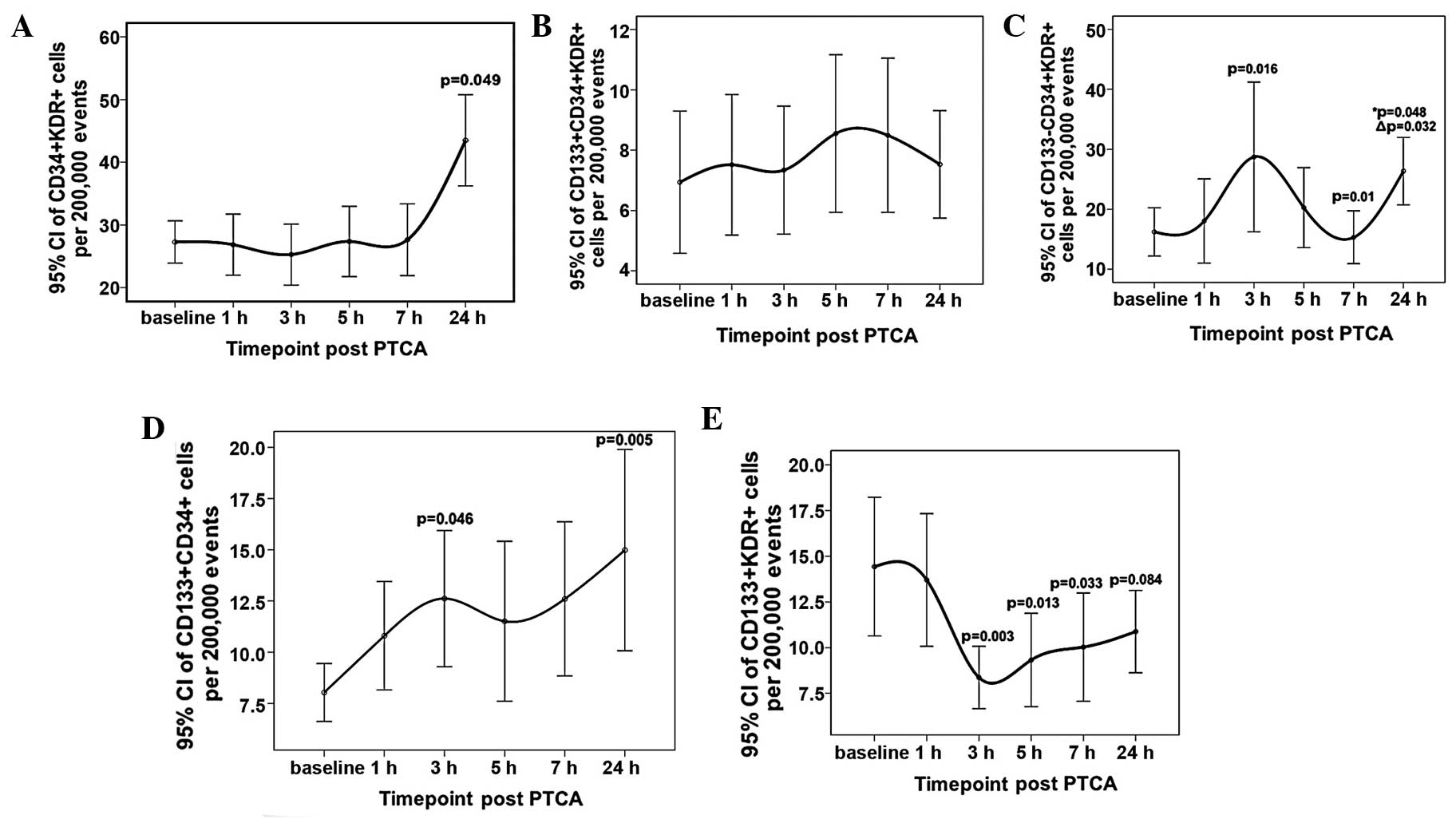
EPC counts are presented as mean ± standard
deviation of cells per 200,000 events and the trends post-PCI are
shown in error bar charts (Fig. 1).
No significant elevation in the count of
CD34+/KDR+ EPCs was found in the control
group compared with the PCI group at baseline, but increased
numbers of CD133+/CD34+/KDR+ and
CD133+/CD34+ cells, which were immature
subpopulations of CD34+/KDR+ or immature
CD34+cells, respectively, were observed. A stable
CD34+/KDR+ count was shown within 7 h
following the PCI procedure, and a mild and delayed upregulation
was shown at 24 h. The levels of the immature
CD133+/CD34+/KDR+ cell
subpopulation were relatively stable during the procedure.
Undulating changes were seen in the
CD133−/CD34+/KDR+ subpopulation
level at the 3, 7 and 24 h time-points (P=0.016, P=0.01 and
P=0.032, respectively) and no tendency to return to the baseline
level was shown at 24 h post PCI (P=0.048). Small but significant
increases were shown in CD133+/CD34+ cell
counts at 3 and 24 h (P=0.046 and P=0.005, respectively). The
CD133+/KDR+ subpopulation showed a moderate
reduction in count at 3 h after the procedure, remained reduced
until 7 h post PCI (P=0.003, P=0.013 and P=0.033, at 3, 5 and 7 h
respectively), and then marginally increased at 24 h, when the
statistical significance of the difference relative to the baseline
count was lost (P=0.084; Table
II).
| Table II.Counts of endothelial progenitor
cells and subpopulations in the PCI and control group per 200,000
events. |
Table II.
Counts of endothelial progenitor
cells and subpopulations in the PCI and control group per 200,000
events.
| Time-points |
CD34+/KDR+ |
CD133−/CD34+/KDR+ |
CD133+/CD34+/KDR+ |
KDR+/CD133+ |
CD34+/CD133+ |
|---|
| PCI group
(n=66) |
|
|
|
|
|
|
Baseline count | 27.28±13.61 | 16.23±16.31 |
6.94±9.51d | 14.43±15.32 |
8.03±5.71d |
| 1
h post-PCI | 26.84±19.52 | 18.05±28.12 | 7.52±9.33 | 13.70±14.53 | 10.80±10.61 |
| 3
h post-PCI | 25.28±19.68 |
28.72±50.39b | 7.34±8.56 |
8.37±6.88a |
12.62±13.41a |
| 5
h post-PCI | 27.37±22.57 | 20.28±26.95 | 8.55±10.55 |
9.32±10.31a | 11.51±15.76 |
| 7
h post-PCI | 27.65±23.13 |
15.32±17.73b | 8.49±10.32 |
10.03±11.96a | 12.60±15.21 |
| 24 h
post-PCI |
43.50±29.59a |
26.38±22.93a,c | 7.53±7.25 | 10.88±9.13 |
14.98±20.00b |
| Control group
(n=17) |
|
|
|
|
|
|
Baseline count | 28.53±9.22 | 14.00±4.76 | 13.06±7.44 | 12.41±7.30 | 17.94±8.59 |
| 7
h post-CAG | 26.53±15.05 | 13.35±6.84 | 11.53±9.75 | 11.71±10.23 | 16.82±14.11 |
| 24 h
post-CAG | 28.94±14.49 | 13.82±4.75 | 14.53±10.45 | 14.65±10.43 | 20.06±13.86 |
Association between EPC phenotype and
clinical factors
Partial correlation analysis was performed to
investigate the association between the maximum change magnitudes
of CD34+/KDR+ EPCs and clinical factors
including age, gender, stent surface area and maximum stent
inflation pressure. The results revealed that the maximum change
magnitude of EPCs CD34+/KDR+ correlated
negatively with basal C-reactive protein (CRP; P=0.034) and
positively with body mass index (BMI), smoking and ACEI or
angiotensin II receptor blocker (ARB) drug treatment (P=0.021,
P=0.02 and P=0.026, respectively). There was also a positive
correlation with the global injury integral (the product of the
stent surface area and the maximum stent inflation pressure;
P<0.001; Table III).
| Table III.Partial correlation analysis between
the maximum change magnitudes of CD34+/KDR+
cells post-angioplasty and relative factors. |
Table III.
Partial correlation analysis between
the maximum change magnitudes of CD34+/KDR+
cells post-angioplasty and relative factors.
| Relative
factors | Partial correlation
coefficient | P-value |
|---|
| Age | −0.2487 |
0.057 |
| BMI | 0.3007 |
0.021 |
| WBC | −0.1859 |
0.159 |
| Neutrophil
ratio | 0.015 | 0.91 |
| Hs-CRP | −0.2759 |
0.034 |
| Surface of stent
area | 0.2168 |
0.099 |
| Maximum dilation
pressure of stent | −0.1541 | 0.24 |
| Stent surface area
× maximum inflation pressure | 0.4467 | <0.001 |
| Gender | −0.2039 |
0.115 |
| Current
smoking | 0.2969 | 0.02 |
| Current
drinking | −0.1563 |
0.229 |
| Essential
hypertension | −0.2208 |
0.087 |
| Diabetes | 0.1378 |
0.289 |
| ACEI or ARB
treatment | 0.2845 |
0.026 |
Discussion
In the present study, the circulating CD133-, CD34-
and KDR-marked progenitor cells were quantified and any changes in
patients with exertional angina were examined at different
time-points within 24 h pre- and post-angioplasty. On the basis of
a previous study (1), the data of
the present study demonstrated that mature EPCs (identified by
CD133−/CD34+/KDR+ status) were
more actively motivated to enter the peripheral blood or home to
the local coronary endothelium when induced by PCI, as indicated by
the earlier and more intensive up- and downregulation of the EPC
count (2). The specific association
between the motivation of CD34+/KDR+ EPCs and
a number of clinical factors was probed during the early stages
following PCI. Finally, the maximum changes of
CD34+/KDR+ EPCs were identified to correlate
with BMI, CRP, current smoking habits and ACEI or ARB treatment
(0.01<P<0.05), and particularly with the global injury
integral from the PCI procedure (P<0.001). Allowing for possible
sampling errors, it is ensured that global injury integral is the
crucial contributor to CD34+/KDR+ EPC
motivation.
A delayed increase of
CD34+/KDR+ levels was observed 24 h post-PCI
on the basis of the prior increase in
CD133−/CD34+/KDR+ EPCs and the
relatively constant level of
CD133+/CD34+/KDR+ EPCs. Since
CD133 is highly expressed in immature stem cells and lost during
the differentiation to mature endothelial cells (16,17), the
CD133+/CD34+/KDR+ subpopulation is
a precursor of CD133−/CD34+/KDR+
cells. The undulating change of
CD133−/CD34+/KDR+ cell counts
suggests that EPCs, particularly mature circulating EPCs, are
preferentially recruited by homing signals such as stromal
cell-derived factor-1 (SDF-1) (18),
which is released from denudated endothelium. It is assumed that
EPC subgroups with prior and robust mobilization may play a more
important role in endothelial reparation.
Intracoronary stents are a potential vehicle for the
delivery of novel therapies directly to the site of vascular
injury. Gene-eluting stents that directly deliver naked plasmid DNA
encoding for VEGF-2 may accelerate re-endothelialization and reduce
lumen loss in animal models (19).
If mature circulating EPCs (particularly
CD133−/CD34+/KDR+ subpopulations)
are preferentially recruited and home to sites of injury where
balloons inflate or stents are deployed, we recommend promoting the
‘capture’ of CD133+/CD34+ and
CD133+/KDR+ cells, or even the mature
CD133−/KDR+/CD34+ subpopulation of
EPCs, by gene-eluting stent implantation to facilitate
re-endothelialization. Secondly, it is suggested that a large-scale
mobilization of EPCs from bone marrow may occur no later than 24 h
after PCI, providing a valuable time-window for the application of
measures to advance or intensify this process.
In the present study, an evaluation was carried out
of whether any associations exist between the degree of damage and
changes in EPCs induced by the combined effect of recruitment and
homing. Damage to the endothelium originating from mechanical
inflation was categorized into injury area and degree, which were
mirrored by stent surface area and the maximum stent inflated
pressure.
In the present study, various possible clinical
factors were listed and individual correlations with the changes in
CD34+/KDR+ EPCs were analyzed. It was
confirmed that a positive correlation existed for
CD34+/KDR+ EPC motivation with current
smoking or ACEI or ARB administration, and a negative correlation
with hs-CRP. This partially conforms with the results of certain
published reports (20,21). It is, therefore, reasonable to accept
that, according to the present results, the mobilization of EPCs
correlated negatively with hs-CRP and correlated positively with
ACEI or ARB drug treatment. The present study found that positive
correlations existed between the mobilization degree of EPCs and
smoking or BMI. This shows that to a certain extent a more robust
motivation can be stimulated post-PCI among respective populations.
By contrast, cigarette smoking may stimulate the release of EPCs
from bone marrow to repair the damaged endothelium and it may be an
eligible reason underlying the mechanism of this positive
connection.
The significant positive correlation between the
global injury integral and EPC mobilization amplitude in the
present study revealed that the degree of endothelial damage in the
PCI procedure depends on both the contact area of the stent strut
with the coronary endothelium and stent inflation pressure. A
higher global injury integral usually represents a larger stent
diameter, in particular with a higher inflation pressure. This may
support complete lesion cover and good positioning during PCI in
order to accelerate the endothelialization process. This also
offers a new theoretical foundation for the post-inflation
advocated by the angiography versus intravascular
ultrasound-directed bare-metal coronary stent placement (AVID)
trial (22). This suggests that more
intensive and effective motivation of EPCs initiated post-dilation
may contribute to the reparation of the damage to the endothelium
caused by PCI, and then to a certain extent decrease the incidence
of in-stent thrombosis or restenosis (23).
In the present study, blood samples were not
collected at specified time-points, so no circadian rhythm was
detected in the control group whereas a diurnal reduction of
circulating EPCs has been recorded between 08.00 and 15.00 of
11–18% in healthy volunteers (24).
The present outcome does not completely agree with
previous studies reported by Thomas et al (9) and Lee et al (10), in which a moderate but marked
reduction of the CD34+/KDR+ EPC phenotype was
detected at 4 and 6 h post-PCI time-points compared with the
baseline level. This difference is ascribed to respective enrolment
criteria or pharmacological therapy; for example, diabetic patients
were excluded by Thomas et al (9), yet Lee et al (10) targeted the dynamic mobilization of
EPC in diabetics. In the present study some diabetic cases comorbid
with hyperlipidemia or hypertension were enrolled. Furthermore, all
patients were treated with statins. Diabetics of types I and II
have been shown to have lower baseline EPC levels and dysfunctional
progenitor cells in terms of proliferation, adhesion and angiogenic
properties, resulting in delayed re-endothelization (25,26).
Statins can facilitate the mobilization of CD34+ and
KDR+ cells into the peripheral circulation (27) in a dose-dependent manner (28). Differences in the study population
and interventional measures may confound the successive changes of
circulating EPCs following PCI.
The present study had various limitations, including
that the fact that the results indicated that single diagnostic
angiography did not induce changes in the levels of EPCs (29). It may be inferred that the act of
injecting contrast agent into the coronary artery is not a
causative factor, although the possibility that the insertion of a
sheath into the femoral artery causes arterial endothelial damage
cannot be excluded and may possibly be a causative factor. Another
limitation of this study is the fact that the number of patients
was relatively small, which helps in understanding why no
significant difference in EPC counts was found at baseline between
the two groups. Furthermore, only the relative changes of EPC
counts in peripheral blood were studied and no functional studies
of the EPCs were conducted. All treated coronary arteries had TIMI
grade 3 blood flow prior to the first balloon dilation and no
iatrogenic myocardial infarction from PCI; hence, a disturbance due
to inflammatory factors from necrotic myocardium can be excluded.
Finally as there was no long-term follow up of these patients, a
delayed and more significant mobilization of EPCs at >24 h
post-PCI cannot be excluded.
In conclusion, endothelial injury from angioplasty
can lead to time-dependent mobilization or homing of EPCs; mature
EPC subpopulations are actively mobilized, and may contribute more
to endothelial reparation; and the mobilization amplitude of the
main EPC subpopulations is significantly influenced by the degree
of endothelial injury and certain clinical factors.
References
|
1
|
Bakogiannis C, Tousoulis D, Androulakis E,
et al: Circulating endothelial progenitor cells as biomarkers for
prediction of cardiovascular outcomes. Curr Med Chem. 19:2597–2604.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kwon O, Miller S, Li N, et al: Bone
marrow-derived endothelial progenitor cells and endothelial cells
may contribute to endothelial repair in the kidney immediately
after ischemia-reperfusion. J Histochem Cytochem. 58:687–694. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sen S, McDonald SP, Coates PT, et al:
Endothelial progenitor cells: Novel biomarker and promising cell
therapy for cardiovascular disease. Clin Sci (Lond). 120:263–283.
2011.PubMed/NCBI
|
|
4
|
Wojakowski W, Pyrlik A, Król M, et al:
Circulating endothelial progenitor cells are inversely correlated
with in-stent restenosis in patients with non-ST-segment elevation
acute coronary syndromes treated with EPC-capture stents (JACK-EPC
trial). Minerva Cardioangiol. 61:301–311. 2013.PubMed/NCBI
|
|
5
|
Damman P, Klomp M, Beijk MA, et al:
e-Healing Investigators: Twelve-month outcomes after coronary
stenting with the Genous™ bio-engineered R Stent™ in diabetic
patients from the e-HEALING registry. J Interv Cardiol. 24:285–294.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Pelliccia F, Pasceri V, Rosano G, et al:
Endothelial progenitor cells predict long-term prognosis in
patients with stable angina treated with percutaneous coronary
intervention: Five-year follow-up of the PROCREATION study. Circ J.
77:1728–1735. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bonello L, Harhouri K, Baumstarck K, et
al: Mobilization of CD34+ KDR+ endothelial
progenitor cells predicts target lesion revascularization. J Thromb
Haemost. 10:1906–1913. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shmelkov SV, St Clair R, Lyden D and Rafii
S: AC133/CD133/Prominin-1. Int J Biochem Cell Biol. 37:715–719.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Thomas HE, Avery PJ, Ahmed JM, et al:
Local vessel injury following percutaneous coronary intervention
does not promote early mobilisation of endothelial progenitor cells
in the absence of myocardial necrosis. Heart. 95:555–558. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lee LC, Chen CS, Choong PF, et al:
Time-dependent dynamic mobilization of circulating progenitor cells
during percutaneous coronary intervention in diabetics. Int J
Cardiol. 142:199–201. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Egan CG, Caporali F, Huqi AF, et al:
Reduced levels of putative endothelial progenitor and
CXCR4+ cells in coronary artery disease: Kinetics
following percutaneous coronary intervention and association with
clinical characteristics. Thromb Haemost. 101:1138–1146.
2009.PubMed/NCBI
|
|
12
|
Garg R, Tellez A, Alviar C, et al: The
effect of percutaneous coronary intervention on inflammatory
response and endothelial progenitor cell recruitment. Catheter
Cardiovasc Interv. 72:205–209. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Banerjee S, Brilakis E, Zhang S, et al:
Endothelial progenitor cell mobilization after percutaneous
coronary intervention. Atherosclerosis. 189:70–75. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Vasa M, Fichtlscherer S, Aicher A, et al:
Number and migratory activity of circulating endothelial progenitor
cells inversely correlated with risk factors for coronary artery
disease. Circ Res. 89:E1–E7. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Steiner S, Niessner A, Ziegler S, et al:
Endurance training increases the number of endothelial progenitor
cells in patients with cardiovascular risk and coronary artery
disease. Atherosclerosis. 181:305–310. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Handgretinger R, Gordon PR, Leimig T, et
al: Biology and plasticity of CD133+ hematopoietic stem
cells. Ann NY Acad Sci. 996:141–151. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Foteinos G, Hu Y, Xiao Q, et al: Rapid
endothelial turnover in atherosclerosis-prone areas coincides with
stem cell repair in apolipoprotein E-deficient mice. Circulation.
117:1856–1863. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yin Y, Zhao X, Fang Y, et al: SDF-1 alpha
involved in mobilization and recruitment of endothelial progenitor
cells after arterial injury in mice. Cardiovasc Pathol. 19:218–227.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Walter DH, Cejna M, Diaz-Sandoval L, et
al: Local gene transfer of phVEGF-2 plasmid by gene-eluting stents:
An alternative strategy for inhibition of restenosis. Circulation.
110:36–45. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Umemura T, Soga J, Hidaka T, et al: Aging
and hypertension are independent risk factors for reduced number of
circulating endothelial progenitor cells. Am J Hypertens.
21:1203–1209. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kränkel N, Lüscher TF and Landmesser U:
‘Endothelial progenitor cells’ as a therapeutic strategy in
cardiovascular disease. Curr Vasc Pharmacol. 10:107–124. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Russo RJ, Silva PD, Teirstein PS, et al:
AVID Investigators: A randomized controlled trial of angiography
versus intravascular ultrasound-directed bare-metal coronary stent
placement (the AVID Trial). Circ Cardiovasc Interv. 2:113–123.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Fröbert O, Sarno G, James SK, et al:
Effect of stent inflation pressure and post-dilatation on the
outcome of coronary artery intervention. A report of more than
90,000 stent implantations. PLoS One. 8:e563482013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Thomas HE, Redgrave R, Cunnington MS, et
al: Circulating endothelial progenitor cells exhibit diurnal
variation. Arterioscler Thromb Vasc Biol. 28:E21–E22. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Tepper OM, Galiano RD, Capla JM, et al:
Human endothelial progenitor cells from type II diabetics exhibit
impaired proliferation, adhesion and incorporation into vascular
structures. Circulation. 106:2781–2786. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ii M, Takenaka H, Asai J, et al:
Endothelial progenitor thrombospondin-1 mediates diabetes-induced
delay in reendothelialization following arterial injury. Circ Res.
98:697–704. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Vasa M, Fichtlscherer S, Adler K, et al:
Increase in circulating endothelial progenitor cells by statin
therapy in patients with stable coronary artery disease.
Circulation. 103:2885–2890. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Leone AM, Rutella S, Giannico MB, et al:
Effect of intensive vs standard statin therapy on endothelial
progenitor cells and left ventricular function in patients with
acute myocardial infarction: Statins for regeneration after acute
myocardial infarction and PCI (STRAP) trial. Int J Cardiol.
130:457–462. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Mills NL, Tura O, Padfield GJ, et al:
Dissociation of phenotypic and functional endothelial progenitor
cells in patients undergoing percutaneous coronary intervention.
Heart. 95:2003–2008. 2009. View Article : Google Scholar : PubMed/NCBI
|