Introduction
Pancreatic cancer is one of the most aggressive
digestive system malignancies, and poses a major threat to human
health, representing a major socioeconomic burden worldwide.
Moreover, the morbidity and mortality rates of pancreatic cancer
continue to rise on a yearly basis (1). The majority of the patients who are
initially inflicted with pancreatic cancer do not exhibit any clear
clinical symptoms, or only display non-specific symptoms, such as
abdominal distention and emesis. Considering that the pancreas is a
retroperitoneal organ that is located behind the stomach and
duodenum, the application of current imaging techniques is limited
(2). As a result, distinguishing
pancreatic cancer from other focal pancreatic diseases remains
challenging. Defining the properties of pancreatic tumors at an
early stage would markedly improve the survival and the quality of
life of the patients (2).
Contrast-enhanced harmonic endoscopic ultrasound (CH-EUS) is a
novel technology that has been used in the diagnosis of pancreatic
diseases over the course of the last decade. This method combines
EUS with tissue harmonic imaging technology, and overcomes two
major shortcomings of the traditionally applied method, abdominal
Doppler ultrasound: The latter is susceptible to gastrointestinal
gas, whereas the former is insensitive to the tiny blood vessels in
which the blood flows at low speed (3). With CH-EUS, it is also possible to
observe the blood vessels of pancreatic masses in more detail, and
it is therefore more accurate in terms of determining pancreatic
mass properties (4). To the best of
our knowledge, using CH-EUS to differentiate pancreatic malignant
from benign masses has only been reported by a few clinical cohort
studies (3,4). To date, however, no systematic reviews
or meta-analyses have been performed to estimate the diagnostic
value of CH-EUS with respect to its ability to differentiate
pancreatic malignant tumors from other focal pancreatic diseases.
Therefore, a systematic review and meta-analysis has been
undertaken in the present study.
Materials and methods
Literature search
Articles published up to January 2017 in the PubMed,
EMBASE, Medline, Web of Science and Cochrane Library databases were
searched. The terms used for the search strategy were [(‘contrast
enhanced’ OR ‘contrast enhancement’ OR ‘contrast imaging’ OR
‘contrast agent’ OR ‘contrast medium’) AND ‘harmonic’], and (‘EUS’
OR ‘endoscopic ultrasound’ OR ‘endosonography’ OR ‘endoscopy
ultrasonographic’) AND (‘pancreatic cancer’ or ‘pancreatic mass’ or
‘pancreatitis’)].
Inclusion criteria
The criteria for studies to be included in the
present systematic review and meta-analysis were as follows: i)
CH-EUS was applied to determine the pancreatic mass quality; ii)
all patients received a definitive final diagnosis, i.e., malignant
tumors were treated with surgical resection or subjected to
EUS-guided fine-needle aspiration (EUS-FNA), and benign tumors was
followed up for >6 months consecutively; iii) the most important
four statistics [true positive (TP), false positive (FP), true
negative (TN) and false negative (FN)] were extractable from these
studies either directly or mediately; (iv) there were no
restrictions on the study design or the number of study centers;
and (v) although full-text original articles were preferred,
abstracts alone were also included in the analysis.
Exclusion criteria
The exclusion criteria were as follows: i) Duplicate
studies, case reports, reviews or letters to the editor; ii)
statistical data insufficient to construct a 2×2 diagnostic table;
iii) the ultimate diagnoses of patients were not recorded, or the
continuous follow-up time of the patients was <6 months.
Data collection
Two independent authors (YL and DL) scanned and
identified the relevant literature according to the same inclusion
and exclusion criteria. When the two interpretations of the data
were inconsistent, two other authors (MX and SH) would also
critically assess the collection, ensuring that the final result
was precise. Detailed information, including the total numbers of
patients, the authors' country, patients' mean age, the diameter of
the mass, type of study (retrospective/prospective), study center
(single/multiple), diagnostic method (qualitative/quantitative),
lesion characteristics (solid/cystic), and the TP, FP, TN and FN
statistics were extracted for further analysis.
Quality assessment
The Quality Assessment of Diagnostic Accuracy
Studies (QUADAS)-2 tool was applied to rate the quality of each
included study (5). The QUADAS-2
tool was applied in four phases: The review question was
summarized, the tool was tailored to produce review-specific
guidance, a flow diagram for the primary study was constructed, and
the publication bias and applicability were assessed. This tool
allows for more transparent rating of bias and applicability of
primary diagnostic accuracy studies (5). This important work was completed by two
independent authors (YL and DL), through discussing their results
with an additional author (MX) at the time of data collection.
Statistical analysis
Statistical analyses were performed using Metadisc
software, version 1.4 (Hospital Universitario Ramon y Cajal) and
Stata software, version 14 (StataCorp LP). First, whether the
meta-analysis could be accomplished using Metadisc software for the
Spearman's test was determined. Subsequently, Metadisc software was
used to merge the diagnostic statistical data. Q-test and
Chi-squared test were used to determine whether there was any
heterogeneity between the results of each study. If P<0.1 or
I2>50% was obtained, then heterogeneity was
determined to exist, and the random effects model was used to
calculate the pooled sensitivity, pooled specificity, pooled
negative likelihood ratio (NLR), pooled positive likelihood ratio
(PLR), and the diagnostic odds ratio (DOR). Otherwise, the fixed
effects model was used to calculate the heterogeneity. Moreover,
the factors that cause heterogeneity were identified using
meta-regression and subgroup meta-analysis. Finally, the publishing
bias of the literature was analyzed by drawing funnel and Egger's
publication bias plots using Stata 14.0 software.
Results
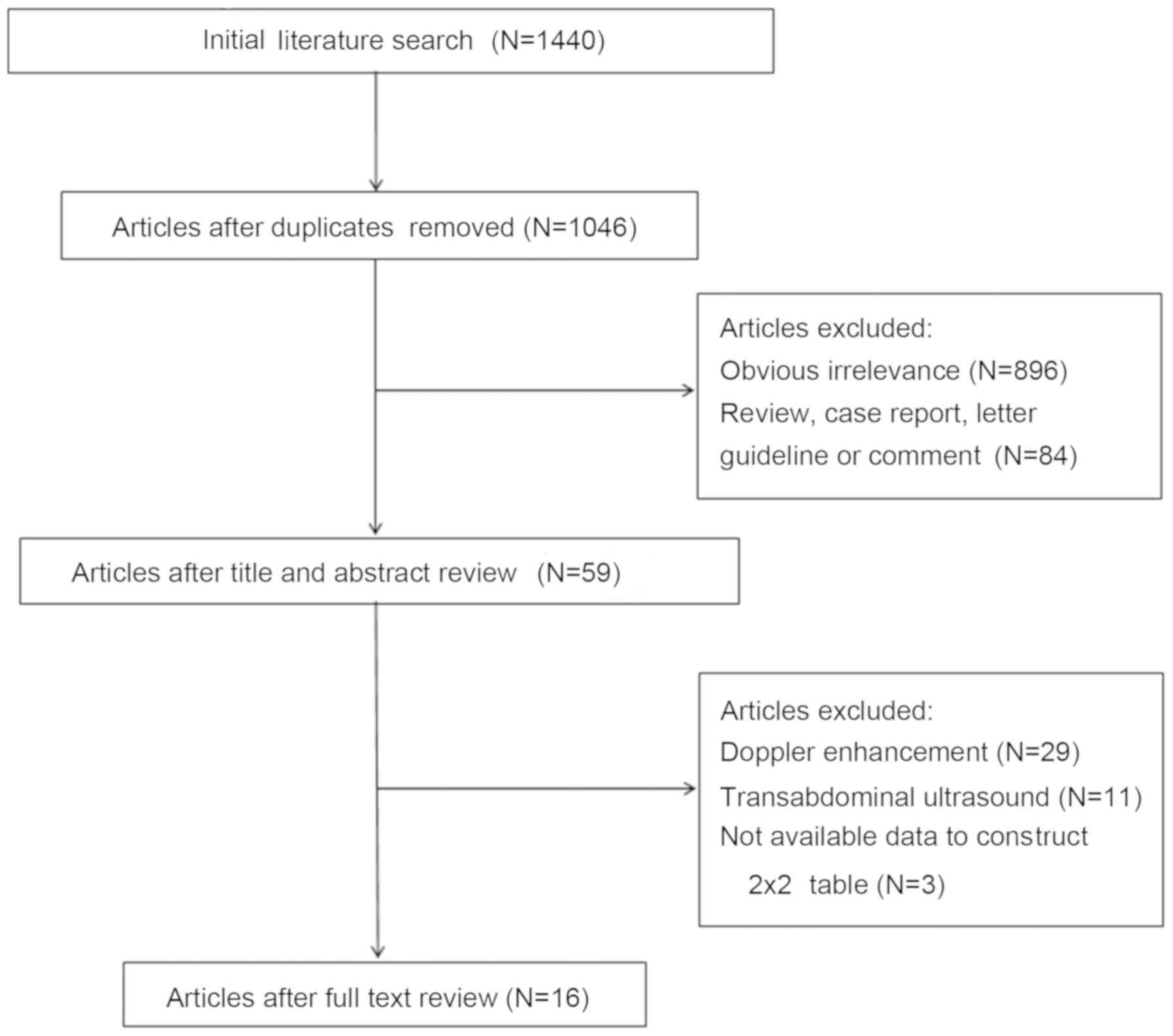
Literature search
A total of 1,440 articles were initially extracted
from the PubMed, EMBASE, Medline, Web of Science and Cochrane
Library databases. Subsequently, 394 duplicate articles were
removed, and clearly irrelevant articles, reviews, case report
articles, letters to the editor, and guidelines were also excluded.
After reading every abstract and full-text article, 29 articles
where Doppler enhancement had been studied, 11 articles on
transabdominal ultrasound and 3 articles in which 2×2 diagnostic
tables could not be extracted were excluded, leaving 16 remaining
studies that were included in this review (Fig. 1).
Study characteristics
The characteristics of the 16 studies (3,4,6–19),
including a total of 1,325 patients, were extracted by two
independent authors. Eight studies, including 534 patients, were
from the USA and Europe, whereas the remaining 8 studies, including
791 patients, were from Asia. The minimum duration of the included
studies was 3 months. Moreover, 12 of the studies also included
>12 months of follow-up. In addition, of the 16 studies, 10 were
retrospective and 6 prospective, whereas 13 were single-center and
3 were multi-center. The majority of the patients included in the
16 studies were aged >60 years; however, Romagnuolo et al
(9) failed to report on the mean age
of the patients. The diameter of the pancreatic masses ranged from
18.6 to 42.5 mm, and the majority of these masses were solid. The
two mainstream ultrasound imaging contrast agents, SonoVue™
(Bracco) and Sonazoid™ (GE Healthcare), were used in 15 of the
studies. Half of the included studies used a qualitative ultrasound
enhancement method, whereas the other half used a quantitative
method. A total of 6 studies failed to report on the
endosonographer, whereas the diagnoses in the remaining 10 studies
were confirmed by more than one endoscopy expert (Table I).
 | Table I.General characteristics of the
included studies. |
Table I.
General characteristics of the
included studies.
| First author,
year | Study ID | Total patient
no. | Country | Duration of study
(months) | Study type (R/P) | Study center
(S/M) | Mean age (years) | Sex (female %) | Diameter (mm) | Agent type | Ultrasound diagnostic
method (qualitative/quantitative) | Final diagnosis
standard | Endosonographer
(expert/U) | Lesion
characteristics (solid/cystic) | (Refs.) |
|---|
| Fusaroli, 2010 | 1 | 90 | Italy | 18 | R | S | 67.0 | 51.1 | 25.0 | SV | Qualitative | PT/CC | Expert | Solid | (3) |
| Napoleon, 2010 | 2 | 35 | France | 12 | P | S | 60.0 | 45.7 | 30.0 | SV | Qualitative | PT/CC | U | Solid | (6) |
| Seicean, 2010 | 3 | 30 | Romania | 3 | R | S | 57.0 | 16.7 | 42.5 | SV | Quantitative | PT | Expert | Solid | (7) |
| Matsubara,
2011 | 4 | 91 | Japan | 30 | R | S | 61.4 | 33.0 | 23.7 | SZ | Qualitative | PT/CC | U | U | (8) |
| Romagnuolo,
2011 | 5 | 11 | USA | U | P | S | U | U | 18.6 | D | Quantitative | PT/CC | U | U | (9) |
| Kitano, 2012 | 6 | 277 | Japan | 25 | P | M | 64.3 | 37.5 | 32.4 | SZ | Quantitative | PT/CC | Expert | Solid | (10) |
| Imazu, 2012 | 7 | 30 | Japan | 21 | R | S | 66.9 | 26.7 | 40.5 | SZ | Quantitative | PT/CC | Expert | U | (11) |
| Gheonea, 2013 | 8 | 51 | Romania | U | R | S | 50.0 | 51.0 | U | SV | Quantitative | PT/CC | Expert | U | (12) |
| Lee, 2013 | 9 | 37 | South Korea | 20 | R | S | 62.3 | 35.1 | 34.0 | SV | Qualitative | PT | Expert | Solid | (13) |
| Gincul, 2014 | 10 | 100 | France | 11 | P | M | 64.6 | 49.0 | 30.6 | SV | Quantitative | PT/CC | Expert | Solid | (4) |
| Park, 2014 | 11 | 90 | South Korea | 31 | R | S | 63.5 | 31.1 | U | SV | Qualitative | PT/CC | Expert | Solid | (14) |
| Yamashita,
2015 | 12 | 147 | Japan | 54 | R | S | 69.0 | 37.4 | 30.0 | SZ | Qualitative | PT/CC | Expert | Solid | (15) |
| Săftoiu, 2015 | 13 | 167 | Spain, Germany,
Romania, Denmark | 33 | P | M | 62.0 | 24.0 | 30.0 | SV | Quantitative | PT/CC | U | Solid | (16) |
| Kamata, 2016 | 14 | 70 | Japan | 61 | P | S | 62.0 | 55.7 | 33.0 | SZ | Qualitative | PT | Expert | Cystic | (17) |
| Iordache, 2016 | 15 | 50 | Romania | 48 | R | S | 54.3 | 14 | U | SV | Quantitative | PT/CC | U | Solid | (18) |
| Uekitani, 2016 | 16 | 49 | Japan | 32 | R | S | 66.5 | 53 | 31.1 | SZ | Qualitative | PT/CC | U | U | (19) |
2×2 diagnostic tables data and quality
of the literature
The four-grid data were registered, and the quality
of the included literature was assessed using the QUADAS-2 method
(Table II). The risk of bias in the
reference index text was not reported by Imazu et al
(11). In addition, there was a high
risk of bias in flow and timing in the studies of Romagnuolo et
al (9), Imazu et al
(11) and Iordache et al
(18). Overall, all 16 studies were
deemed as high-quality.
| Table II.Derived 2×2 table and QUADAS-2
results. |
Table II.
Derived 2×2 table and QUADAS-2
results.
|
|
|
|
|
| Risk of
biasa | Concerns regarding
applicabilitya |
|---|
|
|
|
|
|
|
|
|
|---|
| Study ID | TP | FP | FN | TN | 1 | 2 | 3 | 4 | 1 | 2 | 3 |
|---|
| 1 | 49 | 14 | 2 | 25 | L | L | L | L | L | L | L |
| 2 | 16 | 2 | 2 | 15 | L | L | L | L | L | L | L |
| 3 | 12 | 1 | 3 | 11 | L | L | L | L | L | L | L |
| 4 | 46 | 3 | 2 | 40 | L | U | L | L | L | L | L |
| 5 | 9 | 0 | 0 | 2 | L | L | L | H | L | L | L |
| 6 | 194 | 9 | 10 | 64 | L | L | L | L | L | L | L |
| 7 | 22 | 0 | 0 | 8 | L | U | L | H | L | L | L |
| 8 | 30 | 2 | 2 | 17 | L | L | L | L | L | L | L |
| 9 | 28 | 1 | 2 | 6 | L | L | L | L | L | L | L |
| 10 | 66 | 2 | 3 | 29 | L | L | L | L | L | L | L |
| 11 | 57 | 9 | 5 | 19 | L | L | L | L | L | L | L |
| 12 | 102 | 11 | 7 | 27 | L | L | L | L | L | L | L |
| 13 | 98 | 4 | 14 | 51 | L | L | L | L | L | L | L |
| 14 | 29 | 10 | 1 | 30 | L | L | L | L | L | L | L |
| 15 | 17 | 6 | 2 | 25 | L | L | L | H | L | L | L |
| 16 | 32 | 0 | 8 | 9 | L | L | L | L | L | L | L |
Diagnostic performance of CH-EUS
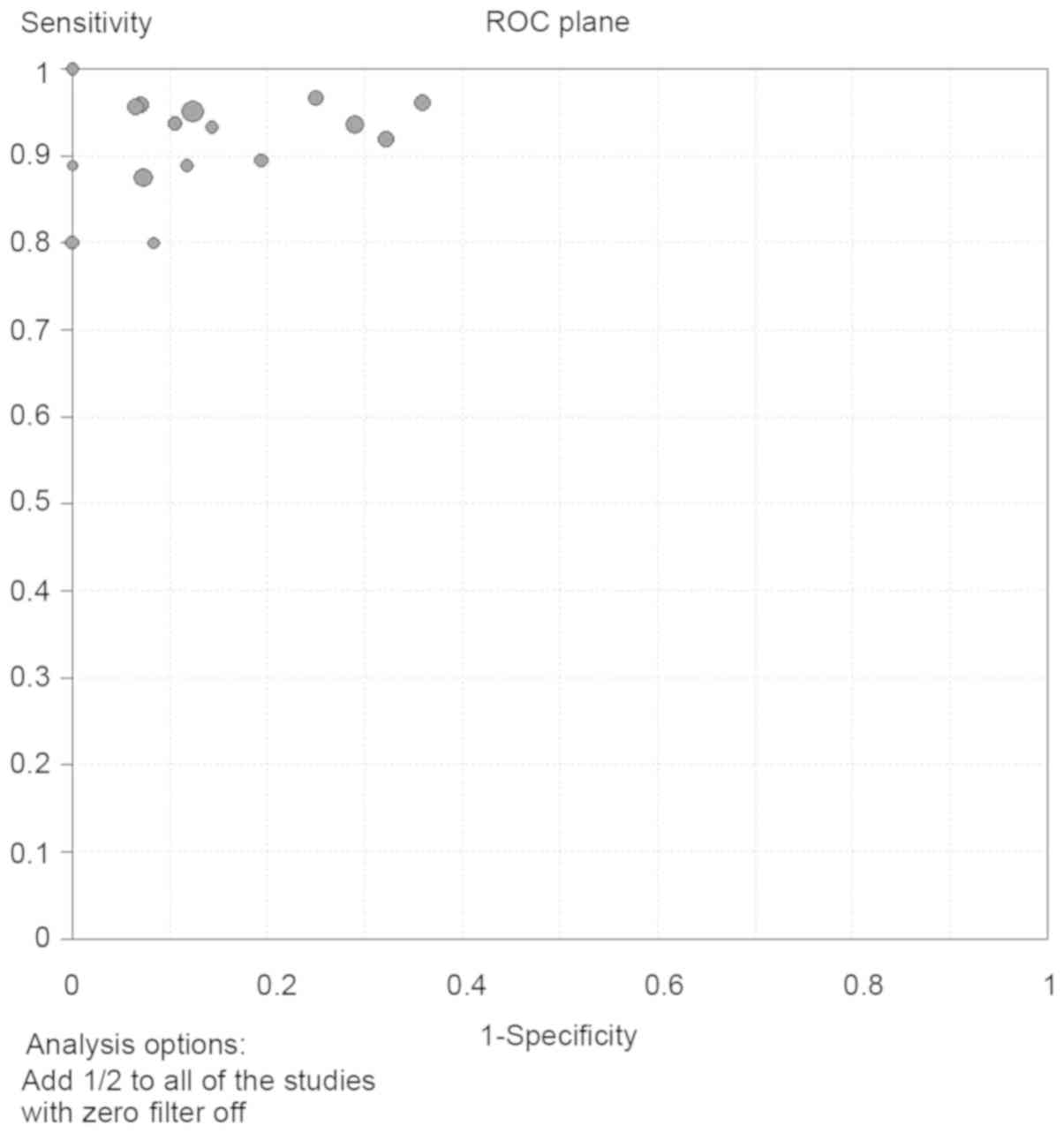
A Spearman's test was performed, and the Spearman's
relative number was identified to be 0.094 (P=0.729). Furthermore,
on the receiver operating characteristic (ROC) plane, the
distribution of the data points did not appear as the
characteristic ‘shoulder-arm’ shape (Fig. 2). Therefore, no threshold effect
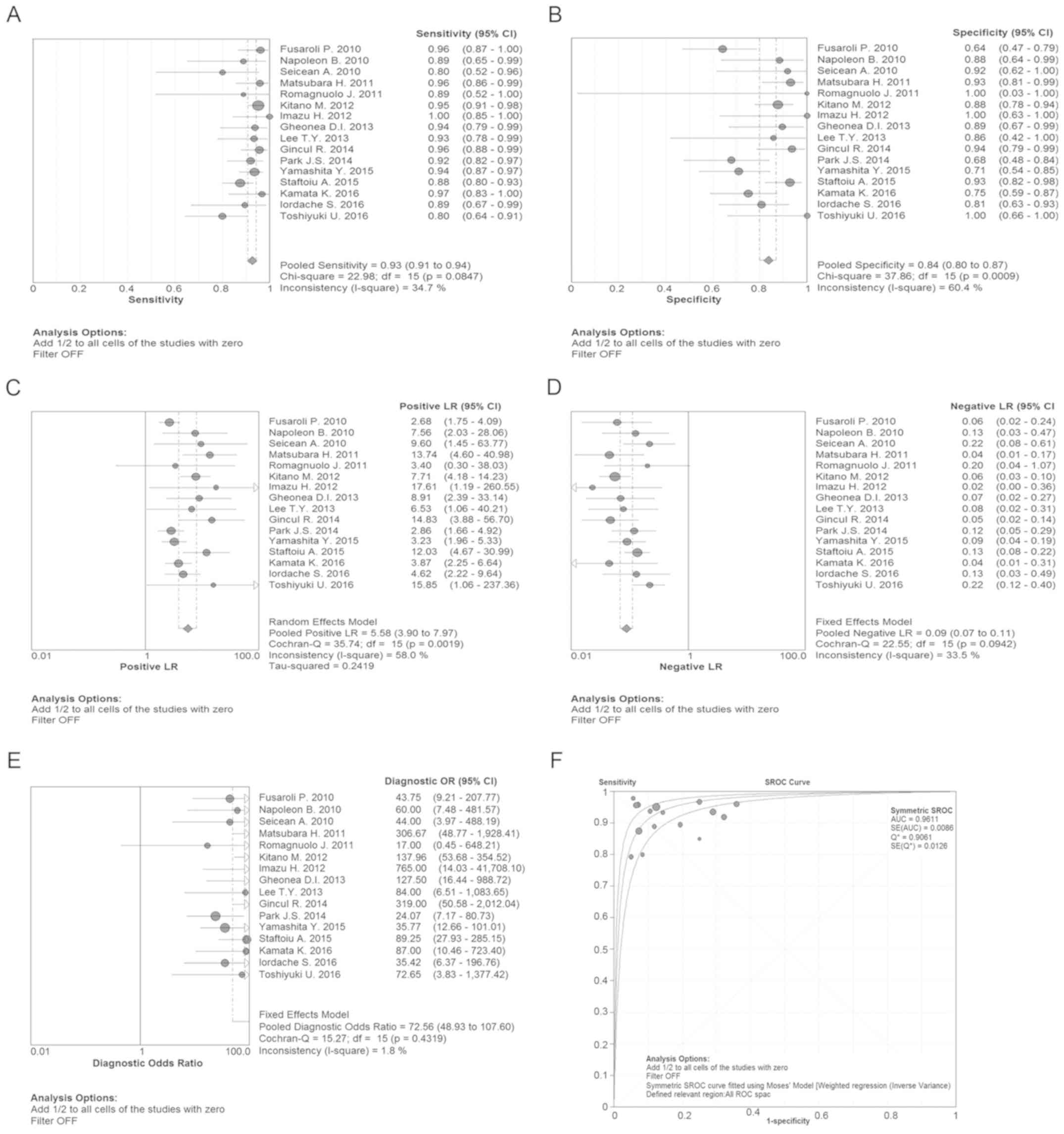
existed among the 16 studies. The pooled sensitivity, specificity,
PLR, NLR and DOR statistics of the CH-EUS analysis were used to
distinguish malignant from benign tumors, and these values were
determined to be 93% [95% confidence interval (CI), 91–94%], 84%
(95% CI: 80–87%), 5.58 (95% CI: 3.90–7.97), 0.09 (95% CI:
0.07–0.11) and 72.56 (95% CI: 48.93–107.60), respectively (Fig. 3A-E). On the summary ROC (SROC) curve,
the area under the curve (AUC) was shown to be 0.9611, which was a
significant result, and therefore the malignant tumors were
successfully differentiated from the benign ones (Fig. 3F).
Heterogeneity analysis
In order to explore the sources of heterogeneity,
subgroup meta-analysis and meta-regression studies were performed,
suggesting that the country of origin, total number of patients,
the experience of the endoscopy experts, average age, study design,
sex, lesion diameter, lesion characteristics, fellow-up duration,
the number of study center, diagnostic method and agent type, were
not the origin of heterogeneity. Taken together, the results of the
subgroup meta-analysis revealed that the diagnostic performance of
CH-EUS in terms of differentiating the pancreatic masses was good
as well as stable (Table III).
| Table III.Predefined subgroup analysis of
indices and subsequent meta-regression on DOR. |
Table III.
Predefined subgroup analysis of
indices and subsequent meta-regression on DOR.
| Subgroup | Study numbers | Pooled sensitivity
(95% CI) | I2% | Pooled specificity
(95% CI) | I2% | Diagnostic odds
ratio (95% CI) | I2% | RDOR (95% CI) | P-value |
|---|
| Area |
|
|
|
|
|
|
|
|
|
|
Europe/America | 8 | 0.91
(0.87–0.94) | 11.8 | 0.85
(0.79–0.89) | 59.6 | 71.60
(38.55–132.95) | 0 | 1.3
(0.45–3.81) | 0.60 |
|
Asian | 8 | 0.94
(0.91–0.95) | 47.0 | 0.83
(0.77–0.87) | 65.2 | 73.30
(43.97–122.20) | 33.3 |
|
|
| Total patients |
|
|
|
|
|
|
|
|
|
|
≥85 | 7 | 0.93
(0.91–0.95) | 26.8 | 0.83
(0.78–0.87) | 78.4 | 78.60
(39.13–157.91) | 50.5 | 0.74
(0.24–2.24) | 0.56 |
|
<85 | 9 | 0.90
(0.85–0.94) | 35.9 | 0.85
(0.78–0.90) | 19.5 | 67.43
(31.13–146.05) | 0 |
|
|
| Duration,
months |
|
|
|
|
|
|
|
|
|
|
≥28 | 7 | 0.94
(0.91–0.95) | 47 | 0.83
(0.77–0.87) | 65.2 | 73.30
(43.97–122.20) | 33.3 | 1.60
(0.76–3.40) | 0.20 |
|
<28 | 7 | 0.94
(0.91–0.95) | 47 | 0.83
(0.77–0.87) | 65.2 | 73.30
(43.97–122.20) | 33.3 |
|
|
|
Unconfirmed | 2 | 0.94
(0.91–0.95) | 47 | 0.83
(0.77–0.87) | 65.2 | 73.30
(43.97–122.20) | 33.3 |
|
|
| Study center |
|
|
|
|
|
|
|
|
|
|
Single | 13 | 0.92
(0.90–0.95) | 25.9 | 0.80
(0.75–0.84) | 55.8 | 54.42
(33.53–88.31) | 0 | 2.32
(0.83–6.45) | 0.10 |
|
Multiple | 3 | 0.93
(0.90–0.95) | 70.0 | 0.91
(0.85–0.95) | 0 | 130.36
(66.11–257.04) | 0 |
|
|
| Design |
|
|
|
|
|
|
|
|
|
|
Retrospective | 10 | 0.92
(0.89–0.95) | 39.1 | 0.80
(0.74–0.85) | 64.4 | 52.93
(31.52–88.87) | 0 | 1.98
(0.75–5.21) | 0.15 |
|
Prospective | 6 | 0.93
(0.90–0.95) | 37.3 | 0.88
(0.82–0.92) | 35.1 | 109.86
(59.68–202.24) | 0 |
|
|
| Mean age,
years |
|
|
|
|
|
|
|
|
|
|
≥60 | 12 | 0.93
(0.91–0.95) | 48.7 | 0.83
(0.79–0.87) | 72 | 77.82
(50.39–120.20) | 25.5 | 0.51
(0.16–1.60) | 0.22 |
|
<60 | 3 | 0.89
(0.81–0.95) | 0 | 0.86
(0.76–0.93) | 0 | 55.62
(20.59–150.19) | 0 |
|
|
|
Unconfirmed | 1 | 0.89
(0.52–1.00) | 0 | 1.00
(0.03–1.00) | 0 | 17.00
(0.45–648.21) |
|
|
|
| Sex (female %) |
|
|
|
|
|
|
|
|
|
|
≥50 | 4 | 0.89
(0.81–0.95) | 0 | 0.86
(0.76–0.93) | 0 | 55.62
(20.59–150.19) | 0 | 0.74
(0.21–2.56) | 0.61 |
|
<50 | 11 | 0.93
(0.91–0.95) | 29.2 | 0.86
(0.82–0.89) | 53.8 | 75.15
(48.95–115.38) | 28.2 |
|
|
|
Unconfirmed | 1 | 0.89
(0.52–1.00) | 0 | 1.00
(0.03–1.00) | 0 | 17.00
(0.45–648.21) |
|
|
|
| Agent type |
|
|
|
|
|
|
|
|
|
|
SonoVue | 9 | 0.91
(0.88–0.94) | 1.1 | 0.83
(0.77–0.87) | 62.5 | 60.69
(35.52–103.68) | 0 | 1.54
(0.64–3.70) | 0.31 |
|
Sonazoid | 6 | 0.94
(0.91–0.96) | 61.2 | 0.84
(0.79–0.89) | 68.8 | 94.23
(52.04–170.61) | 24.7 |
|
|
|
Others | 1 | 0.89
(0.52–1.00) | 0 | 1.00
(0.03–1.00) | 0 | 17.00
(0.45–648.21) |
|
|
|
| Diagnostic
method |
|
|
|
|
|
|
|
|
|
|
Qualitative | 8 | 0.93
(0.89–0.95) | 29.4 | 0.77
(0.71–0.83) | 64.5 | 52.62
(30.29–91.43) | 0 | 1.91
(0.65–5.59) | 0.22 |
|
Quantitative | 8 | 0.93
(0.90–0.95) | 46.3 | 0.90
(0.85–0.93) | 0 | 101.89
(57.81–179.60) | 0 |
|
|
|
Endosonographer |
|
|
|
|
|
|
|
|
|
|
Expert | 10 | 0.94
(0.92–0.96) | 0 | 0.80
(0.75–0.84) | 62.0 | 69.14
(43.23–110.58) | 21.3 | 0.61
(0.17–2.15) | 0.41 |
|
Unconfirmed | 6 | 0.88
(0.84–0.92) | 13.3 | 0.90
(0.85–0.95) | 10.0 | 80.57
(38.97–166.55) | 0 |
|
|
| Lesion
characteristics |
|
|
|
|
|
|
|
|
|
|
Solid | 10 | 0.93
(0.91–0.95) | 18.5 | 0.82
(0.78–0.86) | 64.1 | 63.33
(41.17–97.43) | 12.8 | 1.46
(0.74–2.90) | 0.25 |
|
Cystic | 1 | 0.97
(0.83–1.00) | 0 | 0.75
(0.59–0.87) | 0 | 87.00
(10.46–723.40) |
|
|
|
|
Unconfirmed | 5 | 0.91
(0.86–0.95) | 62.6 | 0.94
(0.86–0.98) | 0 | 145.34
(46.35–455.78) | 0 |
|
|
| Lesion diameter,
mm |
|
|
|
|
|
|
|
|
|
|
≥30 | 10 | 0.92
(0.90–0.94) | 56 | 0.86
(0.82–0.90) | 52.7 | 87.27
(53.55–142.22) | 0 | 0.72
(0.4–12.8) | 0.24 |
|
<30 | 3 | 0.95
(0.90–0.98) | 0 | 0.80
(0.69–0.88) | 82.6 | 79.39
(26.43–238.43) | 39.9 |
|
|
|
Unconfirmed | 3 | 0.92
(0.85–0.96) | 0 | 0.78
(0.67–0.87) | 40.8 | 37.31
(15.88–87.65) | 0 |
|
|
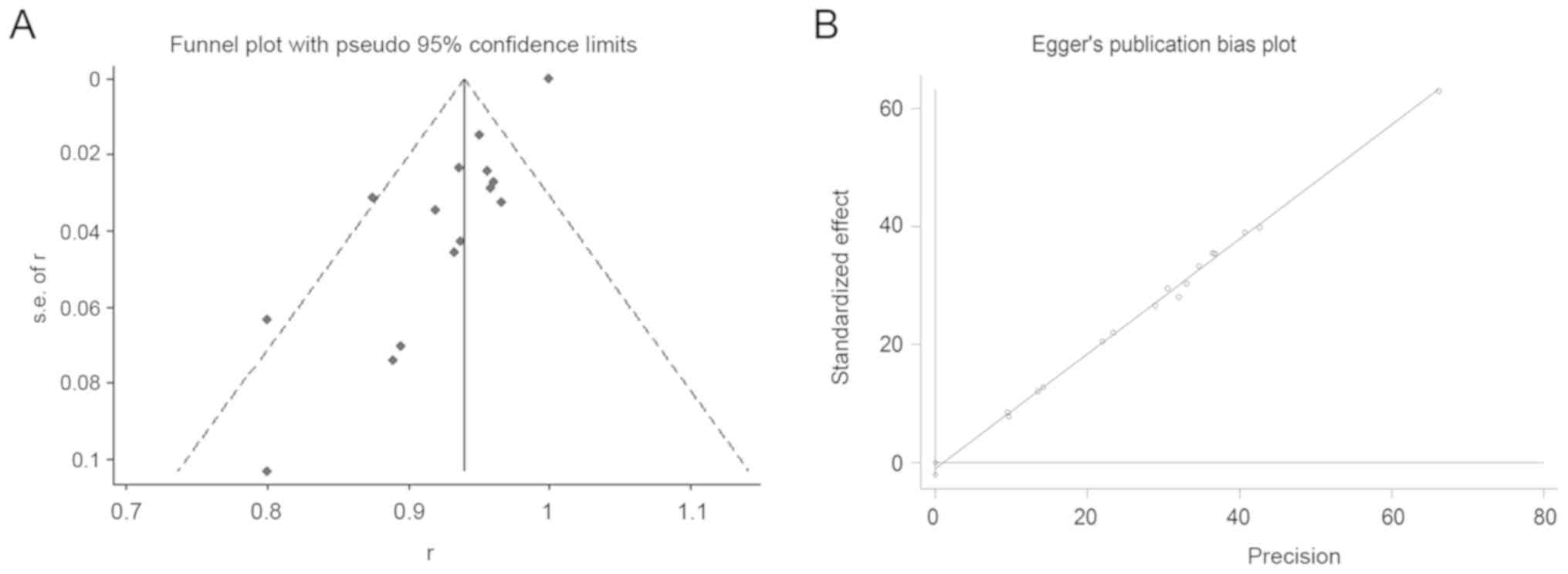
Publication bias
Assessment for the publication bias by funnel plot
construction revealed that 2 of the studies lay on the left of the
funnel plot, whereas 1 study was positioned to the right (Fig. 4A). Regarding the Egger's publication
bias plot, the distribution of spots was linear (Fig. 4B). Based on these results, no
publication bias was identified in this meta-analysis.
Discussion
There are numerous methods that can be employed in
order to differentially evaluate pancreatic masses, including
transabdominal ultrasound, computed tomography (CT) and magnetic
resonance imaging, among others. However, the sensitivity and
specificity of these traditional diagnostic methods are low,
particularly when the diameter of the tumor is <2 cm (20). EUS has been applied in the clinic for
decades, with some success. It is able to overcome the gas
interference associated with transabdominal ultrasound; therefore,
EUS has been established as a suitable method for differentiating
malignant from benign pancreatic masses. However, it is highly
affected by the experience of the endosonographer as regards EUS
image acquisition (21). EUS-FNA, a
technique derived from EUS, is a new diagnostic method by which
tissue samples of pancreatic masses are obtained for pathology
diagnosis. EUS-FNA has achieved diagnostic sensitivity and
specificity rates of up to 95 and 100%, respectively (22). However, EUS-FNA is invasive, and the
procedure is difficult and complicated. If the procedure is not
successful in obtaining positive tissue, repeat EUS-FNA is deemed
necessary. Contrast-enhanced EUS (CE-EUS) combines enhanced
ultrasonography with endoscopy. After injecting a contrast agent,
the blood flow signal of pancreatic tumors was found to be markedly
improved. Sakamoto et al (23) demonstrated that the sensitivity of
the diagnosis of pancreatic cancer was 94.4% with CE-EUS, which was
a significant improvement compared with enhanced CT. However, as an
earlier established enhancement type, Doppler enhancement is not
very sensitive to the small vessels of the pancreas and, therefore,
induces the so-called ‘flower’ phenomenon, which arises from the
fake blood flow signal. The emergence of CH-EUS, however, has made
up for these defects. CH-EUS was reported by Dietrich et al
as early as 2005 (24). This group
first used harmonic enhancement, another more efficient enhancement
mode, to observe the abdominal vessels. CH-EUS utilizes a selective
harmonic detection element that, when mounted at the front of the
endoscope, is able to detect the non-linear signal of the
intravascular microbubble produced by the contrast agent, while
filtering out the differential signal derived from the tissue and
avoiding hypo-enhancement with the heterogeneous pattern of the
pancreatic mass lesion. Upon CH-EUS imaging, pancreatic malignant
tissue exhibits low and uneven vascular enhancement, making it easy
to distinguish malignant from benign tissue. As a result, the
accuracy of CH-EUS in terms of diagnosis of pancreatic cancer was
found to be markedly improved (25,26).
To the best of the authors' knowledge, this is the
first systematic review and meta-analysis to estimate the
diagnostic performance of CH-EUS for the differentiation of
pancreatic masses since 2010, when CH-EUS was introduced by
Fusaroli et al (3). In this
meta-analysis, the characteristic ‘shoulder-arm’ shape of the data
point distribution was found to be lacking on the ROC plane. Of
note, no threshold was set in the sensitivity and specificity among
the 16 included studies. In the present review, the pooled
sensitivity was >90%, and the pooled specificity was also
>80%. It is well established that the likelihood ratios (PLR and
NLR) and DOR are reflections of the composite index of sensitivity
and specificity, which are more sensitive compared with sensitivity
and specificity alone. In the present review, the pooled PLR, NLR
and DOR also revealed that CH-EUS performed well in the diagnosis
of pancreatic masses. The area under SROC, identified to be 0.96,
was very close to 1. Furthermore, it was also demonstrated that the
country of origin, number of patients, study design, selection of
contrast enhancement agent, experience of the endosonographer,
lesion characteristics, ultrasound evaluation method, and an
additional 9 factors, did not have a significant impact on the
diagnostic performance of CH-EUS in terms of the differentiation of
the pancreatic mass by subgroup meta-analysis and meta-regression.
Finally, only articles published in English were searched in the
PubMed, EMBASE, Medline, Web of Science and Cochrane Library
databases, and the overall quality of a number of the studies
identified was not high. However, the literature publication bias
of these included 16 studies was acceptable. Based on the above
findings, and it was possible to conclude that CH-EUS performed
well as a technique in the differential diagnosis of pancreatic
masses.
In conclusion, the present study demonstrated that
CH-EUS is characterized by high accuracy for differentiating
between benign and malignant pancreatic space-occupying lesions,
and it also has the advantages of being non-invasive and
cost-effective. Therefore, it may prove to be an effective method
for the identification of benign and malignant pancreatic lesions
in the future.
Acknowledgements
Not applicable.
Funding
The present study was supported by an innovation
fund of the Jiangsu Hospital of Chinese Medicine (grant no.
Y2018CX57) and the second batch of scientific research special
projects for the construction of the National TCM Clinical Research
Base in 2015 (grant no. JDZX2015086).
Availability of data and materials
All data generated or analyzed during the present
study are included in this published article.
Authors' contributions
YL and DL scanned and identified the relevant
literature according to the inclusion and exclusion criteria. YL,
HJ, BQ and YZ wrote and modified parts of the manuscript. MX and SH
conceived the study and conducted a critical pre-submission review
of the manuscript. All the authors have read and approved the final
version of the manuscript for publication.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
EUS
|
endoscopic ultrasound
|
|
EUS-FNA
|
endoscopic ultrasound-guided
fine-needle aspiration
|
|
CE-EUS
|
contrast-enhanced endoscopic
ultrasound
|
|
PLR
|
positive likelihood ratio
|
|
NLR
|
negative likelihood ratio
|
|
DOR
|
diagnostic odds ratio
|
|
TP
|
true positive
|
|
FP
|
false positive
|
|
FN
|
false negative
|
|
TN
|
true negative
|
|
ROC
|
receiver operating characteristic
|
|
SROC
|
summary receiver operating
characteristic
|
|
AUC
|
area under the curve
|
|
QUADAS
|
Quality Assessment of Diagnostic
Accuracy Studies
|
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hackeng WM, Hruban RH, Offerhaus GJ and
Brosens LA: Surgical and molecular pathology of pancreatic
neoplasms. Diagn Pathol. 11:472016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Fusaroli P, Spada A, Mancino MG and
Caletti G: Contrast harmonic echo-endoscopic ultrasound improves
accuracy in diagnosis of solid pancreatic masses. Clin
Gastroenterol Hepatol. 8:629–634.e1-e2. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Gincul R, Palazzo M, Pujol B, Tubach F,
Palazzo L, Lefort C, Fumex F, Lombard A, Ribeiro D, Fabre M, et al:
Contrast-harmonic endoscopic ultrasound for the diagnosis of
pancreatic adenocarcinoma: A prospective multicenter trial.
Endoscopy. 46:373–379. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Whiting PF, Rutjes AW, Westwood ME,
Mallett S, Deeks JJ, Reitsma JB, Leeflang MM, Sterne JA and Bossuyt
PM; QUADAS-2 Group, : QUADAS-2: A revised tool for the quality
assessment of diagnostic accuracy studies. Ann Intern Med.
155:529–536. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Napoleon B, Alvarez-Sanchez MV, Gincoul R,
Pujol B, Lefort C, Lepilliez V, Labadie M, Souquet JC, Queneau PE,
Scoazec JY, et al: Contrast-enhanced harmonic endoscopic ultrasound
in solid lesions of the pancreas: Results of a pilot study.
Endoscopy. 42:564–570. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Seicean A, Badea R, Stan-Iuga R, Mocan T,
Gulei I and Pascu O: Quantitative contrast-enhanced harmonic
endoscopic ultrasonography for the discrimination of solid
pancreatic masses. Ultraschall Med. 31:571–576. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Matsubara H, Itoh A, Kawashima H, Kasugai
T, Ohno E, Ishikawa T, Itoh Y, Nakamura Y, Hiramatsu T, Nakamura M,
et al: Dynamic quantitative evaluation of contrast-enhanced
endoscopic ultrasonography in the diagnosis of pancreatic diseases.
Pancreas. 40:1073–1079. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Romagnuolo J, Hoffman B, Vela S, Hawes R
and Vignesh S: Accuracy of contrast-enhanced harmonic EUS with a
second- generation perflutren lipid microsphere contrast agent
(with video). Gastrointest Endosc. 73:52–63. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kitano M, Kudo M, Yamao K, Takagi T,
Sakamoto H, Komaki T, Kamata K, Imai H, Chiba Y, Okada M, et al:
Characterization of small solid tumors in the pancreas: The value
of contrast-enhanced harmonic endoscopic ultrasonography. Am J
Gastroenterol. 107:303–310. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Imazu H, Kanazawa K, Mori N, Ikeda K,
Kakutani H, Sumiyama K, Hino S, Ang TL, Omar S and Tajiri H: Novel
quantitative perfusion analysis with contrast-enhanced harmonic EUS
for differentiation of autoimmune pancreatitis from pancreatic
carcinoma. Scand J Gastroenterol. 47:853–860. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gheonea DI, Streba CT, Ciurea T and
Săftoiu A: Quantitative low mechanical index contrast-enhanced
endoscopic ultrasound for the differential diagnosis of chronic
pseudotumoral pancreatitis and pancreatic cancer. BMC
Gastroenterol. 13:22013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lee TY, Cheon YK and Shim CS: Clinical
role of contrast- enhanced harmonic endoscopic ultrasound in
differentiating solid lesions of the pancreas: A single-center
experience in Korea. Gut Liver. 7:599–604. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Park JS, Kim HK, Bang BW, Kim SG, Jeong S
and Lee DH: Effectiveness of contrast-enhanced harmonic endoscopic
ultrasound for the evaluation of solid pancreatic masses. World J
Gastroenterol. 20:518–524. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yamashita Y, Kato J, Ueda K, Nakamura Y,
Kawaji Y, Abe H, Nuta J, Tamura T, Itonaga M, Yoshida T, et al:
Contrast-enhanced endoscopic ultrasonography for pancreatic tumors.
Biomed Res Int 2015. 4917822015.
|
|
16
|
Săftoiu A, Vilmann P, Dietrich CF,
Iglesias-Garcia J, Hocke M, Seicean A, Ignee A, Hassan H, Streba
CT, Ioncică AM, et al: Quantitative contrast-enhanced harmonic EUS
in differential diagnosis of focal pancreatic masses (with videos).
Gastrointest Endosc. 82:59–69. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kamata K, Kitano M, Omoto S, Kadosaka K,
Miyata T, Yamao K, Imai H, Sakamoto H, Harwani Y, Chikugo T, et al:
Contrast-enhanced harmonic endoscopic ultrasonography for
differential diagnosis of pancreatic cysts. Endoscopy. 48:35–41.
2016.PubMed/NCBI
|
|
18
|
Iordache S, Costache MI, Popescu CF,
Streba CT, Cazacu S and Săftoiu A: Clinical impact of EUS
elastography followed by contrast-enhanced EUS in patients with
focal pancreatic masses and negative EUS-guided FNA. Med Ultrason.
18:18–24. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Uekitani T, Kaino S, Harima H, Suenaga S,
Sen-Yo M and Sakaida I: Efficacy of contrast-enhanced harmonic
endoscopic ultrasonography in the diagnosis of pancreatic ductal
carcinoma. Saudi J Gastroenterol. 22:198–202. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Krishna SG and Lee JH: Endosonography in
solid and cystic pancreatic tumors. J Interv Gastroenterol.
1:193–201. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kim J: Endoscopic ultrasound-guided
treatment of pancreatic cystic and solid masses. Clin Endosc.
48:308–311. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Eloubeidi MA, Jhala D, Chhieng DC, Chen
VK, Eltoum I, Vickers S, Mel Wilcox C and Jhala N: Yield of
endoscopic ultrasound-guided fine-needle aspiration biopsy in
patients with suspected pancreatic carcinoma. Cancer. 99:285–292.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sakamoto H, Kitano M, Suetomi Y, Maekawa
K, Takeyama Y and Kudo M: Utility of contrast-enhanced endoscopic
ultrasonography for diagnosis of small pancreatic carcinomas.
Ultrasound Med Biol. 34:525–532. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Dietrich CF, Ignee A and Frey H:
Contrast-enhanced endoscopic ultrasound with low mechanical index:
A new technique. Z Gastroenterol. 43:1219–1223. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wu RI, Yoon WJ, Brugge WR, Mino-Kenudson M
and Pitman MB: Endoscopic ultrasound-guided fine needle aspiration
(EUS-FNA) contributes to a triple-negative test in preoperative
screening of pancreatic cysts. Cancer Cytopathol. 122:412–419.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Wang Y, Yan K, Fan Z, Sun L, Wu W and Yang
W: Contrast- enhanced ultrasonography of pancreatic carcinoma:
Correlation with pathologic findings. Ultrasound Med Biol.
42:891–898. 2016. View Article : Google Scholar : PubMed/NCBI
|