Introduction
Calculus in diverticulum of the bladder is a rare
clinical disease. In elderly males, secondary bladder diverticula
often occur in the bottom of the bladder or the upper back of the
bilateral trigone (1–3). As there is an angle between the body
of a cystoscope or ureteroscope and the diverticulum, the stones
are difficult to remove by transurethral endoscopic lithotripsy.
Consequently, open surgery is often performed to remove the stones,
leading to greater surgical trauma (4). In the present study, percutaneous
cystostomy with ureteroscopic pneumatic lithotripsy was performed
on six elderly male patients with calculi in bladder diverticula
between 2005 and 2011 and the effectiveness of the treatment was
investigated.
Materials and methods
General data
Six elderly male patients with calculi in bladder
diverticula were enrolled in the present study. The patients were
aged 56–80 years, with an average age of 71 years. There were 1–5
stones in each patient (average, 2.3 stones). The average diameter
of the stones was 1.63±0.72 cm. Three patients were preoperatively
diagnosed with bladder diverticula combined with diverticular
stones. One patient was preoperatively diagnosed, using kidney,
ureter and bladder X-ray (KUB), with bladder stones, which are not
detected by transurethral lithotripsy. The diverticular stones were
confirmed by ultrasound or X-ray examination. Two patients were
diagnosed with a combination of prostatic hyperplasia, bladder
stones and bladder diverticula. During transurethral lithotripsy,
the stones moved to the diverticulum and could not be removed.
Consequently, percutaneous cystostomy was performed. Transurethral
resection of the prostate (TURP) was simultaneously performed on
four patients. The patients were treated in the Department of
Minimally Invasive Surgery, Shishi City Hospital, Shishi, China.
The study was approved by the ethics committee of Shishi City
Hospital. Written informed patient consent was obtained from the
patient.
Apparatus and materials
The apparatus and materials used were as follows:
APL-II intracavity perfusion pump, APL pneumatic lithotripsy
machine (EMS Electro Medical Systems SA, Nyon, Switzerland), Wolf
8/9.8 F ureteroscope (Richard Wolf GmbH, Knittlingen, Germany),
Cook fascial dilator (F8–F22) (Cook Medical, Bloomington, IN, USA),
18G renal puncture needle, Urovision 0.035-inch zebra guidewire and
Peel-Away sheath (F16–F22) (Urovision GmbH, Bad Aibling,
Germany).
Surgical methods
Under epidural anesthesia, the modified lithotomy
position (head elevation, 15°) was used for surgery. The
nephrostomy bag was fixed at the pubis position. The stones were
not successfully removed by transurethral ureteroscopic
lithotripsy, so percutaneous cystostomy was performed. After
filling the bladder with saline, an 18G renal puncture needle was
used to puncture the bladder 1–2 cm above the pubic symphysis. The
puncture needle core then was drawn, leading to the appearance of a
flow of urine, and a zebra guidewire was then inserted. A skin
incision of 0.5–0.6 cm was made along the puncture needle and the
fascial dilator was then used to gradually expand the incision to
F18 (F22 for stones too large for F18) along the guidewire. The
Peel-Away sheath was positioned to construct a stone removal
passage. The Wolf 8/9.8 F ureteral endoscope was placed in the
diverticulum and pneumatic lithotripsy was performed. The small
stones were flushed out through the Peel-away sheath using saline
perfusion and the larger stones were removed with lithotomy
forceps. After all the stones had been removed, the F14 balloon
urinary catheter was retained as a cystostomy tube. For patients
also suffering from prostate hyperplasia, TURP was performed
simultaneously. Postoperative ultrasound or X-ray examination was
performed. Finally, the cystostomy tube and urinary catheter were
removed simultaneously.
Results
The stones were successfully removed from all
patients, with no complications such as bladder perforation,
rupture, urethritis or cystitis. The surgery time was 15–60 min,
with an average time of 32 min. Postoperative ultrasound or X-ray
examination showed no stone residues. During the 3–24-month
follow-up (average, 16 months), all patients had unobstructed
urination, with no urethral stricture and no recurrent stones were
detected.
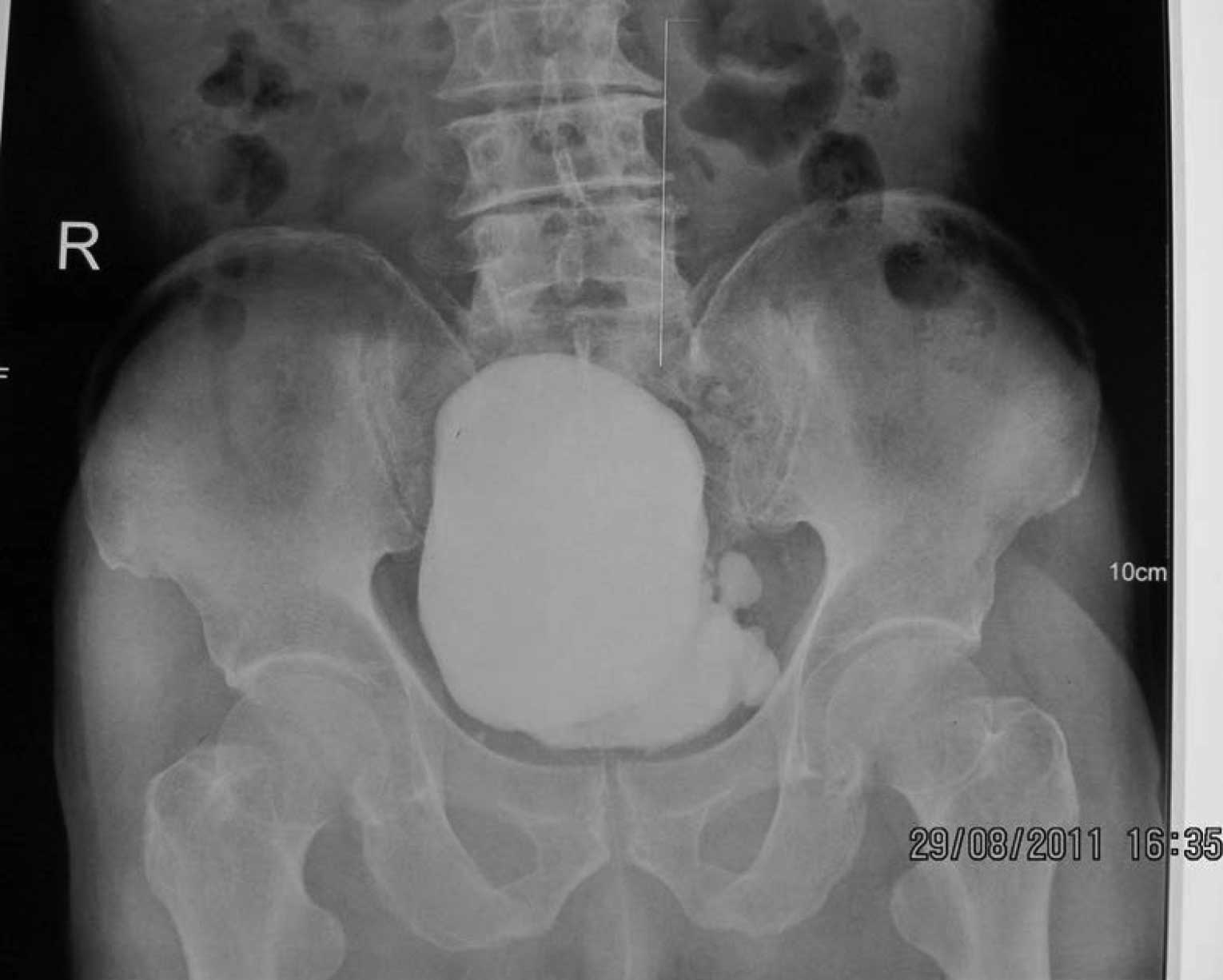
Typical case 1
The patient, a 70-year-old male, was treated for
gross hematuria accompanied by voiding difficulty for two months
and was examined with ultrasound and KUB, which revealed a bladder
diverticulum with bladder calculus (three calculi). The patient was
treated with minimally invasive percutaneous cystostomy with
ureteroscopic pneumatic lithotripsy. After surgery, the urination
of the patient was smooth and no gross hematuria was observed.
Fig. 1 shows the
preoperative KUB of the patient with diverticular bladder calculus
which indicated that multiple calculi existed in the bladder. In
addition, the preoperative radiography results of the patient
indicated that the diverticulum existed at the top on the left
lateral wall of the bladder (Fig.
2). The postoperative pelvic X-ray results of the patient
indicated that the calculi in the bladder diverticulum and bladder
had been completely removed (Fig.
3).
Discussion
A bladder diverticulum is a hernia formed by
urothelium penetration into the muscularis propria of the bladder
wall. It is caused by the protrusion of the bladder wall from the
bundle of detrusor muscle in the bladder due to congenital bladder
wall weakness, lower urinary tract obstructions and increased
intravesical pressure. Bladder diverticula are divided into
congenital and secondary types. Congenital bladder diverticula
often occur in male children, with an incidence of ∼1.7% (1–3) and
are usually beside or behind the ureteral orifice. These
diverticula are mostly large and solitary. As observed by an
endoscope, they are located at the smooth bladder wall, with no
evident trabeculation. Secondary bladder diverticula mostly occur
in elderly males (>60 years), with an incidence of 1–6% in
patients with a history of prostatic hyperplasia (1). Bladder outlet obstruction and
urethral stricture induced by prostatic diseases are the main
causes of these diverticula. There are often multiple diverticula,
with evident trabeculation under a cystoscope. Iatrogenic factors
may also cause a bladder diverticulum to form. The insufficient
closure of a muscle layer after bladder incision may lead to
weakening of the suture position, resulting in bladder diverticulum
formation. In addition, lower extremity venous congestion may also
result in bladder diverticulum formation (4,5).
Calculus in diverticulum of the bladder is reported
less often in the clinic, particularly for treatment using
minimally invasive endoscopic lithotripsy. There is no significant
clinical manifestation of this disease, although urinary infection,
hematuria and prostatic hyperplasia are clinical symptoms. This
disease may be incidentally detected in B-scan ultra-sonography,
KUB and cystoscopic examination. Calculus in diverticulum of the
bladder may be diagnosed due to inguinal hernia caused by the
bladder diverticulum and spontaneous bladder diverticulum rupture
(6–9). In the present study, three cases were
treated due to hematuria and the bladder diverticulum stones were
confirmed by preoperative KUB, ultrasound examination and
cystoscopy. One case was preoperatively diagnosed with bladder
stones, which are not detected by transurethral lithotripsy and the
diverticular stones were confirmed by ultrasound or X-ray
examination. The remaining two cases had a combination of prostatic
hyperplasia, bladder stones and secondary bladder diverticula.
During transurethral lithotripsy, the stones moved to the
diverticulum and could not be removed.
Congenital and secondary bladder diverticula do not
require treatment if there are no clinical symptoms. Otherwise,
diverticulum resection should be performed. For certain patients
with a bladder diverticulum, intradiverticular urine retention,
urinary salt deposition, infection and chronic inflammatory stimuli
lead to the formation of diverticular stones, resulting in symptoms
such as repeated stimulation, obstruction and even carcinogenesis
(10–12). Consequently, bladder diverticulum
stones should be removed as quickly as possible. For patients in
whom prostatic hyperplasia is the cause of the diverticulum and
stones, the prostatic obstruction should be treated simultaneously.
This contributes to the treatment of secondary bladder diverticula
and prevents stone occurrence (13,14).
Bladder diverticulum stones are usually removed by
open surgery, with the occasional use of laparoscopic diverticulum
excision (5,15,16).
Open surgery not only causes larger surgical trauma, but also
results in complications such as ureteral injury and stricture. In
addition, other complications, such as urinary tract infection,
bleeding, postoperative urinary extravasation, urinary fistula and
intestinal injury, may not be completely avoided. Among elderly
male patients, the bladder diverticulum often occurs in the bottom
of the bladder or the upper back of the bilateral trigone. As there
is an angle between the body of a cystoscope or ureteroscope and
the diverticulum, the stones are difficult to remove by
transurethral ureteroscopic lithotripsy. Consequently, open surgery
is often performed.
In the present study, the principle of minimally
invasive percutaneous nephrostomy technology was investigated.
Minimally invasive percutaneous cystostomy was used to treat
bladder diverticulum stones and a satisfactory result was obtained.
According to the present results and associated literature
(6,14,15),
the reported experiences of percutaneous cystostomy with
ureteroscopic pneumatic lithotripsy are as follows (14,15,17,18):
i) The distance between the bladder stoma and bladder cavity is
short and straight and a ureteroscope may easily pass in and out
the bladder, with no angle between the ureteroscope body and
diverticulum. Consequently, the stones are easily identified and
removed; ii) the placement of a Peel-Away sheath maintains the low
intravesical pressure, avoiding urinary extravasation and bladder
rupture. Simultaneous TURP reduces the associated syndromes; iii)
the stone removal and crushing are performed simultaneously under
saline perfusion, which shortens the surgery time; iv) larger
bladder stones may be simultaneously treated; v) this procedure
does not have high equipment requirements and may be performed in
hospitals with pneumatic lithotripsy, ultrasonic lithotripsy or
holmium laser lithotripsy machines. vi) for certain high-risk
patients without anesthetic tolerance, this surgery may be
performed under conditions of basal anesthesia combined with local
infiltration anesthesia; vii) this procedure has advantages of
simple surgery, a short learning curve and a wide application
range.
Minimally invasive percutaneous cystostomy with
ureteroscopic pneumatic lithotripsy is a safe, efficient and easy
treatment for calculi in bladder diverticula. This method provides
a new clinical approach for lithotripsy and we suggest that it is
worthy of wider use.
Acknowledgements
This study was supported by the
Project of Shishi City Science and Technology Bureau (No. 2011SN28)
and Project of Quanzhou City Health Bureau.
References
|
1.
|
Hansel DE, Paner GP, Nese N and Amin MB:
Limited smoothelin expression within the muscularis mucosae:
validation in bladder diverticula. Hum Pathol. 42:1770–1776. 2011.
View Article : Google Scholar
|
|
2.
|
Bogdanos J, Paleodimos I, Korakianitis G,
et al: The large bladder diverticulum in children. J Pediatr Urol.
1:267–272. 2005. View Article : Google Scholar
|
|
3.
|
Garat JM, Angerri O, Caffaratti J, et al:
Primary congenital bladder diverticula in children. Urology.
70:984–988. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Matlaga BR, Kim SC, Watkins SL, et al:
Pre-percutaneous nephrolithotomy opacification for caliceal
diverticular calculi. J Endourol. 20:175–178. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Miller M, Baker LA, Tannin G and Koral K:
Lower extremity venous obstruction secondary to congenital bladder
diverticulum. J Urol. 177:18912007. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Bittle MM, Gunn ML, Gross JA and Rohrmann
CA: Imaging of duodenal diverticula and their complications. Curr
Probl Diagn Radiol. 41:20–29. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Powell CR and Kreder KJ: Treatment of
bladder diverticula, impaired detrusor contractility, and low
bladder compliance. Urol Clin North Am. 36:511–525. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Fuerxer F, Brunner P, Cucchi JM, et al:
Inguinal herniation of a bladder diverticulum. Clin Imaging.
30:354–356. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Stein RJ, Matoka DJ, Noh PH and Docimo SG:
Spontaneous perforation of congenital bladder diverticulum.
Urology. 66:8812005. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Corbett HJ, Talwalker A, Shabani A and
Dickson AP: Congenital diverticulum of the bladder mimicking
tumour. J Pediatr Urol. 3:323–325. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Goljanin D, Yossepowitch O, Beck SD, et
al: Carcinoma in a bladder diverticulum: presentation and treatment
outcome. J Urol. 170:1761–1764. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Moinzadeh A, Latini J and Hamawy KJ: Clear
cell adenocarcinoma of the urinary bladder within a diverticulum.
Urology. 62:1452003. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Shah HN, Shah RH, Hegde SS, et al:
Sequential holmium laser enucleation of the prostate and
laparoscopic extraperitoneal bladder diverticulectomy: initial
experience and review of literature. J Endourol. 20:346–350. 2006.
View Article : Google Scholar
|
|
14.
|
Al-Basam S, Bennett JD, Layton ZA, et al:
Treatment of caliceal diverticular stones: transdiverticular
percutaneous nephrolithotomy with creation of a neoinfundibulum. J
Vasc Interv Radiol. 11:885–889. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Thiel DD, Young PR, Wehle MJ, et al:
Robotic-assisted bladder diverticulectomy: tips and tricks.
Urology. 77:1238–1242. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Juan YS, Li CC, Shen JT, et al:
Laparoscopic bladder diverticulectomy for large bladder
diverticulum: a case report. Kaohsiung J Med Sci. 20:563–566. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
M Ndez-Probst CE, Fuller A, Nott L, et al:
Percutaneous nephrolithotomy of caliceal diverticular calculi: a
single center experience. J Endourol. 25:1741–1745. 2011.PubMed/NCBI
|
|
18.
|
Tzeng BC, Wang CJ, Huang SW and Chang CH:
Doppler ultrasound-guided percutaneous nephrolithotomy: a
prospective randomized study. Urology. 78:535–539. 2011. View Article : Google Scholar : PubMed/NCBI
|