Introduction
Leiomyomatosis peritonealis disseminata (LPD) is a
rare smooth muscle tumor, which is characterized by the
dissemination of multiple smooth muscle-like nodules throughout the
omental and peritoneal surfaces. This disease was first described
by Willson and Peale in 1952, and later designated as LPD by
Taubert et al in 1965 (1).
Since this disease is rarely reported, we herein describe a case of
LPD following laparoscopic myomectomy and myoma morcellation.
Case report
A 33-year-old woman was referred to the Obstetrics
and Gynecology Hospital of Fudan University (Shanghai, China) with
irregular hypogastralgia. The patient had a history of laparoscopic
myomectomy and myoma morcellation in 2009, and the pathology was
bizarre leiomyoma. During the first 2 years after surgery, the
patient remained asymptomatic and in 2011, she underwent a cesarean
section, without any abnormal findings during surgery. However, in
2014 the patient suffered from irregular episodes of right
abdominal pain. In January, 2014 a computerized tomography (CT)
scan of the epigastrium and pelvis in a local hospital revealed
multiple nodules located all over the omentum and pelvis, which was
suspicious for tumor metastasis. The serum carbohydrate antigen
(CA) 125 level was 19.6 U/ml (normal range, 0–35 U/ml). As the
serum CA125 level was within the normal range and the patient was
reluctant to undergo a second surgery, she opted for observation.
However, a contrast-enhanced CT in our hospital 9 months later
revealed that the nodules had increased in number and size, which
was highly suspicious of malignant uterine tumor metastasis or LPD;
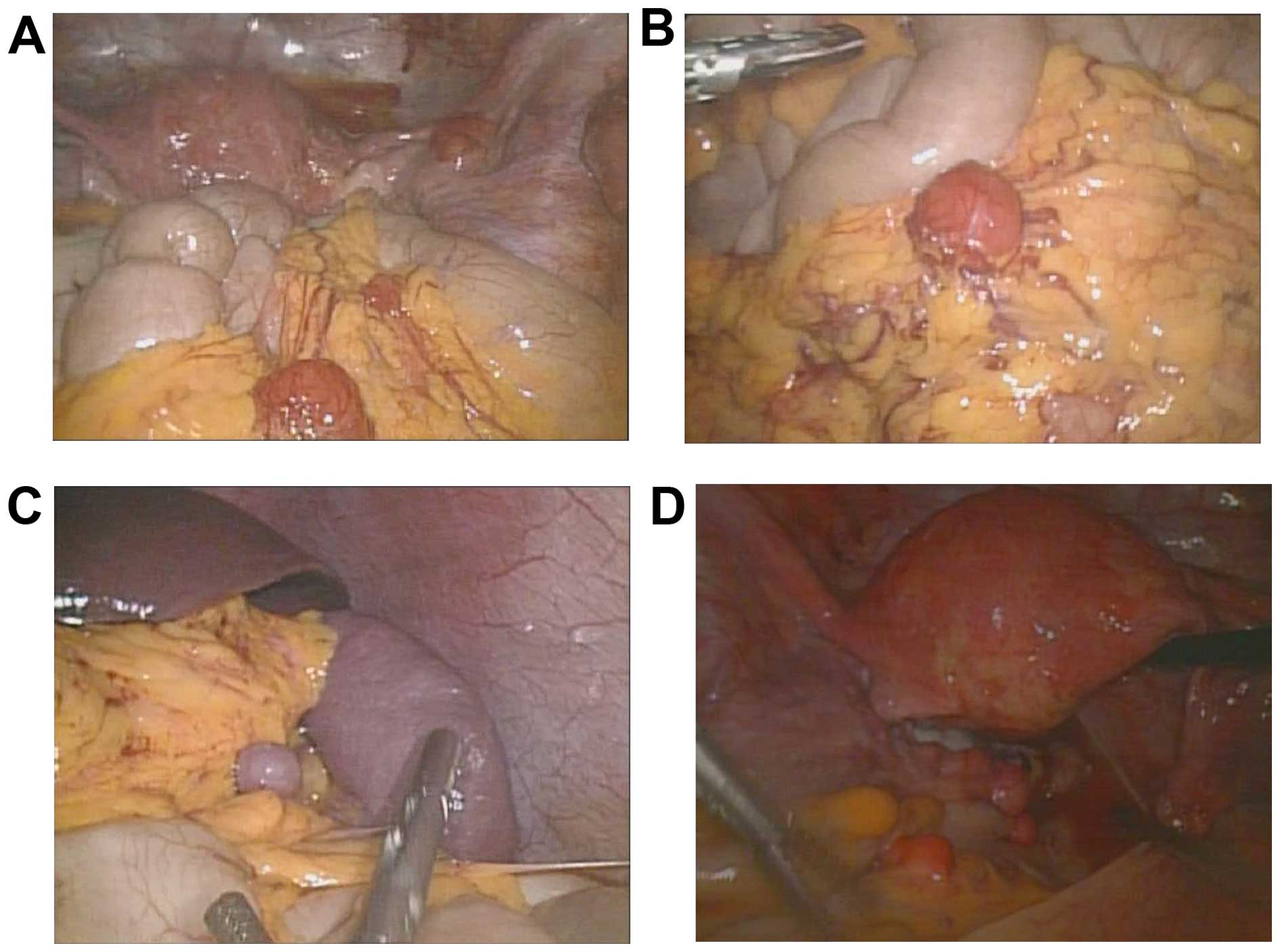
thus, the patient was scheduled to undergo laparoscopy. During this
procedure, numerous grey-red nodules were identified, measuring
1–20 mm in diameter, involving the mesentery, omentum, peritoneum,
Douglas's pouch, serosal surface of the small intestine, large
intestine and rectum (Fig. 1). In the
sigmoid colon, the nodules involved the entire muscular layer of
the colon. Frozen section pathology during surgery revealed the
condition to be LPD. As the patient was not planning to have more
children, she subsequently underwent laparoscopic total
hysterectomy, bilateral salpingo-oopherectomy, omental resection
and excision of some of the disseminated nodules. The final
histological examination confirmed the diagnosis of LPD. The
immunohistochemical examination for estrogen receptors (ER) was
positive, and for progesterone receptors (PR) 85% positive in the
nodules. The patient was followed up for 6 months, without any
signs of recurrence.
Written informed concent was provided for the
publication of the case details.
Discussion
LPD is a rare disease, with an etiology that remains
largely unknown. LPD consists of multiple nodules adherent to and
superficially invading the peritoneum, mimicking metastatic ovarian
carcinoma (2) and it occurs mainly in
premenopausal women (3). Frozen
section examination may help with the diagnosis, although the final
diagnosis relies on pathological examination.
The possible causes of LPD may be divided into
hormonal, subperitoneal mesenchymal stem cell metaplasia, genetic,
or iatrogenic, following myoma morcellation during laparoscopic
surgery (4).
Several authors have hypothesized that LPD occurs
due to unusual and selective sensitivity of subperitoneal
mesenchymal stem cells undergoing metaplasia. Travassoli and Norris
(5) suggested that this process was
promoted by hormonal stimulation. The finding of PR and ER
expression in the nodules support this hormonal theory. In
addition, the majority of patients with LPD were pregnant or taking
oral contraceptives at the time of diagnosis.
According to the genetic theory, based on clonal
analysis, certain authors have suggested that LPD results from the
implantation and proliferation of benign smooth muscle tissue or
cells originating from a uterine myoma. An abnormality in the X
chromosome and in other chromosomes, including chromosomes 17, 12
and 8, may indicate a common pathogenesis between uterine myomas
and LPD (6).
According to the US Food and Drug Administration
(http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm393576.htm),
laparoscopic power morcellation is associated with the risk of
spreading suspected cancerous tissue, notably uterine sarcomas,
beyond the uterus. There have also been increasing reports of
iatrogenic LPD following laparoscopic myomectomy and morcellation
(4).
Accurate diagnosis is difficult prior to surgery. On
magnetic resonance imaging, multiple masses with a signal intensity
similar to that of skeletal and smooth muscle were identified in
T1- and T2-weighted images.
Biopsies may be performed to collect tissue for
histopathological examination and confirmation of the diagnosis
(7).
LPD is a benign condition. However, cytological
atypia, nuclear polymorphism, hyperchromasia, tumor cell necrosis
and increased mitotic figures are histological signs of malignant
transformation.
LPD exhibits a benign biological behavior, and the
decline in sex hormone levels in the body, e.g., following surgical
castration, delivery, or discontinuation of birth control pills,
leads to regression of the disease. Ovarian suppression with a
gonadotropin-releasing hormone agonist may lead to shrinking of the
nodules (8). In women who have
completed their families, total abdominal hysterectomy,
salpingo-oophorectomy, omentectomy and debulking may be the optimal
treatment.
In conclusion, LPD is rare and difficult to
diagnose. The use of laparoscopic power morcellation may contribute
to the development of LPD; therefore, during morcellation, the
fragments of the myoma tissue should not be left in the abdominal
cavity, particularly in women who are planning a pregnancy.
Acknowledgements
The present study was supported by the National Key
Clinical Faculty Construction Program of China.
References
|
1
|
Taubert HD, Wisser SE and Haskins AL:
Leiomyomatosis disseminata; an unusual complication of genital
leiomyomata. Obstet Gynecol. 25:561–574. 1965.PubMed/NCBI
|
|
2
|
Verguts J, Orye G and Marquette S: Symptom
relief of leiomyomatosis peritonealis disseminata with ulipristal
acetate. Gynecol Sur. 11:57–58. 2014. View Article : Google Scholar
|
|
3
|
Tan CH, Ho BC, Shelat V and Tan CH:
Leiomyomatosis peritonealis disseminata presenting as omental
torsion. Singapore Med J. 53:e71–e73. 2012.PubMed/NCBI
|
|
4
|
Al-Talib A and Tulandi T: Pathophysiology
and possible iatrogenic cause of leiomyomatosis peritonealis
disseminata. Gynecol Obstet Invest. 69:239–244. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Travassoli FA and Norris HJ: Peritoneal
leiomyomatosis (leiomyomatosis peritonealis disseminata): A
clinicopathologic study of 20 cases with ultrastructural
observations. Int J Gynecol Pathol. 1:59–74. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Miyake T, Enomoto T, Ueda Y, Ikuma K,
Morii E, Matsuzaki S and Murata Y: A case of disseminated
peritoneal leiomyomatosis developing after laparoscope-assisted
myomectomy. Gynecol Obstet Invest. 67:96–102. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Halama N, Grauling-Halama SA and Daboul I:
Familial clustering of leiomyomatosis peritonealis disseminata: An
unknown genetic syndrome? BMC Gastroenterol. 5:332005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hales HA, Peterson CM, Jones KP and Quinn
JD: Leiomyomatosis peritonealis disseminata treated with a
gonadotropin-releasing hormone agonist. A case report. Am J Obstet
Gynecol. 167:515–516. 1992. View Article : Google Scholar : PubMed/NCBI
|