Introduction
Lower extremity trauma is a type of common
orthopaedic trauma, and the key of its treatment is for the limb to
be rescued in time. Delayed treatment may lead to loss of limb
function and permanent disability as a result of limb amputation
(1–3). However, overemphasis on the rescue of
injured lower extremity may result in ignorance of the general body
condition, cause adverse outcomes, and induce severe complications
that are unfavorable for prognosis (4). Therefore, scientific judgment of the
severity and prognosis of lower extremity trauma should be given
high attention, and it is imperative in the study of orthopaedic
trauma.
Previous findings have shown that more serious lower
extremity trauma may lead to an increased incidence of
complication, infection, and organ dysfunction syndrome and be life
threatening (5,6). Indicators of C-reactive protein (CRP),
interleukin-10 (IL-10), phospholipase A2 (PLA2) and fibrinogen β
polypeptide chain gene (Fbg) are critical inflammatory factors or
important enzymes of inflammatory response. Investigations on how
these indicators are used for predicting progression of lower
extremity trauma have been previously conducted (7–9).
The present study focused on the predictive value of
indicators mentioned above to determine the progression of lower
extremity trauma and is expected to provide theoretical reference
for the treatment of lower extremity trauma.
Subjects and methods
General data
In total, 90 cases of lower extremity trauma were
admitted to the Wuhan Pu'ai Hospital (Hubei, China) from January,
2015 to December, 2015, and served as the study group. The study
group comprised 58 men and 42 women, with an age range of 37–76
years, and an average age of 45.4±2.3 years; ISS grading of 12–18,
averaging, 14.6±1.5; 0.5–5 h of clinical treatment after injury,
averaging, 3.14±0.6 h; factors leading to trauma including traffic
injuries (50 cases), falling injuries (34 cases), and others (6
cases); fracture types including femoral neck fractures (33 cases),
intertrochanteric fractures (25 cases), femoral upper-part
fractures (20 cases), and acetabular fractures (12 cases). The
subjects had no diseases related to heart, kidney and other major
organs, or orthopaedic surgery contraindications and history of
mental disorder. Fifty subjects presenting for physical examination
during the same period were selected as the normal control group.
The normal control group comprised 26 men and 24 women, with an age
range of 38–75 years and an average age of 46.1±2.6 years.
Treatment methods
After confirmed diagnosis, the study group underwent
control of original trauma, early anti-shock treatment, protection
of major organs, and support of gastrointestinal and parenteral
nutrition. Acid-base imbalance and electrolyte disturbances were
corrected and antibiotics were applied to prevent infection of
patients. The study group was then treated with emergency surgery
or damage control technologies.
Testing methods
Level changes of CRP, IL-10, PLA2 and Fbg in serum
prior to surgery and 24 h, and 5 and 7 days thereafter were closely
monitored. IV fluids (4 ml) were collected at the abovementioned
time-points, and applied for hypothermal differential
centrifugation. Serum was kept for testing. ELISA was used to
detect the CRP level [detection kits provided by Xinran Biological
Technology Co., Ltd. (Shanghai, China)]; IL-10 concentration
[detection kits provided by Shanghai Wanjiang Biotech Co.
(Shanghai, China)]; PLA2 level [detection kits provided by Shanghai
Jining Biological Research Co. (Shanghai, China)]; and the Fbg
level [detection kits of Fbg were provided by Beijing Bai'aoLaiBo
Technology Co. (Beijing, China)]. All the detection kits were used
according to the manufacturer's instructions.
Receiver operating characteristic
(ROC) curve
ROC curve was used to detect the accuracy of Fbg in
the prognosis of patients with traumatic fracture of lower limb.
The area under the ROC curve was used as a summary index for the
ROC curve. Ther ROC graph was generated using SPSS 20.0 statistical
software (SPSS, Inc., Chicago, IL, USA).
Statistical analysis
SPSS 20.0 statistical software was used for
statistical analysis. The t-test and Pearson linear correlation
analysis were carried out. P<0.05 was considered to indicate a
statistically significant difference.
Results
Comparison of CRP, IL-1, PLA2 and Fbg
of the two groups
Preoperative levels of CRP, IL-1, PLA2 and Fbg were
markedly higher than those of the normal control group (P<0.01)
(Table I).
 | Table I.Comparison of CRP, IL-1, PLA2 and Fbg
of the two groups. |
Table I.
Comparison of CRP, IL-1, PLA2 and Fbg
of the two groups.
| Groups | CRP (mg/l) | IL-10 (µg/l) | PLA2 (pg/l) | Fbg (g/l) |
|---|
| Research |
43.32±5.41a |
1.92±0.15a |
177.85±13.72a |
3.72±0.35a |
| Control | 4.54±0.33 | 0.95±0.06 | 71.76±6.62 | 2.34±0.21 |
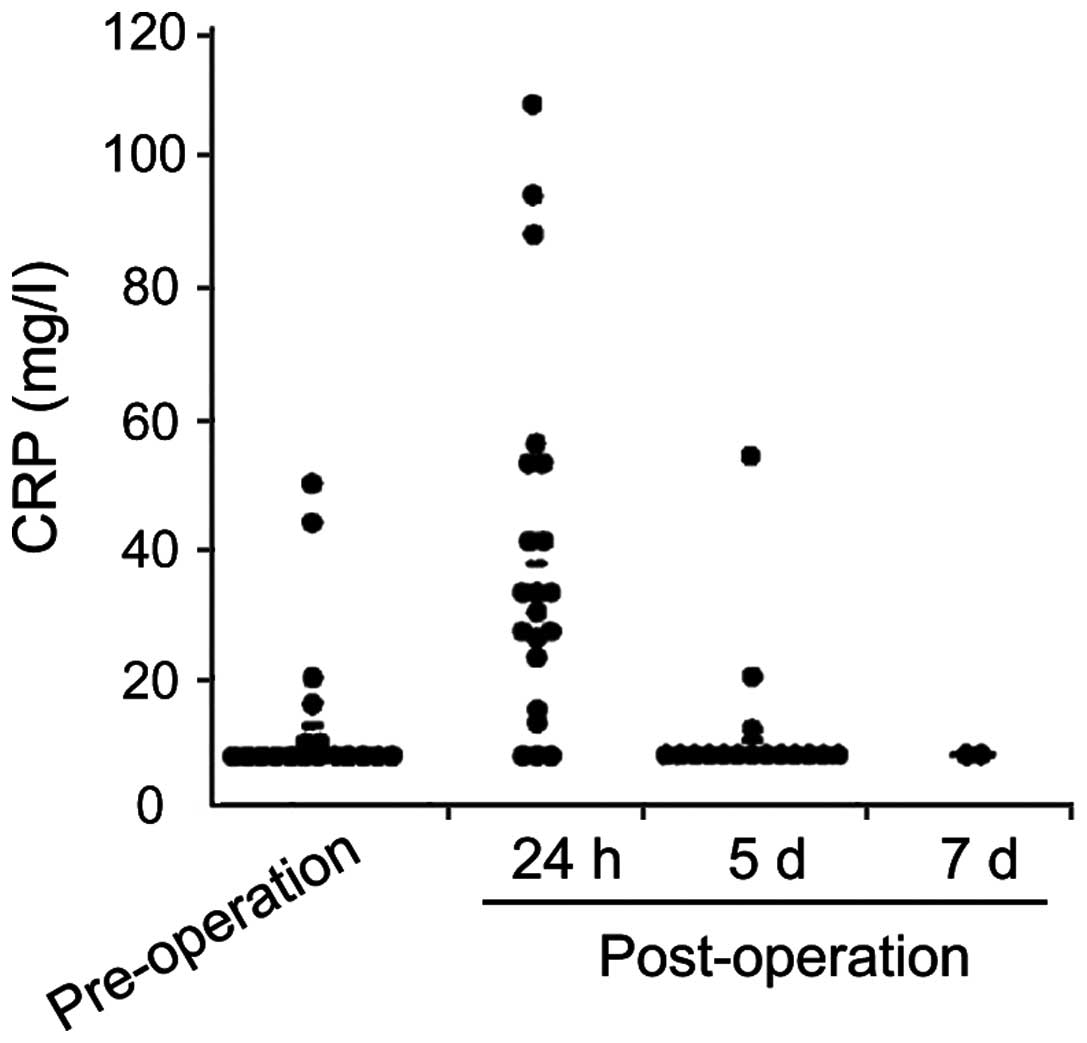
Dynamic changes of CRP at different
time-points
Ninety lower extremity trauma patients were treated
successfully via surgery and their conditions were effectively
controlled. Trauma patients were found with emergent CRP synthesis
24 h after surgery and the CRP concentration gradually decreased
with the control and healing of trauma (Fig. 1).
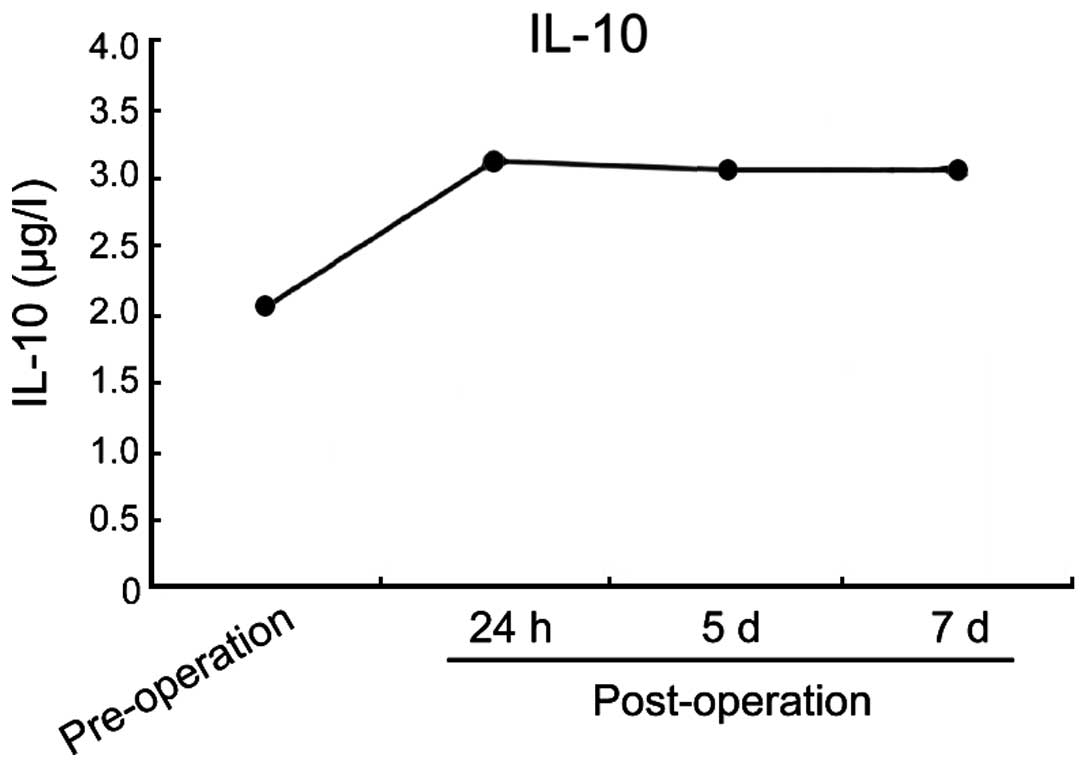
Dynamic changes of IL-10 at different
time-points
IL-10 level of trauma patients was increased during
the first 24 h after operation and then gradually decreased
(Fig. 2).
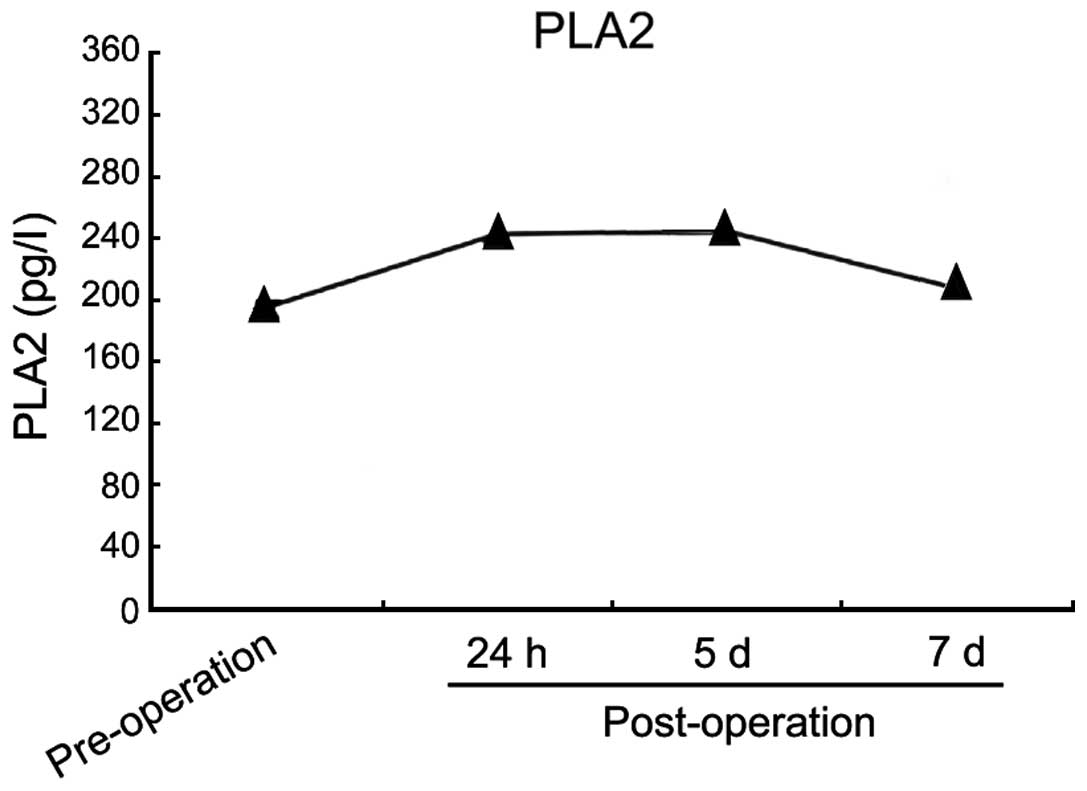
Dynamic changes of PLA2 at different
time-points
PLA2 level of trauma patients was increased before
operation and during the first 24 h after operation, and then
gradually decreased (Fig. 3).
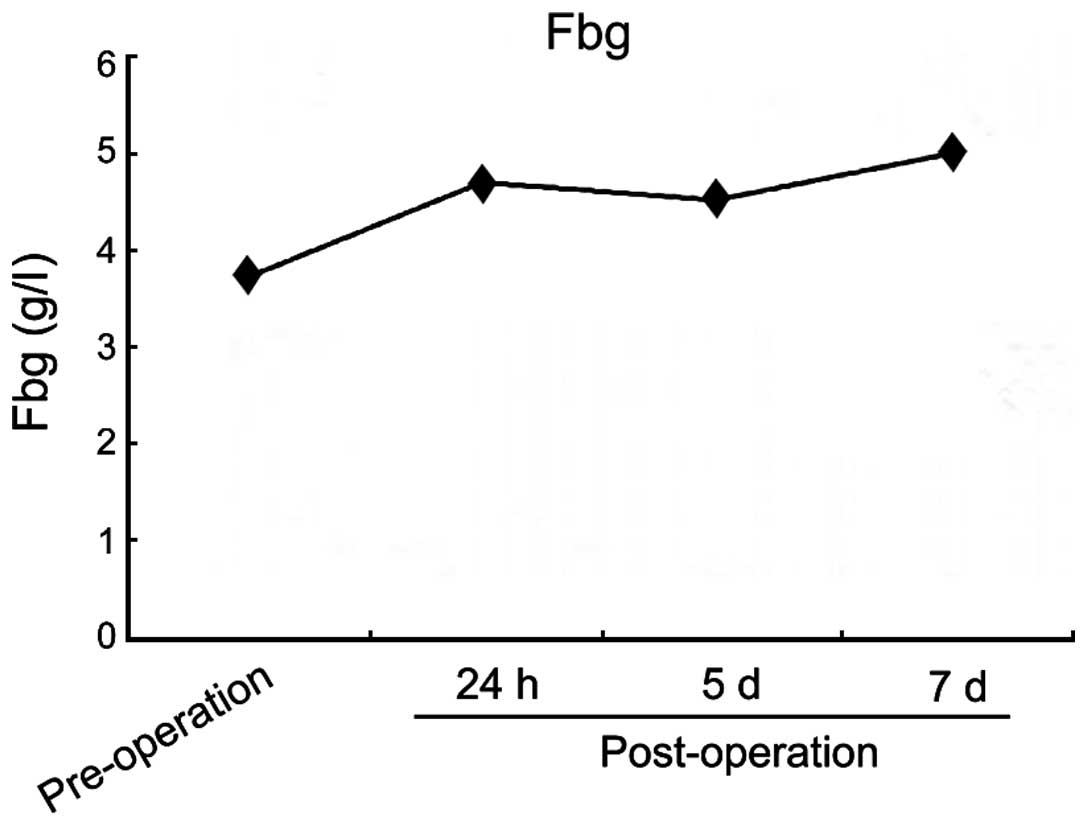
Dynamic changes of Fbg at different
time-points
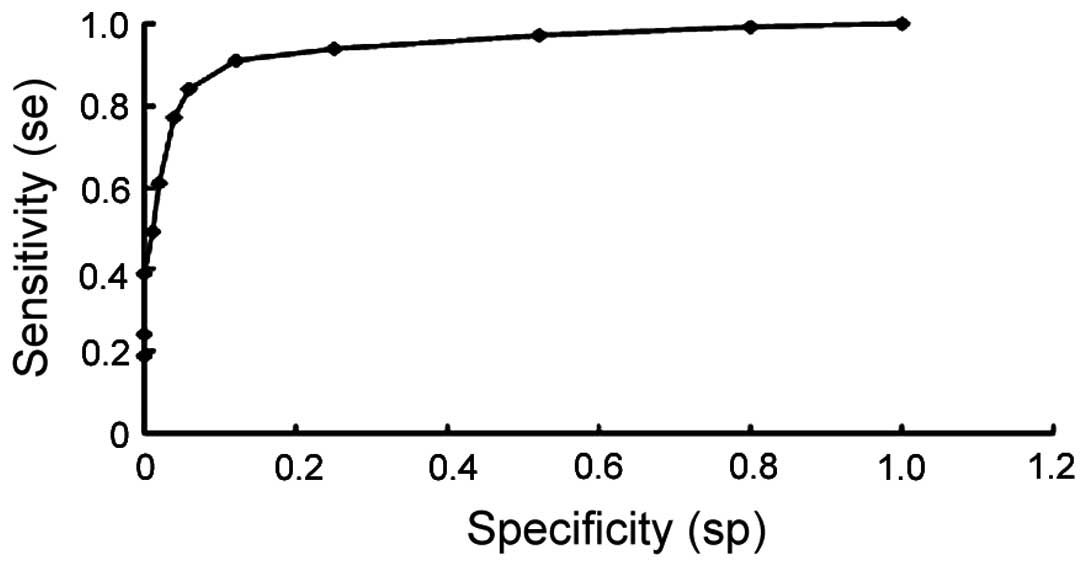
The Fbg level of trauma patients was increased
before operation and during the first 24 h after operation. The Fbg
level gradually decreased and finally gradually increased again
(Fig. 4). The ROC curve showed that
the forming sensitivity and specificity of DVT was determined by
separate observation of Fbg when Fbg >4.71 g/l was defined as
100 and 22.58%, respectively (Fig.
5).
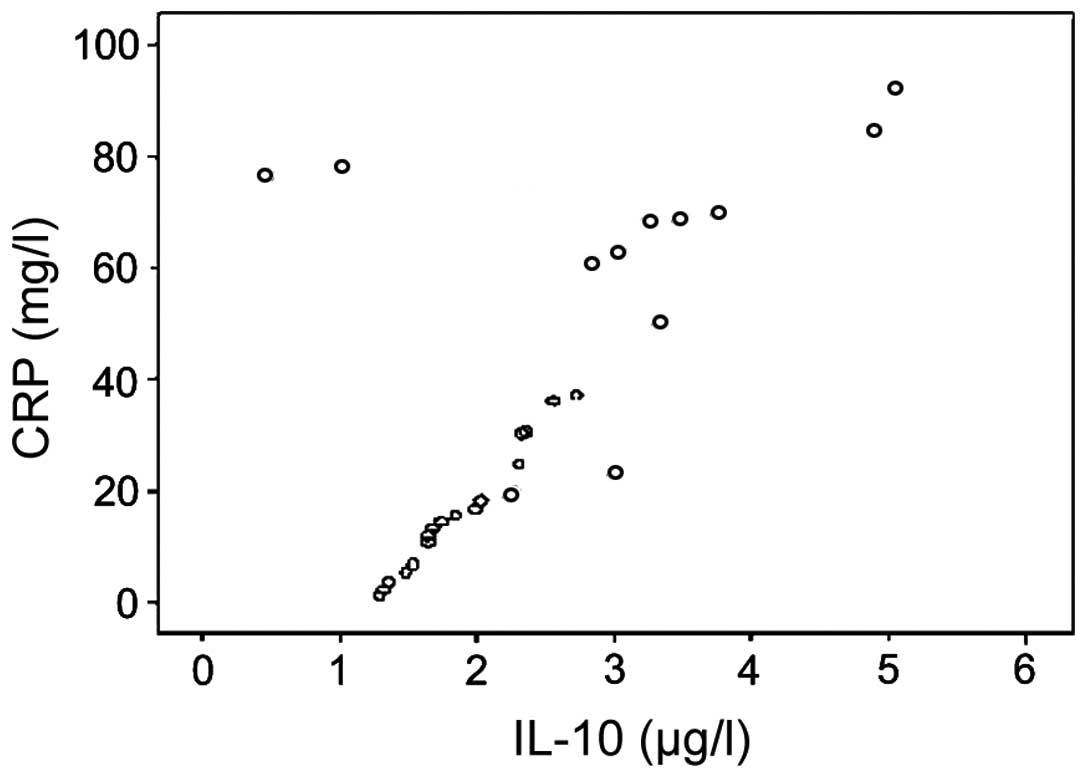
Corrective analysis of some
indicators
CRP levels in serum of trauma patients were
positively correlated with the IL-10 level (r=0.634, P<0.05)
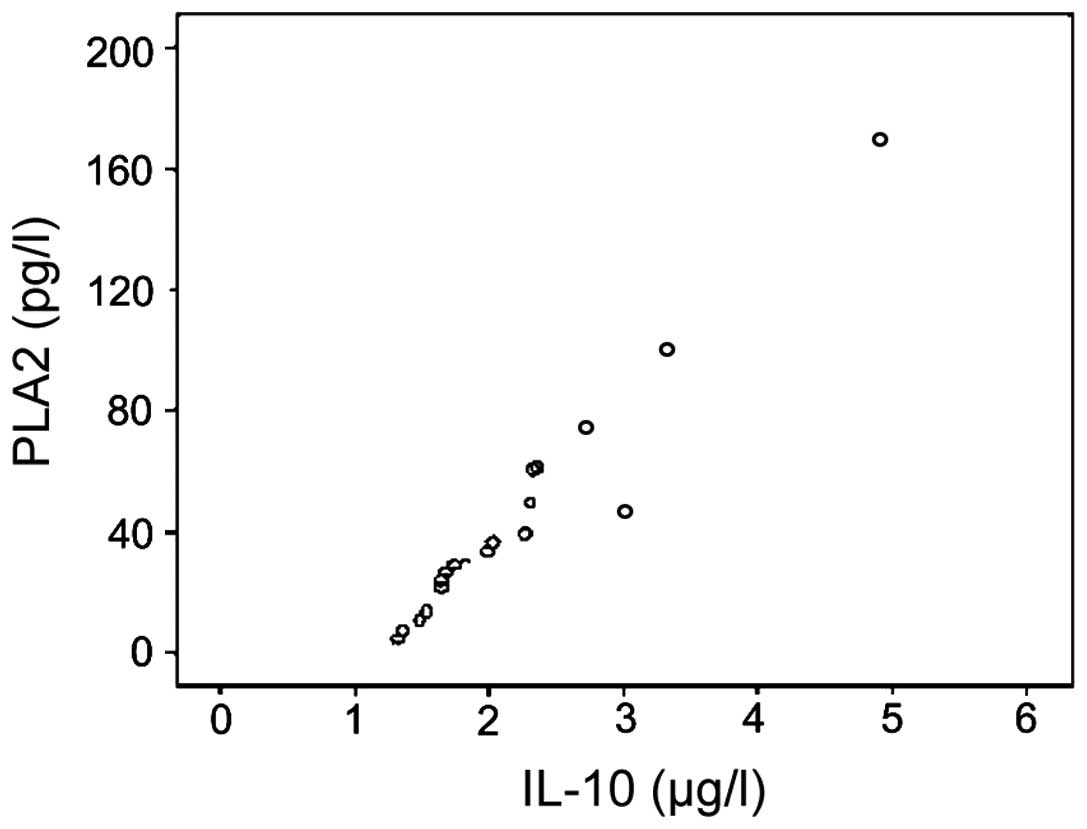
(Fig. 6). PLA2 levels in the serum
of trauma patients were positively correlated with that of the
IL-10 level (r=0.617, P<0.05) (Fig.
7).
Discussion
CRP is a sensitive and non-specific inflammatory
marker of infection or traumas of human beings (10–12).
Previous findings have shown that the CRP concentration in patients
suffering bacterial infection is closely related to their trauma
progression (13–15). If patients are successfully treated
or their status improves, their CRP level is also reduced to normal
level from high concentration. The present study has traced the
level change of CRP in patients with lower extremity trauma and
found that the peak level of CRP is evident 24 h after the
operation as a result of emergency reaction. The CRP level was then
decreased as the trauma became controlled and healed. However, if
the patient CRP level continued to increase after operation,
patients suffered complicated infection (16), and were given high attention.
Patients with lower extremity trauma in the present study were
successfully treated via surgery and no case of infection was
observed. Therefore, an increase of CRP level was not observed
after operation.
IL-10 is a newly found cytokine produced by Th2
cells. Previous studies have identified that IL-10 is closely
related to infection after trauma (17–19).
When the IL-10 level of trauma patients was increased, the
incidence of complication and mortality also increased. However,
few studies are available regarding the early change of level of
IL-10 in serum of patients with lower extremity trauma (19). Our data showed that the level of
IL-10 prior to surgery and during the 24 h after operation was
increased and then decreased, suggesting that patients with lower
extremity trauma were treated with relatively successful operations
and their postoperative traumas were effectively controlled. Of
note, IL-10 can be used for the prediction of progression of lower
extremity trauma.
PLA2, an important enzyme, can release lipid
mediator that actively reacts with inflammation, pathological
changes of tissue damage and becomes involved in intra- and
extracellular metabolic regulation (20). Previously, it was shown that,
compared with healthy individuals, patients with acute pancreatitis
and multiple organ failure have a higher concentration of PLA2 in
their serum (21,22). The present study revealed that the
PLA2 level of trauma patients was increased prior to surgery and
during the first 24 h after operation, and then gradually
decreased. Thus, PLA2 is an important indicator in determining the
injury degree of lower extremity trauma.
Fgb has drawn increasing attention for its
application in determining thrombosis (3,23).
Following lower extremity fractures and operations, lower limbs
experienced a higher incidence of DVT as a result of vein injuries
of different degrees. Clinical manifestations of DVT are not
typical at early stages. Therefore, it is difficult to achieve
accurate diagnosis and false-positive and -negative conditions
become evident (24,25). Therefore, early observation and
diagnosis of DVT has become a study hotspot and challenge. The
present study showed that the Fbg level of trauma patients was
increased prior to surgery and during the first 24 h after
operation, and then gradually decreased before gradually increasing
again, suggesting that the incidence of DVT required attention when
the Fbg level gradually increased following surgery. In the present
study, the forming sensitivity and specificity of DVT was
determined by separate observation of Fbg when Fbg >4.71 g/l was
defined as 100 and 22.58%, respectively. Notably, Fgb concentration
increased in the serum of patients with lower extremity trauma and
the change of Fgb index can be used to determine and prevent DVT
formation.
A correlative analysis on some indicators found that
CRP levels in the serum of trauma patients were positively
correlated with the IL-10 level (r=0.634, P<0.05). Additionally,
PLA2 levels in the serum of trauma patients were positively
correlated with the IL-10 level (r=0.617, P<0.05). Therefore,
levels of CRP and PLA2 increase as the level of IL-10 increases in
patients with lower extremity trauma. Furthermore, levels of CRP
and PLA2 decreased as the level of IL-10 decreased in patients with
lower extremity trauma.
In conclusion, detection of the dynamic changes of
levels of CRP, IL-10, PLA2 and Fbg in serum during the clinical
diagnosis and treatment of lower extremity trauma patients may be
useful regarding progression and provide valuable theoretical clues
and a basis for prediction and determining their treatment effect
and prognosis.
References
|
1
|
Azarpira N, Nikeghbalian S, Kazemi K,
Geramizadeh B, Malekpour Z and Malek-Hosseini SA: Association of
increased plasma interleukin-6 and TNF-α levels in donors with the
complication rates in liver transplant recipients. Int J Organ
Transplant Med. 4:9–14. 2013.PubMed/NCBI
|
|
2
|
Mahar P: Lower extremity trauma. Berman's
Pediatric Decision Making (5th). 442–447. 2011. View Article : Google Scholar
|
|
3
|
Mok JM, Pekmezci M, Piper SL, Boyd E,
Berven SH, Burch S, Deviren V, Tay B and Hu SS: Use of C-reactive
protein after spinal surgery: comparison with erythrocyte
sedimentation rate as predictor of early postoperative infectious
complications. Spine. 33:415–421. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Harris AM, Althausen PL, Kellam J, Bosse
MJ and Castillo R: Complications following limb-threatening lower
extremity trauma. J Orthop Trauma. 23:1–6. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gando S: Tissue factor in trauma and organ
dysfunction. Semin Thromb Hemost. 32:48–53. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gando S, Nanzaki S, Morimoto Y, Ishitani T
and Kemmotsu O: Tissue factor pathway inhibitor response does not
correlate with tissue factor-induced disseminated intravascular
coagulation and multiple organ dysfunction syndrome in trauma
patients. Crit Care Med. 29:262–266. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Waydhas C, Nast-Kolb D, Trupka A, Zettl R,
Kick M, Wiesholler J, Schweiberer L and Jochum M: Posttraumatic
inflammatory response, secondary operations, and late multiple
organ failure. J Trauma. 40:624–630. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Giannoudis PV, Smith RM, Perry SL, Windsor
AJ, Dickson RA and Bellamy MC: Immediate IL-10 expression following
major orthopaedic trauma: relationship to anti-inflammatory
response and subsequent development of sepsis. Intensive Care Med.
26:1076–1081. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lindström T, Gullichsen E, Heinonen O,
Grönroos J, Nevalainen T and Niinikoski J: Group II phospholipase
A2 in serum after knee surgery and intramedullary nailing of tibial
shaft fracture. Injury. 28:169–171. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Holtslag HR, van Beeck EF, Lindeman E and
Leenen LP: Determinants of long-term functional consequences after
major trauma. J Trauma. 62:919–927. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Simmel S and Bühren V: Surviving multiple
trauma - what comes next? The rehabilitation of seriously injured
patients. Unfallchirurg. 112:965–974. 2009.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Manly DA, Boles J and Mackman N: Role of
tissue factor in venous thrombosis. Annu Rev Physiol. 73:515–525.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kim JW, Oh CW, Oh JK, Baek SG, Lee BJ,
Hong HP and Min WK: The incidence and the risk factors of venous
thromboembolism in Korean patients with pelvic or acetabular
fractures. J Orthop Sci. 19:471–477. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yi X, Zhu J, Wei M, Li J, Chen J, Wang Y,
Shen E and Hu B: Risk factors of venous thrombosis in patients with
ankle fractures. Int Angiol. 33:324–328. 2014.PubMed/NCBI
|
|
15
|
Mulsow J, O'Toole GC and McManus F:
Traumatic lower limb fractures following complete spinal cord
injury. Ir Med J. 98:141–142. 2005.PubMed/NCBI
|
|
16
|
Peivandi MT, Yusof-Sani MR and Amel-Farzad
H: Exploring the reasons for orthopedic implant failure in
traumatic fractures of the lower limb. Arch Iran Med. 16:478–482.
2013.PubMed/NCBI
|
|
17
|
Cross AM, Davis C, Penn-Barwell J, Taylor
DM, De Mello WF and Matthews JJ: The incidence of pelvic fractures
with traumatic lower limb amputation in modern warfare due to
improvised explosive devices. J R Nav Med Serv. 100:152–156.
2014.PubMed/NCBI
|
|
18
|
Besemann M: Physical rehabilitation
following polytrauma. The canadian forces physical rehabilitation
program 2008–2011. Can J Surg. 54:S135–S141. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Rowley AH and Shulman ST: Recent advances
in the understanding and management of kawasaki disease. Curr
Infect Dis Rep. 12:96–102. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Rowley AH and Shulman ST: New developments
in the search for the etiologic agent of Kawasaki disease. Curr
Opin Pediatr. 19:71–74. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Harris KC and Hosking MC: Persistent fever
in an infant: incomplete Kawasaki disease. CMAJ. 183:2009–2013.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Beken B, Unal S, Cetin M and Gümrük F: The
relationship between hematological findings and coronary artery
aneurysm in kawasaki disease. Turk J Haematol. 31:199–200. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Schalek P, Hornáčková Z and Hahn A: The
relationship of C-reactive protein levels and positive culture with
quality of life in acute rhinosinusitis. Patient Prefer Adherence.
9:185–189. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wallace GF: Rehabilitation after major
extremity trauma. Clin Podiatr Med Surg. 31:585–595. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Inaba K, Siboni S, Resnick S, Zhu J, Wong
MD, Haltmeier T, Benjamin E and Demetriades D: Tourniquet use for
civilian extremity trauma. J Trauma Acute Care Surg. 79:232–237.
2015. View Article : Google Scholar : PubMed/NCBI
|