Introduction
The term cancer includes lesions manifesting a wide
range of characteristics which may originate in any cell type of an
organism, and each exhibits a distinct behavior and response to
treatment. There is believed to be three main types of cancer:
carcinomas, sarcomas and lymphomas/leukemias; 90% of human cancers
are carcinomas of epithelial origin and 8% are leukemias or
lymphomas which arise in blood stem cells and the immune system,
respectively, while sarcomas are solid tumors of the connective
tissue. Although hundreds of different types of neoplasia have been
described, only a few are reported with relative frequency.
Thirteen sites represent 85% of the total cancer incidence, notably
the prostate, breast and colon. Carcinoma of the lung is by far the
most lethal and is responsible for 30% of cancer-related
deaths.
The World Health Organization (WHO) International
Classification of Diseases defines oral cancer as a neoplasm
arising in the lips, oral cavity, oropharynx, nasopharynx or
hypopharynx. Oral squamous cell carcinoma (OSSC) is considered the
fifth most frequent cancer among males worldwide and the seventh
among females, with a prevalence that varies widely from 2–4% of
all malignant tumors in the US, Europe and Australia to 30% of
those in southern Asia (1). OSSC
represents 3–5% of all malignant tumors in Spain, but this
proportion is rising; the prevalence is generally higher than the
European mean, particularly for tongue and mouth cancers, although
oropharyngeal cancers are less frequent in Spain. Within Spain, the
frequency of cases is higher in northern vs. southern provinces and
highest in the Basque Country and Asturias.
Alongside Calvados in France, the Basque Country has
the highest rates in Europe, with an estimated rate of 13.24 cases
per 100,000 inhabitants (2). The
accumulated incidence (0–74 years; per 100) was 0.54 in males and
0.04 in females for tongue cancer, and 0.59 in males and 0.06 in
females for oral cancer. Alava is a province in the Basque
autonomous community.
Apart from the lips, where the maximum incidence is
recorded, the most frequently involved site is the tongue (25.1%),
followed by the floor of the mouth (10.2%) (3).
The etiology of oral cancer is unknown. Various
agents have been implicated in its development, either by directly
affecting the mucosa or by increasing its sensitivity to oncogenic
viruses or other carcinogenic agents. The combination of external
and internal (intrinsic) factors appears to magnify their potential
to induce the initial irreversible change (initiation), which only
gives rise to a tumor when cell division is stimulated. Known
etiological factors include tobacco, alcohol, genetic
susceptibility, infectious agents, radiation, pre-cancerous
lesions, nutrition, and oral and occupational factors.
The aberrant function of cell control mechanisms
leads to the uncontrolled division of cancer cells, which spread to
the rest of the organism and interfere with the function of normal
tissues where they occur. Although knowledge of the cellular and
molecular mechanisms involved is far from complete, an increasing
number of molecules are known to be implicated in the development
of cancer. Many of these are key proteins in cell cycle regulation
and programmed cell death (apoptosis).
The cell cycle involves a sequence of processes by
which a cell duplicates during the M phase for nuclear division
(mitosis) and cytokinesis. The G1 phase is the interval before the
start of DNA synthesis; the S phase is when the cell duplicates its
DNA content. Finally, the G2 phase is the interval between the end
of the S phase and the start of new mitosis.
The duration of these four phases widely varies
among different cell types. A rapidly proliferative human cell
completes its cycle in 24 h, with 11 h for the G1 phase, 8 for the
S phase, 4 for the G2 phase and ∼1 h for M phase. However, certain
cells of the organism never change; they leave G1 and enter a cell
cycle stage designated G0, in which they remain metabolically
active, but do not divide unless they are specifically stimulated
by extracellular signals (4).
Materials and methods
Data collection
A protocol was established for the collection of the
clinical data considered to have greater prognostic value. A
specifically designed form was completed for each patient to gather
the following data: clinical record no., age, gender, smoking
habits, drinking habits, state of the mouth, reason for
consultation, disease localization and gross appearance, tumor size
(0–1 cm; >1–3 cm; >3 cm), the presence of adenopathies,
disease located in the tongue with no bone involvement, in the
tongue with bone involvement, in the retromolar trigone or in the
hard/soft palate, tumor stage, treatment, disease course and degree
of differentiation.
Inclusion and exclusion criteria
Inclusion criteria were the presence of OSSC, no
previous visit to a medical centre for this condition, no lymph
node metastasis at diagnosis (stages I or II), and no previous
radiotherapy, chemotherapy or surgical treatments. Exclusion
criteria were incomplete clinical records (missing either
affiliation or clinical data), uncertainty about the oral
localization of the primary tumor, inadequate diagnostic material
in blocks, and death of the patient from another cause preventing
evaluation of disease progression.
Results
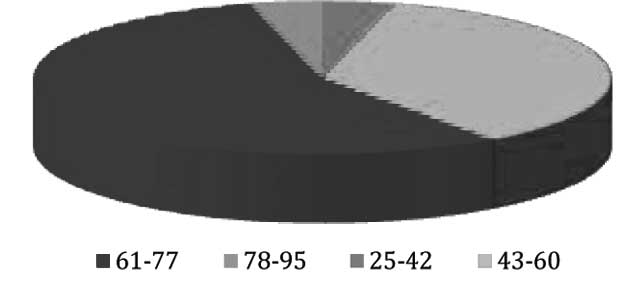
The mean age of the 30 patients (25 males) was 59.15
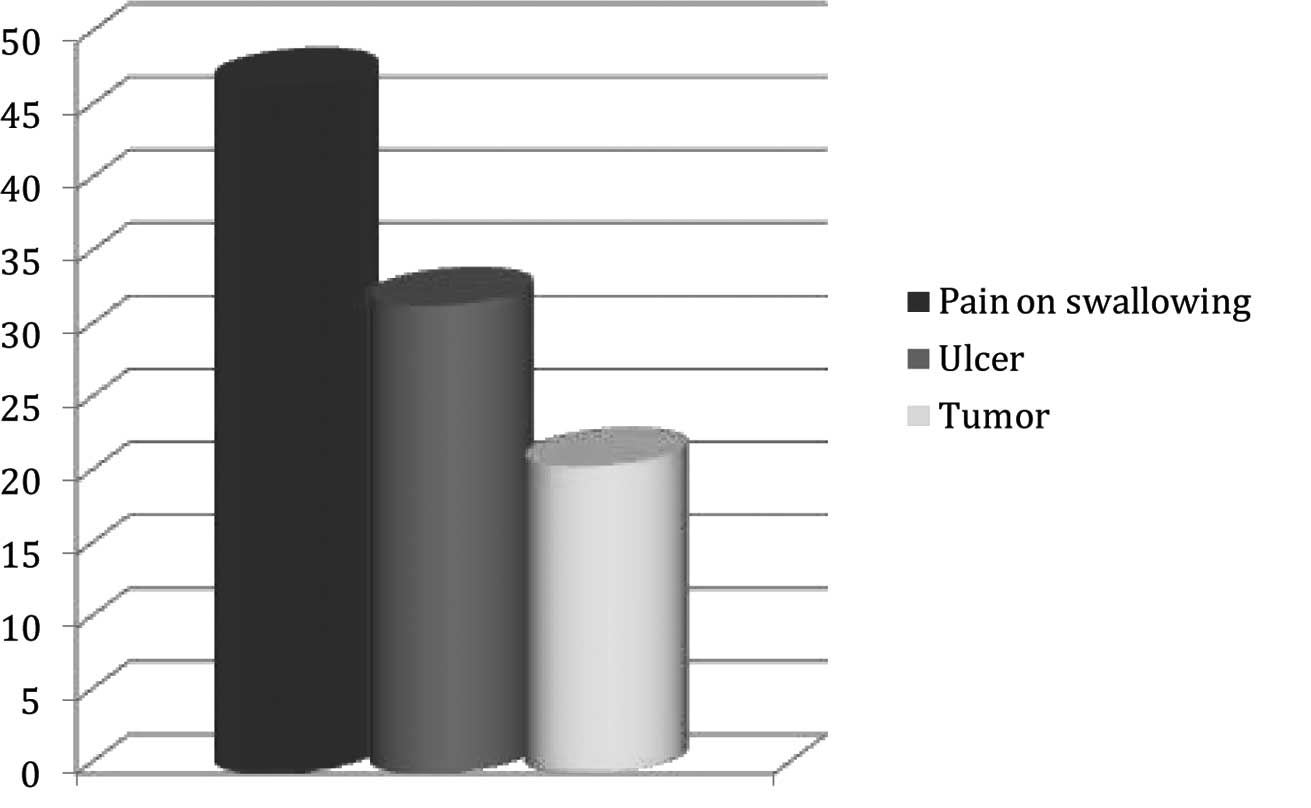
years (range 28–91); the age distribution is depicted in Fig. 1. The most frequent reason for the
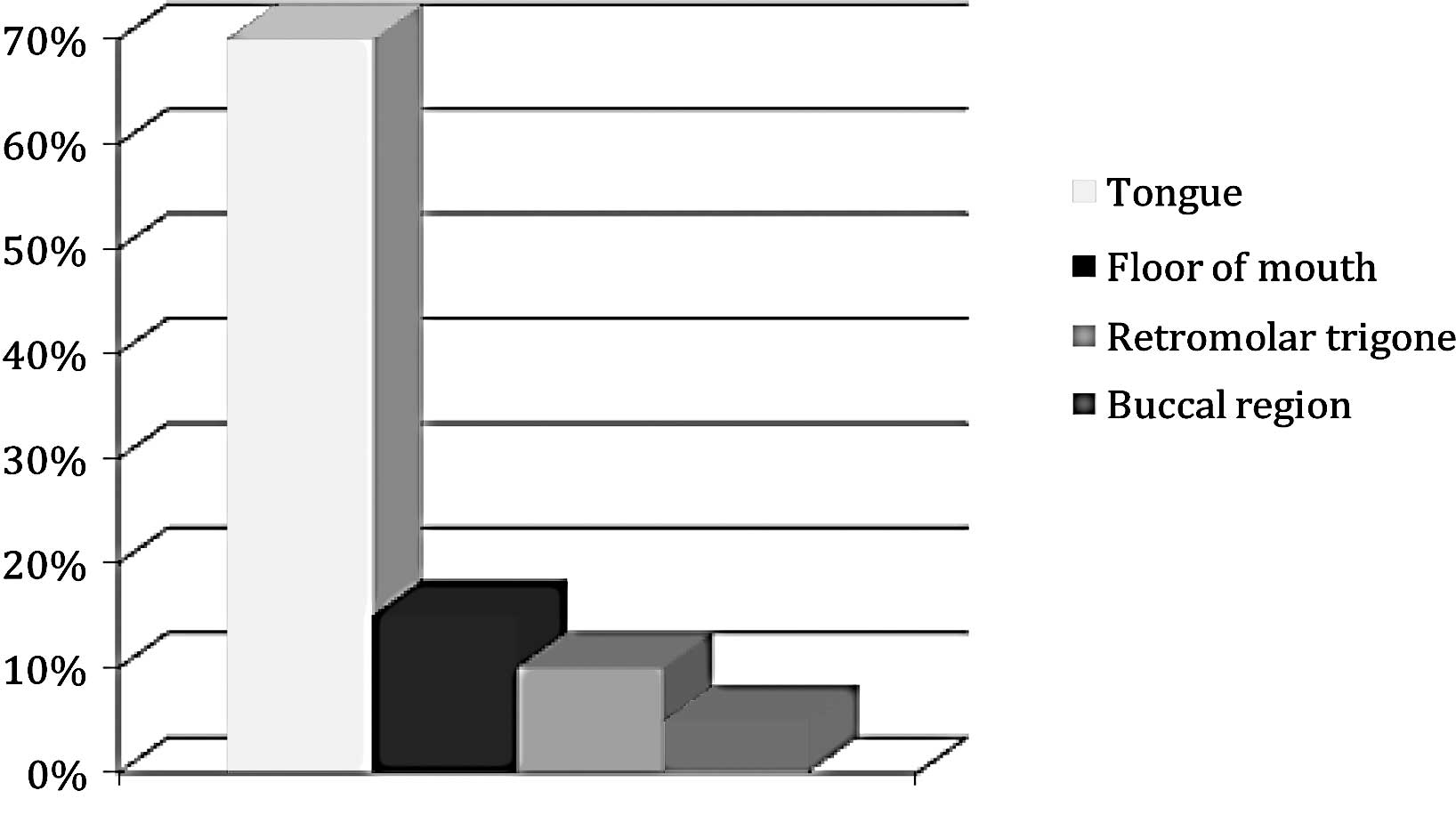
initial visit was pain on swallowing (Fig. 2), and the most frequent site was
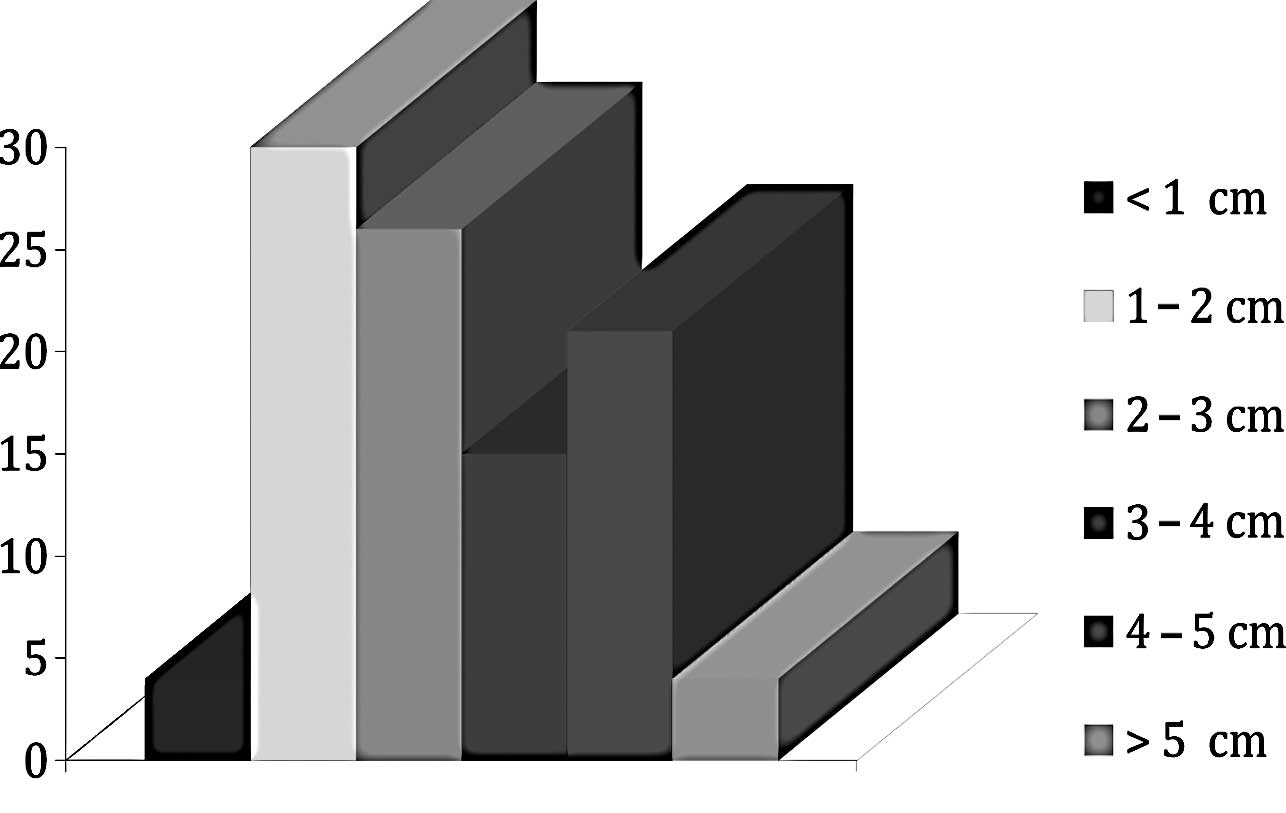
the tongue (Fig. 3). The mean
tumor size was 2.21 cm (Fig. 4).
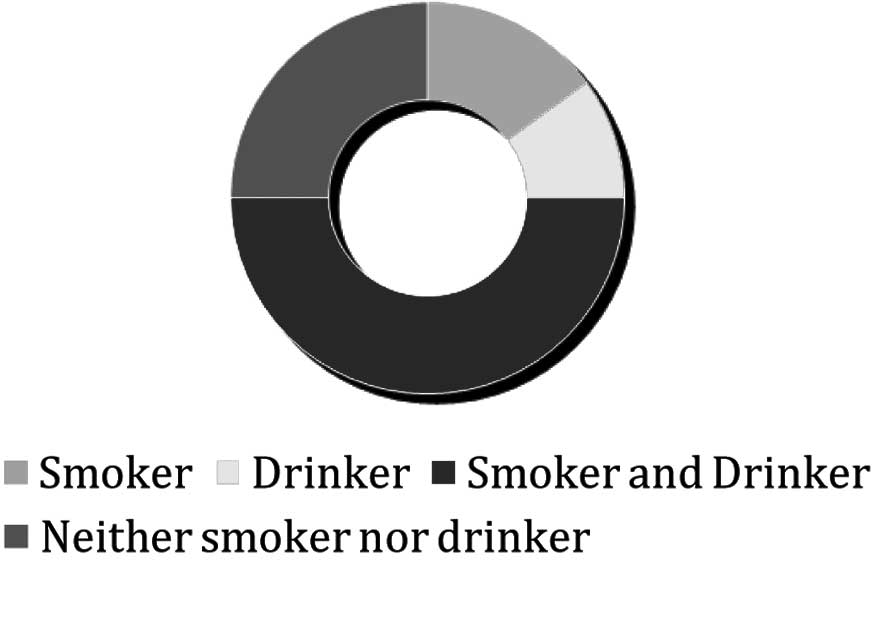
The most frequent risk factors were tobacco and alcohol, which were
both used by 50% of the patients (Fig.
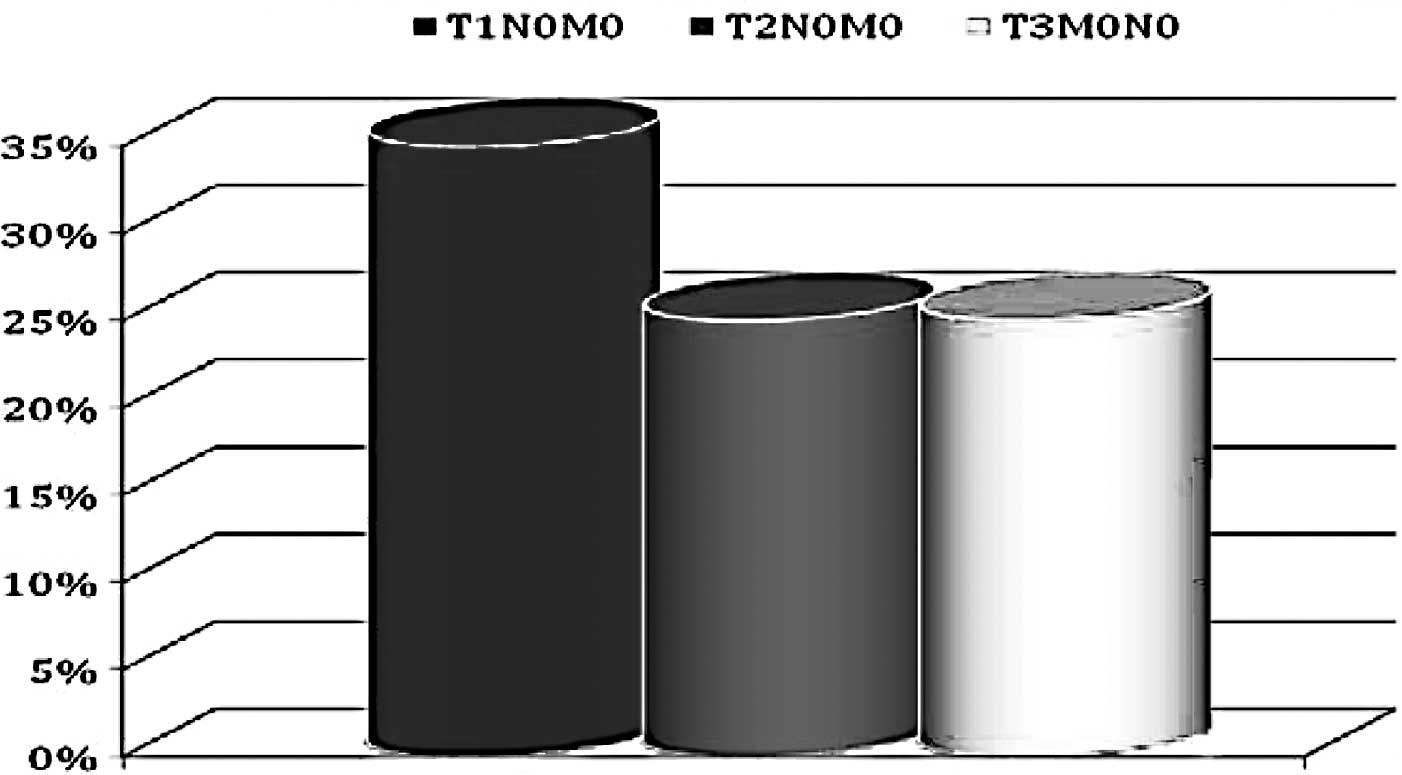
5). The most frequent stage was T1N0M0, in 35% of the patients
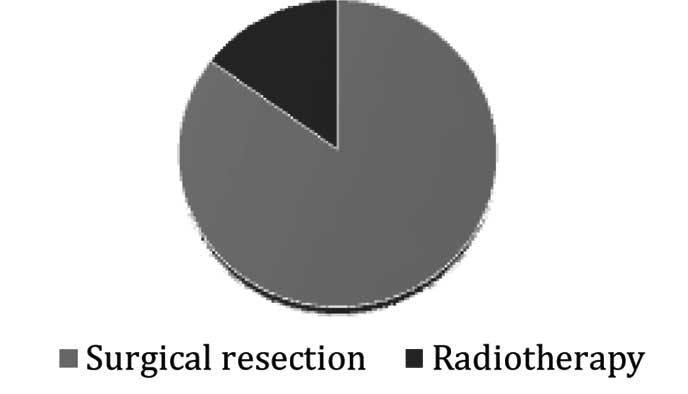
(Fig. 6). The treatment was
surgical resection in the majority of cases (85%), while adjuvant
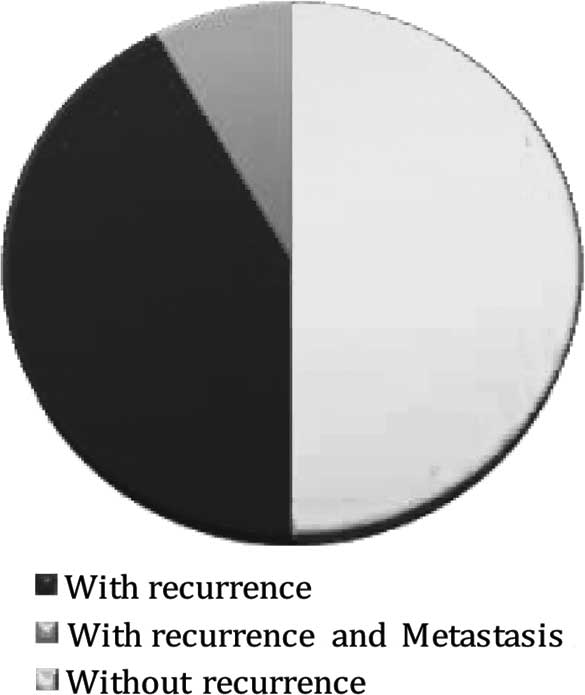
radiotherapy was also applied in several cases (15%) (Fig. 7). Half of the patients did not
present with recurrence, while a small number (10%) presented with
recurrence and metastasis (Fig.
8).
Discussion
In this series of OSCC patients, the disease was
most frequently detected in the sixth decade of life and in males,
as previously reported (2,3). The site was the tongue in 70% of the
patients, explaining why pain on swallowing was the most frequent
reason for admission. The mean tumor size was 2.21 cm and ranged
from 1 to 2 cm in the majority of cases, although a number of them
were 3–4 cm. Among the risk factors, half of our sample used both
tobacco and alcohol, suggesting that a preventive and educational
approach may assist control of this disease (Fig. 6). The most common tumor stage was
T1N0M0, although stages T2 and T3 were also frequent. Surgical
resection was the treatment of choice, while adjuvant radiotherapy
was also used (Fig. 7). Half of
the patients in our series did not present with recurrence.
In conclusion, the most frequent age at OSCC onset
was 61–77 years with the disease being more prevalent in males. The
most prevalent risk factors were found to be tobacco and alcohol.
The most frequent reason for hospital admission was pain on
swallowing with the tongue being the most frequent site. The mean
tumor size was 2.21 cm, and the most frequently presented stage was
T1N0M0. Surgical resection was the treatment of choice. Patient
outcomes were similar between patients with recurrent and
non-recurrent disease.
References
|
1.
|
Chandu A, Adams G and Smith ASH: Factors
affecting survival on patients with oral cancer: an Australian
perspective. Int J Oral Maxiloofac Surg. 34:514–520. 2005.
View Article : Google Scholar
|
|
2.
|
Moreno López LA and Esparza Gómez G: Oral
cancer versus orpharyngeal cancer versus head and neck cancer. Oral
Oncol. 34:576–577. 1998.PubMed/NCBI
|
|
3.
|
Martínez-Conde R, Aguirre JM, Burgos JJ
and Rivera JM: Clinicopathological factors in early squamous cell
carcinoma of the tongue and floor of the mouth in Biscay (the
Basque Country, Spain). Med Oral. 6:87–94. 2001.PubMed/NCBI
|
|
4.
|
Tood R, Hinds PW, Munger K, Rustgi AK,
Opitz OG, Suliman Y and Wong DT: Cell cycle dysregulation in oral
cancer. Crit Rev Oral Biol Med. 13:51–61. 2002. View Article : Google Scholar : PubMed/NCBI
|