Introduction
Developmental anomalies of the inferior vena cava
(IVC) include various congenital malformations that are traced to
the embryogenesis of the IVC. Since the earliest description by
Abernethy and Banks (1) in 1793,
these anomalies have been regarded as normal variations of the
retroperitoneal venous system for over a century, since they rarely
occur and are mainly distinguished in cadaver dissection or
accidentally during surgical exploration. Moreover, these anomalies
cause no significant lifelong problems due to their latency
(2). Thus, the clinical
significance of these conditions has long been underestimated.
Advances in medical imaging technologies and the increasing
availability and accessibility of these methods in clinical use in
the recent decades have provided a reliable method to investigate
these anomalies. Various types of the anomalies have been
identified with the help of cross-sectional imaging (3). Imaging results also serve as a
valuable tool for clinicians to re-evaluate several clinical
conditions, including haematuria (4) and urinary tract infection (5) of unknown aetiology, as well as
recurrent deep vein thrombosis (DVT) and pulmonary embolism
(6,7), which used to be refractory to
conventional treatment and is currently considered to be related to
the underlying anomalies of the IVC.
Despite these advances, knowledge of these anomalies
remains insufficient among most radiologists and clinicians, which
may lead to misdiagnosis in certain circumstances (8). For an interventional radiologist or
surgeon, overlooking the existence of IVC anomalies may pose
potential procedural risk. Hence, a better understanding of these
anomalies and familiarity with their imaging features has become an
essential task for radiologists and clinicians, to reduce
misinterpretation and achieve accurate diagnosis. Cases of several
typical developmental IVC anomalies diagnosed by an abdominal CT
scan are reported in this study and the underlying clinical
significance was evaluated by reviewing relevant literature.
Although the incidence rate of IVC dysplasia is
significant, this condition generally has no serious consequences.
IVC dysplagia is occasionally detected during an imaging
examination or when surgery on a related area is conducted. The
condition commonly includes left IVC, double IVC, IVC absence in
the hepatic segment, left renal vein around the aorta, retroaortic
left renal vein and retrocaval ureter (1). The misinterpretation of this
condition as another lesion may be avoided by providing important
clinical information. In the present study, computed tomography
(CT) manifestations of six different types of IVC dysplasia cases
are reported and their clinical significance is discussed.
Materials and methods
General data
Several patients who received abdominal and chest CT
examinations between July 2009 and September 2011 in the Dongyang
People’s Hospital were reviewed. A number of cases presented IVC
dysplasia. In addition, several cases could not be defined due to
the insufficiency or non-enhancement of the examination range.
Among these cases, six cases of various common IVC dysplasia with
typical manifestations were reviewed as follows: 5 male cases and 1
female case, with ages ranging from 43 to 73 years. This study was
conducted in accordance with the declaration of Helsinki. This
study was conducted with approval from the Ethics Committee of
Tongji University School of Medicine. Written informed consent was
obtained from all participants.
CT examination method and image
processing
Philips Brilliance 64-row spiral CT was used.
According to the corresponding examination items, enhanced or plain
CT scanning examination of the abdomen or chest was conducted, with
a scanning layer thickness of 5 mm. The examination results were
entered into the picture archiving and communication systems and
saved for reading.
Results
A total of six common IVC dysplasia cases were
identified and six different typical cases were reported.
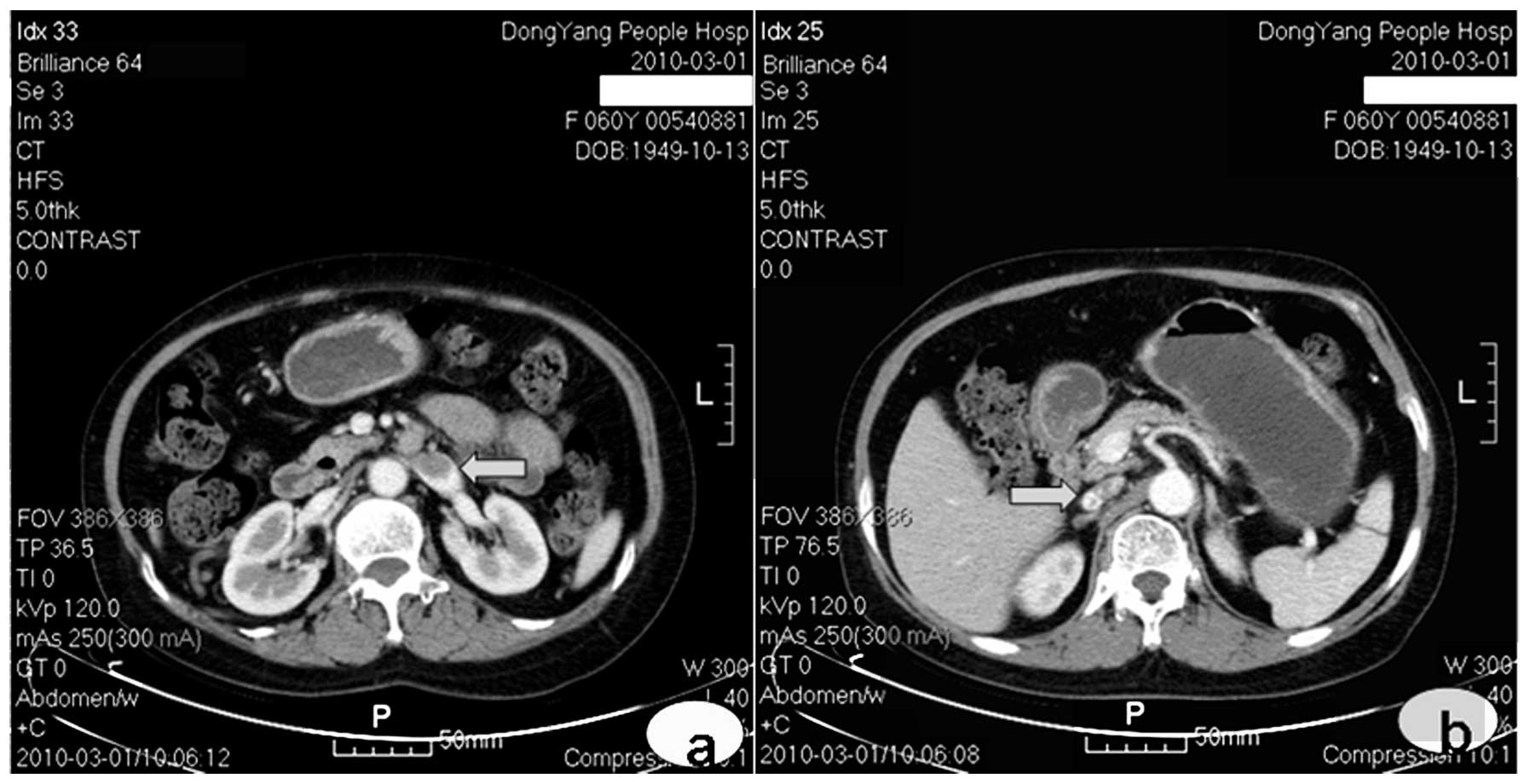
Case 1: left IVC
The patient was female and aged 60 years. Abdominal
enhanced CT was conducted for re-examination following
chemotherapy, due to non-Hodgkin lymphoma. The left renal vein
extended out a large thick vascular shadow downward and the
enhancement conditions complied with the veins. The condition was
also accompanied by an abdominal aorta to the left side of the
normal position of the abdominal aorta, which branched into the
bilateral common iliac veins at the lumbar 5 vertebral level. Over
the right renal vein level, its continuous large thick vascular
shadow was invisible. Over the right renal vein level, it extended
out as a normal running IVC (Fig.
1). This abnormality was diagnosed as left IVC.
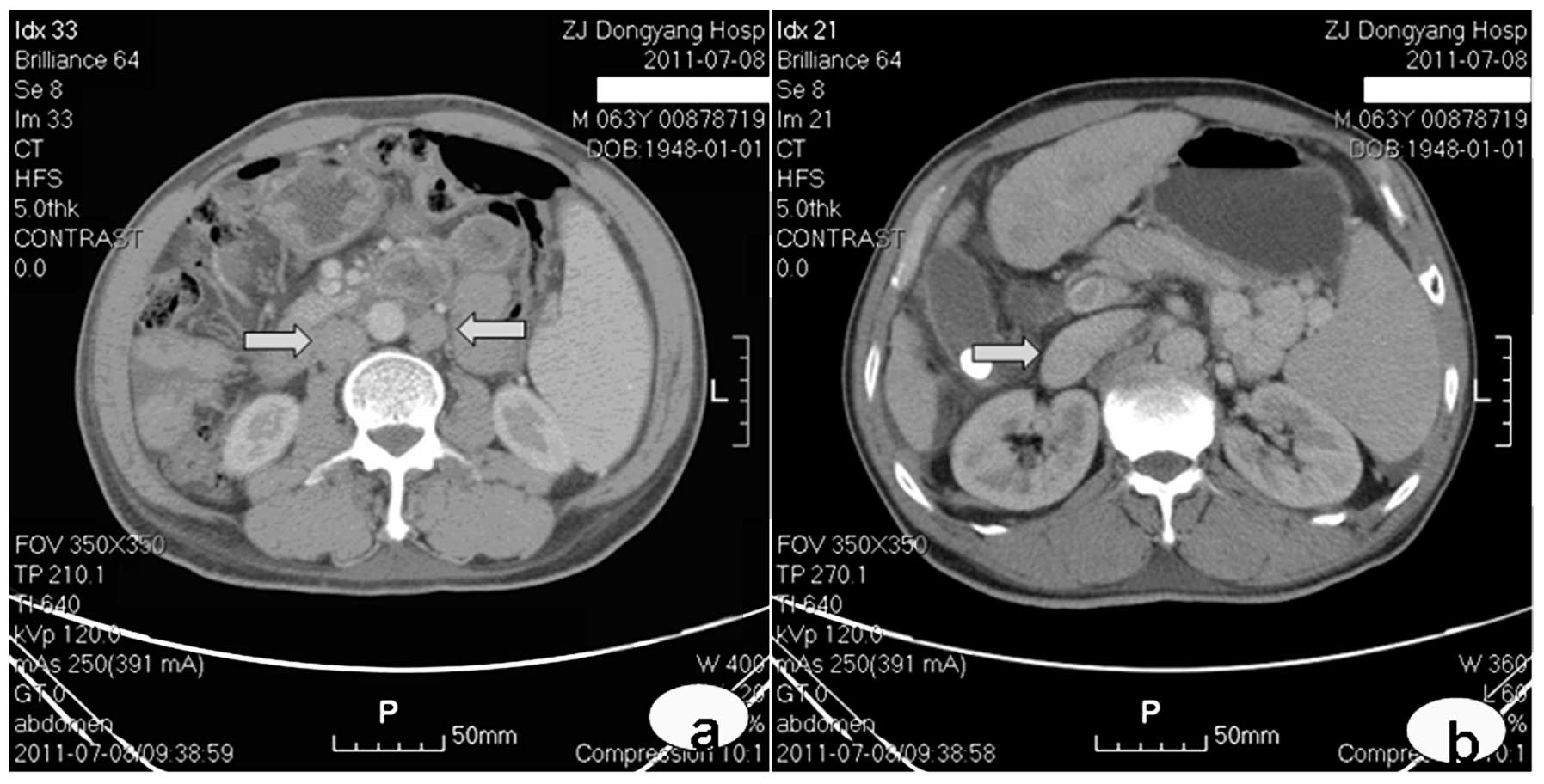
Case 2: double IVC
Abdominal enhanced CT was conducted in a 63-year-old
male due to the space-occupying location in the hepatic left lobe
and the presence of cholecystolithiasis, as confirmed by an
ultrasound examination. The bilateral renal veins extended out a
large thick vascular shadow downward. They were accompanied by the
downward abdominal aorta at the bilateral sides of the abdominal
aorta, which branched into the iliac veins at the lumbar 5
vertebral level. Over the right renal vein level, the bilateral
renal veins extended out as a normal running IVC (Fig. 2). This condition was diagnosed as
double IVC.
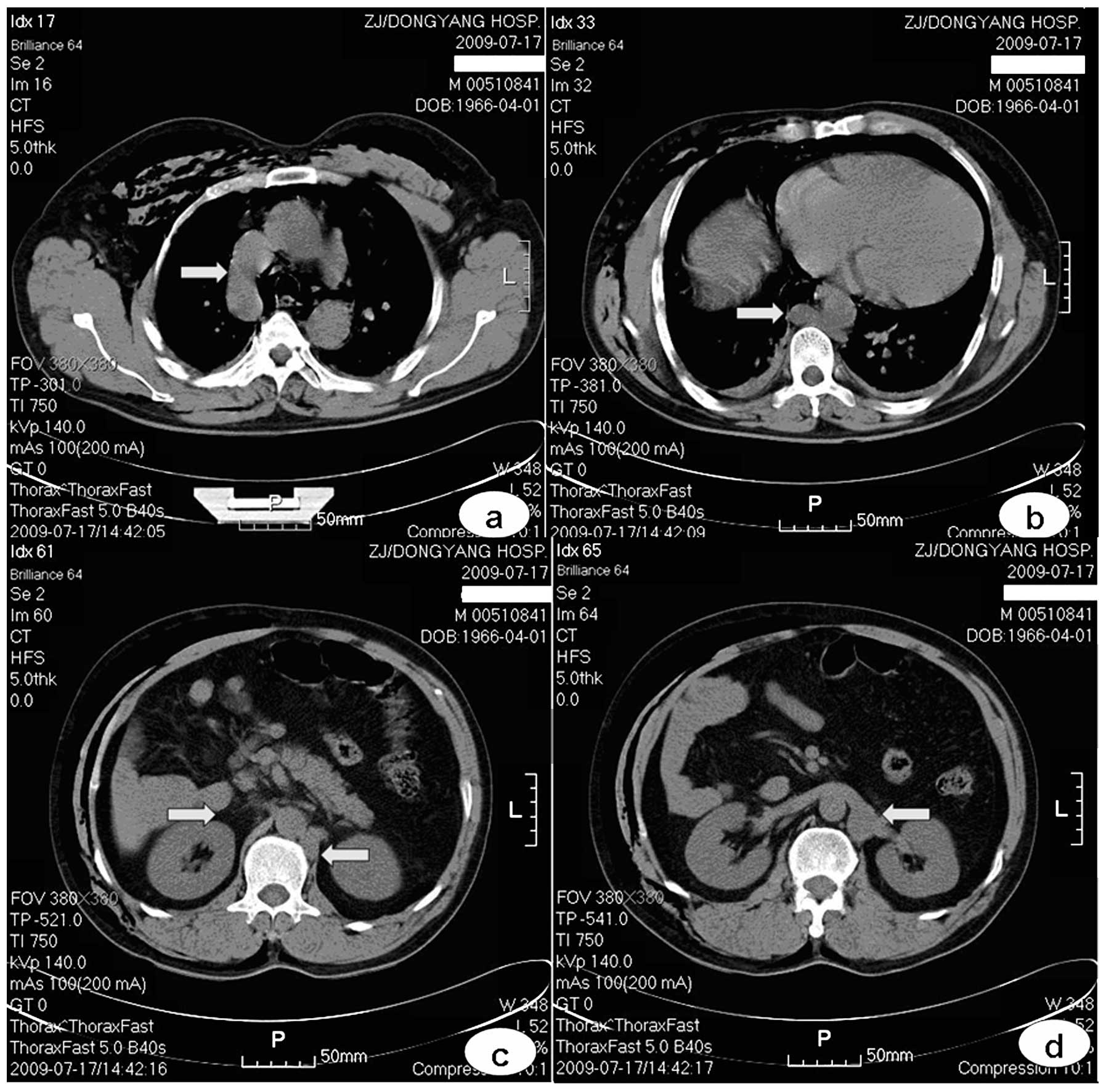
Case 3: absence of IVC in the hepatic
segment
Pectoral and epigastric plain CT was conducted in a
43-year-old male due to an injured abdomen caused by a traffic
accident. The azygos vein thickened (Fig. 3a) and continued as thickened
hemiazygos vein to the pectoral vertebral level 10 body (Fig. 3b) and ran downward to the left
renal vein behind the left crus of the diaphragm (Figs. 3c and d). No IVC was visible over
the right renal vein level. Therefore, the absence of IVC in the
hepatic segment was considered. Left IVC was possibly present;
however, this cannot be confirmed since hypogastric scanning was
not performed. This case of CT examination showed no enhancement;
however, vessel running is clearly shown compared with the
perivascular adipose tissue with trauma-induced mediastinal
emphysema.
Case 4: left renal vein around the
aorta
A 62-year-old male underwent abdominal enhanced CT
for re-examination after biliary stent implantation was conducted
due to bile duct carcinoma. Aside from the superior left renal vein
running anterior to the abdominal aorta (Fig. 4a), an additional inferior vessel
draining the left kidney and crossing the abdominal aorta was
observed to converge into the rear IVC (Fig. 4b). This abnormality was diagnosed
as left renal vein around the aorta.
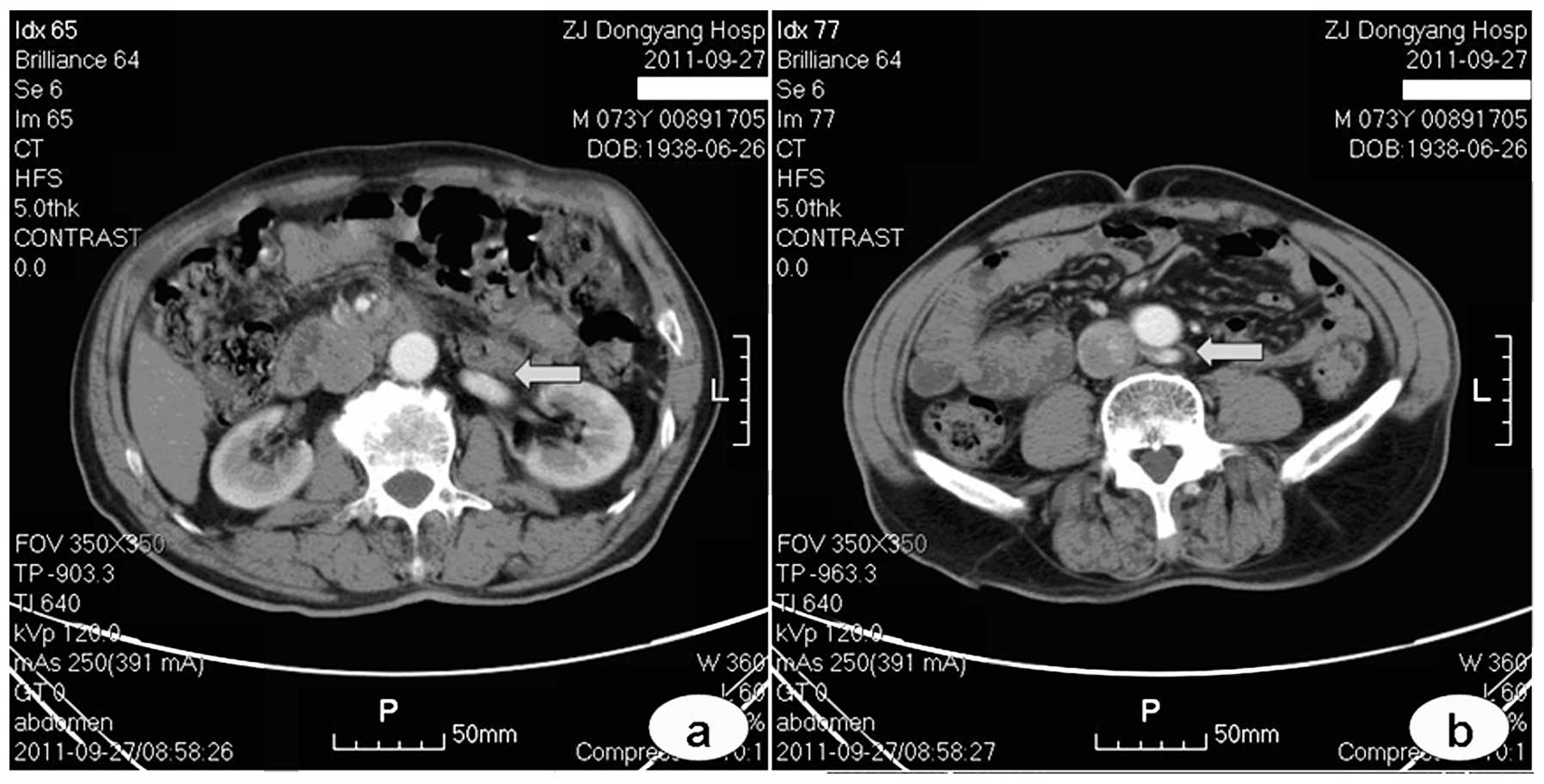
Case 5: retroaortic left renal vein
The patient was male and aged 73 years. Abdominal
enhanced CT was conducted for re-examination following chemotherapy
due to gastric cancer. The left renal vein ran downward to the
right, crossing behind the abdominal aorta at the superior border
of a lumbar vertebra to converge dorsally into the IVC (Fig. 5). This condition was diagnosed as
retroaortic left renal vein.
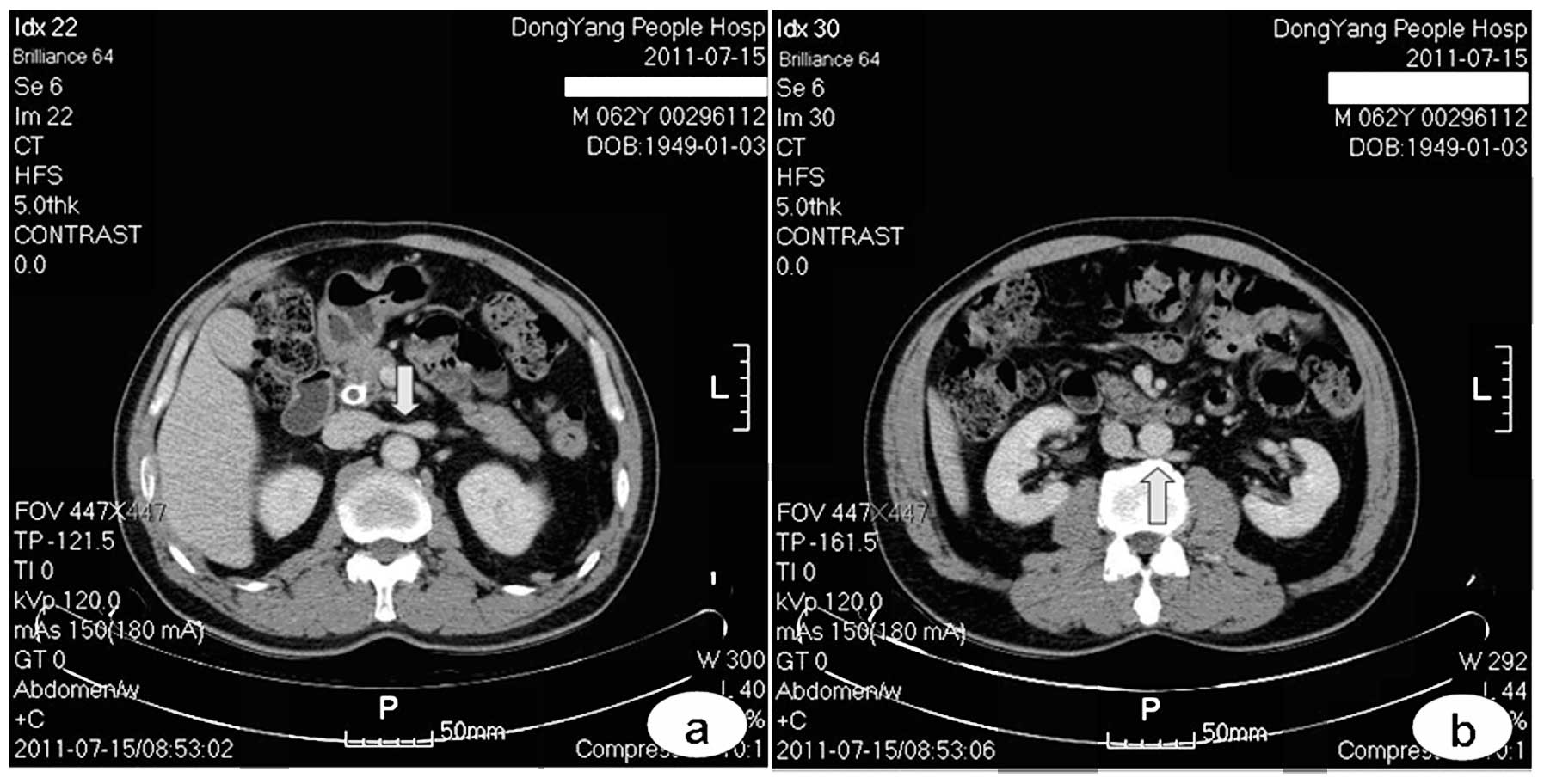
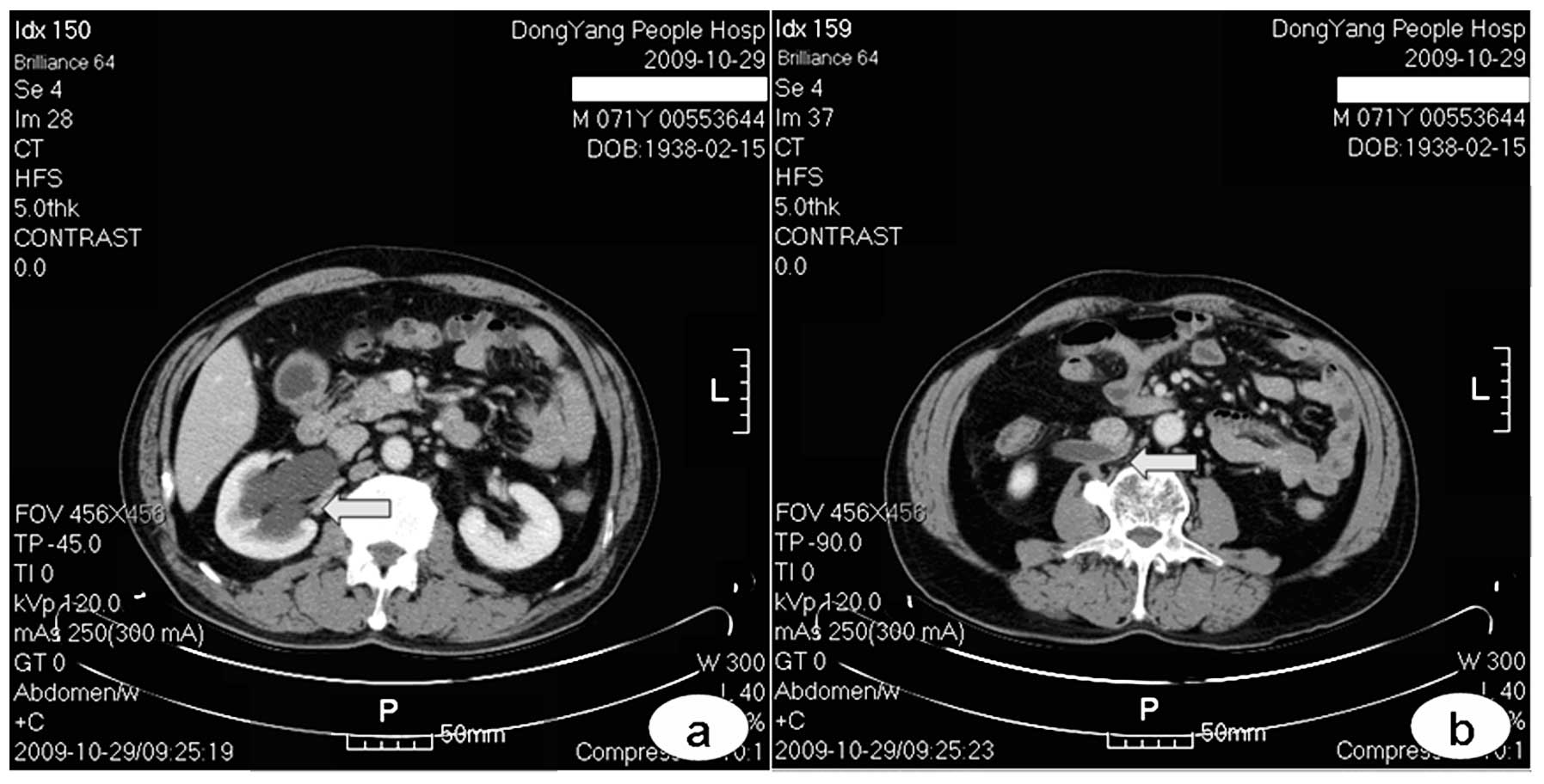
Case 6: retrocaval ureter
A 71-year-old male underwent abdominal enhanced CT
due to cecum carcinoma, as confirmed by enteroscopy. The right
hydronephrosis was visible, renal parenchymal thickness was normal
(Fig. 6a) and the right ureter
abnormally ran inward and crossed behind the IVC (Fig. 6b). Hydrops were observed at the
superior part and the inferior ureter had no apparent hydrops
(Fig. 6b). This disease was
diagnosed as retrocaval ureter.
Discussion
The incidence rate of IVC dysplasia is significant.
The embryonic development of this condition is complex and derived
from the development of three pairs of embryonic veins, including
the vena postcardinalis, subcardinal and supracardinal vein.
Anastomosis, atrophy and disorders that occur during development
will cause dysplasia (9).
A normal IVC includes four segments: hepatic, renal
superior, renal and renal inferior segments (2). The hepatic segment is derived from
the vitelline vein. The right subcardinal vein develops into the
renal superior segment by forming subcardinal vein-hepatic segment
anastomosis. The renal segment is derived from the right
supracardinal vein-subcardinal vein and vena
postcardinalis-subcardinal vein anastomoses. In the chest, the
supracardinal vein develops into azygos and hemiazygos
vein/accessory hemiazygos veins. In the abdomen, vena
postcardinalis is gradually replaced by the subcardinal and
supracardinal veins; however, it persists in existence and develops
into the iliac vein in the pelvic cavity. Anastomosis between the
dorsal supracardinal veins, between the ventral subcardinal veins
and between the vena postcardinalissubcardinal veins
constitute the renal collar. The embryonic kidney is first drained
by pairs of ventral and dorsal branches. Bilateral dorsal branches
degrade. On the right, the ventral branch integrates into the
lateral wall of the IVC in the renal segment. On the left, the
ventral and the anterior branches of the renal collar constitute
the normal left renal vein. The embryonic ureter develops from the
pelvic cavity after the posterior kidney develops and runs at the
vena postcardinalis rear and at the anterior internal
supracardinal vein. Vena postcardinalis-supracardinal vein
anastomosis formed at the inferior part and supracardinal
vein-subcardinal vein anastomosis formed on the renal level
constitute a vein ring around the ureter. In a normal developmental
process, the right vena postcardinalis degrades and withers,
whereas the right supra-cardinal vein develops into the renal
inferior segment IVC.
If the right supracardinal vein cannot form the
normal right IVC due to an abnormal degeneration and the left
supracardinal vein develops into an IVC in the renal inferior
segment, the abnormality is diagnosed as left IVC (10). If both bilateral supracardinal
veins develop into an IVC of the renal inferior segment, the
condition is diagnosed as a double IVC (11). If subcardinal vein-hepatic segment
anastomosis fails, continuous IVC are not developed. As a result,
IVC from over the renal vein to the hepatic vein abouchement level
is absent and hepatic veins converge to flow directly into the
right atrium. This condition is known as the absence of IVC in the
hepatic segment. Lower venous blood flow in the body flows back via
the superior vena cava by the expanded azygos vein or hemiazygos
vein (12). If the dorsal branch
of the embryonic left renal vein and the posterior of the renal
collar persist, two left renal veins are present; the left adrenal
gland flows back via the superior left renal vein and the left
gonadal vein flows back via the inferior left renal vein (13). If the ventral branch of the
embryonic left renal vein and the anterior branch of the renal
collar abnormally degrade and disappear, whereas the dorsal branch
of the embryonic left renal vein and the posterior branch of the
renal collar develop into the left renal vein, the abnormality is
diagnosed as retroaortic left renal vein (14). If the right vena
postcardinalis does not degrade, but develops into the main
component of the IVC in the renal inferior segment, the right
ureter that initially courses behind the IVC runs down inwardly to
the inner side of the vein, and continues downward and finally
circumvents anterior to it. Therefore, a retrocaval ureter forms
(15). In addition, multiple types
of common IVC dysplasia jointly form the complex cases (16).
Considering that a retrocaval ureter directly causes
a serious left ureteral obstruction (17), more studies on this type of IVC
dysplasia are available. In addition, other types of IVC dysplasia
pose important clinical significance. Given the significant
incidence of this condition, a better and complete interpretation
of images is beneficial. Avoiding the misinterpretation of this
condition as retroperitoneal lymph-adenopathy (18), urinary system abnormality, bossing
or as another vessel is advantageous for understanding the various
types of common IVC dysplasia and to master their imaging
manifestations, particularly by CT and magnetic resonance imaging
cross-sectional images. Although vasography confirms IVC dysplasia,
this method is generally not considered as a diagnostic means.
Surgeries via the IVC, including a variety of cardiovascular
interventions and implantation of an IVC filter, require surgeons
to be familiar with a variety of developmental anomalies. For
vascular and general surgeons, as well as urologists, who are
involved in the retroperitoneal region, identifying these
conditions is necessary to prepare the corresponding surgery plan
prior to surgery to prevent intra-operative misjudgement. In
addition, IVC dysplasia changes the normal blood backflow route and
possibly causes DVT (19). As the
aorta stresses the left renal vein towards the lumbar vertebra, the
retroaortic left renal vein may cause a left renal vein backflow
disorder to induce haematuria, namely the posterior nutcracker
syndrome (20).
References
|
1.
|
Abernethy J and Banks J: Account of two
instances of uncommon formation in the viscera of the human body.
Philos Trans R Soc Lond. 83:59–66. 1793.
|
|
2.
|
Moore KL and Persaud TV: The
cardiovascular system. The Developing Human: Clinically Oriented
Embryology. 8th edition. Saunders Elsevier; London: pp. 285–336.
2008
|
|
3.
|
Bass JE, Redwine MD, Kramer LA, Huynh PT
and Harris JH Jr: Spectrum of congenital anomalies of the inferior
vena cava: cross-sectional imaging findings. Radiographics.
20:639–652. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Fitoz S and Yalcinkaya F: Compression of
left inferior vena cava: a form of nutcracker syndrome. J Clin
Ultrasound. 36:101–104. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Cao Avellaneda E, Server Pastor G, López
López AI, et al: Non obstructive retrocaval ureter. Actas Urol Esp.
29:107–109. 2005.(In Spanish).
|
|
6.
|
Mano A, Tatsumi T, Sakai H, et al: A case
of deep venous thrombosis with a double inferior vena cava
effectively treated by suprarenal filter implantation. Jpn Heart J.
45:1063–1069. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Sartori MT, Zampieri P, Andres AL,
Prandoni P, Motta R and Miotto D: Double vena cava filter insertion
in congenital duplicated inferior vena cava: a case report and
literature review. Haematologica. 91(Suppl 6): ECR302006.PubMed/NCBI
|
|
8.
|
Evans JC, Earis J and Curtis J: Thrombosed
double inferior vena cava mimicking paraaortic lymphadenopathy. Br
J Radiol. 74:192–194. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Zhang L, Yang G, Shen W and Qi J: Spectrum
of the inferior vena cava: MDCT findings. Abdom Imaging.
32:495–503. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Gupta A, Naik N and Gulati GS: Mesoaortic
entrapment of a left inferior vena cava. Indian J Radiol Imaging.
20:63–65. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Ng WT and Ng SS: Double inferior vena
cava: a report of three cases. Singapore Med J. 50:211–213.
2009.
|
|
12.
|
Saito T, Watanabe M, Kojima T, et al:
Successful blood sampling through azygos continuation with
interrupted inferior vena cava. A case report and review of the
literature. Int Heart J. 52:327–330. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Rathod K, Ahmed N and Raut A: Circumaortic
renal collar. J Postgrad Med. 50:77–78. 2004.
|
|
14.
|
Karaman B, Koplay M, Ozturk E, et al:
Retroaortic left renal vein: multidetector computed tomography
angiography findings and its clinical importance. Acta Radiol.
48:355–360. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Bagheri F, Pusztai C, Szántó A, et al:
Laparoscopic repair of circumcaval ureter: one-year follow-up of
three patients and literature review. Urology. 74:148–153.
2009.PubMed/NCBI
|
|
16.
|
Köz C, Yokuşoğlu M, Taşar M, Ors F and
Genç C: Complex congenital anomalies of superior vena cava and
pulmonary veins with left-sided inferior vena cava. Anadolu
Kardiyol Derg. 8:223–225. 2008.PubMed/NCBI
|
|
17.
|
Basok EK, Yildirim A and Tokuc R: Type I
and II circumcaval ureter in children: experience in three cases.
Adv Ther. 25:375–379. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Amezyane T, Bassou D, Ghafir D and Ohayon
V: Double inferior vena cava mimicking lymphadenopathy. Ann Saudi
Med. 31:6332011. View Article : Google Scholar
|
|
19.
|
Chee Y, Culligan D and Watson H: Inferior
vena cava malformation as a risk factor for deep venous thrombosis
in the young. Br J Haematol. 114:878–880. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Lee JH and Kim GJ: Significant proteinuria
caused by posterior nutcracker phenomenon. J Korean Soc Pediatr
Nephrol. 14:84–88. 2010. View Article : Google Scholar
|