Introduction
Alveolar ridge atrophy developing after tooth
extraction may result in insufficient bone volume, thus rendering
incorrect implant placement from both functional and esthetic
viewpoints (1). Autogenous onlay
block bone grafts are widely used for external augmentation in
cases of horizontal and vertical alveolar ridge atrophy, as
placement on the surface of the host bone can restore bone volume
(2,3). Furthermore, several reports have noted
that implant treatment with an autogenous onlay block bone graft
for horizontal or vertical alveolar ridge atrophy results in bone
gain and high rates of implant success (3–6).
However, autogenous block bone grafting also has some
disadvantages, such as limited availability of grafts with
sufficient size and shape, and risk of donor site morbidity,
including long-lasting pain, fracture, and nerve damage (7–9). In
addition, other problems associated with resorption of the grafted
bone during the healing process remain.
Interconnected porous hydroxyapatite ceramic
(IP-CHA) materials with high porosity have been developed and used
successfully in the field of orthopedics medicine (10). An IP-CHA block, which consists of a
porous sintered body composed of hydroxyapatite ceramics with a
unique pore structure, is able to undergo extensive incorporation
into host bone more rapidly than conventional porous calcium
hydroxyapatite ceramic (10,11). We speculated that problems associated
with autogenous block bone grafting could be avoided if an IP-CHA
block of the same size as an autogenous block bone were to be used
for onlay grafting. In our previous study, we used titanium
implants in IP-CHA blocks placed on cortical bone surfaces in a
rabbit model, which resulted in direct contact between the implant
surface and new bone incorporated into the block (12). Those results indicated that use of an
IP-CHA block promotes osseointegration of the dental implant from
the surface of the host bone. Here, we present the first report of
clinical application of an IP-CHA block for onlay grafting in
implant treatment in a patient with horizontal alveolar
atrophy.
Case report
The patient was 51-year-old woman, whose left
incisor had been extracted at a primary care dental clinic because
of caries. Six months later, she was referred to our hospital for
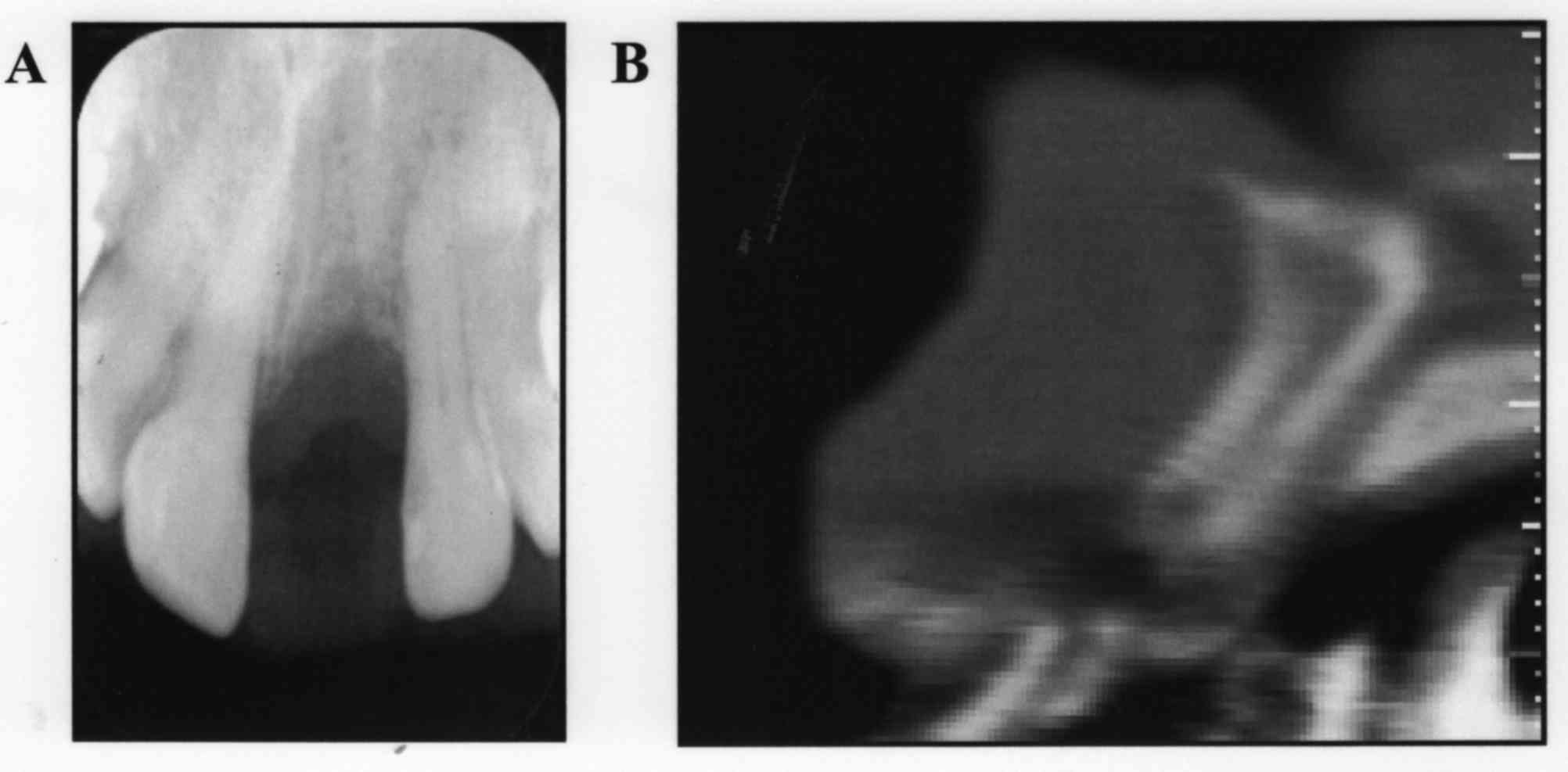
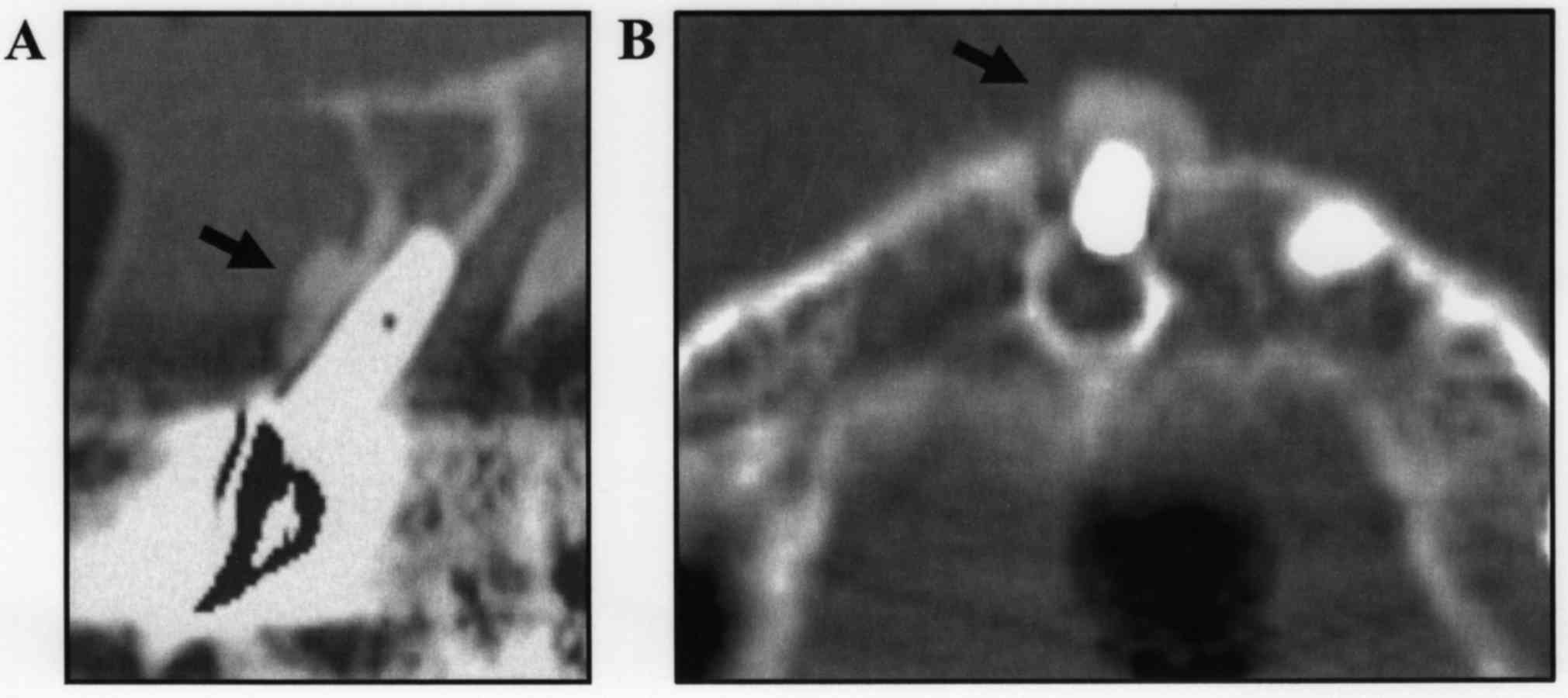
consideration of implant treatment for the missing tooth (Fig. 1). Orthopantomograph and computed
tomography (CT) images showed horizontal alveolar bone atrophy in
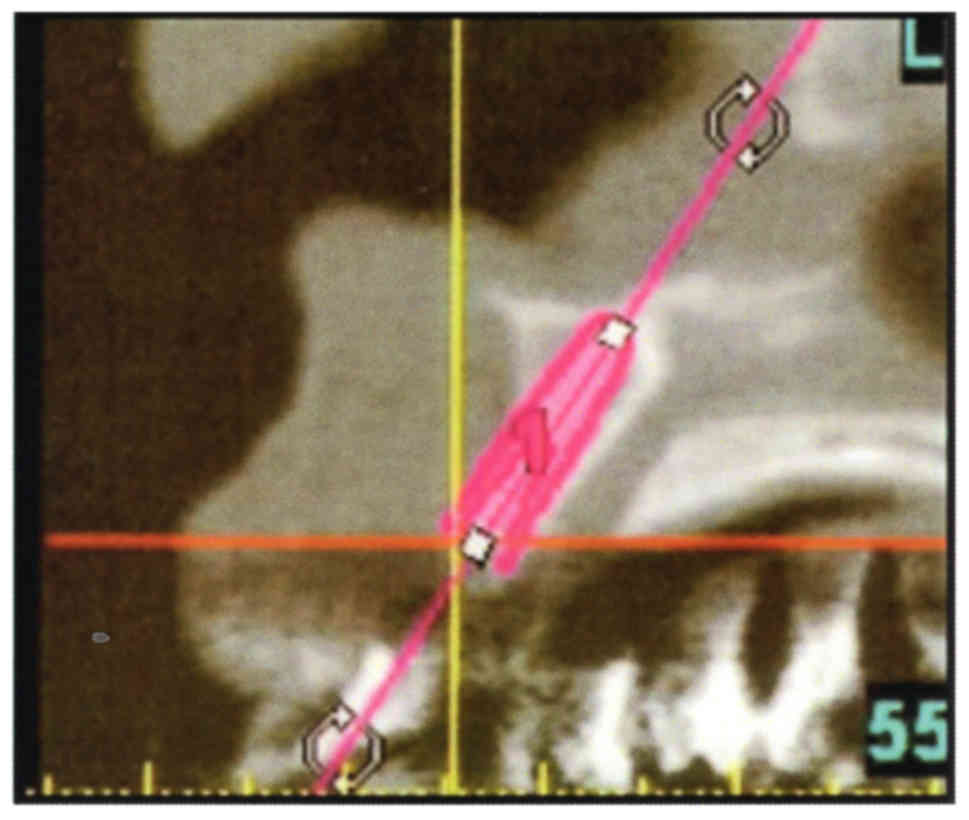
the anterior region (Fig. 2). Data
obtained from the examinations were then transferred to 3D planning
software (SimPlant; Materialise Dental NV, Leuven, Belgium) for
ideal implant placement (Fig. 3),
and those findings showed that the implant thread would be exposed
because of the insufficient bone volume in the alveolar ridge.
Therefore, we planned to use of an onlay graft with an IP-CHA block
to restore bone volume for implant placement in the alveolar ridge
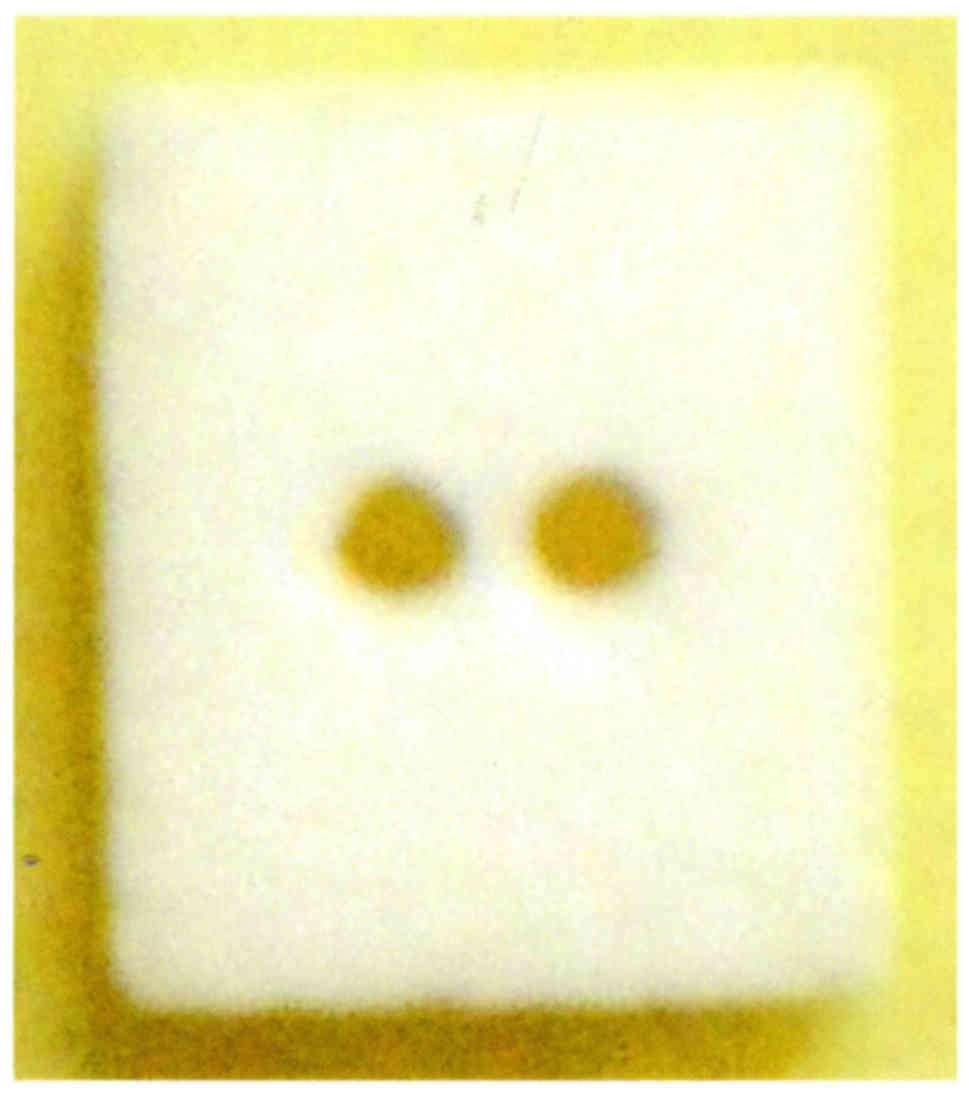
area without collecting autogenous block. The virtual planning data
were then utilized to create a 3D model by a rapid prototyping
machine (Eden 260; Objet Geometries Inc., Rehovot, Israel). An
IP-CHA block was fabricated (6×7×3 mm in size) by MMT. Co., Ltd.,
Osaka, Japan, to fit the alveolar ridge of the patient (Fig. 4).
The patient underwent informed consent according to
a protocol approved by the Ethical Committee of Hiroshima
University Hospital, and onlay grafts and implant placement were
performed under general anesthesia in October 2011. A crestal
incision and 2 vertical releasing incisions were made, after which
the soft tissue flap was raised, and the cortical bone surface was
polished using a small round bur to support blood vessel outgrowth.
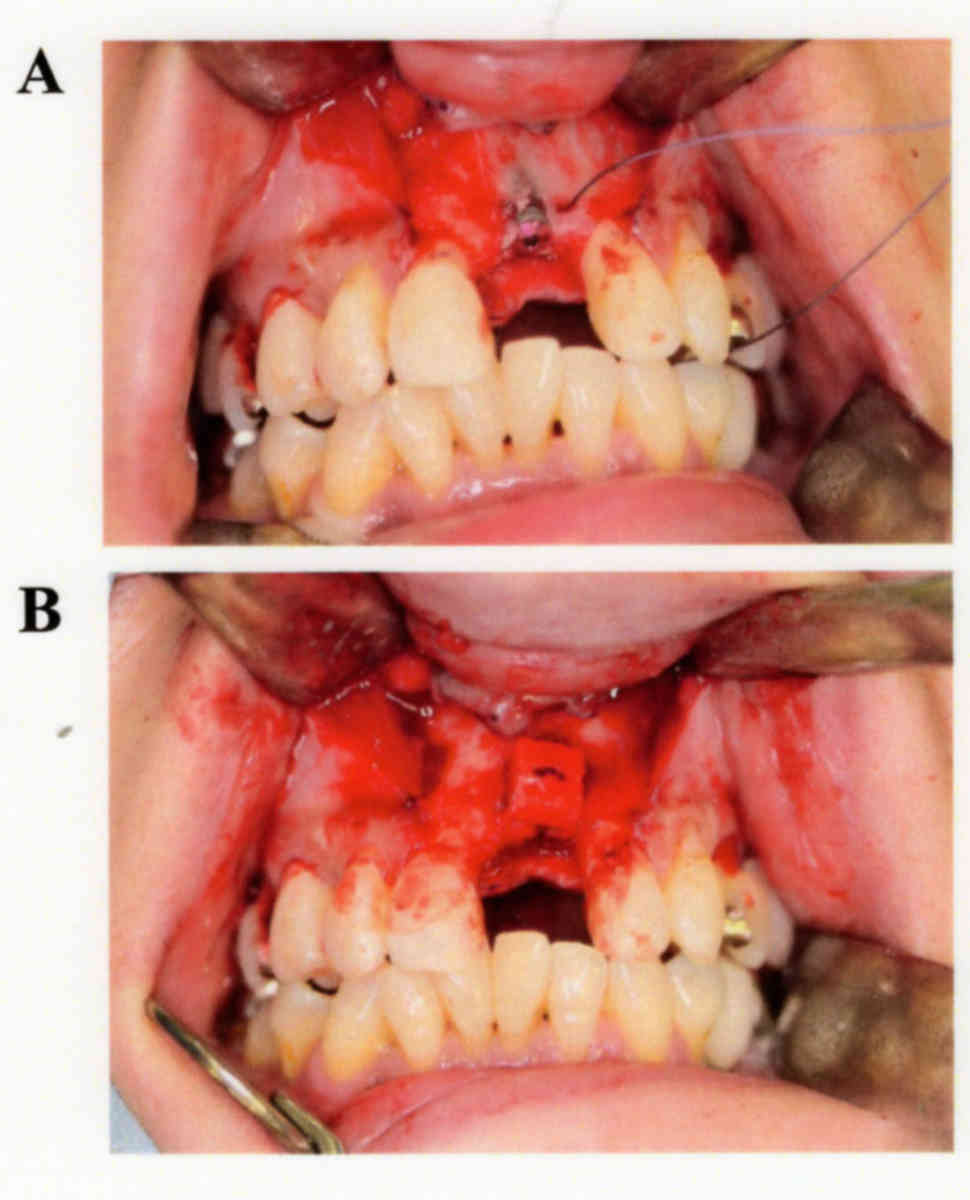
An implant (Replace Tapered groovy NP 3.5×10 mm; Nobel Biocare,
Gottenborg, Sweden) was installed into alveolar bone according to
the manufacturer's instructions, and the thread remained exposed,
as expected (Fig. 5A). Next, 2 small
holes for the suture were opened through labial and palate cortical
bone on both sides of the thread using a small round bur, with CT
imaging employed to avoid injury to the incisive canal, then an
absorbable suture was passed through in the labial and palate
alveolar ridge via these holes. The IP-CHA block was placed over
the exposed thread and fixed to the alveolar ridge with an
absorbable suture (Ethicon, Inc., Somerville, NJ, USA) (Fig. 5B). Another incision was made through
the periosteum at the base of the flap, thus allowing the tissue to
cover the graft without tension, and the flap was sutured. Six
months after the procedure, we performed a second operation for
abutment connection. Using the same incision as before,
subperiosteal dissection of the alveolar bone was performed under
local anesthesia. At that time, we observed that the IP-CHA block
had become stabilized on the host bone, and no abnormal resorption
was found. The ISQ value for the implant obtained at the second
operation was found to be increased to 64.6±0.58 as compared to
that at the first operation (58.6±0.58). Finally, a healing
abutment was exposed above the gingival tissue, and the flap was
then sutured. No complications, including infection, abnormal pain
and hypoethesia, were observed following surgery.
At 16 months after implant placement with the onlay
graft, CT scanning showed that the IP-CHA block had stabilized
without abnormal resorption and no problems with the implant were
revealed (Fig. 6), thus the final
superstructure was placed (Fig. 7).
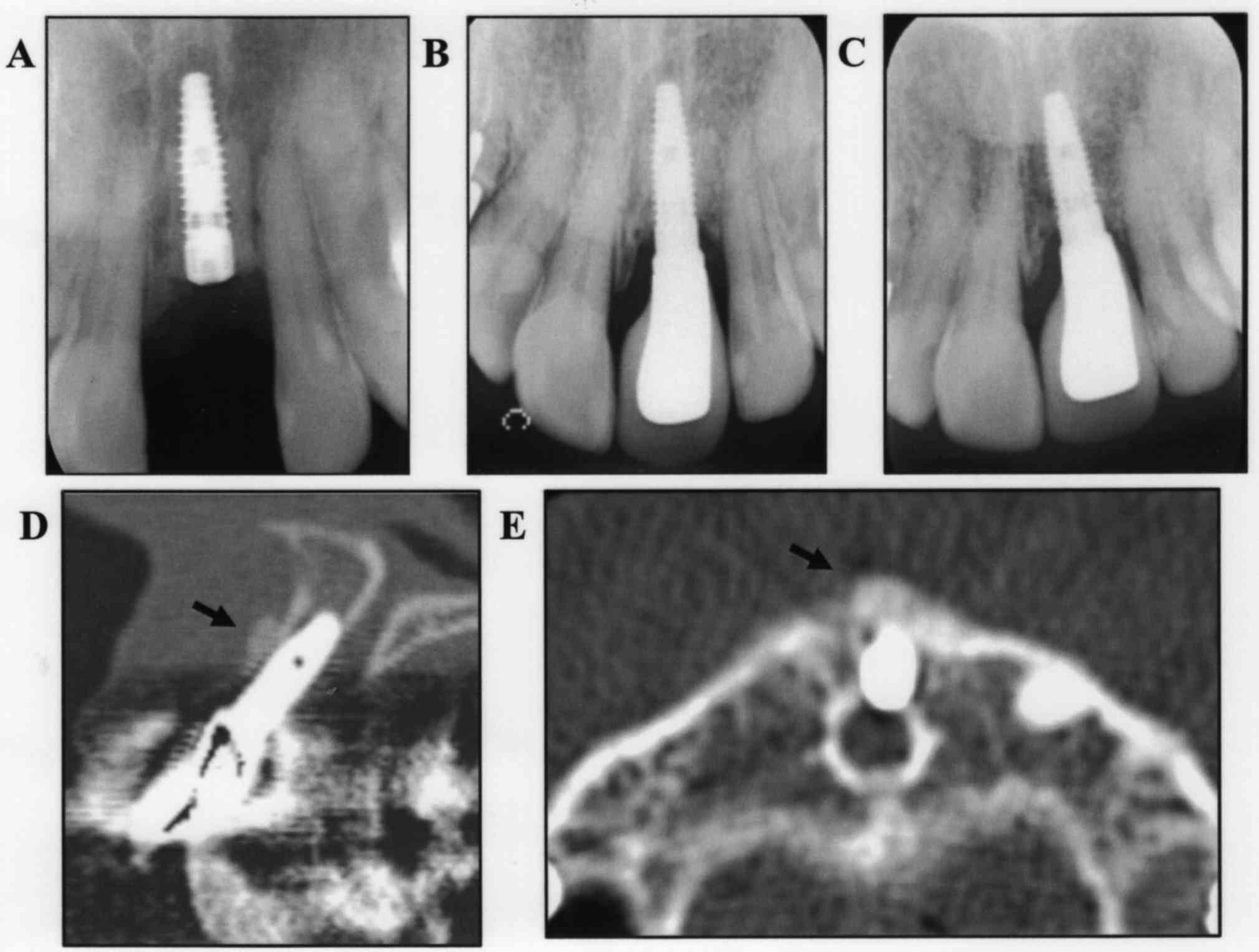
Dental X-ray findings showed that the border of the IP-CHA block
had become increasingly vague over the 3-years period (Fig. 8A-C). CT scan images obtained at 3
years 5 months after onlay grafting showed the IP-CHA block on the
alveolar bone, with a smooth transition in the gap between the
block and bone, indicating that use of IP-CHA improved the process
of integration with host bone (Fig. 8D
and E). In the follow-up examinations conducted over 5 years,
the implants and superstructures have had no problems.
Discussion
Onlay block bone grafts are used for external
augmentation of horizontal or vertical alveolar ridge atrophy, with
autogenous bone harvested from the mandibular ramus or symphysis
used for the graft, as those locations offer the greatest bone
volume (13). However, intraoral
grafts have been reported to have various drawbacks, such as need
for an additional surgical procedure to procure the bone graft
material, increased operative time, graft bone limitations,
post-operative pain, altered sensation in mandibular teeth,
neurosensory disturbances, nerve paresthesia, and mandibular
fracture (8,14). In addition, an autogenous bone block
usually undergoes extensive resorption during healing (15), which may result in implant failure
from osseointegration loss leading to reduced bone-to-implant
contact and an unfavorable outcome.
Hydroxyapatite ceramics (HA) materials have been
used as a substitute for bone grafting because the crystalline
phase of natural bone is similar to that of HA (16,17),
while porous calcium hydroxyapatite ceramics (CHA) materials have
been utilized in orthopedic and craniofacial surgery procedures
since the 1980s (18). However, few
studies have reported cases in which conventional CHA became fully
filled by newly formed bone, which may be due to its structure and
limited connectivity between pores (19). IP-CHA consists of a porous sintered
body made of hydroxyapatite ceramics with a unique pore structure,
in which the pores are fully interconnected, likely allowing
ingrowth of osteoblasts (20,21).
Tamai et al (20) implanted
cylindrical blocks made of IP-CHA into femoral condyles of rabbits,
and observed mature bone ingrowth in most of the pores within 6
months. IP-CHA has adequate compression strength (10–12 MPa),
similar to that of cancellous bone, and was shown to have IP-CHA
increased compression strength up to 9 weeks after implantation,
reaching approximately 30 MPa (20).
It has also been reported that IP-CHA did not show active
resorption in clinical applications (10). Since an IP-CHA block can be
prefabricated into a specific size and shape to match the alveolar
ridge of the patient, application as a substitute autogenous block
bone graft for onlay grafting is possible. In the present study, we
used an IP-CHA block to overcome disadvantages normally associated
with an autogenous bone graft and obtained good results.
Recently, Doi et al (22) reported successful use of IP-CHA as a
grafting material for implant treatment in vivo. They
examined the effects on bone regeneration of an implant/IP-CHA
complex placed directly into femur sockets of dogs as well as
implant stability, and found no significant differences in regard
to bone implant contact and ISQ values between the complex and
control groups at 3–6 months after surgery. In our previous in
vivo study, to examine whether an IP-CHA block could be applied
as an onlay graft substitute, titanium implants were inserted into
IP-CHA blocks placed on the cortical bone surface of the mandibular
in rabbits. We observed high levels of new bone formation from the
host bone in the pores of the IP-CHA as well as significantly
increased ISQ values at 12 weeks after surgery (12). In the present case, the IP-CHA block
became stabilized on the host bone, and no abnormal resorption was
observed during a second operation performed 6 months after the
initial operation. In addition, the ISQ value was increased as
compared with that at the first operation. Together, these results
show that an IP-CHA block can promote osseoconduction from the
surface of the host bone and periosteum, leading to
osseointegration of the implant in host bone tissue.
Clinically, IP-CHA is widely used in the field of
orthopedic surgery (10). Yoshikawa
et al (10) and Shi et
al (23) applied IP-CHA granules
or blocks as bone substitute for treatment of 59 patients with
benign bone tumors and 12 with cystic lesions associated with
rheumatoid arthritis, and reported that none of those patients
showed any signs of inflammatory reaction, rejection, or infection,
nor abnormal results in blood tests. More recently, IP-CHA has been
used as an autogenous bone graft substitute in oral and
maxillofacial surgery cases (24).
We previously reported implant treatment and maxillary sinus floor
augmentation performed with a granular type of IP-CHA in a female
patient, and those results showed a sufficient amount of
osseointegration in the implant fixture, while histological
analysis indicated that IP-CHA granules have strong potential to
induce bone growth (24). In that
case, we collected an autogenous bone block (10×8 mm) from the
maxillary tuberosity to prepare a graft comprised of a mixture of
IP-CHA and cortical bone (Table I).
We have also previously reported a clinical case of horizontal
alveolar ridge atrophy following resection of a maxillary bone
cyst, in which autogenous onlay bone grafting with IP-CHA granules
was successfully used for prosthetic treatment (25). In that case, an autogenous block bone
(10×15 mm) was collected from the mandibular ramus, and a granular
type of IP-CHA was applied to fill gaps between an autogenous bone
block and host bone in order to restore bone volume (Table I). When a granular type of IP-CHA is
applied as a substitute for bone augmentation, a residual bone wall
or additional materials, such as titanium mesh, are needed to
ensure space maintenance of the granules. For the present case, we
used an IP-CHA block for onlay grafting in implant treatment
without autogenous block bone grafting (Table I). At a follow-up examination
performed 3 years 5 month after initial placement, the IP-CHA block
could be observed on the alveolar bone, and the gap between it and
the host bone showed a smooth transition, suggesting that IP-CHA
improves integration with newly-formed bone tissue. At more than 5
years after the initial surgery, the implant and superstructure
continued to show no problems. Application of an IP-CHA block can
overcome disadvantages associated with autogenous bone block
grafting, thus we consider it to be useful as a substitute for
block bone grafting in patients undergoing implant treatment.
 | Table I.Reported applications of IP-CHA in
oral and maxillofacial surgery cases. |
Table I.
Reported applications of IP-CHA in
oral and maxillofacial surgery cases.
| A, |
|---|
|
|---|
| Case | Age (yrs) | Gender | Site | Region | Grafting method | Autogenous block bone
graft |
|---|
| 1 | 59 | Female | Maxilla | Premolar and
molar | Sinus floor
augmentation | Cortical bone block
(10×8 mm) from maxillary tuberosity |
| 2 | 51 | Male | Maxilla | Incisor | Onlay block bone
grafting | Cortical bone block
(10×15 mm) from mandibular ramus |
| 3 | 51 | Female | Maxilla | Incisor | Onlay block bone
grafting | None |
|
| B, |
|
| Type of
IP-CHA | Implant treatment
(diameter × length mm) | (Refs.) |
|
| Granular type (1–2
mm) | 3 implants placed
(4.3×10, 4.3×13, 5.0×13) | (24) |
| Granular type (1–2
mm) | None | (25) |
| Block type (6×7×3
mm) | 1 implant placed
(4.3×10) | Present case |
Acknowledgements
We express our deep appreciation for the late
Professor Nobuyuki Kamata (Hiroshima University, Japan) for the
excellent guidance regarding this case.
References
|
1
|
Chiapasco M, Zaniboni M and Boisco M:
Augmentation procedures for the rehabilitation of deficient
edentulous ridges with oral implants. Clin Oral Implant Res. 17
Suppl 2:S136–S159. 2006. View Article : Google Scholar
|
|
2
|
Pikos MA: Block autografts for localized
ridge augmentation: Part I. The posterior maxilla. Implant Dent.
8:279–285. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Esposito M, Grusovin MG, Felice P,
Karatzopoulos G, Worthington HV and Coulthard P: The efficacy of
horizontal and vertical bone augmentation procedures for dental
implants-a Cochrane systematic review. Eur J Oral Implantol.
2:167–184. 2009.PubMed/NCBI
|
|
4
|
Clementini M, Morlupi A, Agrestini C and
Ottria L: Success rate of dental implants inserted in autologous
bone graft regenerated areas: A systematic review. Oral Implantol
(Rome). 4:3–10. 2012.
|
|
5
|
Donos N, Mardas N and Chadha V: Clinical
outcomes of implantsfollowing lateral bone augmentation: Systematic
assessment of available options (barrier membranes, bone grafts,
split osteotomy). J Clin Periodontol. 35 8 Suppl:S173–S202. 2008.
View Article : Google Scholar
|
|
6
|
Kuchler U and von Arx T: Horizontal ridge
augmentation in conjunction with or prior to implant placement in
the anterior maxilla: A systematic review. Int J Oral Maxillofac
Implants. 29 Suppl:S14–S24. 2014. View Article : Google Scholar
|
|
7
|
Misch CM: Comparison of intraoral donor
sites for onlay grafting prior to implant placement. Int J Oral
Maxillofac Implants. 12:767–776. 1997.PubMed/NCBI
|
|
8
|
Stubinger S, Nuss K, Landes C, von
Rechenberg B and Sader R: Harvesting of intraoral autogenous block
grafts from the chin and ramus region: Preliminary results with a
variable square pulse Er: YAG laser. Lasers Surg Med. 40:312–318.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Banwart JC, Asher MA and Hassanein RS:
Iliac crest bone graft harvest donor site morbidity. A statistical
evaluation. Spine (Phila Pa 1976). 20:1055–1060. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yoshikawa H, Tamai N, Murase T and Myoui
A: Interconnected porous hydroxyapatite ceramics for bone tissue
engineering. J R Soc Interface. 6 Suppl 3:S341–S348. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yoshikawa H and Myoui A: Bone tissue
engineering with porous hydroxyapatite ceramics. J Artif Organs.
8:131–136. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Minami M, Takechi M, Ohta K, Ohta A,
Ninomiya Y, Takamoto M, Fukui A, Tada M and Kamata N: Bone
formation and osseointegration with titanium implant using
granular- and block-type porous hydroxyapatite ceramics (IP-CHA).
Dent Mater J. 32:753–760. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Misch CM: Comparison of intraoral donor
sites for onlay grafting prior to implant placement. Int J Oral
Maxillofac Implant. 12:767–776. 1997.
|
|
14
|
Pourabbas R and Nezafati S: Clinical
results of localized alveolar ridge augmentation with bone grafts
harvested from symphysis in comparison with ramus. J Dent Res Dent
Clin Dent Prospect. 1:7–12. 2007.
|
|
15
|
Stellingsma C, Vissink A, Meijer HJ,
Kuiper C and Raghoebar GM and Raghoebar GM: Implantology and the
severely resorbed edentulous mandible. Crit Rev Oral Biol Med.
15:240–248. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bucholz RW, Carlton A and Holmes R:
Interporous hydroxyapatite as a bone graft substitute in tibial
plateau fractures. Clin Orthop Relat Res. 53–62. 1989.PubMed/NCBI
|
|
17
|
Holmes RE, Bucholz RW and Mooney V: Porous
hydroxyapatite as a bone graft substitute in diaphyseal defects: A
histometric study. J Orthop Res. 5:114–121. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Uchida A, Araki N, Shinto Y, Yoshikawa H,
Kurisaki E and Ono K: The use of calcium hydroxyapatite ceramic in
bone tumour surgery. J Bone Joint Surg Br. 72:298–302.
1990.PubMed/NCBI
|
|
19
|
Ayers RA, Simske SJ, Nunes CR and Wolford
LM: Long-term bone ingrowth and residual micro hardness of porous
block hydroxyapatite implants in humans. J Oral Maxillofac Surg.
56:1297–1302. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tamai N, Myoui A, Tomita T, Nakase T,
Tanaka J, Ochi T and Yoshikawa H: Novel hydroxyapatite ceramics
with an interconnective porous structure exhibit superior
osteoconduction in vivo. J Biomed Mater Res. 59:110–117. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tamai N, Myoui A, Kudawara I, Ueda T and
Yoshikawa H: Novel fully interconnected porous hydroxyapatite
ceramic in surgical treatment of benign bone tumor. J Orthop Sci.
15:560–568. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Doi K, Oue H, Morita K, Kajihara S, Kubo
T, Koretake K, Perrotti V, Lezzi G, Piattelli A and Akagawa Y:
Development of implant/interconnected porous hydroxyapatite complex
as new concept graft material. PLoS One. 7:e490512012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Shi K, Hayashida K, Hashimoto J, Sugamoto
K, Kawai H and Yoshikawa H: Hydroxyapatite augmentation for bone
atrophy in total ankle replacement in rheumatoid arthritis. J Foot
Ankle Surg. 45:316–321. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Shigeishi H, Takechi M, Nishimura M,
Takamoto M, Minami M, Ohta K and Kamata N: Clinical evaluation of
novel interconnected porous hydroxyapatite ceramics (IP-CHA) in a
maxillary sinus floor augmentation procedure. Dent Mater J.
21:54–60. 2012. View Article : Google Scholar
|
|
25
|
Kubozono K, Takechi M, Ohta K, Ono S,
Nakagawa T, Fujimoto S and Kamata N: Aesthetic recovery of alveolar
atrophy following autogenous onlay bone grafting using
interconnected porous hydroxyapatite ceramics (IP-CHA) and
resorbable poly-L-lactic/polyglycolic acid screws: Case report. BMC
Oral Health. 14:602014. View Article : Google Scholar : PubMed/NCBI
|