Introduction
On March 11, 2011, a huge earthquake occurred off
the Pacific coast of the Tohoku region of Japan, followed by a
giant tsunami that caused unprecedented damage. Although it was
initially named ‘The 2011 Tohoku earthquake and tsunami,’ it was
later renamed ‘The Great East Japan Earthquake’ because the
affected area was not limited to the Tohoku region. However, the
prefectures of Iwate, Miyagi, and Fukushima, located on the Pacific
coast of the Tohoku region, were particularly affected. Numerous
lives were lost and many cities, towns, and villages were
destroyed. Following the earthquake and tsunami, infrastructure
such as the traffic network, electricity supply, water supply,
sewerage system, and telephone network suffered widespread damage.
To make matters worse, due to the power outage caused by the
tsunami, an accident occurred at the Fukushima Daiichi Nuclear
Power Plant (FDNPP), forcing many people to evacuate from their
homes.
The FDNPP is located astride the neighboring towns
Okuma and Futaba on the Pacific coast of Fukushima prefecture. The
evacuation zone included 13 neighboring towns and villages,
designated according to the level of radioactive contamination. A
large proportion of the residents were forced to evacuate to
temporary housing or to other areas. The number of evacuees peaked
at 164,000 (pref.fukushima.lg.jp/site/portal-english/en03-08.html).
At present, 6 years after the disaster, approximately 90,000
evacuees are still forced to live outside their hometowns
(reconstruction.go.jp/topics/main-cat2/sub-cat2-1/20170728_hinansha.pdf).
Temporary housing was quickly built to provide accommodation for
the evacuees in the months following the disaster. Assembly
facilities were constructed for each 50 houses (approximately) to
enhance the community and improve communication among the residents
(fdma.go.jp/concern/publication/higashinihondaishinsai_kirokushu/pdf/honbun/03-06.pdf).
Motoya (1) reported
the issues experienced by the evacuees living in the temporary
housing 2 years after the FDNPP accident. He indicated that because
the temporary housing was located in the highlands to avoid
tsunamis, it lacked convenience and isolated the evacuees from
public transport. Further, temporary housing was allocated almost
independently of preexisting social ties. In addition,
prefabricated housing was used for the temporary dwellings, and
this is often too hot in summer and too cold in winter. The
residents also complained of high levels of noise and a lack of
privacy. An increase in mental and physical health problems was
reported in evacuees following the earthquake and FDNPP disaster.
Recent studies have also demonstrated increases in depression,
disturbed sleep, lack of exercise and increases in body weight in
the evacuees after the disaster (2–4).
Studies reporting objective or quantitative
indicators expressing the severity of stress in the evacuees
following the disaster were not found. Therefore, we decided to use
urinary 8-hydroxy-2′-deoxyguanosine (8-OHdG) as a biomarker to
quantitatively and noninvasively assess oxidative stress in the
evacuees living in temporary housing to determine appropriate
levels of support for the evacuees. 8-OHdG is known as one of the
dominant forms of oxidatively generated base modifications produced
by the reaction of a hydroxyl radical on the C8 position of
2′-deoxyguanosine (dG) (5) in DNA or
on the guanine in the nucleotide pool (6). Because 8-OHdG is relatively stable, it
is excreted into urine in the unchanged form following its
intracellular production (7,8). The biomarker 8-OHdG is associated with
aging, smoking, exercise level, employment status, obesity,
diabetes, and depression (9,10). Thus, we inferred that 8-OHdG could be
used as an indicator to evaluate the mental and physical stress of
the evacuees.
In this study, we aimed to evaluate the changing
level of mental and physical stress in the evacuees by serially
measuring urinary 8-OHdG after the FDNPP disaster and to relate
this to health problems of the evacuees living in difficult
circumstances in temporary housing.
Materials and methods
Subjects and methods
Evacuees who originally lived in Namie town in
Fukushima prefecture and moved to temporary housing following the
FDNPP disaster were recruited to this study (Table I). The number of participants was
486, 346 and 195 in 2013, 2014, and 2015, respectively. Average
ages [± standard deviation, (SD)] in 2013, 2014, and 2015 were
62.8±18.2, 66.5±14.6, and 68.3±14.8 years, respectively. The
male/female ratios were 217/269, 160/186, and 81/114, respectively.
Among the participants chronic diseases including cardiovascular
disease and diabetes were present, which were diagnosed and
categorized by a physician (Yasushi Mariya, MD, PhD), based on the
detailed self-reports from them concerning health condition and
disease. The participants were inspected once a year for internal
radiation exposure using the whole-body counter FASTSCAN
(FASTSCAN™, Canberra Inc., Meriden, CT, USA) owned by
Namie town and none showed a committed effective dose over 1 mSv.
Five adult healthy volunteers also participated in this study as
control. Written informed consent was obtained from all the
participants. The study was performed in accordance with ethical
standards and was approved by the Ethics Committee of the Hirosaki
University Graduate School of Medicine (approval no. 2013-115).
 | Table I.Background of the study
participants. |
Table I.
Background of the study
participants.
|
| Year |
|---|
|
|
|
|---|
| Characteristic | 2013 | 2014 | 2015 |
|---|
| Participants (n) | 486 | 346 | 195 |
| Male/female (n) | 217/269 | 160/186 | 81/114 |
| Age (years) mean ±
SD | 62.8±18.2 | 66.5±14.6 | 68.3±14.8 |
We collected urine samples in November or December
at the first year. Thus, the urine sampling of the second year and
the third year was also in November or December to prevent effects
of seasonal fluctuation of oxidative stress. Analysis of urinary
8-OHdG was performed using Oxidative Stress Analyzer ICR-001
(Techno Medica, Japan). Measurements of 8-OHdG and creatinine were
made by immunochromatography and Jaffe's method, respectively
(www.technomedica.co.jp/t01/products/labo_tests/5/icr-001.html).
In a vial tube, 100 µl of urine sample and 100 µl of pure water
were mixed according to the analyzer protocol, and then measured.
Urinary 8-OHdG was corrected by the concentration of urinary
creatinine (CRE) and the value was expressed as the corrected value
(ng/mg CRE). The detection limits of 8-OHdG and CRE were estimated
to be 1.0 ng/ml and 10 mg/dl, respectively (technomedica.co.jp/t01/EnglishPage/products/labo_tests/2/icr-001.html).
The median value of the coefficient of variance was 0.130 (range:
0.093–0.197) obtained from urine samples of the five healthy
volunteers.
Each year, data from all the participants were
analyzed. At the same time, to exclude the influence of the age of
the participants, data were analyzed from 127 participants who
provided urine samples continually over the 3 years. Of these
participants, the average age in 2013 was 69.5±13.5 years, and the
male/female ratio was 52/75. In 2014 and 2015, the age composition
of the participants was significantly older than expected from the
2013 results (Table I).
The 127 participants who provided samples for 3
years continually were separated into two groups based on their
age. Those aged 65 or older in 2013 were defined as the ‘elderly’
group, and those younger than 65 as the ‘non-elderly’ group. The
elderly group comprised 90 participants with an average age of
76.2±7.6 years. The non-elderly group comprised 37 participants
with an average age of 53.0±10.0 years. In addition, of the 127
continual participants, 23 (18.1%) had no chronic disease, 83
(65.4%) had cardiovascular disease, 26 (20.5%) suffered from
diabetes, and 76 (59.8%) had been diagnosed with other chronic
diseases. There were a proportion of the 127 participants with
several diseases.
Statistical analyses
Continuous variables were expressed as mean average
± SD. One-way analysis of variance (ANOVA) was used to evaluate the
differences between groups for all participants, followed by
post-hoc analysis using the Games-Howell test. For the 127
continual participants, repeated ANOVA was used to evaluate the
differences between groups, followed by post-hoc analysis using
Tukey's HSD test or the Friedman test as appropriate. Two sample
t-test was used to compare the urinary 8-OHdG values of all the
participants with those for the 127 continual participants. Two-way
repeated-measures ANOVA was used to compare the mean urinary 8-OHdG
values between the elderly and non-elderly groups. The Mann-Whitney
test was used to evaluate the difference between the values by
gender.
Statistical analysis was performed using IBM SPSS
Statistics version 22 (IBM Corp., Armonk, NY, USA). P<0.05 was
considered to indicate a statistically significant difference.
Results
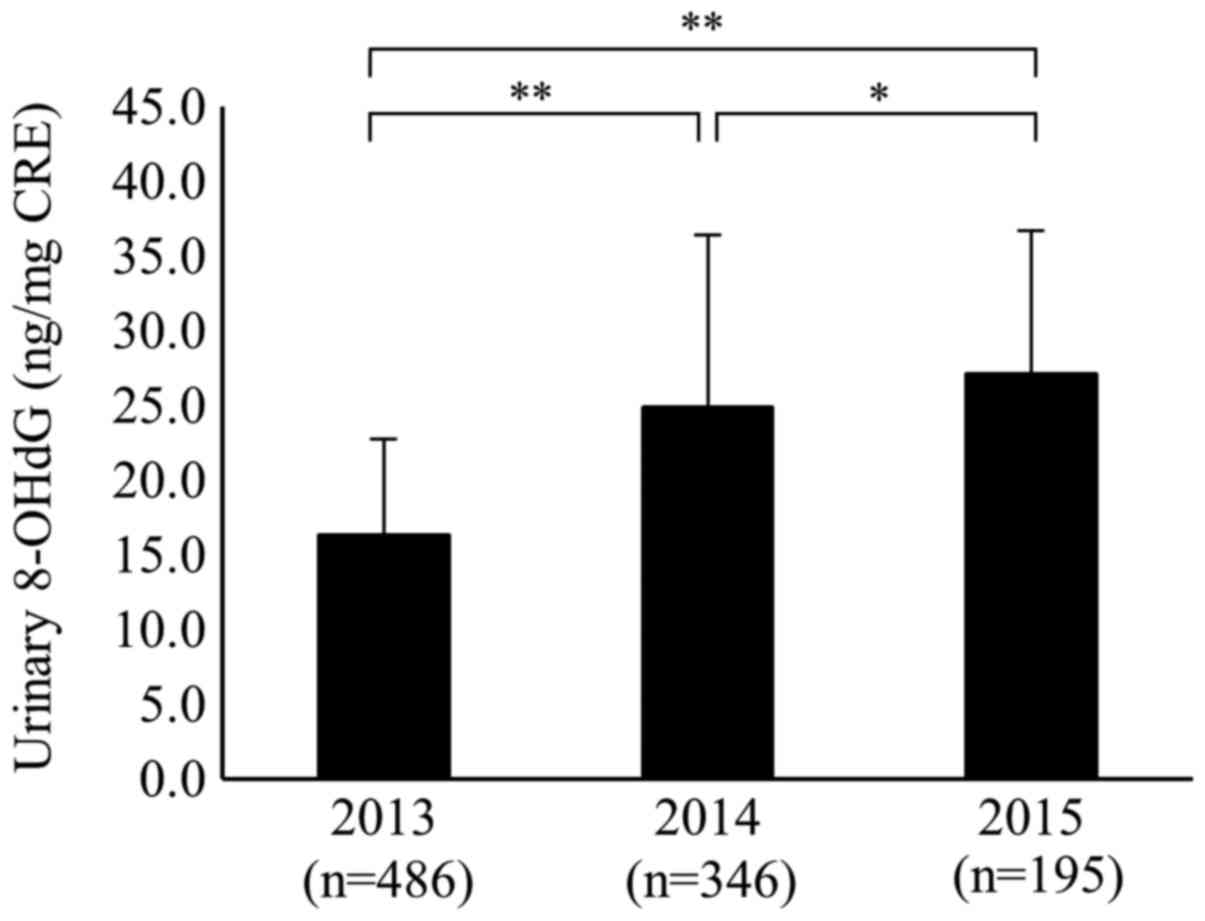
The mean values of urinary 8-OHdG for all subjects
were 16.4±6.4 (ng/mg CRE), 24.9±11.6, and 27.1±9.5 in 2013, 2014,
and 2015, respectively. The mean values of urinary 8-OHdG in 2014
and 2015 were significantly higher than that in 2013 (P<0.01).
Furthermore, the mean value of urinary 8-OHdG in 2015 was
significantly higher than that in 2014 (P<0.05; Fig. 1).
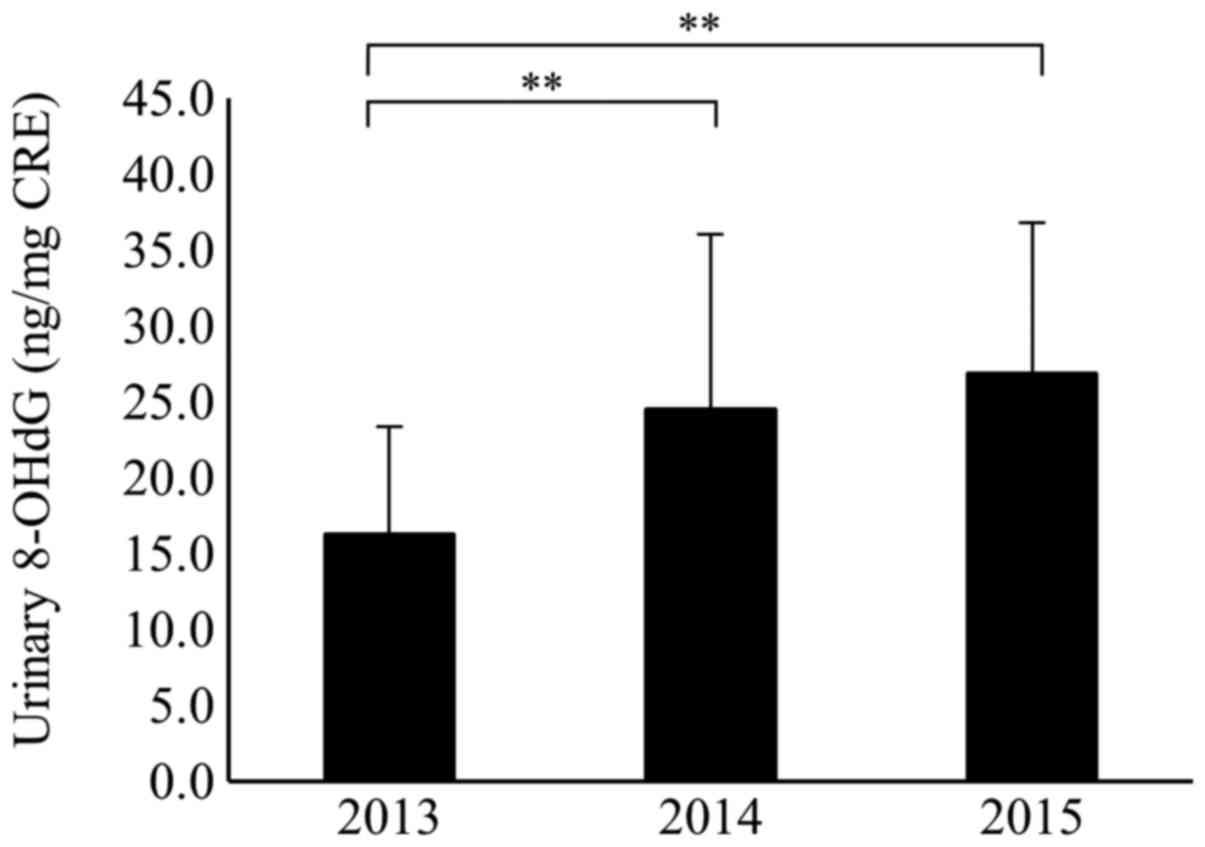
The 127 participants who continually provided urine
samples for 3 years were analyzed. The mean values of urinary
8-OHdG were 16.3±7.1, 24.6±11.5, and 26.9±9.8 in 2013, 2014, and
2015, respectively. Among them the mean values of urinary 8-OHdG in
2014 and 2015 were significantly higher than that in 2013
(P<0.01; Fig. 2). When comparing
the level of urinary 8-OHdG of the 127 continual participants with
that of all the participants, there was no significant difference
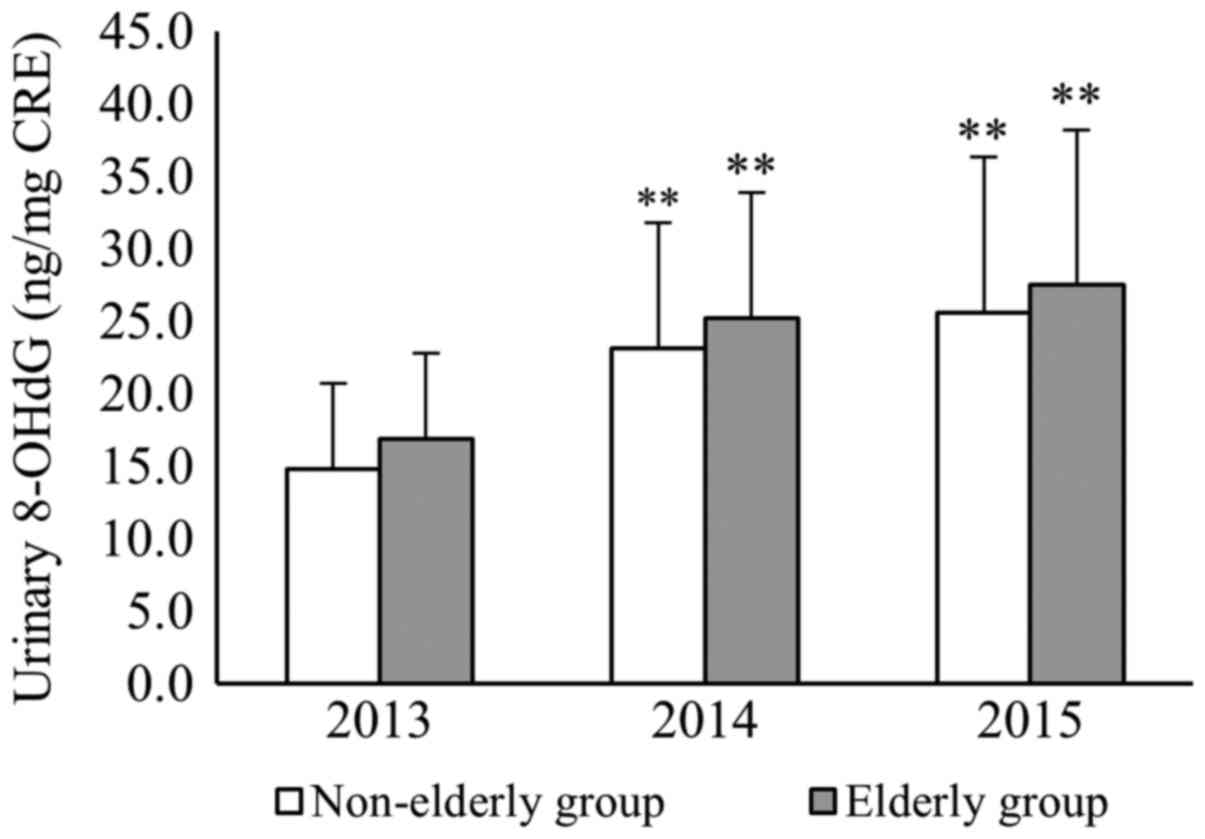
in the mean values between the two groups each year (Table II). Furthermore, in the elderly
group of the continual participants, the mean values of urinary
8-OHdG were 16.9±7.5, 25.2±12.5, and 27.5±9.5 in 2013, 2014, and
2015, respectively. In the non-elderly group, values were 14.8±5.9,
23.1±8.7, and 25.6±10.7 in 2013, 2014, and 2015, respectively. In
both of the age groups, the mean values of urinary 8-OHdG in 2014
and 2015 were significantly higher than that in 2013 (P<0.01).
For each year, there was no significant difference in the mean
values of urinary 8-OHdG between the elderly and non-elderly groups
within the 127 continual participants (Fig. 3).
| Table II.Mean values of urinary 8-OHdG. |
Table II.
Mean values of urinary 8-OHdG.
|
| Mean 8-OHdG (ng/mg
creatine) |
|---|
|
|
|
|---|
| Group | 2013 | 2014 | 2015 |
|---|
| All subjects | 16.4±6.4 | 24.9±11.6 | 27.1±9.5 |
| 127 subjects | 16.3±7.1 | 24.6±11.5 | 26.9±9.8 |
For gender, the mean values of urinary 8-OHdG of all
the male participants were 13.9±4.6, 22.7±9.2, and 26.4±9.1 in
2013, 2014, and 2015, respectively. For all females, the mean
values of urinary 8-OHdG were 18.0±7.9, 25.9±12.8, and 27.3±10.4 in
2013, 2014, and 2015, respectively. Only in 2013, the mean value of
urinary 8-OHdG of the females was significantly higher than that of
the males (P<0.01), and there was no significant difference in
the values by gender in 2014 and 2015.
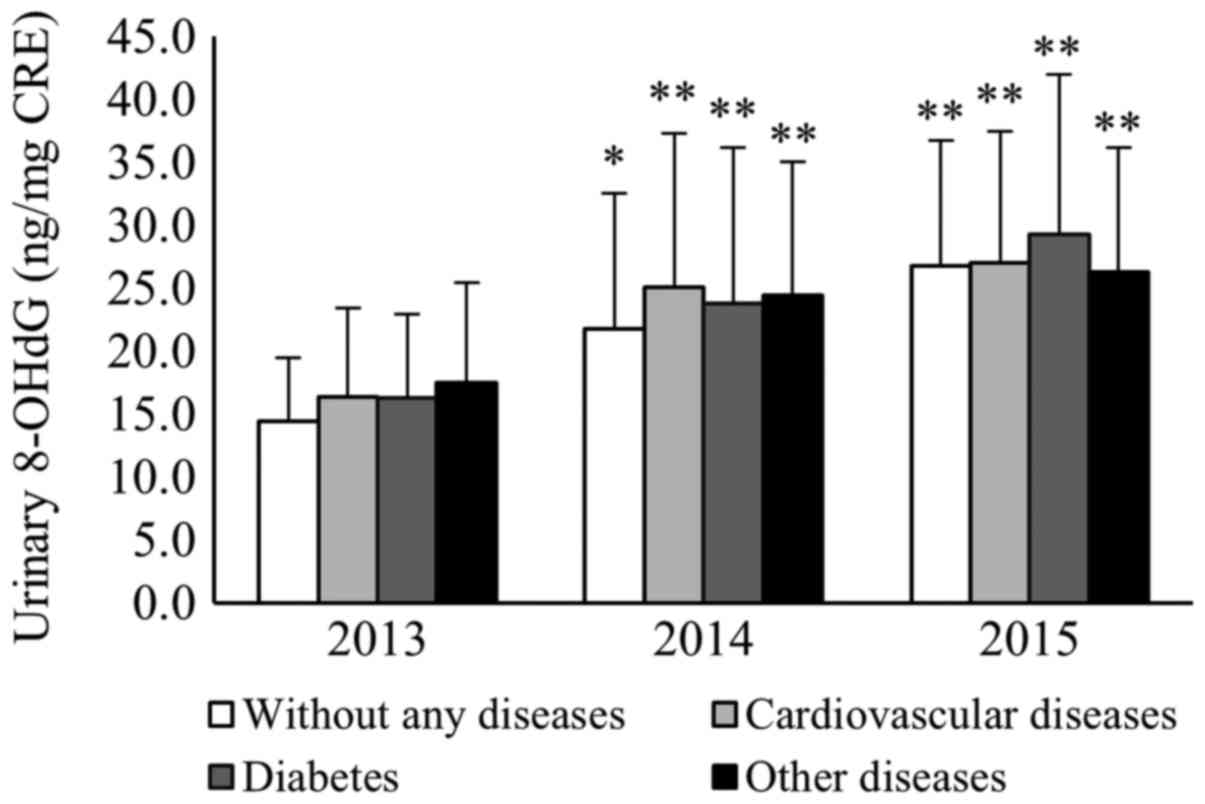
The mean values of urinary 8-OHdG for the 127
continual participants with no chronic diseases were 14.4±5.0,
21.8±10.8, and 26.7±10.0 in 2013, 2014, and 2015, respectively. The
mean values of urinary 8-OHdG in 2014 and 2015 were higher than
that in 2013 (P<0.05 and P<0.01, respectively). In contrast,
the mean values of urinary 8-OHdG for participants with
cardiovascular disease were 16.3±7.1, 25.1±12.2, and 27.0±10.4 in
2013, 2014, and 2015, respectively. Those with diabetes had values
of 16.3±6.7, 23.8±12.4, and 29.3±12.7 in 2013, 2014, and 2015,
respectively. Mean values for those with other chronic diseases
were 17.5±8.0, 24.5±10.6, and 26.3±9.9 in 2013, 2014, and 2015,
respectively. The mean values of urinary 8-OHdG for participants
with cardiovascular disease, diabetes, and other chronic diseases
in 2014 and 2015 were significantly higher than those in 2013
(P<0.01; Fig. 4).
Discussion
There are several phases of evacuation. In the
initial phase, evacuees go into emergency shelters, if possible, or
stay in their cars. They face medical issues such as emotional
stress and/or sleep disturbance, and may not have access to regular
medication. In addition, limited living space increases the risk of
thrombosis. After several months, evacuees move into temporary
housing. To evaluate the mental and physical stress of evacuees, we
analyzed the serial change of urinary 8-OHdG in the evacuees living
in temporary housing following the 2011 FDNPP disaster, starting
from 2013, once a year for 3 years. The level of urinary 8-OHdG
significantly increased in the second and third years compared with
that in the first year.
Kimura et al (11) measured urinary 8-OHdG in 248 healthy
Japanese volunteers using enzyme-linked immunosorbent assay
(ELISA), and the mean urinary 8-OHdG concentration was 15.2±5.71
ng/mg CRE. In the present study, measurement of urinary 8-OHdG was
initiated 2 years after the FDNPP disaster. The level of urinary
8-OHdG in the first year in our participants was similar to those
in healthy Japanese people reported by Kimura et al
(11). In 2004, the Chuetsu
earthquake occurred in Niigata prefecture in Japan, and Saito et
al (12) reported the level of
oxidative stress of 73 elderly residents living in temporary
housing. The survey was initiated 10 months after the earthquake
and continued for ~1 year. They also measured urinary 8-OHdG as an
oxidative stress marker using ELISA and reported that the urinary
8-OHdG level remained within normal range during the observation
(12). However, our results revealed
that the level of urinary 8-OHdG rose in the second and third years
compared with that in the first year. We consider that the
different period until the measurement was initiated, 10 months and
2 years after the disaster, played an important role in the
difference in results between the two surveys.
There was a shift in age composition of participants
in this study to significantly older participants in the second and
third years. The elderly generally have a higher prevalence of
chronic diseases (9). Therefore, at
first, we speculated that aging and chronic diseases might
influence the level of urinary 8-OHdG. We separated 127
participants who continually provided urine samples for 3 years,
into elderly and non-elderly groups. There was no significant
difference in the level of urinary 8-OHdG between the two groups.
Further, we categorized the 127 continual participants into four
groups: those with no chronic diseases, those with cardiovascular
disease, those with diabetes, and those with other chronic
diseases. The urinary 8-OHdG levels increased in the second and
third years regardless of the presence of each chronic disease. A
similar result was obtained regarding gender. These results suggest
that the stress level of the evacuees was not associated with age,
gender, or presence of chronic disease.
None of the evacuees showed the committed effective
dose over 1 mSv, and the physical effect of radiation was
negligible. However, there are specific properties of a radiation
disaster, which are derived from the psychosocial effects.
Participants' concerns included radioactive fallout, radiation
exposure, food safety, loss of employment, and loss of their own
homes. Furthermore, they lost social connection due to the
evacuation distance (13,14). Consequently, the evacuees in
radiation disasters have different stressors from other natural
disasters, which could accelerate mental and physical stress.
It has been reported that there are several
effective interventional programs providing exercise or a combined
program of exercise and craftwork for the evacuees (15,16).
Itaki et al (16) suggested
that these attempts were intended to improve physical conditions
and quality of life and that they reduced the risk of progression
of cognitive dysfunction. We consider that it is important to
provide opportunities for stress relief for the evacuees in the
chronic phase. In this case, 6 years have passed since the FDNPP
disaster, and public housing has been recently built in safe areas.
The temporary housing that we visited to conduct the survey was
closed; therefore, our survey ended at 3 years.
There are several limitations to the present study.
We measured only urinary 8-OHdG as an oxidative stress marker.
Also, detailed clinical information was not obtained according to
the wishes of the evacuees. Nevertheless, we believe that the
results are important because the data were obtained from the rare
situation of a nuclear-associated disaster.
In conclusion, evaluation of the stress level of
evacuees living in temporary housing following the FDNPP disaster,
employing the oxidative stress marker urinary 8-OHdG, demonstrated
a significant increase in stress level as the length of time living
in temporary housing increased.
Acknowledgements
Not applicable.
Funding
This study was in part supported by JSPS KAKENHI
(grant no. 25461900).
Availability of data and materials
The datasets used or analyzed during the current
study are available from the corresponding author on reasonable
request.
Author's contributions
CI and YM designed the research. YF, AN, CI and YM
conducted the research. YM provided essential reagents or
materials. YF and AN analyzed the data and ST and MY interpreted
the data. YF, CI and YM performed the statistical analyses. YF, CI,
ST, MY and YM wrote the paper. YM had primary responsibility for
the final content. All authors contributed to and approved the
final version of the manuscript.
Ethics approval and consent to
participate
Written informed consent was obtained from all the
participants. The study was performed in accordance with recognized
ethical standards and was approved by The Ethics Committee of the
Hirosaki University Graduate School of Medicine (approval number
2013-115).
Consent for publication
Written informed consent was obtained from all
participants for the publication of their data.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
8-OHdG
|
8-hydroxy-2′-deoxyguanosine
|
|
CRE
|
creatinine
|
|
FDNPP
|
Fukushima Daiichi Nuclear Power
Plant
|
References
|
1
|
Motoya R: Health Promotion for the Victims
and Evacuees of the Great East Japan Earthquake. Jap J Behavioral
Med. 19:68–74. 2013.(In Japanese).
|
|
2
|
Kitajima M, Otsu H, Tomisawa T, Sasatake
H, Itaki C, Yonaiyama C, Urushizaka M and Nishizawa Y: The
perception of health condition and radiation among elderly evacuees
four years after the Fukushima Nuclear Disaster. J Radiolo Nursing
Soc Jap. 5:47–55. 2017.(In Japanese).
|
|
3
|
Murakami H, Yoshimura E, Ishikawa-Takata
K, Nishi N, Tsuboyama-Kasaoka N, Yokoyama Y, Yaegashi Y, Sakata K,
Kobayashi S and Miyachi M: The longitudinal change in physical
activity among Great East Japan Earthquake victims living in
temporary housing. Nihon Koshu Eisei Zasshi. 61:86–92. 2014.(In
Japanese). PubMed/NCBI
|
|
4
|
Ohira T, Hosoya M, Yasumura S, Satoh H,
Suzuki H, Sakai A, Ohtsuru A, Kawasaki Y, Takahashi A, Ozasa K, et
al: Effect of evacuation on body weight after the great East Japan
earthquake. Am J Prev Med. 50:553–560. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kasai H and Nishimura S: Hydroxylation of
the C-8 position of deoxyguanosine by reducing agents in the
presence of oxygen. Nucleic Acids Symp Ser. 165–167.
1983.PubMed/NCBI
|
|
6
|
Hayakawa H, Taketomi A, Sakumi K, Kuwano M
and Sekiguchi M: Generation and elimination of
8-oxo-7,8-dihydro-2′-deoxyguanosine 5′-triphosphate, a mutagenic
substrate for DNA synthesis, in human cells. Biochemistry.
34:89–95. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Loft S and Poulsen HE: Estimation of
oxidative DNA damage in man from urinary excretion of repair
products. Acta Biochim Pol. 45:133–144. 1998.PubMed/NCBI
|
|
8
|
Valavanidis A, Vlachogianni T and Fiotakis
C: 8-hydroxy-2′- deoxyguanosine (8-OHdG): A critical biomarker of
oxidative stress and carcinogenesis. J Environ Sci Health C Environ
Carcinog Ecotoxicol Rev. 27:120–139. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kasai H, Iwamoto-Tanaka N, Miyamoto T,
Kawanami K, Kawanami S, Kido R and Ikeda M: Life style and urinary
8-hydroxydeoxyguanosine, a marker of oxidative DNA damage: Effects
of exercise, working conditions, meat intake, body mass index, and
smoking. Jpn J Cancer Res. 92:9–15. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Irie M, Miyata M and Kasai H: Depression
and possible cancer risk due to oxidative DNA damage. J Psychiatr
Res. 39:553–561. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kimura S, Yamauchi H, Hibino Y, Iwamoto M,
Sera K and Ogino K: Evaluation of urinary 8-hydroxydeoxyguanine in
healthy Japanese people. Basic Clin Pharmacol Toxicol. 98:496–502.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Saito K, Aoki H, Fujiwara N, Goto M,
Tomiyama C and Iwasa Y: Association of urinary 8-OHdG with
lifestyle and body composition in elderly natural disaster victims
living in emergency temporary housing. Environ Health Prev Med.
18:72–77. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Harada N, Shigemura J, Tanichi M, Kawaida
K, Takahashi S and Yasukata F: Mental health and psychological
impacts from the 2011 Great East Japan Earthquake Disaster: A
systematic literature review. Disaster Mil Med. 1:172015.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Maeda M and Oe M: Mental Health
Consequences and Social Issues After the Fukushima Disaster. Asia
Pac J Public Health. 29 Suppl 2:36S–46S. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Tomata Y, Sato N, Kogure M, Suto S, Imai
Y, Aoki H, Sugiyama K, Suzuki R, Sugawara Y, Watanabe T, et al:
Health effects of interventions to promote physical activity in
survivors of the 2011 Great East Japan Earthquake A longitudinal
study. Nihon Koshu Eisei Zasshi. 62:66–72. 2015.(In Japanese).
PubMed/NCBI
|
|
16
|
Itaki C, Fukushi Y, Kato T, Osanai T,
Ohtsu H, Sasatake H, Kitajia M, Tomisawa T, Hosokawa Y and
Nishizawa Y: The actual situation of motor functional decline of
elderly person who is continuing life as an evacuee by The
Fukushima Daiichi nuclear disaster and intervention to physical
activity preventive improvement. J Health Sci Res. 7:21–27.
2017.(In Japanese).
|