Introduction
Dose-dense (DD) chemotherapy every 2 weeks is
commonly prescribed for patients with high-risk, invasive, operable
breast cancer (1–5). The prophylactic use of pegfilgrastim is
also recommended by consensus guidelines in order to prevent
chemotherapy-induced febrile neutropenia (FN) (1–10). FN is
a potentially life-threatening condition characterized by the
development of fever in addition to chemotherapy-induced
neutropenia. The FN risk may be mitigated by reducing chemotherapy
dosage or extending dosing intervals. However, these measures also
reduce the relative dose intensity of the chemotherapy and,
consequently, survival rates. Therefore, a granulocyte
colony-stimulating factor is often administered to manage
chemotherapy-associated FN and to allow anticancer drugs to be
administered more effectively. Similar efficacy and safety profiles
have been observed in individual studies (11–16)
comparing an average of 11 days of filgrastim treatment with
pegfilgrastim, and a meta-analysis (17,18)
suggested that, overall, pegfilgrastim may be more efficacious
compared with filgrastim. While daily administration of filgrastim
is required, pegfilgrastim is administered as a single
once-per-cycle injection. Based on the convenience and patient
adherence, pegfilgrastim may be preferred to filgrastim for the
prevention of chemotherapy-induced FN. Pegfilgrastim at 3.6 mg is
considered safe and effective for Japanese patients with breast
cancer and has been administered in the country since September
2014 (19,20). Numerous reports have demonstrated
that the prophylactic use of pegfilgrastim is associated with
clinical and economic benefits; however, symptomatic adverse
events, such as bone and back pain and fatigue, are frequently
reported (19,21,22). We
herein report the case of a patient with breast cancer who required
pegfilgrastim dose reduction to 1.8 mg during DD chemotherapy after
experiencing severe fatigue and leukocytosis. Although such
complications are rare, pegfilgrastim dose reduction was effective
in palliating the symptoms and preventing interruption of DD
chemotherapy. Since pegfilgrastim at 3.6 mg was first approved in
Japan, 55 patients with breast cancer who received chemotherapy at
Shiga General Hospital were administered this agent between January
2015 and March 2018, The medical records of all 55 patients were
retrospectively reviewed, and the laboratory data of this patient
were compared with those of the 54 other patients with breast
cancer receiving chemotherapy along with pegfilgrastim.
Case report
A 29-year-old woman presented to the outpatient
clinic of the Department of Breast Surgery at Shiga General
Hospital (Moriyama, Japan) during lactation with a lump in her
right breast. Physical examination revealed a mass ≥2 cm in size
without skin invasion in the upper-lateral region, along with
axillary lymph node enlargement.
Ultrasonography, computed tomography and breast
magnetic resonance imaging revealed a breast mass and axillary
lymph node enlargement on the right side. Core needle biopsy led to
the diagnosis of a high-grade invasive ductal carcinoma that was
triple-negative [for estrogen receptor (ER), progesterone receptor,
and human epidermal growth factor receptor (HER)2]. The Ki-67
labeling index was 80%, basal cytokeratins 5/6 were focally
positive, and androgen receptor was negative (Fig. SI). The tumor was radiologically
classified as cT2N1M0 stage IIB according to the eighth edition of
the Union for International Cancer Control-TNM classification
(23).
The patient was premenopausal and had two children,
and preservation of fertility was not considered necessary. She was
found to be BRCA mutation-negative, and had no history of
other diseases. Thus, preoperative chemotherapy was commenced,
using four cycles of DD-90 mg/m2 epirubicin and 600
mg/m2 cyclophosphamide (EC), followed by four cycles of
DD-75 mg/m2 docetaxel (DTX) every 2 weeks, along with
3.6 mg of pegfilgrastim administered on day 3 of each cycle
(1–5).
Absolute neutrophil count (ANC) was measured at the
start of each cycle and was found to increase gradually (Fig. 1A). The patient also experienced
significant fatigue after each pegfilgrastim injection, worsening
the Eastern Cooperative Oncology Group performance status score
(from 0 to 1) for 3 days. Expert physicians of the cancer board,
comprising breast surgeons, medical oncologists and
pharmacologists, concluded that the patient was highly sensitive to
pegfilgrastim, and recommended decreasing the dose to 1.8 mg on day
3 of the first DD-DTX cycle. Subsequently, on day 1 of the second
DD-DTX cycle, her ANC was reduced slightly to
13,090/mm3. The patient also experienced less fatigue
after the pegfilgrastim dose was halved; however, she still
experienced a significant decline in performance. Given that no
published evidence exists regarding administration of pegfilgrastim
at doses <1.8 mg, it was omitted from the second DD-DTX cycle
onwards. The patient also wished to switch to filgrastim
administration. On day 14, the patient developed viral enteritis
and fever (38°C), with an ANC of 297/mm3. Therefore, the
third cycle of DD-DTX was postponed, and the patient was commenced
on oral levofloxacin (500 mg) for 5 days. The patient's ANC had
recovered to 2,480/mm3 1 week later, and the third cycle
of DD-DTX was initiated, using 3.6 mg of pegfilgrastim on day 3.
The patient still experienced fatigue, albeit milder, due to the
absence of continuous pegfilgrastim administration and lack of
leukocytosis.
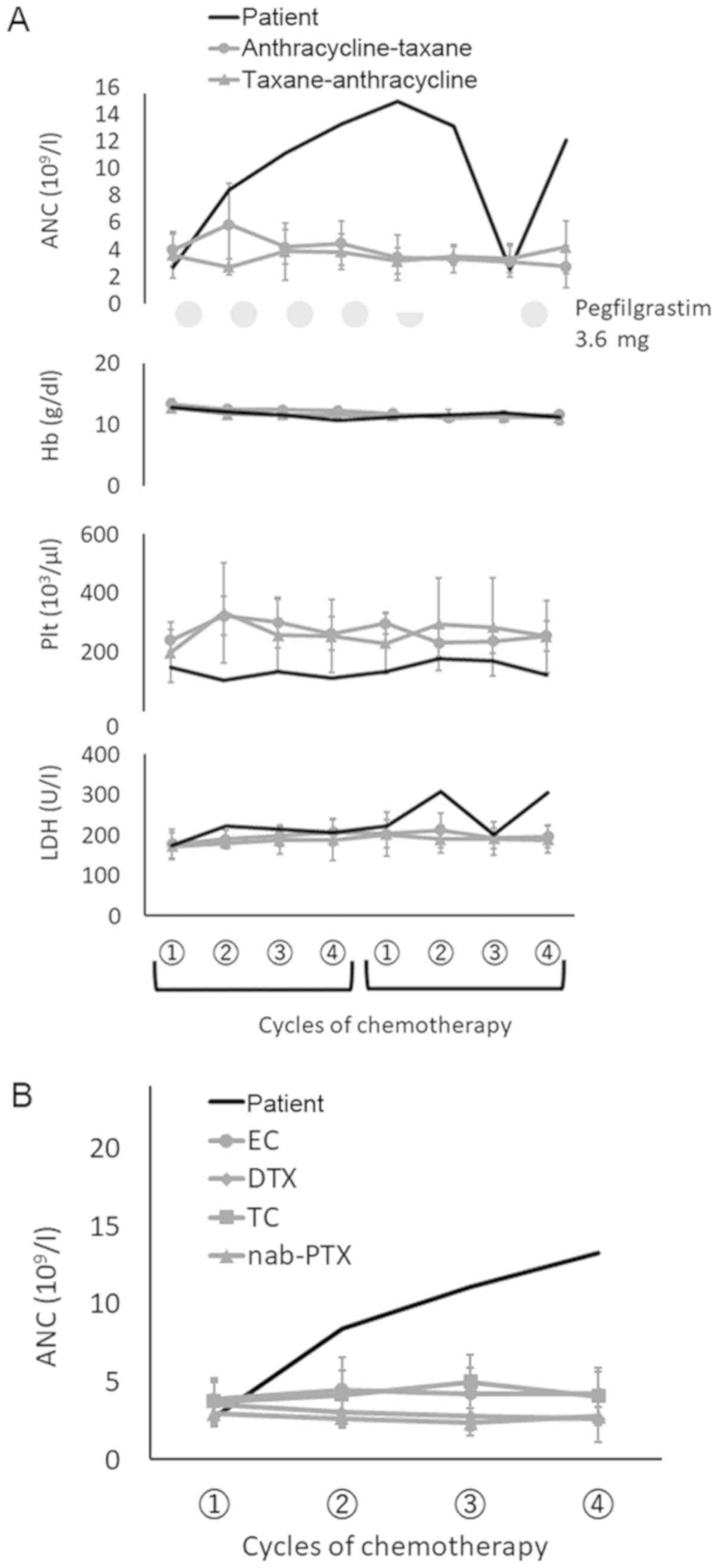 | Figure 1.(A) Median ANC, hemoglobin, platelet
count and LDH changes in our patient on day 1 of each cycle. The
black line shows the ANC changes in this case; the gray line with
circle and triangle points shows ANC changes in patients receiving
anthracycline followed by a taxane-based regimen, and those who
received taxane followed by anthracycline, respectively. Light gray
circle and semicircle indicate 3.6 mg and 1.8 mg pegfilgrastim,
respectively, for the present case on day 3. (B) Median ANC changes
on day 1 of each cycle in each indicated regimen. The black line
shows ANC changes in our patient during DD-EC. Gray line with
circle, rhombus, square and triangle points indicate ANC changes in
other patients who received EC, DTX, TC and nab-PTX, respectively.
The EC and DTX groups include patients who underwent DD
chemotherapy every 2 weeks. ANC, absolute neutrophil count; Hb,
hemoglobin; Plt, platelets; LDH, lactate dehydrogenase; DD,
dose-dense; EC, epirubicin (90 mg/m2) and
cyclophosphamide (600 mg/m2); DTX, docetaxel (75
mg/m2); TC, docetaxel (75 mg/m2) and
cyclophosphamide (700 mg/m2); nab-PTX, nab-paclitaxel
(260 mg/m2). |
Patients
Since pegfilgrastim (3.6 mg) was first approved in
Japan, 55 patients with breast cancer who underwent chemotherapy at
Shiga General Hospital were administered this agent between January
2015 and March 2018. The medical records of all 55 patients were
retrospectively reviewed.
Chemotherapy is regularly prescribed for relatively
young, high-risk patients with breast cancer, including ER-negative
patients and those who are ER-positive but exhibit high Ki-67
indices. According to patient data reviewed by our team, 6 of the
55 patients (10.9%) had bilateral breast tumors or multiple tumors
on one side. One patient had metachronous bilateral breast cancer;
however, data regarding previous history of breast cancer were not
available. Therefore, 60 tumors from 55 patients were investigated
in total (Table SI). Chemotherapy
was administered as primary adjuvant therapy in 49 patients
(89.1%), and for other situations (adjuvant systemic therapy of
local recurrence or second-primary ipsilateral breast cancer
without distant metastasis) in 6 patients (10.9%). Furthermore, 3
patients had metachronous bilateral breast cancer with a previous
history of chemotherapy on the contralateral side, and 2 patients
experienced local recurrence without distant metastasis, both of
whom had a previous history of primary therapy. Additionally, a
31-year-old patient with metastatic breast cancer was administered
high-dose emergency chemotherapy, owing to the rapid growth of
liver metastases.
Patients were administered EC every 2 or 3 weeks,
DTX every 2 or 3 weeks, DTX (75 mg/m2)/cyclophosphamide
(700 mg/m2) every 3 weeks, or nab-paclitaxel (nab-PTX;
260 mg/m2) every 3 weeks (24,25). In
patients with HER2-positive breast cancer, a loading dose of 8
mg/kg trastuzumab followed by a maintenance dose of 6 mg/kg was
used in conjunction with taxane-based therapy (DTX,
DTX/cyclophosphamide, or nab-PTX) every 3 weeks. A proportion of
patients who received triweekly DTX and were at risk of FN received
pegfilgrastim, including those aged ≥65 years and those with
locally advanced breast cancer and infectious or ulcerative
disease, reduced performance status, history of FN, or neutropenia
(8–10). Patients received 4–6 cycles of each
regimen along with 3.6 mg of pegfilgrastim on days 2–4 (24–72 h
after administration of chemotherapy).
Supportive treatment for patients receiving the EC
regimen consisted of 6.6 mg of dexamethasone and 0.75 mg of
palonosetron administered intravenously on day 1, 125 mg aprepitant
administered on day 1 and 80 mg on days 2 and 3 (26), and 8 mg dexamethasone administered
orally twice daily on days 1–3. For taxane-based regimens, 6.6 mg
dexamethasone was administered intravenously on day 1. Furthermore,
each patient was instructed to wear two surgical gloves that were a
size too small for their hands to prevent peripheral neuropathy,
beginning 30 min before taxane administration and ending 30 min
after the end of the infusion (27).
The completion rates of scheduled chemotherapy
regimens are shown in Table SII.
Causes of dose reduction included prolonged neutropenia or anemia
related to chemotherapy, mainly occurring in elderly patients and
those with comorbidities. Furthermore, 12 patients underwent
sequential anthracycline and taxane treatments with pegfilgrastim
in both regimens (Table SIII). The
ANC changes in these patients are shown in Fig. 1A, and B shows the ANC changes
observed in all patients apart from the subject of this report
during each regimen (the subject of this case report is denoted as
patient 1 in Table SIII). The
median ANC count on day 1 of each cycle was 4,195/mm3
(range, 1,400-9,300/mm3) across the 55 patients prior to
chemotherapy on day 1 of each cycle. No patients other than the
subject of this report developed leukocytosis during
chemotherapy.
Discussion
Pegfilgrastim-induced fatigue is known to occur in
10–20% of patients (19,21,22), and
can interfere with quality of life and treatment adherence. The
mechanisms of fatigue secondary to pegfilgrastim are not fully
understood; however, they appear to involve bone marrow expansion,
hyperstimulated production of novel bone marrow cells, and
augmented activity of pre-existing bone marrow owing to the
elevation of cytokine levels and induction of leukocytosis
(27–29).
Conversely, pegfilgrastim-induced hyperleukocytosis
is reported in <1% of the patients, but is not always associated
with adverse clinical effects (30).
Hyperleukocytosis is defined as a peripheral leukocyte count of
>100×103/µl. Rheingold and Lange previously reported
that hyperleukocytosis may cause death via central nervous system
hemorrhage or thrombosis, pulmonary leukostasis and metabolic
imbalances, particularly when accompanied by tumor lysis (31,32).
In this report, the proportion of patients who
underwent sequential anthracycline and taxane treatments with
pegfilgrastim was small. This was due to pegfilgrastim not being
administered with regimens such as triweekly DTX or weekly
paclitaxel (Table SIII).
Pegfilgrastim represents an important supportive therapy for
ensuring the continuation of the DD schedule. ANC normally recovers
to baseline values (day 1 of administration) if patients receive
pegfilgrastim along with chemotherapy (19,33).
Kosaka et al reported changes in ANC during the first cycle
of chemotherapy for 177 Japanese patients who received 3.6 mg
pegfilgrastim on day 2. ANC increased to a maximum of
11×103/µl on day 11, and decreased to
<10×103/µl by day 15 (20). As shown in Fig. 1, none of the patients, apart from the
subject of this case report, developed leukocytosis during
chemotherapy, regardless of the treatment regimen. Furthermore, no
major hematological changes were observed in any of these patients.
Supportive treatment during chemotherapy was prescribed equally to
almost all patients. Other supportive treatments, such as oral
dexamethasone, only exerted a minor effect on leukocytosis in our
patient. Additionally, the severe fatigue observed in our patient
can be distinguished from chemotherapy-induced fatigue by the
presence of leukocytosis following pegfilgrastim
administration.
The cancer board considered application other
granulocyte colony-stimulating factors, such as filgrastim, as
alternatives to 3.6 mg pegfilgrastim. Our patient did not receive
filgrastim, since it requires daily administration until ANC
recovery due to its shorter biological half-life. The patient
wanted to reduce her frequency of hospital visits in order to care
for her children. In our patient, who weighed 67 kg, the original
pegfilgrastim dose of 3.6 mg was not considered excessive (19,20,34). A
phase I/II study demonstrated the safety and efficacy of 30 µg/kg
and 1.8 mg of pegfilgrastim treatment in Japan. The appropriate
pegfilgrastim dose for Japanese patients with breast cancer was
evaluated in a previous study comparing doses of 1.8, 3.6 and 6.0
mg (19). The primary end-point of
that study was the duration of severe (grade 4) neutropenia in the
first chemotherapy cycle, which correlated with the incidence of
FN. Masuda et al (19)
demonstrated a dose-response relationship between pegfilgrastim
dose and primary end-point; a significant linear reduction was
observed with a significant plateau at 3.6 mg and non-significant
reduction at 6.0 mg. However, no statistically significant
differences were observed between the three arms regarding the
frequency of adverse hematological events or duration of severe
neutropenia. Thus, the dose reduction to 1.8 mg in our study
preserved the patient's neutrophil count.
Although there was no apparent dose-dependent
induction of adverse events, the biological half-life of
pegfilgrastim was not affected by the dose; therefore,
pegfilgrastim dose in our patient should have been switched from
3.6 to 1.8 mg before the onset of leukocytosis.
Following administration of 1.8 mg pegfilgrastim,
the patient's ANC on day 1 of the second DD-DTX cycle was
13,090/mm3. However, after the omission of prophylactic
use of pegfilgrastim, the ANC was 297/mm3 on day 14.
Although this indicates that the effect of 1.8 mg pegfilgrastim was
not sustained for more than 14 days, a limitation of this study was
that the nadir duration of 1.8 mg pegfilgrastim was not measured
during chemotherapy. Considering that the patient did not
experience FN during the cycle after 1.8 mg pegfilgrastim
injection, the effect of administering each cycle can be expected.
Indeed, an apparent ANC drop following administration of 1.8 mg was
observed; therefore, continuous use of 1.8 mg pegfilgrastim during
each cycle of chemotherapy may have improved leukocytosis.
Younger patients (<30 years) respond strongly to
3.6 mg pegfilgrastim. Adverse events associated with pegfilgrastim
may however affect the continuity of chemotherapy. A 1.8-mg dose of
pegfilgrastim was considered an option for palliating fatigue and
leukocytosis in this patient with high-risk breast cancer receiving
DD chemotherapy, with the aim of preventing treatment interruption.
For young patients (<30 years) with aggressive disease, such as
TNBC, dose reduction should be avoided to maintain therapeutic
effect. Conversely, treatment with daily administration of
granulocyte colony-stimulating factor, may not be feasible for
patients who cannot visit the hospital frequently.
The limitation of the present study was that 1.8 mg
pegfilgrastim was only administered on a single occasion during
treatment; therefore, conclusions regarding its regular use
compared with 3.6 mg pegfilgrastim cannot be made based solely on
this case report. However, we believe that the half-dose
pegfilgrastim administration used in this case may help with the
completion of optimal-dose chemotherapy with reduced inoculation
frequency of granulocyte colony-stimulating factor in patients with
fatigue and leukocytosis.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All the data supporting the findings of the present
study are included in this published manuscript and supplementary
data.
Authors' contributions
HT, WT and FY participated in the treatment, data
interpretation and manuscript preparation. TG and TO are the member
of the cancer board, discussed about the strategy of 1.8 mg dose of
pegfilgrastim administration to this patient. HT wrote and edited
the manuscript. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
All study participants provided informed consent,
and the study design was approved by the Ethics Review Board of
Shiga General Hospital. All experiments were performed in
accordance with the principles outlined in the Declaration of
Helsinki.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this case report and any accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Mobus V, Jackisch C, Luck HJ, du Bois A,
Thomssen C, Kuhn W, Nitz U, Schneeweiss A, Huober J, Harbeck N, et
al: Ten-year results of intense dose-dense chemotherapy show
superior survival compared with a conventional schedule in
high-risk primary breast cancer: Final results of AGO phase III
iddEPC trial. Ann Oncol. 29:178–185. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Mobus V, von Minckwitz G, Jackisch C, Luck
HJ, Schneeweiss A, Tesch H, Elling D, Harbeck N, Conrad B, Fehm T,
et al: German adjuvant intergroup Node-positive Study (GAIN): A
phase III trial comparing two dose-dense regimens (iddEPC versus
ddEC-PwX) in high-risk early breast cancer patients. Ann Oncol.
28:1803–1810. 2017.PubMed/NCBI
|
|
3
|
Lambertini M, Ceppi M, Cognetti F,
Cavazzini G, De Lurentiis M, De Placido S, Michelotti A, Bisagni G,
Durando A, Valle E, et al: Dose-dense adjuvant chemotherapy in
premenopausal breast cancer patients: A pooled analysis of the MIG1
and GIM2 phase III studies. Eur J Cancer. 71:34–42. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Foukakis T, von Minckwiz G, Bengtsson NO,
Brandberg Y, Wallberg B, Fornander T, Mineritsch B, Schmatloch S,
Singer CF, Steger G, et al: Effect of tailored dose-dense
chemotherapy vs standard 3-weekly adjuvant chemotherapy on
recurrence-free survival among women with high-risk early breast
cancer: A Randomized Clinical Trial. JAMA. 316:1888–1896. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Del Mastro L, De Placido S, Bruzi P, De
Laurentiis M, Boni C, Cavazzini G, Durando A, Turletti A, Nisticò
C, Valle E, et al: Fluorouracil and dose-dense chemotherapy in
adjuvant treatment of patients with early-stage breast cancer: An
open-label, 2 × 2 factorial, randomised phase 3 trial. Lancet.
385:1863–1872. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Aapro M, Boccia R, Leonard R, Camps C,
Campone M, Choquet S, Danova M, Glaspy J, Hus I, Link H, et al:
Refining the role of pegfilgrastim (a long-acting G-CSF) for
prevention of chemotherapy-induced febrile neutropenia: Consensus
guidance recommendations. Support Care Cancer. 25:3295–3304. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Vehreschild JJ, Bohme A, Cornely OA, Kahl
C, Karthaus M, Kreuzer KA, Maschmeyer G, Mousset S, Ossendorf V,
Penack O, et al: Prophylaxis of infectious complications with
colony-stimulating factors in adult cancer patients undergoing
chemotherapy-evidence-based guidelines from the infectious diseases
working party AGIHO of the German society for haematology and
medical oncology (DGHO). Ann Oncol. 25:1709–1718. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Smith TJ, Bohlke K, Lyman GH, Carson KR,
Crawford J, Cross SJ, Goldberg JM, Khatcheressian JL, Leighl NB,
Perkins CL, Somlo G, et al: Recommendations for the Use of WBC
Growth Factors: American Society of Clinical Oncology Clinical
Practice Guideline Update. J Clin Oncol. 33:3199–212. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Aapro MS, Bohlius J, Cameron DA, Dal Lago
L, Donnelly JP, Kearney N, Lyman GH, Pettengell R, Tjan-Heijnen VC,
Walewski J, Weber DC, et al: 2010 update of EORTC guidelines for
the use of granulocyte-colony stimulating factor to reduce the
incidence of chemotherapy-induced febrile neutropenia in adult
patients with lymphoproliferative disorders and solid tumours. Eur
J Cancer. 47:8–32. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Crawford J, Becker PS, Armitage JO,
Blayney DW, Chavez J, Curtin P, Dinner S, Fynan T, Gojo I,
Griffiths EA, Hough S, et al: Myeloid Growth Factors, Version
2.2017, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr
Canc Netw. 15:1520–1541. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Green MD, Koelbl H, Baselga J, Galid A,
Guillem V, Gascon P, Siena S, Lalisang RI, Samonigg H, Clemens MR,
et al: A randomized double-blind multicenter phase III study of
fixed-dose single-administration pegfilgrastim versus daily
filgrastim in patients receiving myelosuppressive chemotherapy. Ann
Oncols. 14:29–35. 2003. View Article : Google Scholar
|
|
12
|
Grigg A, Solal-Celigny P, Hoskin P, Taylor
K, McMillan A, Forstpointner R, Bacon P, Renwick J and Hiddemann W;
International Study Group, : Open-label, randomized study of
pegfilgrastim vs. daily filgrastim as an adjunct to chemotherapy in
elderly patients with non-Hodgkin's lymphoma. Leuk Lymphoma.
44:1503–1508. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Holmes FA, Jones SE, O'Shaughnessy J,
Vukelja S, George T, Savin M, Richards D, Glaspy J, Meza L, Cohen
G, et al: Comparable efficacy and safety profiles of once-per-cycle
pegfilgrastim and daily injection filgrastim in
chemotherapy-induced neutropenia: A multicenter dose-finding study
in women with breast cancer. Ann Oncol. 13:903–909. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Holmes FA, O'Shaughnessy JA, Vukelja S,
Jones SE, Shogan J, Savin M, Glaspy J, Moore M, Meza L, Wiznitzer
I, et al: Blinded, randomized, multicenter study to evaluate single
administration pegfilgrastim once per cycle versus daily filgrastim
as an adjunct to chemotherapy in patients with high-risk stage II
or stage III/IV breast cancer. J Clin Oncol. 20:727–731. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Vose JM, Crump M, Lazarus H, Emmanouilides
C, Schenkein D, Moore J, Moore J, Frankel S, Flinn I, Lovelace W,
et al: Randomized, multicenter, open-label study of pegfilgrastim
compared with daily filgrastim after chemotherapy for lymphoma. J
Clin Oncol. 21:514–519. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhang W, Jiang Z, Wang L, Li C and Xia J:
An open-label, randomized, multicenter dose-finding study of
once-per-cycle pegfilgrastim versus daily filgrastim in Chinese
breast cancer patients receiving TAC chemotherapy. Med Oncol.
32:1472015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Cooper KL, Madan J, Whyte S, Stevenson MD
and Akehurst RL: Granulocyte colony-stimulating factors for febrile
neutropenia prophylaxis following chemotherapy: Systematic review
and meta-analysis. BMC Cancer. 11:4042011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Pinto L, Liu Z, Doan Q, Bernal M, Dubois R
and Lyman G: Comparison of pegfilgrastim with filgrastim on febrile
neutropenia, grade IV neutropenia and bone pain: A meta-analysis of
randomized controlled trials. Curr Med Res Opin. 23:2283–2295.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Masuda N, Tokuda Y, Nakamura S, Shimazaki
R, Ito Y and Tamura K: Dose response of pegfilgrastim in Japanese
breast cancer patients receiving six cycles of docetaxel,
doxorubicin, and cyclophosphamide therapy: A randomized controlled
trial. Support Care Cancer. 23:2891–2898. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kosaka Y, Rai Y, Masuda N, Takano T, Saeki
T, Nakamura S, Shimazaki R, Ito Y, Tokuda Y and Tamura K: Phase III
placebo-controlled, double-blind, randomized trial of pegfilgrastim
to reduce the risk of febrile neutropenia in breast cancer patients
receiving docetaxel/cyclophosphamide chemotherapy. Support Care
Cancer. 23:1137–1143. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Pawloski PA, Larsen M, Thoresen A and
Giordana MD: Pegfilgrastim use and bone pain: A cohort study of
community-based cancer patients. J Oncol Pharm Pract. 22:423–429.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Moukharskaya J, Abrams DM, Ashikaga T,
Khan F, Schwartz J, Wilson K, Verschraegen C, Openshaw T, Valentine
J, Eneman J, et al: Randomized phase II study of loratadine for the
prevention of bone pain caused by pegfilgrastim. Support Care
Cancer. 24:3085–3093. 2016.PubMed/NCBI
|
|
23
|
Union for International Cancer Control-TNM
classification. 8th. https://www.uicc.org/July 17–2019
|
|
24
|
Untch M, Jackisch C, Schneeweiss A, Conrad
B, Aktas B, Denkert C, Eidtmann H, Wiebringhaus H, Kümmel S,
Hilfrich J, et al: Nab-paclitaxel versus solvent-based paclitaxel
in neoadjuvant chemotherapy for early breast cancer (GeparSepto-GBG
69): A randomised, phase 3 trial. Lancet Oncol. 17:345–356. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Shimada H, Ueda S, Saeki T, Shigekawa T,
Takeuchi H, Hirokawa E, Sugitani I, Sugiyama M, Takahashi T,
Matsuura K, et al: Neoadjuvant triweekly nanoparticle albumin-bound
paclitaxel followed by epirubicin and cyclophosphamide for Stage
II/III HER2-negative breast cancer: Evaluation of efficacy and
safety. Jpn J Clin Oncol. 45:642–649. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Saito M, Aogi K, Sekine I, Yoshizawa H,
Yanagita Y, Sakai H, Inoue K, Kitagawa C, Ogura T and Mitsuhashi S:
Palonosetron plus dexamethasone versus granisetron plus
dexamethasone for prevention of nausea and vomiting during
chemotherapy: A double-blind, double-dummy, randomised, comparative
phase III trial. Lancet Oncol. 10:115–124. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Tsuyuki S, Senda N, Kanng Y, Yamaguchi A,
Yoshibayashi H, Kikawa Y, Katakami N, Kato H, Hashimoto T, Okuno T,
et al: Evaluation of the effect of compression therapy using
surgical gloves on nanoparticle albumin-bound paclitaxel-induced
peripheral neuropathy: A phase II multicenter study by the Kamigata
Breast Cancer Study Group. Breast Cancer Res Treat. 160:61–67.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Lambertini M, Del Mastro L, Bellodi A and
Pronzato P: The five ‘Ws’ for bone pain due to the administration
of granulocyte-colony stimulating factors (G-CSFs). Crit Rev Oncol
Hematol. 89:112–128. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Hamilton JA: Colony-stimulating factors in
inflammation and autoimmunity. Nat Rev Immunol. 8:533–544. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Stosser S, Schweizerhof M and Kuner R:
Hematopoietic colony-stimulating factors: New players in
tumor-nerve interactions. J Mol Med (Berl). 89:321–329. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Package insert, . Neulasta
(pegfilgrastim). Thousand Oaks, CA, Amgen. September 15–2005,
https://www.accessdata.fda.gov/drugsatfda_docs/label/2002/pegfamg013102LB.pdf#search=%27Package+insert.+Neulasta+%28pegfilgrastim%29.+Thousand+Oaks%2C+CA%3A+Amgen%2C+September+15%2C+2005.%27July
17–2019
|
|
32
|
Rheingold SD and Lange BJ: Oncogenic
emergencies. Principkes and Practice of Pediatric Oncology. 4th.
Pizzo PA and Poplack DG: Philadelphia: Lippincott Williams &
Wilkins; pp. 1177–1203. 2002
|
|
33
|
Schirm S, Engel C, Loibl S, Loeffler M and
Scholz M: Model-based optimization of G-CSF treatment during
cytotoxic chemotherapy. J Cancer Res Clin Oncol. 144:343–358. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Ishiguro H, Kitano T, Yoshibayash i, Toi
M, Ueno T, Yasuda H, Yanagihara K, Garbo CL and Fukushima M:
Prolonged neutropenia after dose-dense chemotherapy with
pegfilgrastim. Ann Oncol. 19:1019–1020. 2008. View Article : Google Scholar : PubMed/NCBI
|














