Introduction
Diabetic nephropathy (DN) is a progressive disease
with an increasing prevalence in developed and developing
countries, and has a significant impact on morbidity and mortality
from chronic kidney disease (CKD), end-stage renal disease (ESRD)
and cardiovascular disease (1–3).
Although significant progress has been made in understanding the
pathogenesis of DN, the current treatments for diabetic kidney
disease only provide partial therapeutic effects; more effective
therapies for DN are required (4).
Erigeron breviscapus (Vant.) Hand.-Mazz. is a
native plant species of Yunnan, China. Breviscapine, as a purified
flavonoid extract from this species, was first isolated by Zhang
et al (5). Breviscapine
primarily contains two flavonoids, namely scutellarin and
apigenin-7-O-β-glucoside. Scutellarin accounts for ~90% of the
extract; apigenin-7-O-β-glucoside accounts for ~4% (6).
Breviscapine has a broad range of pharmacological
effects, including dilation of micro-blood vessels, reduction of
blood viscosity and improvement of the microcirculation; it also
has an anti-platelet, anti-thrombotic action and can decrease
plasma fibrin content and promote fibrinolytic activity (7,8). Since
the 1970s, breviscapine injections have been extensively used in
China for the treatment of ischemic cardiovascular and
cerebrovascular diseases, such as angina pectoris, myocardial
infarction and focal cerebral infarction (9,10).
Breviscapine has been demonstrated to possess a
number of pharmacological functions in addition to its hemodynamic
effects; it has been reported to serve as an anti-oxidative stress
agent and a protein kinase C (PKC) inhibitor, and can improve renal
function and reduce urinary micro-albuminuria, suggesting that this
drug has great therapeutic potential for the treatment of DN
(11,12). Although a number of clinical trials
have investigated the renal protection provided by breviscapine in
DN, uncertainties remain regarding the efficacy of breviscapine.
This is primarily a result of the lack of high-quality,
large-sample randomized clinical trials. The purpose of the present
study was to systematically review randomized control trials (RCTs)
and explore the effect of breviscapine in DN.
Materials and methods
Study design
All the RCTs that were identified to investigate the
effect of breviscapine on DN were included. There was no
restriction on the language or year of publication.
Subject criteria
Each patient included in the analysis fulfilled the
definition of diabetic mellitus (13,14).
Patients with DN in stages III–IV according to the DN diagnostic
criteria of Mogensen et al (15) were included in the study. Patients
with chronic diseases [chronic liver disease, chronic respiratory
disease, heart failure, cerebrovascular disease, malignant tumors,
serious hypertension, autoimmune disease, acute diabetic
complications (for example, diabetic ketoacidosis), hyperglycemic
hyperosmolar status], infectious diseases, organ transplants or a
recent history of the application of nephrotoxic drugs, were
excluded from the study.
Data extraction and appraisal of
methodological quality
A standard data extraction method was performed
independently by two authors, and the following information from
each eligible study was recorded: Study design, participant
characteristics [age, gender, history of diabetes mellitus (DM),
number of patients in the breviscapine group and the control
group], therapeutic intervention [basic treatment including diet
control, the control of blood glucose, antihyperlipidemics,
antihypertensives, angiotensin-converting enzyme inhibitor (ACEI)
and angiotensin receptor blocker (ARB), and treatment duration].
Whether these parameters were comparable between the breviscapine
treatment group and the control group was assessed.
An intravenous drip of breviscapine was administered
to the patients in the treatment group. The commercial injection
fluid (sourced from numerous companies across these studies) was
produced from extracted flavonoids of Erigeron breviscapus
(Vant) Hand.-Mazz., and was manufactured in accordance with the
quality standards of the Chinese State Drug Administration. Each
patient in the treatment groups received the same type of injection
using the same standards; the dosage ranged from 20 to 100 mg/day,
and the studies had a treatment duration of between 2 weeks and 1
month.
Therapeutic effect criteria included 24-h urine
protein levels, urinary albumin excretion rate, renal function
[serum creatinine (SCr) and blood urea nitrogen (BUN) levels], and
levels of cholesterol, triglycerides, high density lipoproteins
(HDL) and fibrinogen.
Search strategy
A systematic literature search was performed to
identify studies concerning the treatment of patients with DN using
breviscapine. MEDLINE/PubMed, Embase, the China National Knowledge
Infrastructure (CNKI) Database, Chinese Evidence-Based Medicine
Database (CEBM), Wanfang Digital Periodicals Database (WFDP),
Chinese Journal Full-text Database (CJFD), Chinese Biological and
Medical Database (CBM), China Doctoral and Masters Dissertations
Full-text Database and the Chinese Proceedings of Conference
Full-text Database were searched. Reference lists from the relevant
studies were examined to identify further studies and previous
reviews of the field. Articles citing the aforementioned studies
were examined to identify additional relevant studies.
Assessment methodology
All articles that were identified in the database
search were screened by two authors independently, and
disagreements were resolved by consensus. Missing data from trials
were obtained from the principal investigators of the relevant
studies, if possible. The studies were graded for methodological
quality according to the Jadad scale (16). A study was considered high quality if
graded with ≥3 scores on the Jadad scale.
Statistical analysis
A meta-analysis was conducted using Stata version
11.0 for Windows (StataCorp LP, College Station, TX, USA). The
principal measure of effect was the weighted mean difference (WMD)
between the breviscapine and control groups, and the standardized
mean difference (SMD) was used when analyzing 24-h urine protein as
this is a continuous variable with large differences in mean. The
confidence interval (CI) was 95%, as the outcome measurements were
the same for each analysis. Heterogeneity was assessed using a
χ2 test (P<0.1 was considered to indicate a
statistically significant difference) and an I2 test
(I2>50%, significant heterogeneity;
I2<25%, insignificant heterogeneity). Begg's test was
used to assess publication bias.
Results
Study characteristics
A total of 126 publications were initially
identified; 64 were excluded as they were not relevant to the study
question. A total of 62 clinical trials were retrieved for detailed
evaluation. Of these, 28 were excluded for the following reasons:
No measurement data (n=5), absence of a control group for
comparison with the breviscapine group (n=1), patients were at
clinical stage V of DN (n=2), supplementing the breviscapine
treatment with other, similar drugs (n=11), breviscapine was
administered as a control drug (n=5), oral administration (n=1) and
duplicate publication (n=2). Thus, 34 studies comprising 34 RCTs
were eligible for inclusion in the present analysis (11,17–50)
These 34 RCTs are summarized in Tables
I–III. A total of 2,260
patients were included (1,158 patients in treatment group and 1,102
patients in the control group). Each study was performed in China
and all of the patients involved were Chinese.
 | Table I.Study characteristics: Effect of
breviscapine on renal function in patients with DN. |
Table I.
Study characteristics: Effect of
breviscapine on renal function in patients with DN.
|
| Blood urea nitrogen
(mmol/l) | Serum creatinine
(µmol/l) |
|
|---|
|
|
|
|
|
|---|
| First author,
year | Stage of DN | n | Age (years) | History of DM | Intervention
(breviscapine) | Treatment
duration | Baseline | After
intervention | Baseline | After
intervention | Refs. |
|---|
| Chen, 2007 |
|
| 56.4 | 12 (y) |
|
|
|
|
|
| (17) |
|
| III | T: 12 |
|
| T: 100 mg i.v.
drip. Qd-b | 2 weeks | N | 4.4±1.4 | N | 78±14 |
|
|
|
| C: 12 |
|
| C: -b |
|
| 4.8±1.5 |
| 79±17 |
|
|
| IV | T: 13 |
|
| T: 100 mg i.v.
drip. Qd-b | 2 weeks | N | 7.8±2.6 | N | 120±36 |
|
|
|
| C: 13 |
|
| C: -b |
|
| 12.3±3.8 |
| 149±25 |
| Yu, 2010 | III | T: 34 | 63.5±4.5 | 10.0±6.5 (y) | T: 50 mg i.v. drip.
Qd-a | 4 weeks | N | N | 85±18 | 78±12 | (18) |
|
|
| C: 34 | 64.0±3.5 | 10.6±3.5 (y) | C: -a |
|
|
| 91±15 | 85±16 |
|
| Wang, 2009 | III | T: 20 | 68 (mean) | 8 (y) (mean) | T: 50 mg i.v. drip.
Qd-a | 2 weeks | N | N | 85±18 | 78±12 | (19) |
|
|
| C: 20 | 70 (mean) | 10 (y) (mean) | C: -a |
|
|
| 92±14 | 86±15 |
|
| Huang, 2011 | III | T: 18 | 64 (mean) | 8 (y) (mean) | T: 50 mg i.v. drip.
Qd-a | 4 weeks | N | N | 85.0±18.0 | 78.0±12.0 | (20) |
|
|
| C: 18 | 66 (mean) | 10 (y) (mean) | C: -a |
|
|
| 92.1±13.9 | 86.0±15.0 |
|
| Shen, 2011 | IV | T: 36 | 52.3±5.7 | N | T: 50 mg i.v. drip.
Qd-a | 3 weeks | 10.12±2.02 | 6.09±2.52 | 153.7±35.3 | 106.9±27.1 | (21) |
|
|
| C: 39 | 51.9±6.8 | N | C: -a |
|
9.35±1.87 | 6.93±2.65 | 150.1±39.5 | 125.2±30.5 |
|
| Wu, 2009 | IV | T: 36 | 62±2 | 5.01±1.85 (y) | T: 50 mg i.v. drip.
Qd-a | 1 month | 11.15±1.32 | 6.02±1.36 | 155.32±12.26 | 70.58±25.25 | (22) |
|
|
| C: 34 | 61±3 | 5.32±2.45 (y) | C: -a |
| 12.31±2.54 | 9.86±1.55 | 153.25±15.74 | 132.36±23.21 |
|
| Huang, 2004 | III | T: 34 | 66.5±8.4 | 4.8±2.5 (y) | T: 60 mg i.v. drip.
Qd-u | 3 weeks |
5.48±1.26 | 5.46±1.35 | 85.59±20.12 | 84.34±19.89 | (23) |
|
|
| C: 28 | 65.3±6.5 | 4.58±2.10 (y) | C: -u |
|
5.32±1.34 | 5.45±1.43 | 79.38±19.78 | 81.45±21.45 |
|
| Li, 2006 | III–IV | T: 40 | 48–77 (mean
54.5) | 4–18 (m) | T: 50 mg i.v. drip.
Qd-a | 4 weeks | 12.06±1.84 | 5.28±1.57 | 218.63±18.84 | 132.53±17.32 | (24) |
|
|
| C: 36 | 50–75 (mean
53.5) | 5–17 (m) | C: -a |
| 11.63±2.25 | 9.04±1.35 | 218.54±19.20 | 180.60±20.1 |
|
| Fang, 2011 | III | T: 58 |
43.76±11.92 | 2.36±0.97 (y) | T: 30 mg i.v. drip.
Qd-a | 3 weeks | 13.45±3.02 | 7.76±1.69 | 139.41±10.13 | 117.05±6.94 | (25) |
|
|
| C: 58 |
42.67±10.42 | 2.69±1.05 (y) | C: -a |
| 13.34±2.98 | 9.27±2.16 | 137.35±9.79 | 126.72±8.35 |
|
| Qiao, 2009 |
| | 62.25±8.90 | N |
|
|
|
|
|
| (26) |
|
| IV | T: 52 |
|
| T: 40 mg i.v. drip.
Qd-a | 4 weeks |
16.1±10.1 | 10.2±9.0 | 310.9±156.4 | 220.1±66.4 |
|
|
|
| C: 40 |
|
| C: -a |
| 14.7±9.2 | 11.5±9.3 | 289.1±123.1 | 210.2±49.8 |
|
| Zhong, 2011 |
|
| 41–65 (mean
54) | 3–8 (y) |
|
|
|
|
|
| (27) |
|
| III | T: 30 |
|
| T: 30 mg i.v. drip.
Qd-a | 3 weeks |
7.31±1.58 | 5.48±0.87 | 94.52±10.31 | 92.45±9.86 |
|
|
|
| C: 29 |
|
| C: -a |
|
7.01±1.32 | 6.89±1.19 | 96.22±11.08 | 96.79±9.83 |
|
| Liu, 2011 | III | T: 34 | 58.7±9.1 | 8.6±5.7 (y) | T: 50 mg i.v. drip.
Qd-u | 15 days |
8.48±1.32 | 8.43±1.28 | 91.63±15.82 | 88.47±16.21 | (28) |
|
|
| C: 34 | 59.3±8.3 | 8.4±6.1 (y) | C: -u |
|
8.39±1.29 | 8.41±1.33 | 89.85±14.78 | 90.45±15.58 |
|
| Xu, 2008 | III–IV | T: 36 | 42–79 | N | T: 100 mg i.v.
drip. Qd-b | 4 weeks | 12.36±2.84 | 6.09±2.50 | 253.25±87.20 | 102.53±77.19 | (29) |
|
|
| C: 40 | 41–76 | N | C: -b |
| 11.04±1.62 | 9.96±1.55 | 239.40±101.17 | 196.68±88.24 |
|
| Wu, 2011 | III | T: 30 | 58.3±7.4 | 7.1±4.5 (y) | T: 40 mg i.v. drip.
Qd-a | 2 weeks |
4.98±1.76 | 5.01±1.64 | 75.64±15.23 | 73.68±12.45 | (30) |
|
|
| C: 30 | 55.9±8.1 | 6.8±5.1 (y) | C: -a |
|
5.11±0.98 | 5.07±0.86 | 74.47±14.86 | 73.48±13.12 |
|
| Liu, 2007 | III | T: 23 | 66±5 | 10±5 (y) | T: 50 mg i.v. drip.
Qd-a | 4 weeks | N | N |
101.00±25.10 |
94.73±19.78 | (31) |
|
|
| C: 22 | 66±6 | 10±5 (y) | C: -a |
|
|
|
85.00±18.50 |
78.00±11.53 |
|
| Liu, 2007 |
|
| 66±5 | 10±4 (y) |
|
|
|
|
|
| (32) |
|
| III | T: 22 |
|
| T: 50 mg i.v. drip.
Qd-a | 2 weeks | N | N | 85.0±18.5 | 78.0±11.5 |
|
|
|
| C: 23 |
|
| C: -a |
|
|
| 91.6±13.8 | 85.6±15.4 |
|
| Jiang, 2010 | III | T: 42 | 54.12±8.56 | N | T: 40 mg i.v. drip.
Qd-a | 4 weeks | 5.31±1.12 | 5.45±1.05 | 69.04±12.35 | 67.24±8.14 | (33) |
|
|
| C: 38 | 58.15±7.25 | N | C: -a |
| 5.35±1.21 | 5.26±0.95 | 69.25±9.20 | 68.15±10.15 |
|
| Zhang, 2006 | III | T: 40 | 60±3 | 9.1±4.8 (y) | T: 20 mg i.v. drip.
Qd-a | 4 weeks | 12.22±5.14 | 7.51±2.69 | 153.31±46.67 | 104.47±30.43 | (34) |
|
|
| C: 40 | 61±3 | 9.3±5.4 (y) | C: -a |
| 12.32±5.26 | 8.54±3.26 | 152.24±50.14 | 123.78±35.67 |
|
| Qiao, 2010 |
| | 66±3 | 9±3 (y) |
|
|
|
|
|
| (35) |
|
| III | T: 30 | 49–72 | 6–21 (y) | T: 40 mg i.v. drip.
Qd-a | 1 month | 16.3±2.8 | 10.0±0.9 | 121.03±24.90 | 72.82±11.48 |
|
|
|
| C: 30 | 50–78 | 5–23 (y) | C: -a |
| 15.9±3.1 | 12.5±2.8 | 123.02±18.40 | 87.02±12.83 |
|
| Lan, 2008 |
|
| 30–76 (mean
57.3) | 5–28 (mean 1.9)
(y) |
|
|
|
|
|
| (36) |
|
| III | T: 13 |
|
| T: 100 mg i.v.
drip. Qd-b | 2 weeks | N | 4.1±1.2 | N | 75±13 |
|
|
|
| C: 13 |
|
| C: -b |
|
| 4.6±1.5 |
| 78±14 |
|
|
| IV | T: 15 |
|
| T: 100 mg i.v.
drip. Qd-b | 2 weeks | N | 7.6±2.3 | N | 122±36 |
|
|
|
| C: 15 |
|
| C: -b |
|
| 12.0±3.5 |
| 150±25 |
|
| Huang, 2012 |
|
| 69.62±4.28 | N |
|
|
|
|
|
| (37) |
|
| III | T: 21 |
|
| T: 100 mg i.v.
drip. Qd-a | 15 days | N | 4.2±1.3 | N | 76±12 |
|
|
|
| C: 21 |
|
| C: -a |
|
| 4.7±1.4 |
| 79±13 |
|
|
| IV | T: 22 |
|
| T: 100 mg i.v.
drip. Qd-a | 15 days | N | 7.5±2.2 | N | 121±35 |
|
|
|
| C: 22 |
|
| C: -a |
|
| 7.7±3.2 |
| 151±30 |
|
| Table III.Study characteristics: Effect of
breviscapine on blood fat and fibrinogen in patients with DN. |
Table III.
Study characteristics: Effect of
breviscapine on blood fat and fibrinogen in patients with DN.
|
| Cholesterol
(mmol/l) | Triglyceride
(mmol/l) | HDL | Fg (g/l) |
|
|---|
|
|
|
|
|
|
|
|---|
| First author,
year | Stage of DN | n | Age (years) | History of DM
(years) | Intervention
(breviscapine) | Treatment
duration | Baseline | After
intervention | Baseline | After
intervention | Baseline | After
intervention | Baseline | After
intervention | Refs. |
|---|
| Wang, 2009 | III | T: 20 | 68 (mean) | 8 (mean) | T: 50 mg i.v.drip.
Qd-a,x | 2 weeks | 5.8±0.9 | 5.8±0.7 | 1.9±0.8 | 1.9±0.7 | N | N | N | N | (19) |
|
|
| C: 20 | 70 (mean) | 10 (mean) | C: -a,x |
| 5.9±0.8 | 5.9±0.8 | 1.9±0.7 | 1.9±0.7 |
|
|
|
|
|
| Huang, 2011 | III | T: 18 | 64 (mean) | 8 (mean) | T: 50 mg i.v.drip.
Qd-a,x | 4 weeks | 5.8±0.9 | 5.8±0.7 | 1.9±0.8 | 1.9±0.7 | N | N | N | N | (20) |
|
|
| C: 18 | 66 (mean) | 10 (mean) | C: -a,x |
| 5.9±0.8 | 5.9±0.8 | 1.9±0.7 | 1.9±0.7 |
|
|
|
|
|
| Wu, 2009 | IV | T: 36 | 62±2 | 5.01±1.8 | T: 50 mg i.v.drip.
Qd-a,x | 1 month | 6.36±0.33 | 4.21±0.42 | 3.85±0.26 | 2.21±0.39 | N | N | 5.48±0.35 | 4.01±0.38 | (22) |
|
|
| C: 34 | 61±3 | 5.32±2.45 | C: -a,x |
| 6.48±0.26 | 5.95±0.31 | 3.65±0.41 | 3.35±0.31 |
|
| 5.35±0.36 | 5.15±0.28 |
|
| Huang, 2004 | III | T: 34 | 66.5±8.4 | 4.8±2.5 | T: 60 mg i.v.drip.
Qd-u,x | 3 weeks | 5.59±1.34 | 3.87±1.46 | 2.25±0.97 | 1.56±0.78 | N | N | N | N | (23) |
|
|
| C: 28 | 65.3±6.5 | 4.58±2.1 | C: -u,x |
| 5.79±1.56 | 3.99±1.65 | 2.19±0.89 | 1.67±0.67 |
|
|
|
|
|
| Qiao, 2009 |
|
| 62.25±8.9 | N |
|
|
|
|
|
|
|
|
|
| (26) |
|
| IV | T: 52 |
|
| T: 40 mg i.v.drip.
Qd-a,w | 4 weeks | 4.95±0.90 | 4.41±0.52 | 1.70±0.80 | 1.60±0.56 | 0.93±0.17 | 1.24±0.35 | N | N |
|
|
|
| C: 40 |
|
| C: -a,w |
| 4.80±0.89 | 4.76±0.81 | 1.76±0.62 | 1.78±0.61 | 0.96±0.15 | 0.98±0.18 |
|
|
|
| Zhong, 2011 |
|
| 41–65 (mean
54) | 3–8 |
|
|
|
|
|
|
|
|
|
| (27) |
|
| III | T: 30 |
|
| T: 30 mg i.v.drip.
Qd-a,x | 3 weeks | N | N | 2.86±0.45 | 1.84±0.29 | N | N | 5.99±0.75 | 3.83±0.53 |
|
|
|
| C: 29 |
|
| C: -a,x |
|
|
| 2.73±0.35 | 2.25±0.27 |
|
| 5.86±0.75 | 4.62±0.31 |
|
| Wang, 2011 | III | T: 18 | N | N | T: 40 mg i.v.drip.
Qd-b,x | 20 days | N | N | 2.90±0.31 | 1.74±0.16 | 1.26±0.12 | 4.52±0.08 | N | N | (39) |
|
|
| C: 18 |
|
| C: -b,x |
|
|
| 2.91±0.29 | 2.71±0.21 | 1.25±0.14 | 2.41±0.06 |
|
|
|
| Qian, 2011 |
|
| 37.5±65.8 | 6.7 (mean) |
|
|
|
|
|
|
|
|
|
| (40) |
|
| III | T: 30 |
|
| T: 60 mg i.v.drip.
Qd-u,x | 2 weeks | N | N | 2.80±0.31 | 1.93±0.33 | 1.45±0.43 | 4.85±0.49 | N | N |
|
|
|
| C: 30 |
|
| C: -u,x |
|
|
| 3.70±1.09 | 2.99±0.40 | 1.74±0.45 | 2.50±0.29 |
|
|
|
| Huang, 2006 | IV | T: 22 | 18–76 (mean
56.8) | N | T: 40 mg i.v.drip.
Qd-b,x | 2 weeks | N | N | N | N | N | N | 5.30±1.73 | 2.84±1.64 | (49) |
|
|
| C: 22 | 20–74 (mean
55.4) |
| C: -b,x |
|
|
|
|
|
|
| 5.45±1.52 | 4.05±1.43 |
|
| Li, 2011 | III | T: 50 | 41–72 (mean
52.5) | 4–11 (mean
8.2) | T: 60 mg i.v.drip.
Qd-u,w | 15 days | 5.24±0.98 | 5.13±0.94 | 2.18±0.89 | 1.94±0.92 | N | N | N | N | (43) |
|
|
| C: 50 | 40–72 (mean
51.8) | 4–10 (mean
7.8) | C: -u,w |
| 5.28±0.96 | 5.25±0.93 | 2.16±0.86 | 2.14±0.94 |
|
|
|
|
|
| Liu, 2003 | III–IV | T: 24 | 46±6.6 | 6.5±4.4 | T: 100 mg i.v.drip.
Qd-b,x | 1 month | 9.33±3.22 | 4.12±1.45 | 2.69±1.53 | 2.06±1.61 | N | N | 5.18±0.61 | 3.13±1.03 | (46) |
|
|
| C: 24 | 46.2±6.8 | 6.2±4.8 | C: -b,x |
| 9.29±3.19 | 5.38±1.36 | 2.78±1.69 | 2.14±1.55 |
|
| 5.24±1.67 | 5.35±1.06 |
|
| Guo, 2008 |
|
| 54.2 | 9.8 |
|
|
|
|
|
|
|
|
|
| (48) |
|
| IV | T: 34 |
|
| T: 50 mg i.v.drip.
Qd-a,x | 20 days | N | N | N | N | N | N | 5.40±0.95 | 4.00±0.44 |
|
|
|
| C: 30 |
|
| C: -a,x |
|
|
|
|
|
|
| 5.20±1.65 | 5.10±0.85 |
|
| Kang, 2003 | III | T: 48 | 61.5±14.6 | 18.7±12.8 | T: 100 mg i.v.drip.
Qd-b,x | 2 weeks | 7.12±0.46 | 6.48±0.21 | 2.50±0.27 | 1.79±0.24 | 0.86±0.15 | 1.08±0.17 | 3.75±0.62 | 2.81±0.57 | (11) |
|
|
| C: 20 | 62.3±11.5 | 18.2±11.6 | C: -b,x |
| 7.08±0.42 | 6.98±0.40 | 2.51±0.26 | 2.47±0.28 | 0.89±0.13 | 0.90±0.12 | 3.64±0.82 | 3.71±0.48 |
|
| Xu, 2008 | III–IV | T: 36 | 42–79 | N | T: 100 mg i.v.drip.
Qd-b,x | 4 weeks | 5.20±0.76 | 3.05±0.72 | 2.69±1.53 | 1.36±1.61 | N | N | 5.18±0.61 | 3.13±1.03 | (29) |
|
|
| C: 40 | 41–76 |
| C: -b,x |
| 5.18±0.73 | 4.98±0.68 | 2.78±1.61 | 2.64±1.55 |
|
| 5.35±1.67 | 5.24±1.06 |
|
| Liu, 2007 |
|
| 66±5 | 10±4 |
|
|
|
|
|
|
|
|
|
| (31) |
|
| III | T: 22 |
|
| T: 50 mg i.v.drip.
Qd-a,x | 2 weeks | 5.79±0.88 | 5.85±0.74 | 1.94±0.83 | 1.90±0.72 | N | N | N | N |
|
|
|
| C: 23 |
|
| C: -a,x |
| 5.91±0.81 | 5.86±0.81 | 1.90±0.66 | 1.89±0.69 |
|
|
|
|
|
| Jiang, 2010 | III | T: 42 | 54.12±8.56 | N | T: 40 mg i.v.drip.
Qd-a,x | 4 weeks | N | N | N | N | N | N | 4.72±2.01 | 2.53±1.65 | (33) |
|
|
| C: 38 | 58.15±7.25 |
| C: -a,x |
|
|
|
|
|
|
| 4.69±1.52 | 4.32±1.29 |
|
| Qiao, 2010 |
|
| 66±3 | 9±3 |
|
|
|
|
|
|
|
|
|
| (35) |
|
| III | T: 30 | 49–72 | 6–21 | T: 40 mg i.v.drip.
Qd-a,y | 1 month | 4.93±0.81 | 4.29±0.50 | 1.73±0.71 | 1.40±0.40 | N | N | N | N |
|
|
|
| C: 30 | 50–78 | 5–23 | C: -a,y |
| 4.80±0.29 | 4.78±0.80 | 1.75±0.18 | 1.73±0.60 |
|
|
|
|
|
| Yuan, 2005 | III | T: 24 | N | N | T: 40 mg i.v. drip.
Qd-b,x | 30 days | 8.17±1.04 | 6.49±1.30 | 2.89±0.33 | 1.75±0.15 | 1.25±0.13 | 4.95±0.09 | 3.96±0.08 | 3.28±0.02 | (47) |
|
|
| C: 24 |
|
| C: -b,x |
| 8.19±1.00 | 7.81±1.23 | 2.90±0.29 | 2.69±0.20 | 1.24±0.15 | 2.00±0.07 | 3.97±0.08 | 3.88±0.05 |
|
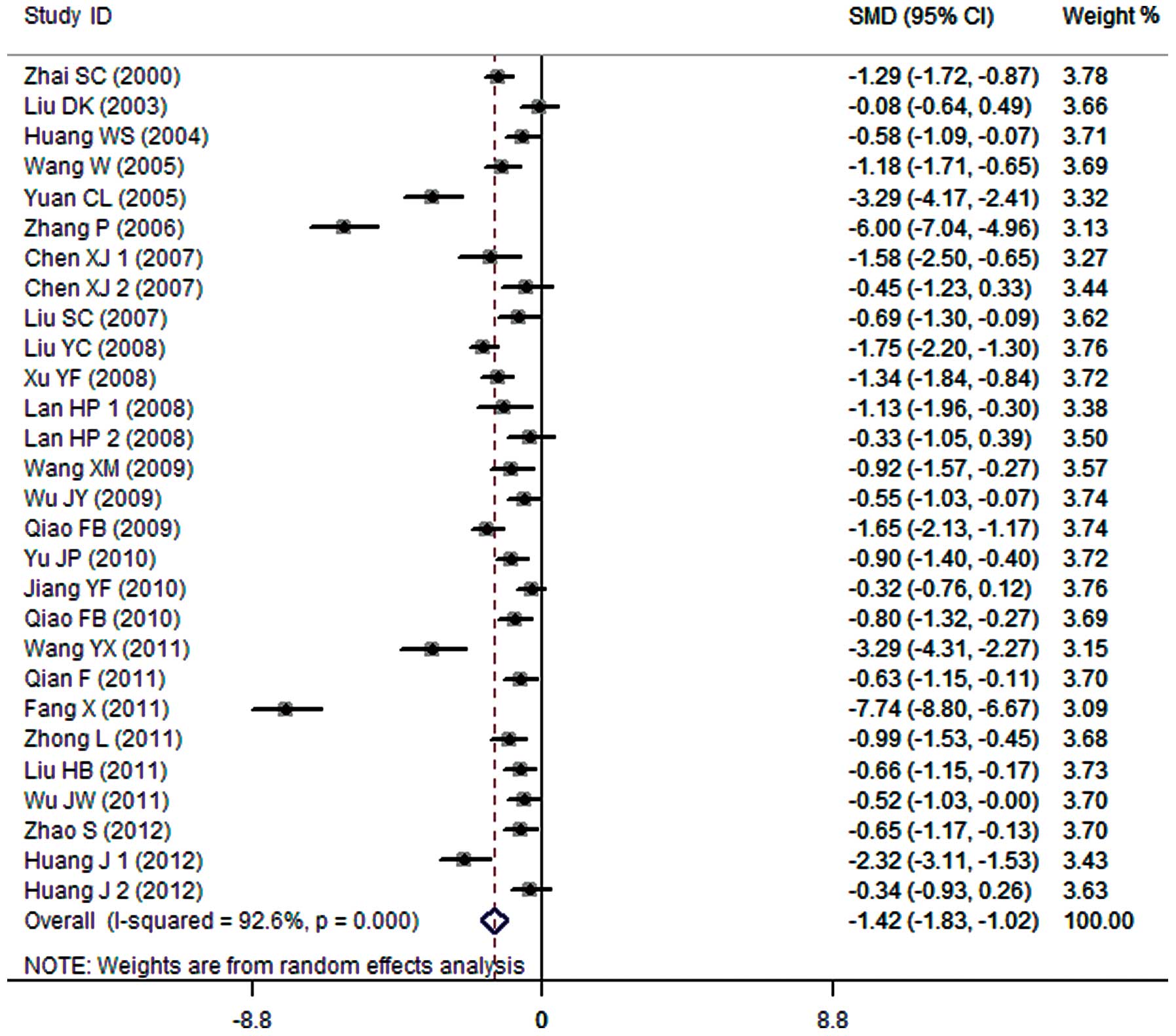
24-h urine protein
A total of 25 clinical trials evaluated the 24-h
urine protein in patients treated with breviscapine (n=858) and the
control group (n=836). Fig. 1
presents a forest plot for the outcome measurements (SMD, −1.42;
95% CI, −1.83 to −1.02). In comparison with the control group,
breviscapine significantly reduced 24-h urine protein in patients
with DN (P<0.001).
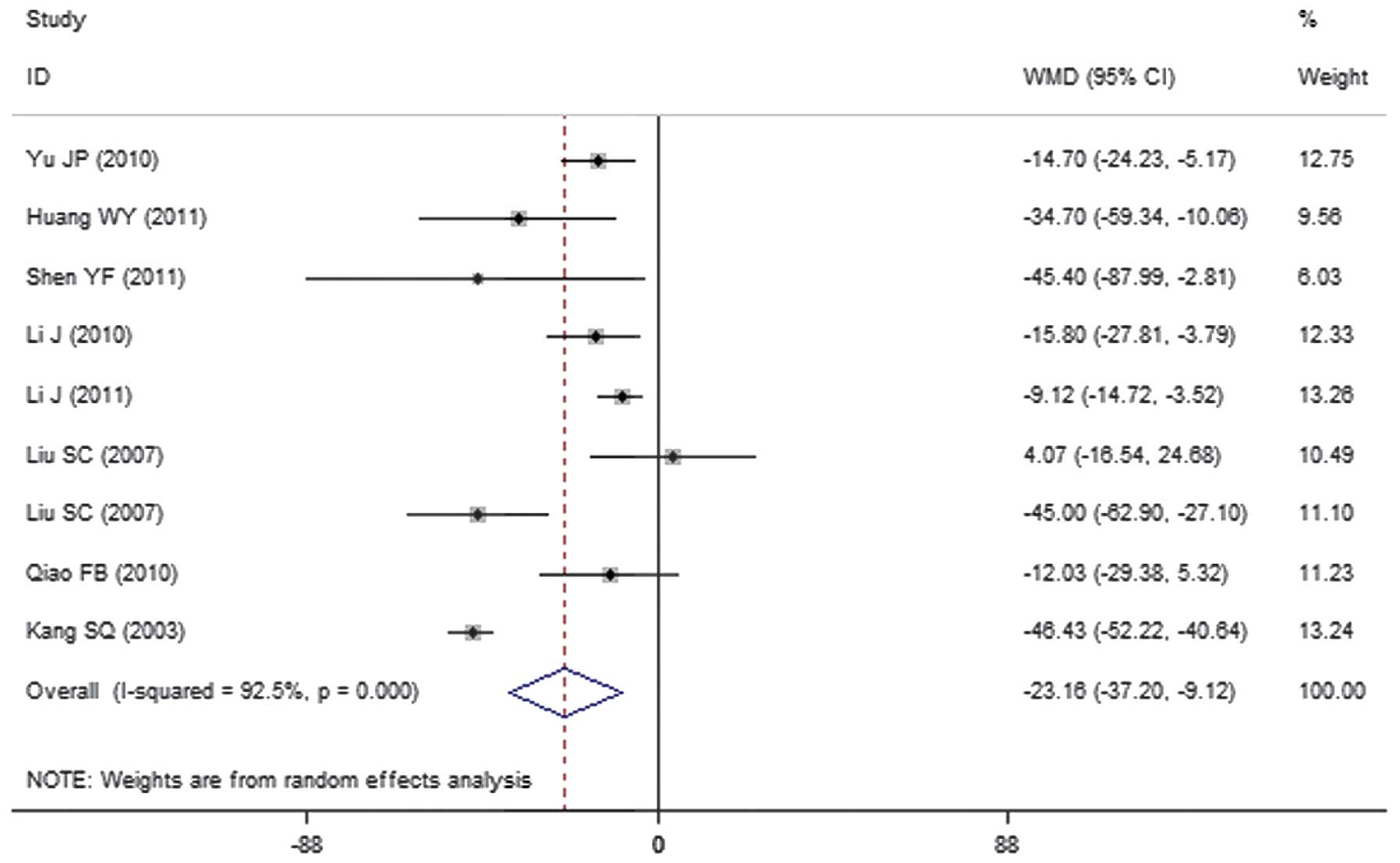
Urinary albumin excretion rate
A total of 9 clinical trials evaluated the urinary
albumin excretion rate in patients treated with breviscapine
(n=291) and the control group (n=264). Fig. 2 presents a forest plot for the
outcome measurements (WMD, −23.16; 95% CI, −37.20 to −9.12). In
comparison with the control group, breviscapine significantly
reduced the urinary albumin excretion rate in patients with DN
(P<0.001).
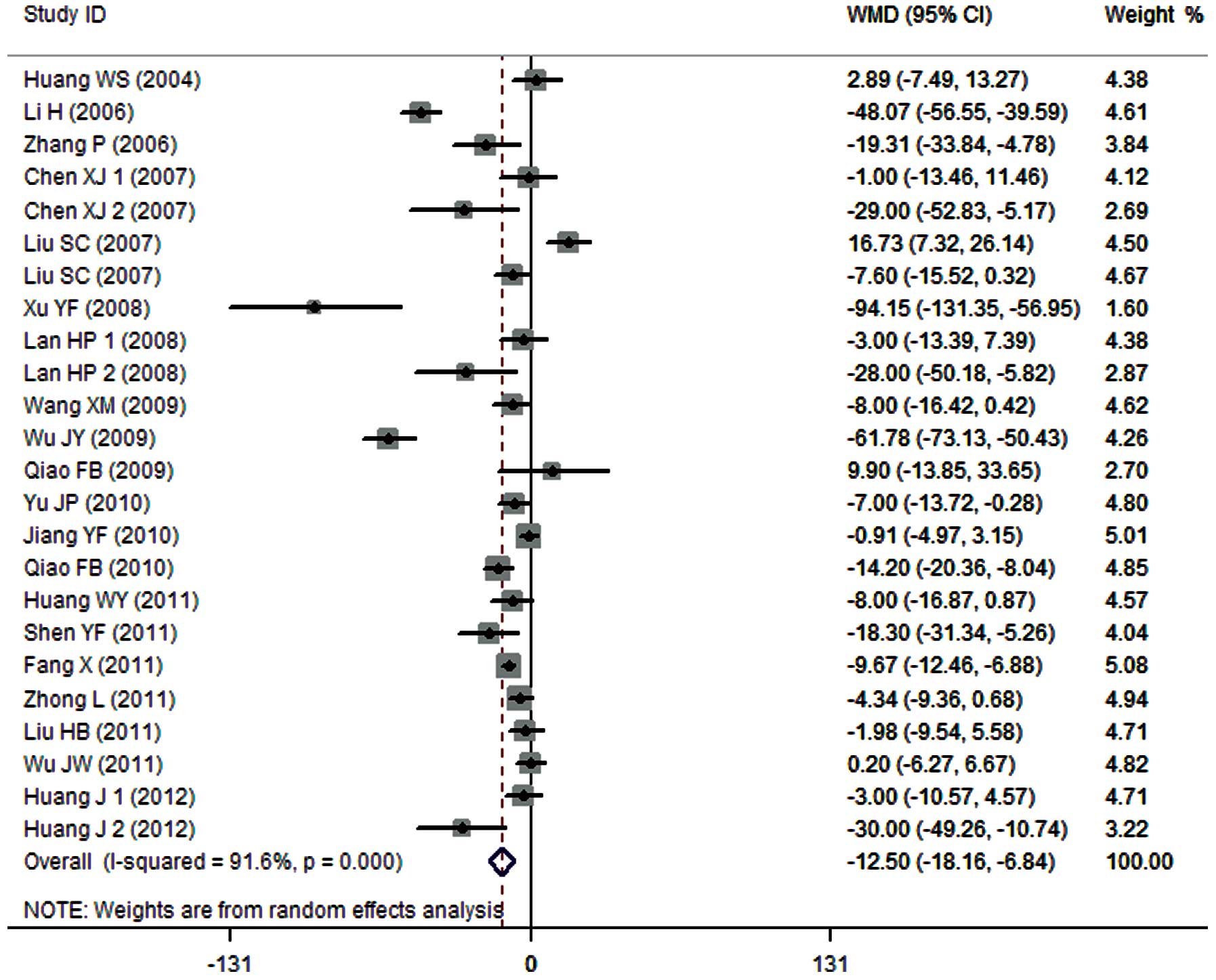
SCr expression levels
A total of 21 clinical trials evaluated the
expression level of SCr in patients treated with breviscapine
(n=711) and the control group (n=689). Fig. 3 presents a forest plot for the
outcome measurements (WMD, −12.50; 95% CI, −18.16 to −6.84). In
comparison with the control group, breviscapine significantly
reduced the expression level of SCr in patients with DN
(P<0.001).
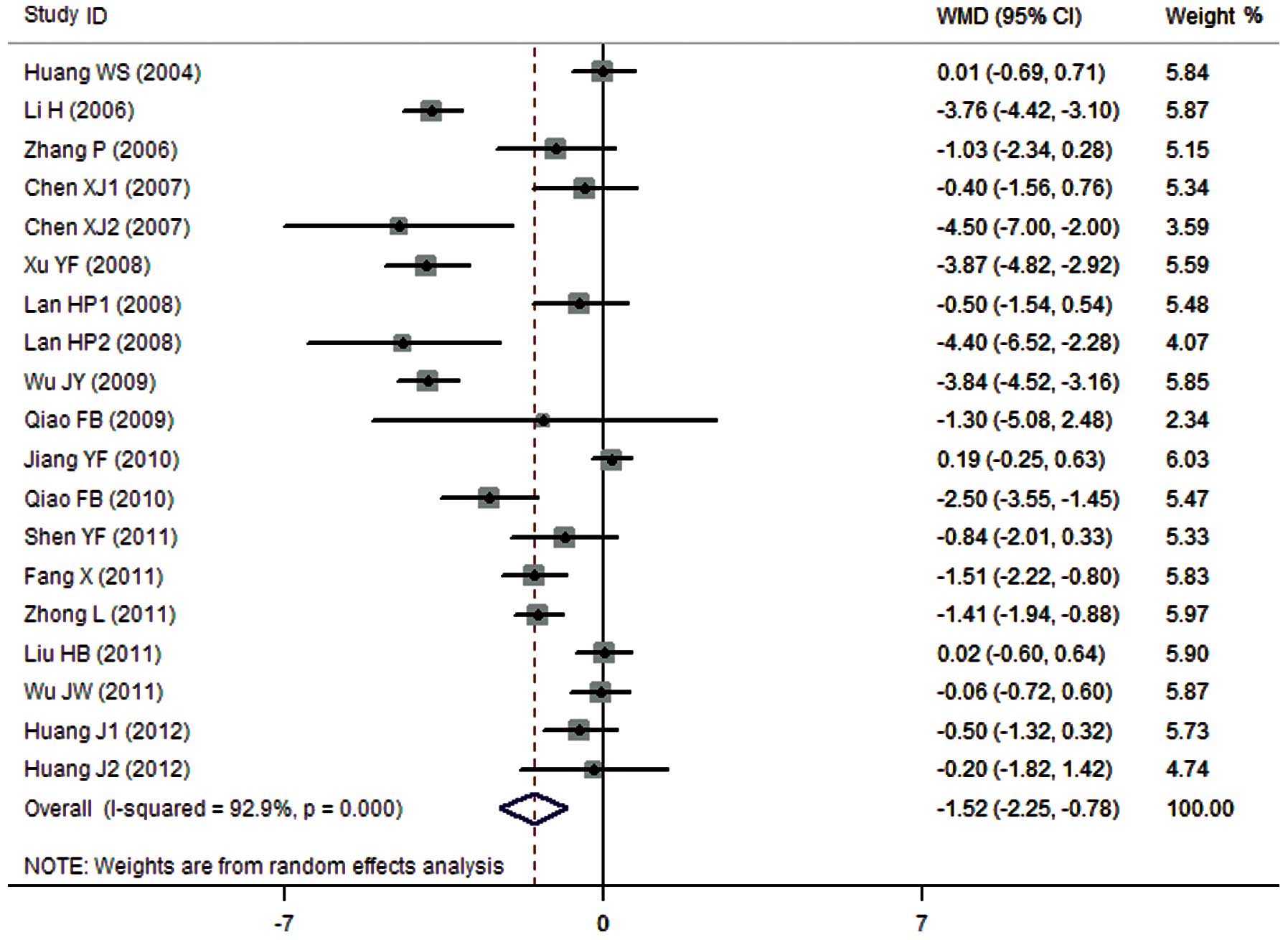
BUN expression levels
A total of 16 clinical trials evaluated the
expression level of BUN in patients treated with breviscapine
(n=594) and the control group (n=572). Fig. 4 presents a forest plot for the
outcome measurements (WMD, −1.52; 95% CI, −2.25 to −0.78). In
comparison with the control group, breviscapine significantly
reduced the expression level of BUN in patients with DN
(P<0.001).
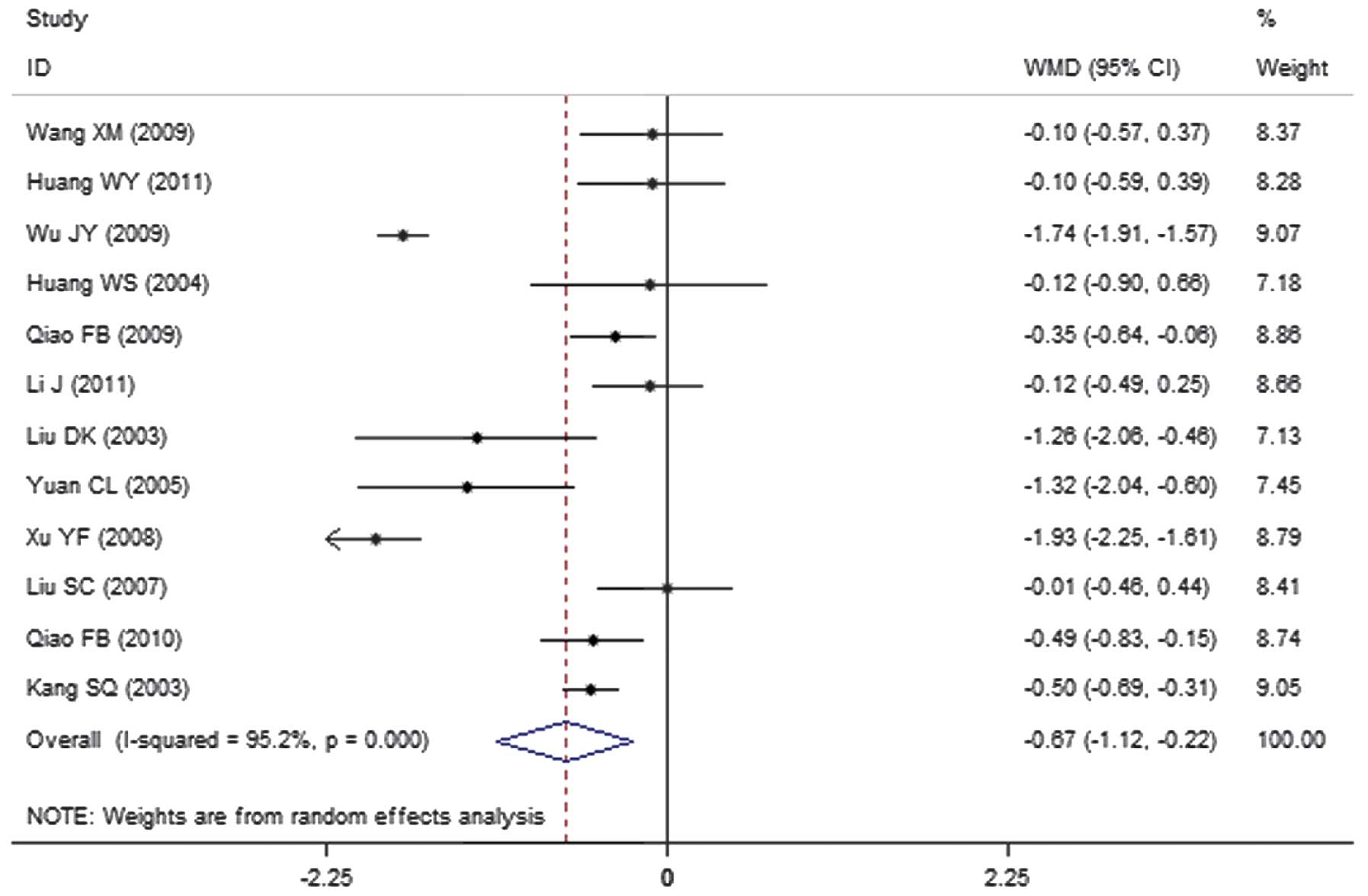
Cholesterol expression levels
A total of 12 clinical trials evaluated the
expression level of cholesterol in patients treated with
breviscapine (n=394) and the control group (n=351). Fig. 5 presents a forest plot for the
outcome measurements (WMD, −0.67; 95% CI, −1.12 to −0.22). In
comparison with the control group, breviscapine significantly
reduced the expression level of cholesterol in patients with DN
(P<0.001).
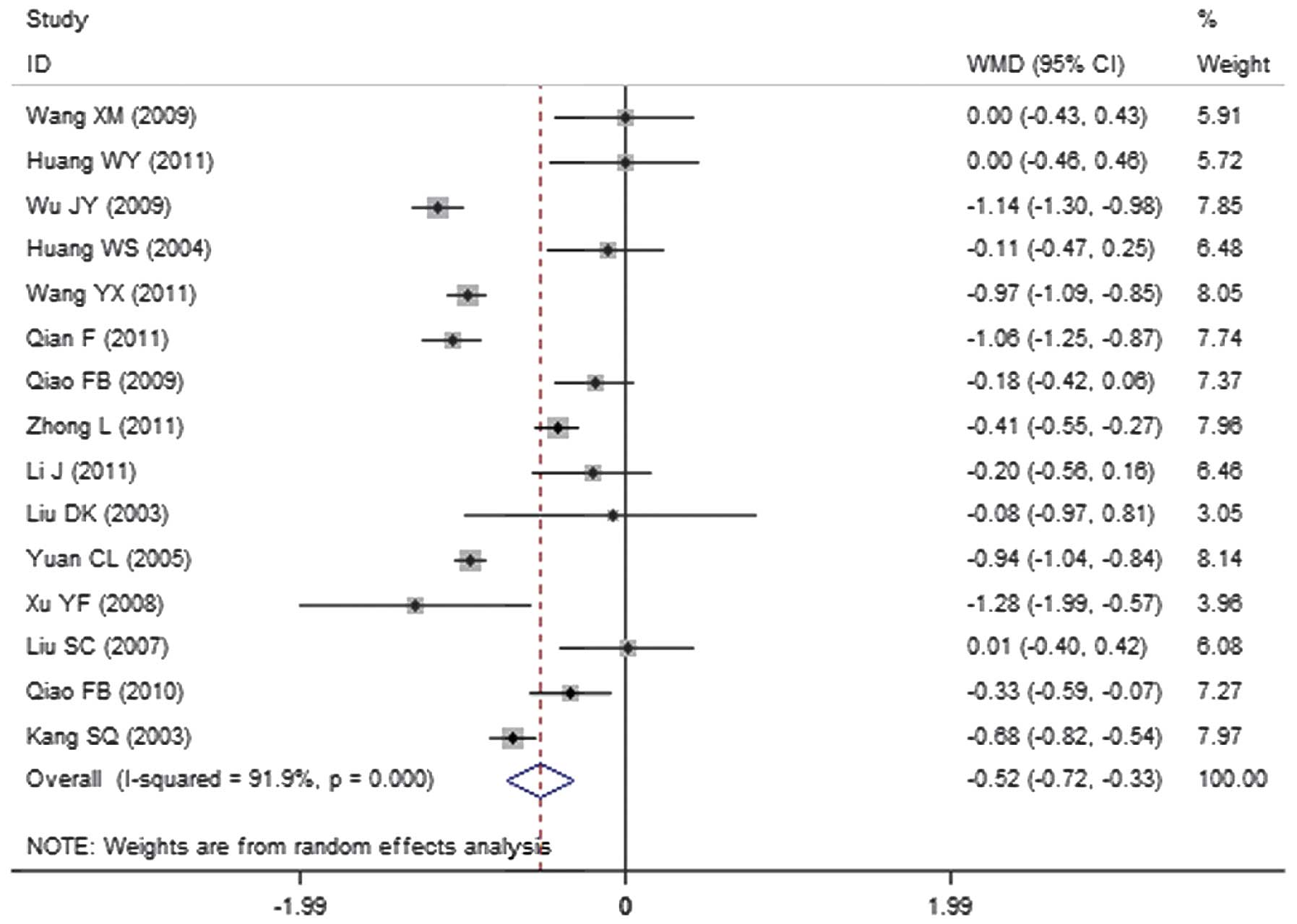
Triglyceride expression levels
A total of 15 clinical trials evaluated the
expression level of triglycerides in patients treated with
breviscapine (n=472) and the control group (n=428). Fig. 6 presents a forest plot for the
outcome measurements (WMD, −0.52; 95% CI, −0.72 to −0.33). In
comparison with the control group, breviscapine significantly
reduced the expression level of triglycerides in patients with DN
(P<0.001).
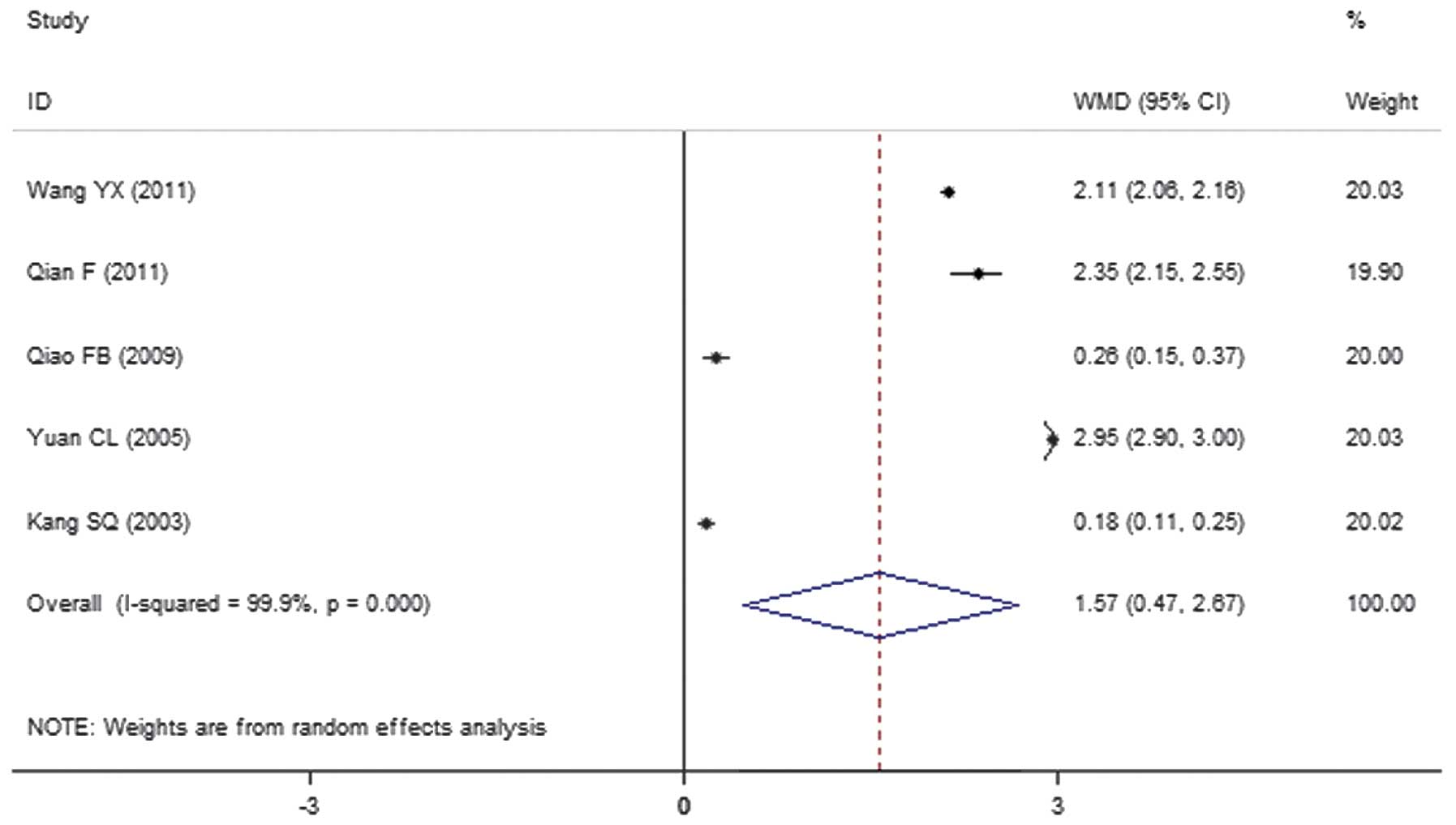
HDL expression levels
A total of 5 clinical trials evaluated the
expression level of HDL in patients treated with breviscapine
(n=172) and the control group (n=132). Fig. 7 presents a forest plot for the
outcome measurements (WMD, 1.57; 95% CI, 0.47 to 2.67). In
comparison with the control group, breviscapine significantly
increased the expression level of high density lipoproteins in
patients with DN (P<0.001).
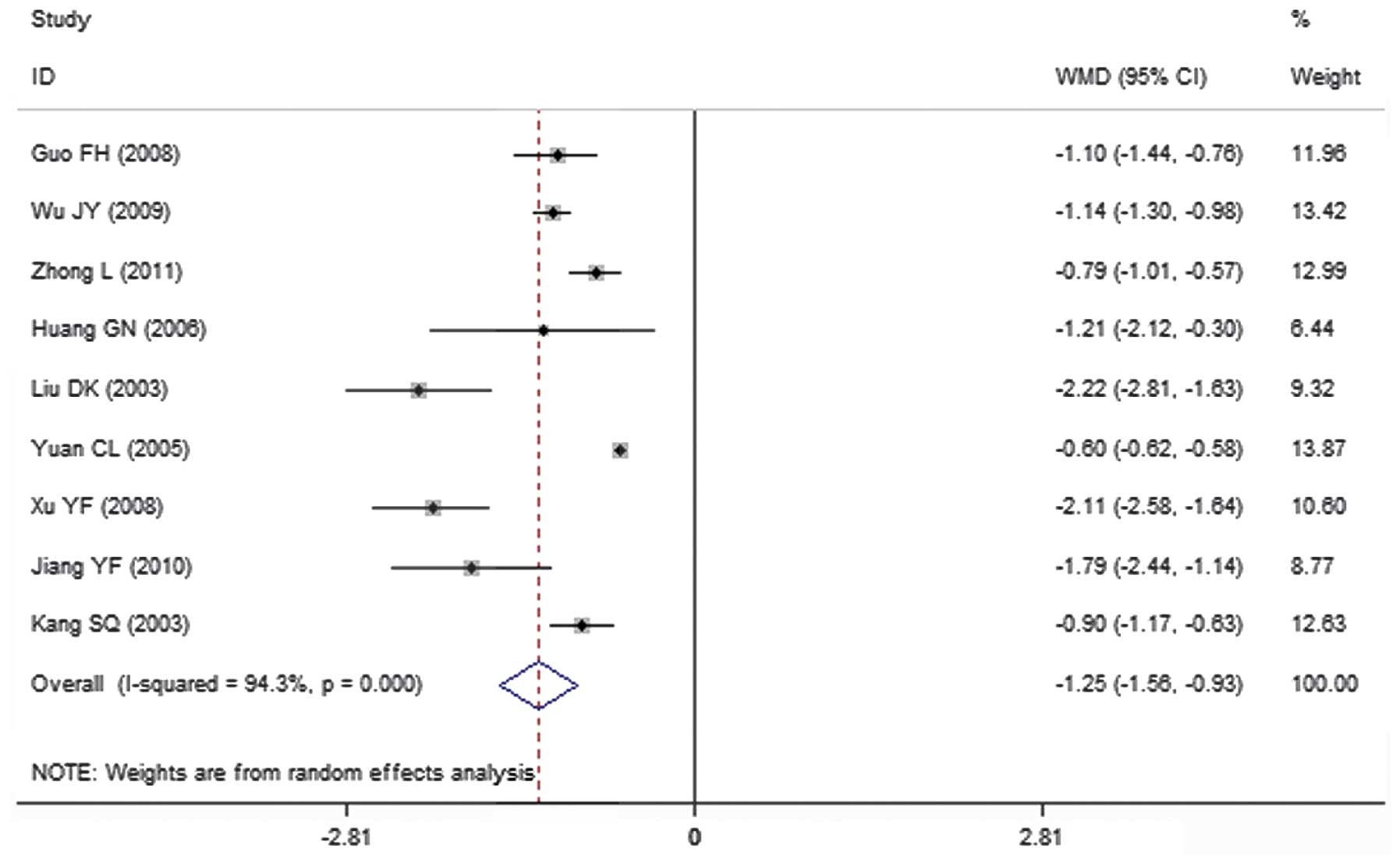
Fibrinogen expression levels
A total of 9 clinical trials evaluated the
expression level of fibrinogen in patients treated with
breviscapine (n=296) and the control group (n=261). Fig. 8 presents a forest plot for the
outcome measurements (WMD, −1.25; 95% CI, −1.56 to −0.93). In
comparison with the control group, breviscapine significantly
reduced the expression level of fibrinogen in patients with DN
(P<0.001).
Adverse effects
No systematic review on adverse effects was
conducted as reporting of side effects was lacking in the clinical
trials in this meta-analysis.
Publication bias assessment
The Begg's test determined that bias assessment was
not significant in any of the RCTs analyzed (P>0.1).
Discussion
The prevalence of DM has markedly increased in
recent years and is projected to affect 4.4% of the world's
population by 2030 (51). DN is
considered to be the most devastating complication associated with
diabetes, with respect to a patients' quality of life and chances
of survival (52). Current
treatments are not adequate, and as the burden of DN continues to
increase worldwide there is a requirement for the development of
novel treatments (53).
Oxidative stress caused by increased free radical
production is understood to serve a central role in the development
of DN (54). The abnormal metabolism
of glucose or free fatty acids via mitochondria pathways, and the
activation of nicotinamide adenine dinucleotide phosphate oxidases
via PKC have been recognized as contributors towards the production
of oxidants (55). Breviscapine
possesses a variety of pharmacological functions other than
hemodynamic effects, and can serve as an anti-oxidative stress
agent and inhibitor of PKC (56,57). In
addition, Zhao et al (58)
and Wagener et al (59)
observed in diabetic rat models that breviscapine can inhibit
podocyte apoptosis by modulating the expression of B-cell lymphoma
2 (Bcl-2) and Bcl-2-Associated X Protein genes.
The present meta-analysis quantitatively evaluated
the clinical effect of breviscapine in the treatment of patients
with DN by integrating the outcomes of 35 RCTs that studied the
effects of breviscapine on 1,188 patients with DN and 1,132 control
subjects. The results demonstrated that the expression levels of
SCr and BUN were significantly lower in patients treated with
breviscapine in comparison with control subjects, suggesting that
the drug serves a protective role in the renal system of patients
with DN.
Microalbuminuria is regarded as the earliest
clinical sign of DN. It is defined as a urinary albumin excretion
rate ranging from 30–300 mg/day, and the definitive measurement is
based on a timed urine collection during a 24-h period (60). The present meta-analysis indicated
that breviscapine can reduce urinary protein levels, with a
reduction in 24-h urine protein values and the urinary albumin
excretion rate; a reduction in urinary protein may contribute
towards the renal protective effect of breviscapine in patients
with DN.
There is evidence that dyslipidemia serves an
important role in the progression of kidney disease in patients
with diabetes (61). Dyslipidemia in
diabetes is a condition that results in hypertriglyceridemia, low
high-density lipoprotein levels, and increased small and
low-density lipoprotein particles (62). Dyslipidemia is associated with the
occurrence and progression of DN, and chronic kidney disease
affects dyslipidemia (63). Lipids
may cause glomerular and tubulointerstitial injury through
mediators such as reactive oxygen species, cytokines and
chemokines, and through hemodynamic changes (64). A number of trials have demonstrated
that treating dyslipidemia not only decreased the risk of
cardiovascular events, but also delayed the progression of DN
(65). The present meta-analysis
indicates that breviscapine reduces the levels of cholesterol and
triglyceride, but increases the level of HDL, in patients with DN;
breviscapine is, therefore, capable of reversing dyslipidemia and
protecting the renal system.
The present meta-analysis also demonstrated that
breviscapine can reduce fibrinogen levels in patients with DN,
which is in accordance with its function of promoting fibrinolytic
activity, or may be related associated indirectly with the
reduction of urine protein levels by breviscapine.
The protective effect of breviscapine is important
with regard to the treatment of patients with DN; breviscapine
reduces urine protein, improves renal function and adjusts
dyslipidemia. However, the present study explores only the clinical
effect of breviscapine, and further studies are required to
identify its underlying mechanisms. It is important to note that
the majority of the RCTs analyzed in the present study were not of
the highest quality; the toxicity of the drug was not thoroughly
investigated and in a number of RCTs the lack of liver and kidney
toxicity was discussed, but the associated data was not presented
in detail. Further research is required that will adopt high
quality methodology, including double-blind, multi-centered RCTs
with large samples, and conduct long-term follow ups of patients
treated with breviscapine in order to investigate its long-term
safety.
Acknowledgements
The present study was supported by the Chinese
Society of Nephrology (grant no. 13030320417).
References
|
1
|
Liu R, Zhong Y, Li X, Chen H, Jim B, Zhou
MM, Chuang PY and He JC: Role of transcription factor acetylation
in diabetic kidney disease. Diabetes. 63:2440–2453. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lai X, Zhang AH, Chen SY, He L, Su CY, Fan
MH and Wang T: Outcomes of stage 1–5 chronic kidney disease in
Mainland China. Ren Fail. 36:520–525. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Stanton RC: Frontiers in diabetic kidney
disease: Introduction. Am J Kidney Dis. 63(2 Suppl 2): S1–S2. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Roscioni SS, Heerspink HJ and de Zeeuw D:
The effect of RAAS blockade on the progression of diabetic
nephropathy. Nat Rev Nephrol. 10:77–87. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zhang RW, Zhang YL, Wang JS, Lin YY and
Shang B: Isolation and identification of flavonoids from shortscape
fleabane (Erigeron breviscapus). Zhong Cao Yao. 19:199–201.
1988.(In Chinese).
|
|
6
|
Wang M, Xie C, Cai RL, Li XH, Luo XZ and
Qi Y: Studies on antioxidant activities of breviscapine in the
cell-free system. Am J Chin Med. 36:1199–1207. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wang M, Zhang WB, Zhu JH, Fu GS and Zhou
BQ: Breviscapine ameliorates cardiac dysfunction and regulates the
myocardial Ca(2+)-cycling proteins in streptozotocin-induced
diabetic rats. Acta Diabetol. 47(Suppl 1): S209–S218. 2010.
View Article : Google Scholar
|
|
8
|
Jia JH, Chen KP, Chen SX, Liu KZ, Fan TL
and Chen YC: Breviscapine, a traditional Chinese medicine,
alleviates myocardial ischaemia reperfusion injury in diabetic
rats. Acta Cardiol. 63:757–762. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cao W, Liu W, Wu T, Zhong D and Liu G:
Dengzhanhua preparations for acute cerebral infarction. Cochrane
Database Syst Rev. 4:CD0055682008.PubMed/NCBI
|
|
10
|
He M, Xue ZM, Li J and Zhou BQ:
Breviscapine inhibits high glucose-induced proliferation and
migration of cultured vascular smooth muscle cells of rats via
suppressing the ERK1/2 MAPK signaling pathway. Acta Pharmacol Sin.
33:606–614. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kang SQ and Liu JY: Effect of breviscapine
on urinary micro-albumine in patients with diabetes mellitus type
2. Zhongguo Zhong Xi Yi Jie He Za Zhi. 23:458–459. 2003.(In
Chinese). PubMed/NCBI
|
|
12
|
Wei L and Tan J: Clinical observation on
Breviscapine in treating hypertension patients complicated with
micro-albuminuria of renal impairment. Chin J Integr Med. 11:31–33.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Definition, Diagnosis and Classification
of Diabetes Mellitus and its Complications. World Health
Organisation. 1999.
|
|
14
|
American Diabetes Association. Report of
the expert committee on the diagnosis and classification of
diabetes mellitus. Diabetes Care. 7:1183–1197. 1997.
|
|
15
|
Mogensen CE, Christensen CK and Vittinghus
E: The stages in diabetic renal disease. With emphasis on the stage
of incipient diabetic nephropathy. Diabetes. 32(Suppl 2): 64–78.
1983. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Olivo SA, Macedo LG, Gadotti IC, Fuentes
J, Stanton T and Magee DJ: Scales to assess the quality of
randomized controlled trials: a systematic review. Phys Ther.
88:156–175. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Chen XH: Clinical observation of therapy
with Breviscapine for diabetic nephropathy. Zhongguo Liao Yang Yi
Xue. 16:168–169. 2007.(In Chinese).
|
|
18
|
Yu JP: Breviscapine valsartan combined
treatment of early diabetic nephropathy. Zhonghua Zhong Yi Yao Xue
Kan. 28:1337–1338. 2010.(In Chinese).
|
|
19
|
Wang XM: Impact of valsartan combined
breviscapine trace urinary albumin in diabetic nephropathy and
serum C-reactive protein. Lin Chuang He Li Yong Yao Za Zhi.
2:25–26. 2009.(In Chinese).
|
|
20
|
Huang WY: Observation of therapeutic
effects with losartan and breviscapine on early diabetic
nephropathy. Zhongguo Xiang Cun Yi Xue. 18:27–28. 2011.(In
Chinese).
|
|
21
|
Shen YF and Dai Z: Clinical observation of
therapy with candesartan and breviscapine on diabetic nephropathy.
Zhongguo Shi Yong Yi Yao. 6:148–149. 2011.(In Chinese).
|
|
22
|
Wu JY, Liang D, Ma ZH and Chen GH:
Clinical observation of therapeutic effects with irbesartan and
breviscapine on diabetic nephropathy. Guo Ji Yi Yao Wei Sheng Dao
Bao. 15:53–55. 2009.(In Chinese).
|
|
23
|
Huang WS and Sheng P: Clinical observation
of therapy with breviscapine injection on early diabetic
nephropathy. Dang Dai Yi Xue. 10:58–59. 2004.(In Chinese).
|
|
24
|
Li H: Clinical observation of treatment
effects with breviscapine injection and enalapril on 76 patients
with diabetic nephropathy. Shi Yong Lin Chuang Yi Yao Za Zhi.
10:85–86. 2006.(In Chinese).
|
|
25
|
Fang X: Evaluation of therapeutic effects
with breviscapine injection and enalapril on early diabetic
nephropathy. Dang Dai Yi Xue. 17:131–132. 2011.(In Chinese).
|
|
26
|
Qiao FB, Tian Z and He YL: Observation of
treatment with breviscapine injection and benazepril on 52 cases
with azotemia of diabetic nephropathy. Zhongguo Yao Ye. 18:55–56.
2009.(In Chinese).
|
|
27
|
Zhong L and Li K: Therapeutic effect of
Breviscapine combined with Enalapril on early diabetic nephropathy.
Hua Xi Yi Xue. 26:493–495. 2011.(In Chinese).
|
|
28
|
Liu HB, Liu CHa and Li XN: Observation of
therapeutic effects with breviscapin on 68 cases with early
diabetic nephropathy. Qingdao Yi Yao Wei Sheng. 43:41–42. 2011.(In
Chinese).
|
|
29
|
Xu YF and Yu JH: Clinical observation of
treatment with breviscapin on 36 cases with diabetic nephropathy.
Fu Jian Yi Yao Za Zhi. 30:133–134. 2008.(In Chinese).
|
|
30
|
Wu JW, Ling JH and Huang XN: Clinical
observation of treatment with breviscapin and telmisartan on early
diabetic nephropathy. Lin Chuang He Li Yongyao Za Zhi. 4:54–55.
2011.(In Chinese).
|
|
31
|
Liu SC, Wen FG and Zhao CY: Clinical
observation of treatment with breviscapin and lotensin on urinary
protein of early diabetic nephropathy. Zhongguo Zhong Xi Yi Jie He
Za Zhi. 27:5302007.(In Chinese).
|
|
32
|
Liu SC and Zhao CY: Protective effects of
treatment with breviscapin and lotensin on early diabetic
nephropathy. Guo Ji Zhong Yi Zhong Yao Za Zhi. 29:246–247. 2007.(In
Chinese).
|
|
33
|
Jiang YF, He LQ and Shen LP: Clinical
observation on therapeutic effects of combined use of dengzhanhuasu
and losartan in treating early diabetic nephropathy. Liaoning Zhong
Yi Xue Yuan Xue Bao. 12:43–45. 2010.(In Chinese).
|
|
34
|
Zhang P: Clinical observation on
breviscapin combined with cozaar for diabetic nephropathy. Zhongguo
Yao Fang. 17:1403–1404. 2006.(In Chinese).
|
|
35
|
Qiao FB, Li CT, Li LF, Zhang CJ, He QL and
Ren LX: Clinical observation of treatment with breviscapine and
candesartan on early diabetic nephropathy. Yi Nan Bing Za Zhi.
9:606–608. 2010.(In Chinese).
|
|
36
|
Lan HP and Wu FQ: Clinical observation of
treatment with breviscapine on diabetic nephropathy. Zhengjiang Lin
Chuang Yi Xue. 10:3892008.(In Chinese).
|
|
37
|
Huang J, Wen Z and Feng Y: Clinical
observation of treatment with breviscapine on diabetic nephropathy.
Zhongguo Bao Jian Ying Yang. 9:3347–3348. 2012.(In Chinese).
|
|
38
|
Zhai SC: Analysis of treatment with
breviscapine on diabetic nephropathy. Shandong Yi Yao. 40:69–70.
2000.(In Chinese).
|
|
39
|
Wang YX: Clinical observation of therapy
with breviscapine injection on diabetic nephropathy. Zhong Wai Yi
Liao. 30:1262011.(In Chinese).
|
|
40
|
Qian F: Clinical observation of
therapeutic effects with breviscapine injection on 60 patients with
diabetic nephropathy. An Mo Yu Kang Fu Yi Xue. 2:91–92. 2011.(In
Chinese).
|
|
41
|
Li J: Observation of therapeutic effects
with breviscapine injection and valsartan on early diabetic
nephropathy. Zhongguo She Qu Yi Shi. 12:1172010.(In Chinese).
|
|
42
|
Wang W, Xing L, Wang CH and Li JC:
Influence of breviscapine injection on hemorrheology and
microcirculation of patients with diabetic nephropathy. Zhonghua
Zhong Yi Yao Xue Hui. 14:963–997. 2005.(In Chinese).
|
|
43
|
Li J, Wu LY and Wang CY: Influence of
breviscapine injection to correlated inflammatory cytokines in
patients with type 2 early diabetic nephropathy. Zhong Yao Yao Li
Yu Lin Chuang. 27:110–112. 2011.(In Chinese).
|
|
44
|
Zhao S: Observation of therapeutic effects
with breviscapin on diabetic microalbuminuria. Guiyang Zhong Yi Xue
Yuan Xue Bao. 34:37–38. 2012.(In Chinese).
|
|
45
|
Liu YC: Observation of therapeutic effects
with breviscapine on diabetic nephropathy. She Qu Zhong Yi Yao.
10:762008.(In Chinese).
|
|
46
|
Liu DK: Observation of therapeutic effects
with breviscapin on hyperviscosity in diabetic nephropathy. Hubei
Zhong Yi Za Zhi. 25:13–14. 2003.(In Chinese).
|
|
47
|
Yuan CL and Yuan LY: Clinical observation
of therapeutic effects with breviscapine on diabetic nephropathy.
Shi Yong Tang Niao Bing Za Zhi. 2:232005.(In Chinese).
|
|
48
|
Guo FH, Lv GY and Fan P: Clinical
observation of therapy with valsartan and Dengzhanhuasu for
diabetic nephropathy. Zhonghua Quan Ke Yi Xue. 6:895–896. 2008.(In
Chinese).
|
|
49
|
Huang GN, Chen JY and Zhang MY:
Hemorrheology impact of treatment with breviscapine injection on
diabetic nephropathy. Xin Zhong Yi. 38:34–35. 2006.(In
Chinese).
|
|
50
|
Cai HY: Clinical observation of treatment
with breviscapin on 30 cases with early diabetic nephropathy. Dang
Dai Yi Xue. 15:1482009.(In Chinese).
|
|
51
|
Tabák AG, Herder C, Rathmann W, Brunner EJ
and Kivimäki M: Prediabetes: a high-risk state for diabetes
development. Lancet. 379:2279–2290. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Higgins GC and Coughlan MT: Mitochondrial
dysfunction and mitophagy: The beginning and end to diabetic
nephropathy? Br J Pharmacol. 171:1917–1942. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Stanton RC: Clinical challenges in
diagnosis and management of diabetic kidney disease. Am J Kidney
Dis. 63(2 Suppl 2): S3–S21. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Badal SS and Danesh FR: New insights into
molecular mechanisms of diabetic kidney disease. Am J Kidney Dis.
63(2 Suppl 2): S63–S83. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Mima A: Inflammation and oxidative stress
in diabetic nephropathy: New insights on its inhibition as new
therapeutic targets. J Diabetes Res. 2013:2485632013. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Xu XX, Zhang W, Zhang P, Qi XM, Wu YG and
Shen JJ: Superior renoprotective effects of the combination of
breviscapine with enalapril and its mechanism in diabetic rats.
Phytomedicine. 20:820–827. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Qi XM, Wu GZ, Wu YG, Lin H, Shen JJ and
Lin SY: Renoprotective effect of breviscapine through suppression
of renal macrophage recruitment in streptozotocin-induced diabetic
rats. Nephron Exp Nephrol. 104:e147–e157. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Zhao Y, Yang QP, Xiao H, Zhao C, Liu H and
Song DP: The effect of Erigeron breviscapus on apoptosis and
expression of bax, bcl-2 in kidney of diabetic rats. Zhonghua Tang
Niao Bing Za Zhi. 17:864–867. 2009.(In Chinese).
|
|
59
|
Wagener FA, Dekker D, Berden JH,
Scharstuhl A and van der Vlag J: The role of reactive oxygen
species in apoptosis of the diabetic kidney. Apoptosis.
14:1451–1458. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Chadban S, Howell M, Twigg S, Thomas M,
Jerums G, Cass A, Campbell D, Nicholls K, Tong A, Mangos G, et al:
The CARI guidelines. Assessment of kidney function in type 2
diabetes. Nephrology (Carlton). 15(Suppl1): S146–S161. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Wang SH, Wang L, Zhou Y, Guo YJ, Yuan Y,
Li FF, Huang Y and Xia WQ: Prevalence and control of dyslipidaemia
among diabetic patients with microalbuminuria in a Chinese
hospital. Diab Vasc Dis Res. 10:169–178. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Tomkin GH: Targets for intervention in
dyslipidemia in diabetes. Diabetes Care. 31(Suppl 2): S241–248.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Stadler K, Goldberg IJ and Susztak K: The
evolving understanding of the contribution of lipid metabolism to
diabetic kidney disease. Curr Diab Rep. 15:402015. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Chen HC, Guh JY, Chang JM, Hsieh MC, Shin
SJ and Lai YH: Role of lipid control in diabetic nephropathy.
Kidney Int Suppl. S60–S62. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Chen SC and Tseng CH: Dyslipidemia, kidney
disease and cardiovascular disease in diabetic patients. Rev Diabet
Stud. 10:88–100. 2013. View Article : Google Scholar : PubMed/NCBI
|