Introduction
In most of the world, high-risk human papilloma
viruses (HPVs), particularly HPV16, are the cause of a rapidly
growing subset of oropharyngeal squamous cell carcinomas (OPSCCs)
mostly located in the tonsils and arising from the crypt epithelium
of the palatine and lingual tonsils (1-3).
These types of cancer differ markedly from those traditionally
induced by tobacco and alcohol abuse, particularly at the
biological level (4,5). Specifically, patients with
HPV-positive head and neck squamous cell carcinoma (HNSCC) have a
survival advantage over their HPV-negative counterparts (6-11).
However, HPV-positive OPSCC exhibits significant geographical
variations in the incidence rate among patients who are smokers,
and the evaluation of the smoking status is not uniform among a
series of OPSCC patients (6-8,12,13).
Thus, tobacco use may be a confounding factor in HPV-positive
patients with a history of smoking (11,14)
and may explain their significantly increased risk of oncological
failure (7,8,15-18).
The process of tumor transformation from dysplasia into an invasive
tumor involves a number of molecular abnormalities. In HNSCC, these
abnormalities result from chromosomal instability rather than
microsatellite instability (5). If
smoking and HPV are distinct risk factors for OPSCC (19), then the nature of the interaction
between these two risk factors in mediating HNSCC development
remains unclear. As regards the tobacco smoking status, tobacco
smoking synergistically increases the risk of HPV-associated OPSCC
(19,20); however, the mechanisms through
which smoking can biologically affect the development of
HPV-related OPSCC remain unclear.
In terms of chromosomal activity, tobacco and HPV
may act as either synergistic or competitive factors: Tobacco use
may increase chromosomal instability, although the rate of
chromosomal alterations is low in HPV-induced cancer, with a higher
incidence of the wild-type genome. As regards HPV-induced HNSCC,
the HPV16 oncoproteins E6 and E7 have been shown to independently
cause structural and numerical chromosomal instability (21,22)
by inducing centrosome abnormalities and potentially decreasing the
G2-M checkpoint response (4).
Nevertheless, in vitro experiments have demonstrated that
HPV16 is a high-risk HPV that induces one of the lowest rates of
chromosomal copy number alterations (CNAs) following keratinocyte
immortalization (23). By
increasing chromosomal instability and promoting DNA breaks in
HPV-positive OPSCC, tobacco smoking may increase HPV integration at
fragile sites or 'hotspots' of DNA breakage, which may modify
pathways leading to cellular transformation in HPV-positive
patients with a previous or current smoking status compared to
HPV-positive patients who have never smoked. Mooren et al
(24) analyzed chromosome
stability in 77 tonsillar squamous cell carcinoma samples via
fluorescence in situ hybridization (FISH). This team studied
imbalances in the copy number ratios of chromosomes 1 and 7, as
CNAs in these two chromosomes had been detected by FISH in previous
studies on head and neck (pre)malignancies (25,26).
The authors correlated the chromosome copy number with the HPV16
status and clinicoepidemiological profiles. Other array-based
comparative genomic hybridization (aCGH) have studies investigated
chromosomal instability in OPSCC according to HPV status, but none
to date have considered smoking status (27-29),
at least to the best of our knowledge.
Therefore, patients with OPSCC with a low rate of
genomic alterations for whom efforts to deescalate treatment would
be justified, must be differentiated from patients with other
HPV-positive OPSCCs resulting from more complex biological drivers,
specifically, those due to tobacco/alcohol exposure, for whom
conventional treatments would be continued. Thus, this study aimed
to evaluate chromosomal instability in patients with OPSCC who are
HPV-positive based on smoking status by comparing a group of
patients with a strict non-smoking history with a group of patients
with HPV-positive OPSCC and a past or present history of smoking
regardless of the level of tobacco abuse.
Materials and methods
Patient samples
Tumor samples from 50 patients with OPSCC were
retrieved from the Tenon Hospital tissue bank between July, 2008
and July, 2016. All samples were collected prior to treatment.
These samples were fresh-frozen tumor specimens (stored at −80°C).
The medical files of each patient, including clinical and
pathological reports, were prospectively analyzed by the
investigators. The study criteria were as follows: A histological
diagnosis of OPSCC; the collection of tumor samples before
treatment; and the availability of clinicoepidemiological data, HPV
status and tobacco use data. Patients were considered non-tobacco
smokers if their past consumption was fewer than 100 cigarettes
according to the definition of the American National Health
Interview Survey (NHIS). TNM classification and tumor stage were
assessed according to the 8th edition of the American Joint
Committee on Cancer (AJCC)/Union for International Cancer Control
(UICC) staging manual. A separate algorithm for high-risk
HPV-associated cancer (distinguishing this etiology from other
causes) is one of the major changes in this recent classification
(30). Tumors were considered
HPV-driven if HPV16/18 DNA was identified in combination with p16
protein overexpression or E6/E7 mRNA identification. Our
institutional review board (the CEORL, from the French ENT Society)
approved the study protocol, and all patients provided written
informed consent.
DNA extraction
Genomic DNA was isolated using a QIAamp®
DNA Mini kit (Qiagen) according to the manufacturer's instructions
and stored at −4°C.
HPV genotyping
Genomic DNA was isolated using our in-house
protocol. Tumor samples were screened by polymerase chain reaction
(PCR) followed by hybridization using an INNO-LiPA HPV Genotyping
Extra diagnostic assay (Fujirebio Europe N.V.) according to the
manufacturer's instructions.
aCGH
DNA isolated from the specimens was fluorescently
labeled with the cyanine dye Cy5, and control DNA was labeled with
the cyanine dye Cy3 using an Agilent SureTag DNA (Agilent
Technologies) labeling kit according to the manufacturer's
instructions. Labeled products were cohybridized to a PerkinElmer
CGX Oncochip (PerkinElmer) with oligonucleotide coverage targeting
2,410 cancer-relevant regions based on human genome build 19. The
microarray design was a 4×180 Custom SurePrint G3 Human CGHplusSNP
Microarray 4×180K (AMADID 046984). The hybridization design was a
tumor sample versus a systematic commercial normal male reference
(Promega G1471; Thermo Fisher Scientific). The average target
spacing was 1 probe every 2-5 kb, and the average backbone spacing
was 1 probe every 65 kb. CGX oncoarrays also feature backbone
single nucleotide polymorphism (SNP) coverage, affording combined
CGH/SNP results. Arrays were scanned with an Agilent G2539A DNA
Microarray Scanner (Agilent Technologies), and images were
processed with Agilent Feature extraction for CytoGenomics and
Agilent CytoGenomics Edition 2.7.22.0 software (Agilent
Technologies).
Statistical analysis
All data manipulations were performed in the R
environment (v3.4). Raw intensities were normalized according to
their dye composition (Ref/Cy3 fitted over Test/Cy5). The data were
transformed as log2(Test/Ref) and normalized according to the local
GC content through Loess regression. A common 'wave-effect' bias
track was modeled from the 50 normalized profiles using the cghseg
package (v1.0.2-1) (31) and
subtracted from each profile through Loess regression. The
resulting profiles were segmented with the circular binary
segmentation (CBS) algorithm implemented in the DNAcopy package
(v1.42) using the default parameters (32). The segmented profiles were centered
using the most centered of the three most populated peaks in the
smoothed log2(Test/Ref) distribution density. Aberration levels
were called by setting an unsigned log2(Test/Ref) threshold
automatically adapted to the internal noise for each profile, which
was considered one-fourth of the median value of the absolute
differences between consecutive log2(Test/Ref) measurements along
the genome. Differential analysis of CGH profile subpopulations was
performed using a Wilcoxon rank-sum test for two classes or a
Kruskal-Wallis test for more than two classes. The obtained CGH
clusters and categorical clinical annotations were compared using
Fisher's exact test. All P-values were FDR-adjusted using the
Benjamini-Hochberg method. Minimum common regions were identified
using 'region'-level results from GISTIC2 (v2.0.22) with the
default parameters, except for recentering (none performed)
(33). Differences in chromosomal
alterations were considered significant with P-values <0.05.
Differential regions were considered significantly different when
their respective raw P-values were <0.001.
Results
Patient description
Fifty patients with OPSCC treated between July, 2008
and July, 2016 were available for this study. The median age of the
patients was 61 years, and 68% were males (n=34). The main tumor
locations were the tonsils (n=35, 70%) and tongue base (n=11,
22%).
The patients were classified into 4 groups as
follows: Patients who were HPV-positive, with a positive smoking
status (HPV+ smoker+) (n=16); patients who
were HPV-positive, with a non-smoking (HPV+
smoker−) (n=10); patients who were HPV-negative, with a
positive smoking status (HPV− smoker+)
(n=22); and patients who were HPV-negative, with a non-smoking
status (HPV− smoker−) (n=2). The cohort
consisted of patients with locoregionally advanced oropharyngeal
tumors, 16 (32%) who had stage IV disease. The patient
characteristics are presented in Table
I.
 | Table IPatient characteristics. |
Table I
Patient characteristics.
| Patient
characteristics | Number | Percentage |
|---|
| Median age at | 61 | - |
| diagnosis
(years) | | |
| Sex | | |
| Male | 34 | 68 |
| Female | 16 | 32 |
| HPV genotyping | | |
| HPV16 | 24 | 48 |
| HPV33 | 1 | 2 |
| HPV82 | 1 | 2 |
| Negative | 24 | 48 |
| HPV and smoking
status | | |
| HPV+
smoker+ | 16 | 32 |
| HPV+
smoker− | 10 | 20 |
| HPV−
smoker+ | 22 | 44 |
| HPV−
smoker− | 2 | 4 |
| Oropharyngeal
site | | |
| Tonsils | 35 | 70 |
| Tongue base | 11 | 22 |
| Soft palate | 3 | 6 |
| Other | 1 | 2 |
| T
classificationa | | |
| T1 | 6 | 12 |
| T2 | 18 | 36 |
| T3 | 23 | 46 |
| T4a | 3 | 6 |
|
T4b | 0 | 0 |
| N
classificationa | | |
| N0 | 10 | 20 |
| N1 | 23 | 46 |
| N2 | 15 | 30 |
| N3 | 2 | 4 |
| M
classificationa | | |
| M0 | 49 | 98 |
| M1 | 1 | 2 |
| Overall tumor
stagea | | |
| I | 15 | 30 |
| II | 13 | 26 |
| III | 6 | 6 |
| IV | 16 | 32 |
The results of HPV genotyping were as follows: The
majority of the positive cases were HPV16 (n=24), 1 case was HPV33
(an HPV+ smoker+ patient), and 1 case was
HPV82 (an HPV+ smoker+ patient); 24 cases
were HPV-negative.
aCGH data
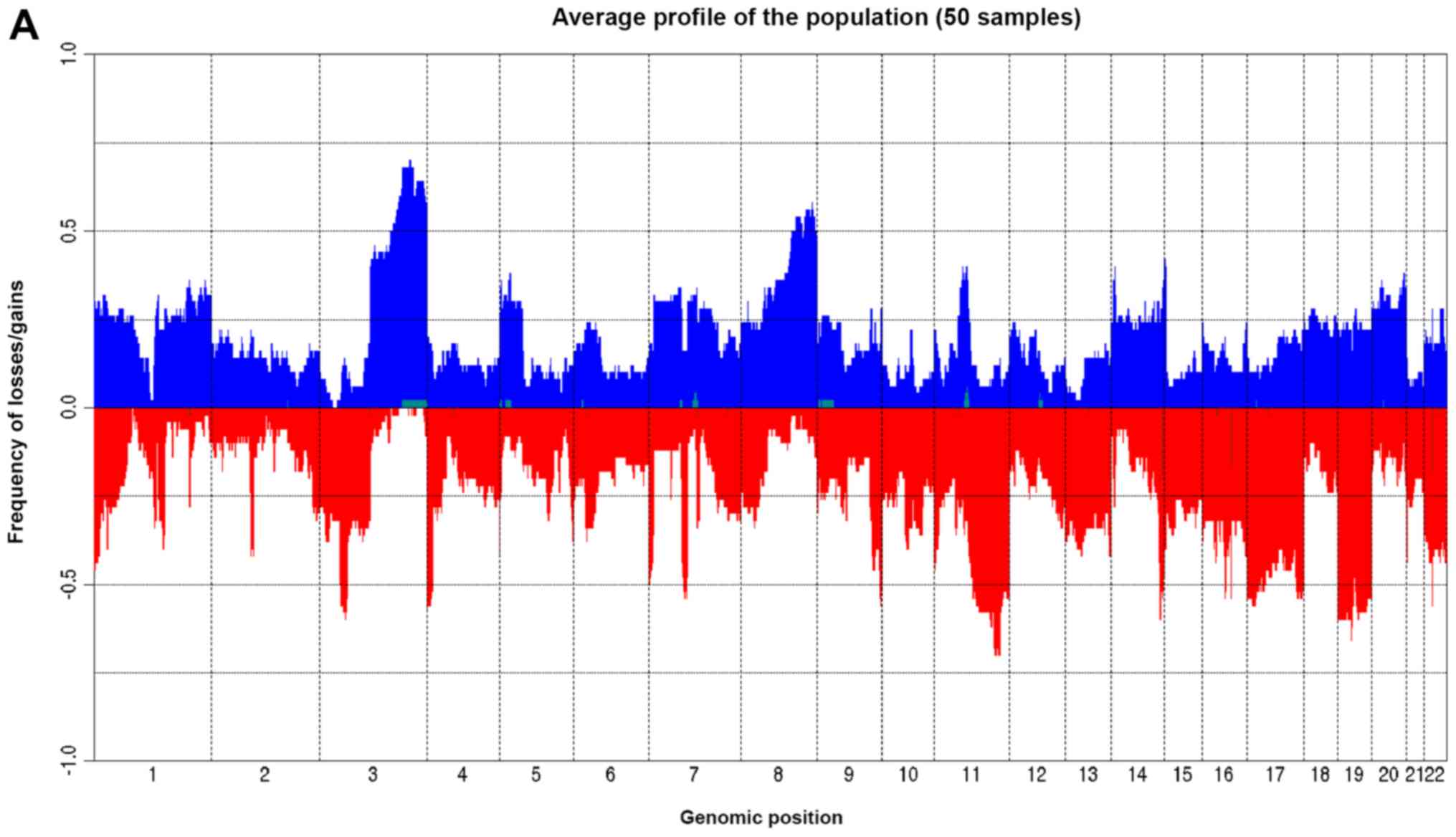
As regards the global aCGH data, acquired genomic
CNAs were detected in all samples. The CNA frequency and summed
alterations are shown in Fig. 1.
The analysis of the minimum common regions (MCRs), which identifies
the regions of limited size most likely to have recurrent genes of
interest, was conducted in all of our patients. A total of 59 MCRs
were identified with 95% confidence (12 gains and 47 losses) and
were distributed across all chromosomes. The gains ranged from 0.15
to 46.4%, and the losses ranged from 0.87 to 65.63%. The percentage
of genomic aberration ranged from 4.06 to 81.67%. The median number
of breakpoints was 79 (range, 34-474). The size of the aberrations
ranged from 7.56 Kb to 35.2 Mb, with a mean of 6.12 Mb (data not
shown).
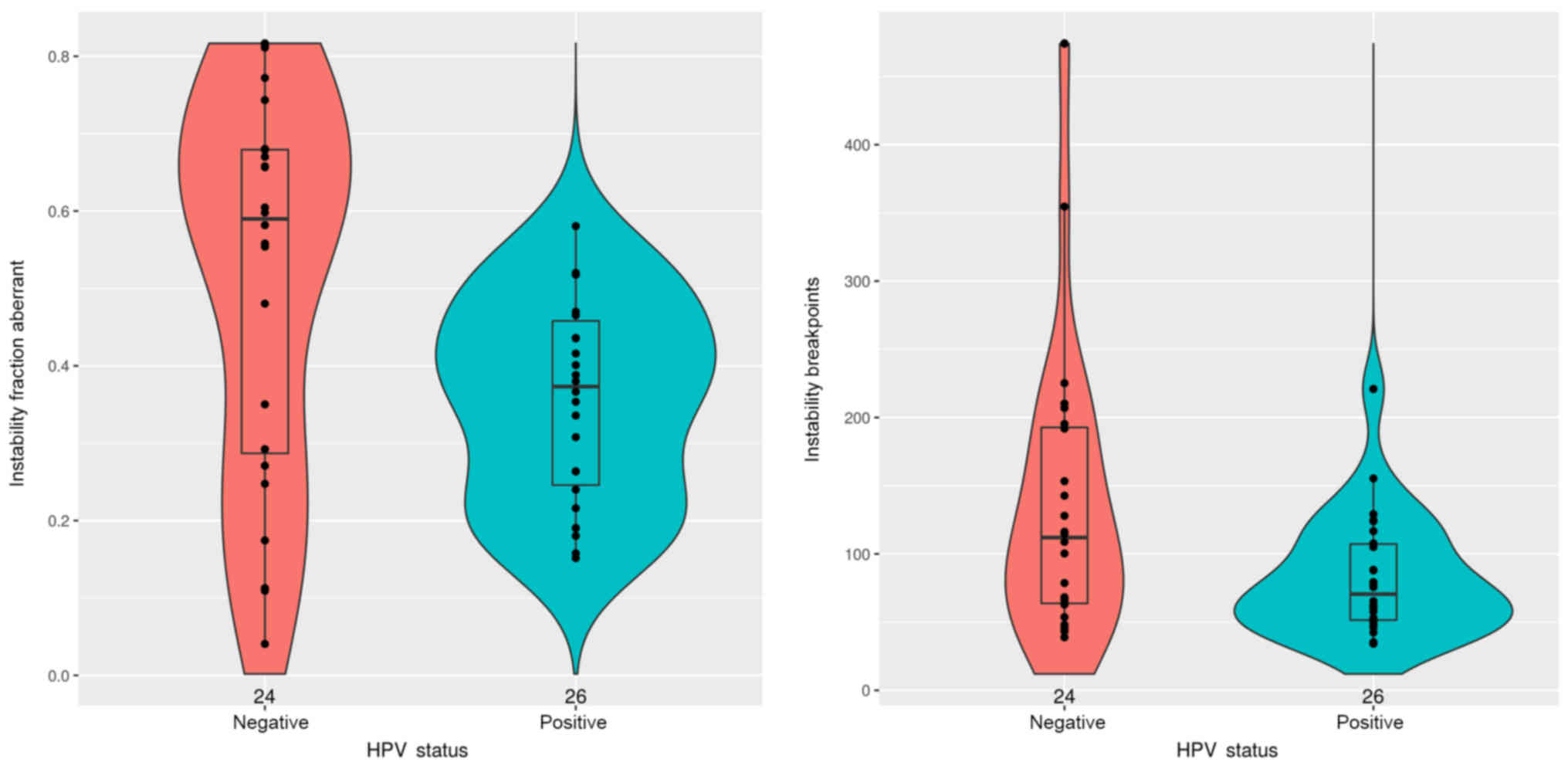
The aCGH results for the number of chromosome
alterations by patient group are shown in Table II and Figs. 2-4. Sex was not significantly associated
with a variation in either chromosome aberration or breakpoint
number (data not shown). A positive HPV status was significantly
associated with reductions in chromosomal aberrations (P=0.0082)
and chromosomal losses (P=0.048). No significant difference was
observed in chromosomal gains as regards the HPV status. In
addition, a positive HPV status was associated with a reduction in
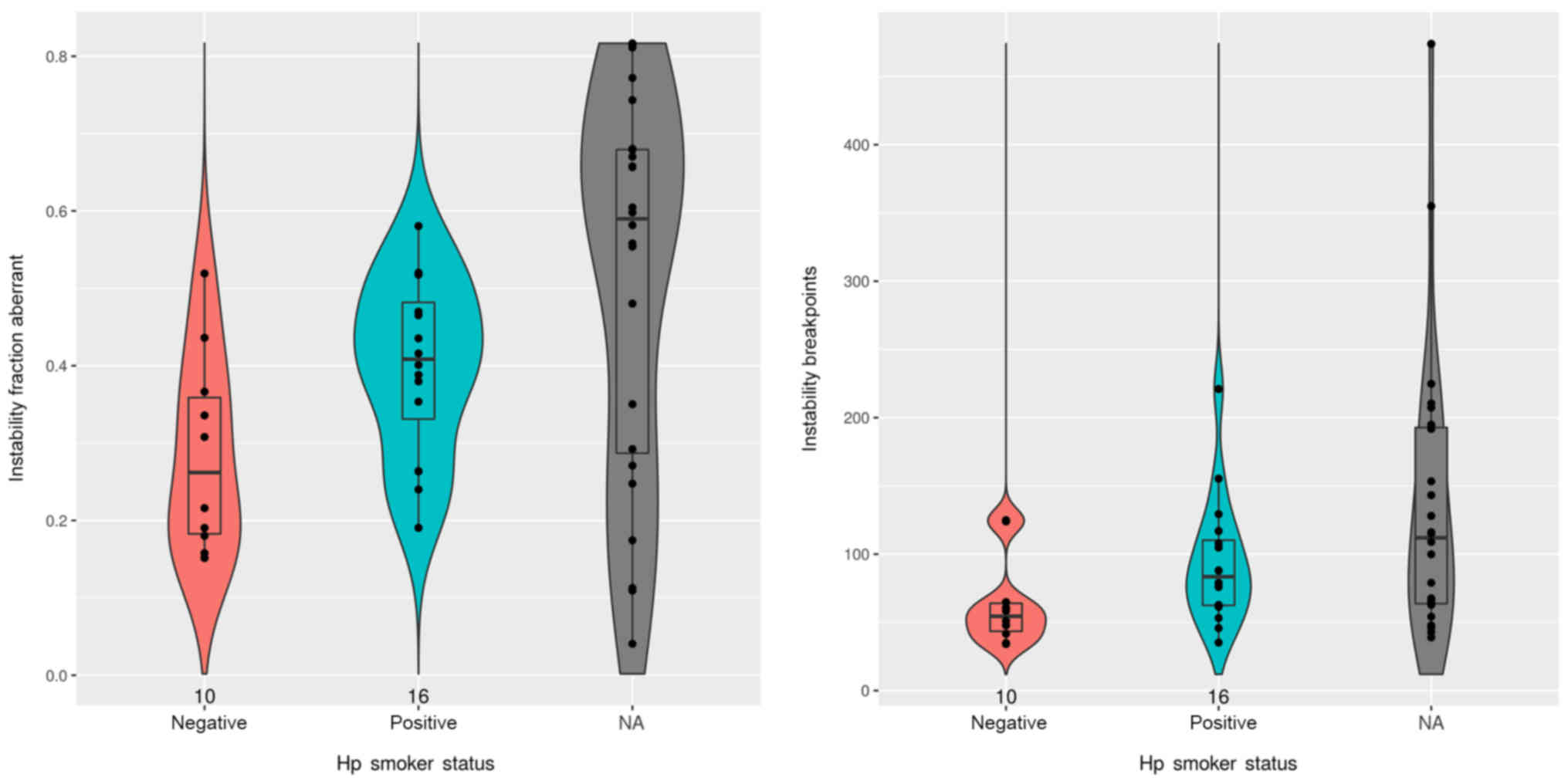
instability breakpoints (P=0.042) (Fig. 2 and Table II). In patients with OPSCC who
were HPV-positive, the total number of chromosomal aberrations per
tumor was significantly lower in the non-smoking patients than in
the smoking patients (P=0.027) (Fig.
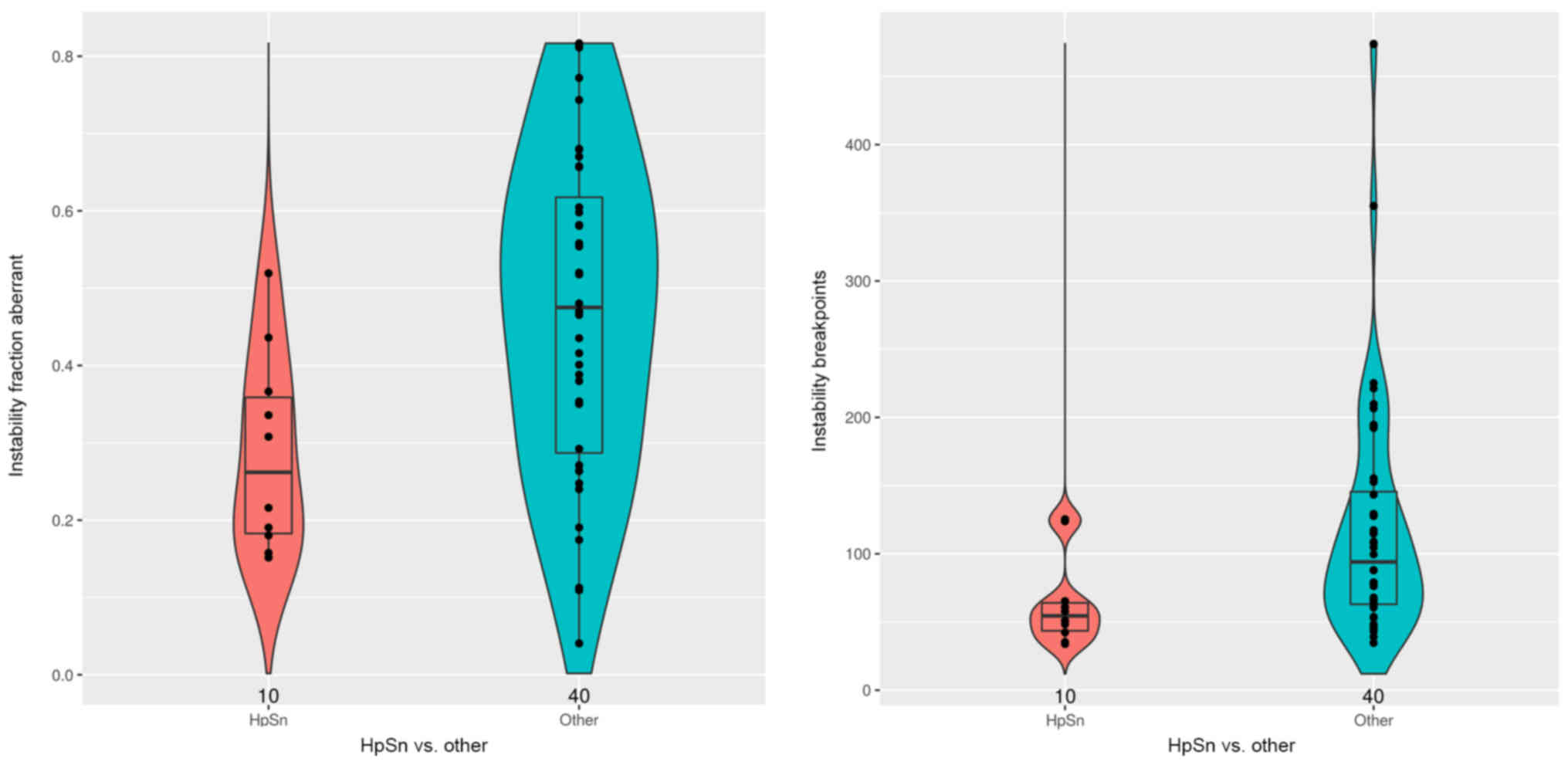
3 and Table II). Furthermore,
patients in the HPV+ smoker− group had
significantly fewer chromosomal gains (P=0.038), genomic
aberrations (P=0.0097) and instability breakpoints (P=0.013) than
their counterparts (HPV+ smoker+,
HPV− smoker− and HPV−
smoker+ patients) (Fig.
4 and Table II).
| Table IIComparison of aberrant genome
fraction and of instability breakpoints according to HPV and
smoking status. |
Table II
Comparison of aberrant genome
fraction and of instability breakpoints according to HPV and
smoking status.
| Annotations | HPV+ vs.
HPV− | HPV+
according to smoking status | HPV+
smoker− vs. others |
|---|
| Chromosomal gain
fraction (median ± SD) | HPV− =
0.20±0.15 | HPV+
smoker− = 0.12±0.088 | HPV+
smoker− = 0.12±0.088 |
| HPV+ =
0.13±0.096 | HPV+
smoker+ = 0.19±0.097 | Others =
0.19±0.13 |
| P=0.050 | P=0.15 | P=0.038 |
| Chromosomal loss
fraction (median ± SD) | HPV− =
0.26±0.16 | HPV+
smoker− = 0.17±0.10 | HPV+
smoker− = 0.17±0.10 |
| HPV+ =
0.19±0.11 | HPV+
smoker+ = 0.20±0.10 | Others =
0.24±0.14 |
| P=0.048 | P=0.36 | P=0.092 |
| Chromosomal
aberration fraction (median ± SD) | HPV− =
0.59±0.25 | HPV+
smoker− = 0.26±0.13 | HPV+
smoker− = 0.26±0.13 |
| HPV+ =
0.37±0.13 | HPV+
smoker+ = 0.41±0.11 | Others =
0.48±0.21 |
|
P=0.0082 | P=0.027 |
P=0.0097 |
| Instability
breakpoints (median ± SD) | HPV− =
112±105 | HPV+
smoker− = 54.50±33.36 | HPV+
smoker− = 54.50±33.40 |
| HPV+ =
70.50±43.70 | HPV+
smoker+ = 83.50±46.41 | Others =
94±88.40 |
| P=0.042 | P=0.054 | P=0.013 |
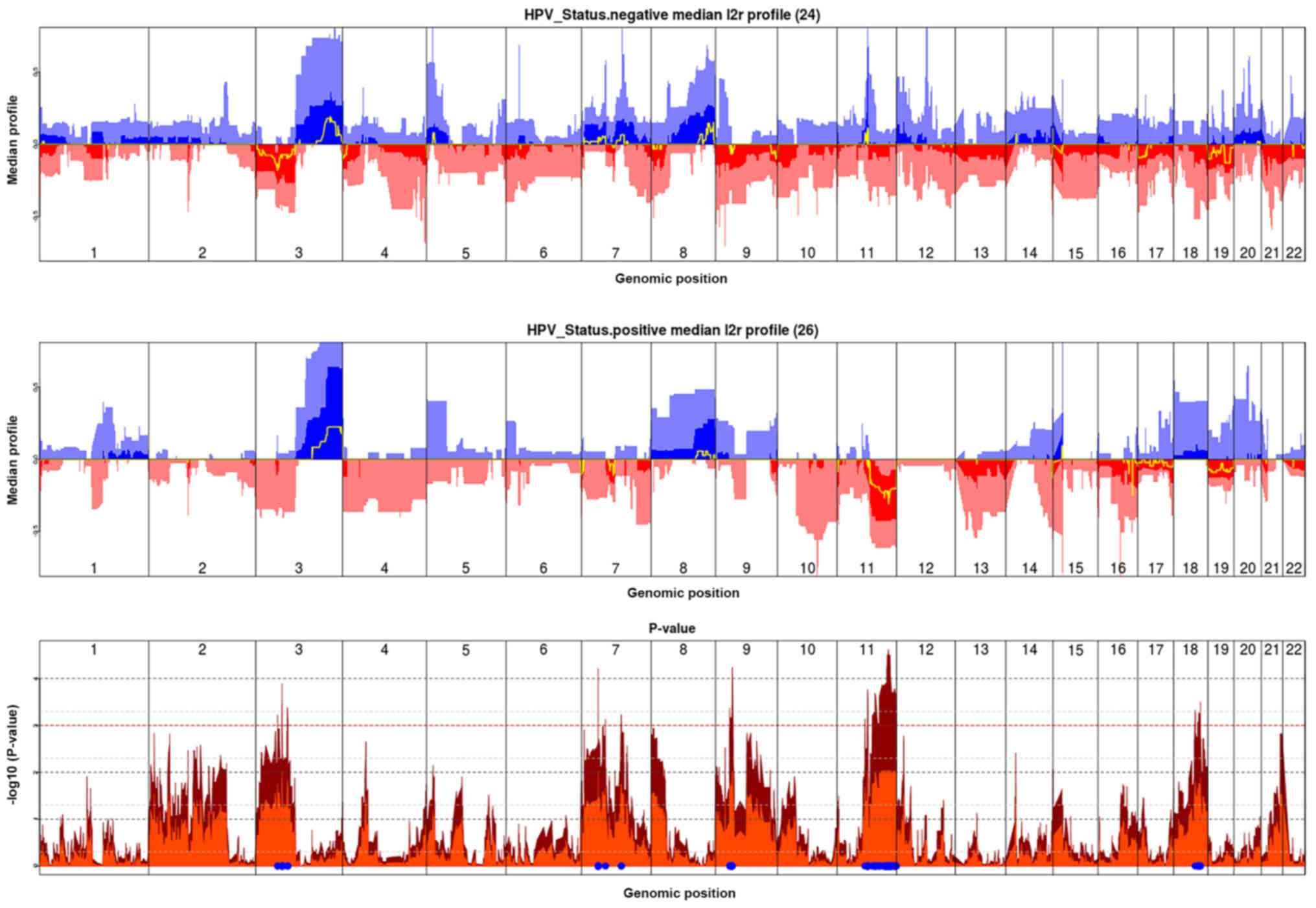
Compared with the patients with HPV-negative tumors,
HPV-positive patients exhibited significant differences at several
chromosomal arms (Fig. 5).
HPV-positive patients had fewer chromosomal losses at 3p (3p13,
3p14 and 3p21) (P<0.03), fewer chromosomal gains at 7p (7p11 and
7p14) (P<0.03), fewer chromosomal gains at 7q21 (P<0.03) and
fewer chromosomal losses at 9p (9p13 and 9p21) (P<0.03).
Furthermore, HPV-positive tumors exhibited more chromosomal gains
at 18q21 (P<0.03).
Many differences in chromosomal aberrations were
observed on chromosome 11: In total, 36 cytobands differed between
the HPV-negative and HPV-positive tumors. HPV-positive tumors had
significantly more losses at some 11q cytobands (11q14, 11q21,
11q22, 11q23, 11q24 and 11q25), while HPV-negative tumors had
significantly more gains at 11q13 (both P<0.03). No difference
was found at the other chromosome arms between HPV-positive and
HPV-negative tumors (data not shown).
Finally, no significant differences were observed in
the various cytobands at these chromosomal arms between the
patients with HPV-positive tumors with a smoking and non-smoking
status (data not shown).
Discussion
The question of whether the confounding factors of
tobacco and/or alcohol abuse can act as cofactors and/or effect
modifiers in either the risk or the etiology of HPV-related OPSCC
remains unanswered. Anantharaman et al (34) demonstrated that smoking was
consistently associated with an increased risk of OPSCC regardless
of the HPV status, suggesting that smoking and HPV16 may act as
independent risk factors. The population-level burden of
HPV-positive oropharyngeal cancers is significantly higher among
ever-smokers than never-smokers in the US, although HPV-related
OPSCC is characterized as a disease of never-smokers due to the
high HPV prevalence in OPSCC cases among never-smokers (35). Therefore, the biological mechanisms
underlying the interrelation between high-risk HPVs, particularly
HPV16, and smoking toxicity can be questioned. To date, three
studies have compared mutations in HPV-driven OPSCCs according to
tobacco consumption (36-38). However, only one of these studies
found statistically significant differences in five mutated genes
between smokers and non-smokers (38). Additional studies with a meaningful
number of genes and a large patient population seem necessary in
order to further describe the mutational landscape of HPV-positive
OPSCC according to the smoking status of patients.
Mooren et al (24) studied chromosomal stability in 77
tonsillar squamous cell carcinomas and found that the disomy of
chromosomes 1 and 7 was associated with HPV16-positive tumors
(P=0.002) and that aneusomies significantly correlated with tobacco
and alcohol consumption (P=0.001 and P=0.016, respectively).
Moreover, the authors observed greater chromosome instability and
poorer prognoses in 13 of 32 HPV-positive patients, 10 of whom were
smokers (24). The authors
recommended that the chromosomal ploidy status should be considered
a prognostic factor in HPV-positive tonsillar squamous cell
carcinoma (24).
Previous aCGH studies have identified differences in
the distributions of DNA gains and losses between HPV-positive and
HPV-negative samples, with more chromosomal alterations in the
HPV-negative samples; however, they did not consider the smoking
history of the patients (27-29).
To the best of our knowledge, this study is the first to use global
aCGH covering 2,410 targeted cancer-relevant regions based on human
genome build 19 in OPSCC considering both the HPV and smoking
statuses of patients. Our aim was to determine whether chromosomal
alterations are more important in HPV-positive OPSCCs for smoking
patients than non-smoking patients and whether these alterations
may be a possible mechanism affecting the prognosis of such
patients. We clearly demonstrated that chromosomal instability is
substantially increased in smoking patients with HPV-positive
OPSCC. HPV-positive tumors have fewer genomic aberrations and
breakpoints than HPV-negative tumors. Furthermore, among the
HPV-positive OPSCC patients, the total number of chromosomal
aberrations per tumor was significantly lower in non-smoking
patients than in smoking patients. As regards the cytobands in the
present study, HPV-negative tumors had significantly more losses at
3p and 9p and gains at 7q and 11q13 than HPV-positive tumors,
confirming the results of previous studies (27-29).
Moreover, we observed that HPV-negative tumors had more chromosomal
gains at 7p. We described 11q losses in patients with HPV-positive
OPSCC, similar to the study of Dahlgren et al (27), and we also described 18q21 gains in
these patients.
This study confirmed that chromosomal alterations
are more important in patients with HPV-positive (particularly
HPV16-positive) OPSCC and a history of smoking. As our data were
not verified by FISH, we cannot exclude the possibility that tri-
or tetraploid tumors with no unbalanced rearrangements appeared
normal. However, no differences were found in the cytobands between
smoking and non-smoking patients with HPV-positive OPSCC.
Nevertheless, we did not identify a clear chromosomal pattern that
could differentiate these two groups of tumors, which may be due to
the random distributions of chromosomal gains and losses or low
discrimination (regarding the number of pack-years or a possible
duration of smoking cessation of longer than ten years) within the
smoking group. Although the association between tobacco abuse and
chromosomal instability has been well established, specifically in
lung cancer (39), the mechanisms
through which smoking induces chromosomal damage remain unclear.
Tobacco smoke contains >60 carcinogens, including polycyclic
aromatic hydrocarbons, aromatic amines and nitrosamines (40). Among these carcinogens, nitrosamine
4-(methynitrosamino)-1-(3-pyridyl)-1-butanone (NKK) and arylamine
4-aminobiphenyl (4-ABP) increase chromosomal instability (41-43).
In addition, cigarette smoke has been shown to suppress the
activity of the Fanconi anemia (FA)/BRCA pathway, which is
essential for the maintenance of chromosomal stability (44). Speculation has arisen regarding the
possible role of smoking abuse in the integration of HPV DNA into
the host genome, specifically by altering DNA breakage hotspots,
for example, common fragile sites.
In conclusion, in this study, we found that
chromosomal instability was more important in patients with
HPV16-positive OPSCC and a history of smoking. This finding may
help to improve the stratification of HPV-positive OPSCC patients,
particularly if these data are complemented by next-generation
sequencing (NGS) studies on large gene panels to establish the
mutational and transcriptomic profiles of these tumors according to
patient smoking status.
Abbreviations:
|
HPV
|
human papilloma virus
|
|
OPSCC
|
oropharyngeal squamous cell
carcinoma
|
|
aCGH
|
array-based comparative genomic
hybridization
|
|
HNSCC
|
head and neck squamous cell
carcinoma
|
|
CNAs
|
copy number alterations
|
|
SNP
|
single nucleotide polymorphism
|
|
DNA
|
deoxyribonucleic acid
|
|
mRNA
|
messenger ribonucleic acid
|
|
FISH
|
fluorescence in situ
hybridization
|
|
NHIS
|
National Health Interview Survey
|
|
AJCC
|
American Joint Committee on Cancer
|
|
UICC
|
Union for International Cancer
Control
|
|
PCR
|
polymerase chain reaction
|
|
MCR
|
minimum common region
|
|
NKK
|
nitrosamine
4-(methynitrosamino)-1-(3-pyridyl)-1-butanone
|
|
4-ABP
|
arylamine 4-aminobiphenyl
|
|
FA
|
Fanconi anemia
|
|
BRCA
|
breast cancer (gene)
|
|
NGS
|
next-generation sequencing
|
Acknowledgments
The authors are grateful for the contribution of
Emmanuel Roux (Tumor Bank Unit and Department of Pathology, Tenon
Hospital, 4 rue de la Chine, 75020 Paris, France) for logistical
support.
Funding
This study was supported by a grant from the
association 'Les amis du Centre des Tumeurs de Tenon' (ACTT), Tenon
Hospital.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article or are available from the
corresponding author on reasonable request.
Author's contributions
AV, RL, JLStG, BB and SA were involved in the
acquisition of the data and the study design. AV, RL, JLStG, BB and
SA were involved in the writing of the manuscript. AV and SH
performed the DNA extraction and aCGH experiments. BJ performed the
statistical analysis. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
This research was performed in accordance with the
Declaration of Helsinki. Our institutional review board (the CEORL,
from the French ENT Society) approved the study protocol, and all
patients provided written informed consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Mork J, Lie AK, Glattre E, Hallmans G,
Jellum E, Koskela P, Møller B, Pukkala E, Schiller JT, Youngman L,
et al: Human papil-lomavirus infection as a risk factor for
squamous-cell carcinoma of the head and neck. N Engl J Med.
344:1125–1131. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Gillison ML and Shah KV: Human
papillomavirus-associated head and neck squamous cell carcinoma:
Mounting evidence for an etiologic role for human papillomavirus in
a subset of head and neck cancers. Curr Opin Oncol. 13:183–188.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kreimer AR, Clifford GM, Boyle P and
Franceschi S: Human papillomavirus types in head and neck squamous
cell carcinomas worldwide: A systematic review. Cancer Epidemiol
Biomarkers Prev. 14:467–475. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Moody CA and Laimins LA: Human
papillomavirus oncoproteins: Pathways to transformation. Nat Rev
Cancer. 10:550–560. 2010. View
Article : Google Scholar : PubMed/NCBI
|
|
5
|
Leemans CR, Snijders PJF and Brakenhoff
RH: The molecular landscape of head and neck cancer. Nat Rev
Cancer. 18:269–282. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lacau St Guily J, Rousseau A, Baujat B,
Périé S, Schultz P, Barry B, Dufour X, Malard O, Pretet JL, Clavel
C, et al Papillophar Group: Oropharyngeal cancer prognosis by
tumour HPV status in France: The multicentric Papillophar study.
Oral Oncol. 67:29–36. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ang KK, Harris J, Wheeler R, Weber R,
Rosenthal DI, Nguyen-Tân PF, Westra WH, Chung CH, Jordan RC, Lu C,
et al: Human papillomavirus and survival of patients with
oropha-ryngeal cancer. N Engl J Med. 363:24–35. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Gillison ML and Restighini C: Anticipation
of the impact of human papillomavirus on clinical decision making
for the head and neck cancer patient. Hematol Oncol Clin North Am.
29:1045–1060. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Posner MR, Lorch JH, Goloubeva O, Tan M,
Schumaker LM, Sarlis NJ, Haddad RI and Cullen KJ: Survival and
human papillo-mavirus in oropharynx cancer in TAX 324: A subset
analysis from an international phase III trial. Ann Oncol.
22:1071–1077. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ragin CC and Taioli E: Survival of
squamous cell carcinoma of the head and neck in relation to human
papillomavirus infection: Review and meta-analysis. Int J Cancer.
121:1813–1820. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wittekindt C, Wagner S, Mayer CS and
Klussmann JP: Basics of tumor development and importance of human
papilloma virus (HPV) for head and neck cancer. GMS Curr Top
Otorhinolaryngol Head Neck Surg. 11:Doc092012.
|
|
12
|
Hong A, Zhang X, Jones D, Veillard AS,
Zhang M, Martin A, Lyons JG, Lee CS and Rose B: Relationships
between p53 mutation, HPV status and outcome in oropharyngeal
squamous cell carcinoma. Radiother Oncol. 118:342–349. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Combes JD, Chen AA and Franceschi S:
Prevalence of human papillomavirus in cancer of the oropharynx by
gender. Cancer Epidemiol Biomarkers Prev. 23:2954–2958. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pytynia KB, Dahlstrom KR and Sturgis EM:
Epidemiology of HPV-associated oropharyngeal cancer. Oral Oncol.
50:380–386. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Huang SH, Xu W, Waldron J, Siu L, Shen X,
Tong L, Ringash J, Bayley A, Kim J, Hope A, et al: Refining
American Joint Committee on Cancer/Union for International Cancer
Control TNM stage and prognostic groups for human
papillomavirus-related oropharyngeal carcinomas. J Clin Oncol.
33:836–845. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Maxwell JH, Kumar B, Feng FY, Worden FP,
Lee JS, Eisbruch A, Wolf GT, Prince ME, Moyer JS, Teknos TN, et al:
Tobacco use in human papillomavirus-positive advanced oropharynx
cancer patients related to increased risk of distant metastases and
tumor recurrence. Clin Cancer Res. 16:1226–1235. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hafkamp HC, Manni JJ, Haesevoets A, Voogd
AC, Schepers M, Bot FJ, Hopman AH, Ramaekers FC and Speel EJ:
Marked differences in survival rate between smokers and nonsmokers
with HPV 16-associated tonsillar carcinomas. Int J Cancer.
122:2656–2664. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Weller MA, Ward MC, Berriochoa C, Reddy
CA, Trosman S, Greskovich JF, Nwizu TI, Burkey BB, Adelstein DJ and
Koyfman SA: Predictors of distant metastasis in human
papillomavirus-associated oropharyngeal cancer. Head Neck.
39:940–946. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Smith EM, Rubenstein LM, Haugen TH,
Hamsikova E and Turek LP: Tobacco and alcohol use increases the
risk of both HPV-associated and HPV-independent head and neck
cancers. Cancer Causes Control. 21:1369–1378. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sinha P, Logan HL and Mendenhall WM: Human
papillomavirus, smoking, and head and neck cancer. Am J
Otolaryngol. 33:130–136. 2012. View Article : Google Scholar
|
|
21
|
Duensing S and Münger K: The human
papillomavirus type 16 E6 and E7 oncoproteins independently induce
numerical and structural chromosome instability. Cancer Res.
62:7075–7082. 2002.PubMed/NCBI
|
|
22
|
Duensing S and Münger K: Mechanisms of
genomic instability in human cancer: Insights from studies with
human papillomavirus oncoproteins. Int J Cancer. 109:157–162. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Schütze DM, Krijgsman O, Snijders PJ,
Ylstra B, Weischenfeldt J, Mardin BR, Stütz AM, Korbel JO, de
Winter JP, Meijer CJ, et al: Immortalization capacity of HPV types
is inversely related to chromosomal instability. Oncotarget.
7:37608–37621. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Mooren JJ, Kremer B, Claessen SM, Voogd
AC, Bot FJ, Peter Klussmann J, Huebbers CU, Hopman AH, Ramaekers FC
and Speel EJ: Chromosome stability in tonsillar squamous cell
carcinoma is associated with HPV16 integration and indicates a
favorable prognosis. Int J Cancer. 132:1781–1789. 2013. View Article : Google Scholar
|
|
25
|
Morrison LE, Jacobson KK, Friedman M,
Schroeder JW and Coon JS: Aberrant EGFR and chromosome 7 associate
with outcome in laryngeal cancer. Laryngoscope. 115:1212–1218.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Veltman JA, Bot FJ, Huynen FC, Ramaekers
FC, Manni JJ and Hopman AH: Chromosome instability as an indicator
of malignant progression in laryngeal mucosa. J Clin Oncol.
18:1644–1651. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Dahlgren L, Mellin H, Wangsa D,
Heselmeyer-Haddad K, Björnestål L, Lindholm J, Munck-Wikland E,
Auer G, Ried T and Dalianis T: Comparative genomic hybridization
analysis of tonsillar cancer reveals a different pattern of genomic
imbalances in human papillomavirus-positive and -negative tumors.
Int J Cancer. 107:244–249. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Klussmann JP, Mooren JJ, Lehnen M,
Claessen SM, Stenner M, Huebbers CU, Weissenborn SJ, Wedemeyer I,
Preuss SF, Straetmans JM, et al: Genetic signatures of HPV-related
and unrelated oropharyngeal carcinoma and their prognostic
implications. Clin Cancer Res. 15:1779–1786. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Jung AC, Briolat J, Millon R, de Reyniès
A, Rickman D, Thomas E, Abecassis J, Clavel C and Wasylyk B:
Biological and clinical relevance of transcriptionally active human
papillomavirus (HPV) infection in oropharynx squamous cell
carcinoma. Int J Cancer. 126:1882–1894. 2010. View Article : Google Scholar
|
|
30
|
Brierley JD, Gospodarowicz MK and
Wittekind C: TNM Classification of Malignant Tumours. 8th edition.
Wiley-Blackwell; New Jersey: pp. p2722017
|
|
31
|
Picard F, Lebarbier E, Hoebeke M, Rigaill
G, Thiam B and Robin S: Joint segmentation, calling, and
normalization of multiple CGH profiles. Biostatistics. 12:413–428.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Olshen AB, Venkatraman ES, Lucito R and
Wigler M: Circular binary segmentation for the analysis of
array-based DNA copy number data. Biostatistics. 5:557–572. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Mermel CH, Schumacher SE, Hill B, Meyerson
ML, Beroukhim R and Getz G: GISTIC2.0 facilitates sensitive and
confident localization of the targets of focal somatic copy-number
alteration in human cancers. Genome Biol. 12:R412011. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Anantharaman D, Muller DC, Lagiou P,
Ahrens W, Holcátová I, Merletti F, Kjærheim K, Polesel J, Simonato
L, Canova C, et al: Combined effects of smoking and HPV16 in
oropharyngeal cancer. Int J Epidemiol. 45:752–761. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Chaturvedi AK, D'Souza G, Gillison ML and
Katki HA: Burden of HPV-positive oropharynx cancers among ever and
never smokers in the U.S. population. Oral Oncol. 60:61–67. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Zevallos J, Yim E, Brennan P, Liu AY,
Taylor JM, Weissler M, Anantharaman D, Abedi-Ardekani B, Olshan AF
and Hayes NN: Molecular profile of human papillomavirus-positive
oropharyngeal squamous cell carcinoma stratified by smoking status.
Int J Radiat Oncol Biol Phys. 94:8642016. View Article : Google Scholar
|
|
37
|
Mirghani H, Lacroix L, Rossoni C, Sun R,
Aupérin A, Casiraghi O, Villepelet A, Lacave R, Faucher G, Marty V,
et al: Does smoking alter the mutation profile of human
papillomavirus-driven head and neck cancers? Eur J Cancer.
94:61–69. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Grønhøj C, Jensen DH, Agander T, Kiss K,
Høgdall E, Specht L, Bagger FO, Nielsen FC and von Buchwald C: Deep
sequencing of human papillomavirus positive loco-regionally
advanced oropha-ryngeal squamous cell carcinomas reveals novel
mutational signature. BMC Cancer. 18:6402018. View Article : Google Scholar
|
|
39
|
Masuda A and Takahashi T: Chromosome
instability in human lung cancers: Possible underlying mechanisms
and potential consequences in the pathogenesis. Oncogene.
21:6884–6897. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Hecht SS: Tobacco carcinogens, their
biomarkers and tobacco-induced cancer. Nat Rev Cancer. 3:733–744.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Hecht SS: Carcinogenicity studies of
inhaled cigarette smoke in laboratory animals: Old and new.
Carcinogenesis. 26:1488–1492. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Herzog CR, Desai D and Amin S: Array CGH
analysis reveals chromosomal aberrations in mouse lung
adenocarcinomas induced by the human lung carcinogen
4-(methylnitrosamino)-1-(3-pyridyl) -1-butanone. Biochem Biophys
Res Commun. 341:856–863. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Saletta F, Matullo G, Manuguerra M, Arena
S, Bardelli A and Vineis P: Exposure to the tobacco smoke
constituent 4-aminobi-phenyl induces chromosomal instability in
human cancer cells. Cancer Res. 67:7088–7094. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Hays LE, Zodrow DM, Yates JE, Deffebach
ME, Jacoby DB, Olson SB, Pankow JF and Bagby GC: Cigarette smoke
induces genetic instability in airway epithelial cells by
suppressing FANCD2 expression. Br J Cancer. 98:1653–1661. 2008.
View Article : Google Scholar : PubMed/NCBI
|