Introduction
Hepatic perivascular epithelioid cell neoplasm
(PEComa) is a rare mesenchyme-derived neoplasm that is primarily
composed of histologically distinctive perivascular epithelioid
cells (PECs), which share the expression of the monoclonal
antibody, HMB-45, smooth muscle cell markers and/or the melanocytic
differentiation marker, Melan-A (1).
In the majority of hepatic PEComas, adipocytes may also be found
intermixing with PECs in varying proportions (2). Larger tumors may have necrosis, or be
associated with hemorrhage. The imaging presentation of hepatic
PEComa is highly variable, and often leads to misdiagnosis as
hepatocellular carcinoma (HCC), hepatic hemangioma, or other liver
tumors (3–5). The clinical and histological
characteristics of PEComa have yet to be fully documented.
In the present study, the clinical data of 7
patients with hepatic PEComa admitted to the Sun Yat-Sen Memorial
Hospital were retrospectively analyzed. To optimize the diagnosis
and treatment of the disease, a systemic analysis was performed,
highlighting the clinical, imaging and pathological
characteristics.
Materials and methods
Patients and tissue specimens
Specimens from a total of 7 patients with hepatic
PEComa were collected at the Sun Yat-Sen Memorial Hospital, Sun
Yat-Sen University (Guangzhou, China) between January 2004 and
December 2015. The samples were obtained from surgery or biopsy,
with the patients' informed consent, and were histologically
confirmed. All tissue samples were derived from untreated patients,
fixed with formalin and embedded in paraffin.
Hepatic imaging
All patients were evaluated with imaging. A total of
4 patients underwent a computed tomography (CT) scan and
contrast-enhanced CT. The other 3 patients were examined with
magnetic resonance imaging (MRI), and 4 patients underwent
additional ultrasonography. Manifestation of the following
abnormalities was recorded: Morphology of the lesion, blood vessel
invasion, blood vessel displacement, bile duct invasion,
cholangiectasis and lymphadenectasis.
Statistical analysis
Statistical analysis was performed using SPSS
version 19.0 software (SPSS, Inc., Chicago, IL, USA). Continuous
variables were compared using analysis of variance, and were
expressed as the mean ± standard deviation.
Results
Clinical data
The median age of the 7 patients with hepatic PEComa
was 43 years old (range, 32–57 years), including 6 females (85.7%)
and 1 male (14.3%). A total of 4 patients (57.1%) were
asymptomatic, and the lesions were detected incidentally during
routine health check-ups. Two patients presented with abdominal
discomfort (28.6%). In the 7th patient (14.3%), who was suffering
from turberculous lymphadenitis, the initial symptoms were
emaciation and lymphadenectasis. All the patients denied having had
a history of viral hepatitis or drinking, with the exception of the
male patient. He had a 10-year history of alcohol abuse (Table I). Laboratory examinations revealed
normal liver function, with the exception of the male with a
history of alcohol abuse, who had a moderately elevated level of
alanine transaminase. Levels of the tumor markers [α-fetoprotein
(AFP), carcinoembryonic antigen (CEA) and cancer antigen 19–9
(CA19-9)] were within the normal range. One patient was identified
as being positive for hepatitis E virus immunoglobulin M (HEV-IgM;
Table II).
 | Table I.Clinical features of the 7 patients
with hepatic PEComa. |
Table I.
Clinical features of the 7 patients
with hepatic PEComa.
|
|
|
|
|
|
| Clinical
features | Personal history and
anamnesis |
|---|
|
|
|
|
|
|
|
|
|
|---|
| Case no. | Age (year) | Gender | Lesion location | Lesion amount | Size (cm) | Abdominal pain | Jaundice | Emaciation | Lymphadenectasis | Drinking history | Viral hepatitis | Other disease |
|---|
| 1 | 44 | F | Right lobe | 2 | 2.95×2.59,
0.8×0.8 | √ | N | N | N | N | N | N |
| 2 | 48 | F | Left lobe | 1 | 3.5×3.5×5 | N | N | N | N | N | N | N |
| 3 | 32 | F | Right lobe | 1 | 2.4×1.9 | N | N | N | N | N | N | N |
| 4 | 42 | F | Right lobe | 1 | 1.7×1.7 | √ | N | N | N | N | N | N |
| 5 | 37 | F | Left lobe | 1 | 5×3.2×3 | N | N | √ | √ | √ | N | Tuberculous
lymphadenitis, pulmonary tuberculosis, epidermoid cyst |
| 6 | 43 | M | Left lobe | 1 | 4×2.5×3 | N | N | N | N | N | N | N |
| 7 | 57 | F | Caudate lobe | 1 | 5×5x4.8 | N | N | N | N | N | N | N |
| Table II.Demographic characteristics of the 7
patients with hepatic PEComaa. |
Table II.
Demographic characteristics of the 7
patients with hepatic PEComaa.
| Characteristic | Value (mean ±
SD) |
|---|
| Total no. of
participants | 7 |
| Age, y | 43.29±7.95 |
| Gender, female,
% | 6 (85.7%) |
| TBIL, µmol/l | 11.40±4.47 |
| DBIL, µmol/l | 3.09±1.68 |
| Albumin, g/l | 44.67±4.51 |
| Hemoglobin, g/l | 128.14±4.98 |
| ALT, U/l | 18.86±15.26 |
| AST, U/l | 19.57±6.19 |
| AFP, µg/l | 3.06±2.03 |
| CEA, µg/l | 1.24±0.30 |
| CA19-9, U/ml | 13.14±7.99 |
| Viral hepatitis,
positive, % | 1 (14.28%) |
A total 6 out of the 7 patients had one lesion
(85.7%); the remaining patient had two lesions (14.3%). The tumors
originated from the right liver lobe in 3 patients (42.9%) from the
left lobe in 3 patients (42.9%), and from the caudate lobe in 1
patient (14.3%). With respect to tumor size, 3 patients (42.9%) had
a maximum diameter of the lesion of <3 cm, and 4 patients
(57.1%) had tumor sizes of between 3 and 5 cm.
Imaging characteristics
A total of 4 patients underwent CT (57.1%); the
other 3 patients were subjected to MRI (42.9%), and for 4 of the
patients (57.1%), additional ultrasonography was performed.
Generally speaking, all images demonstrated that the lesions were
of an ovoid shape with well-demarcated margins, with the exception
of one case subject, who exhibited no clear boundary. No blood
vessel or bile duct invasion was detected; neither was any
metastasis or infiltration of adjacent organs observed.
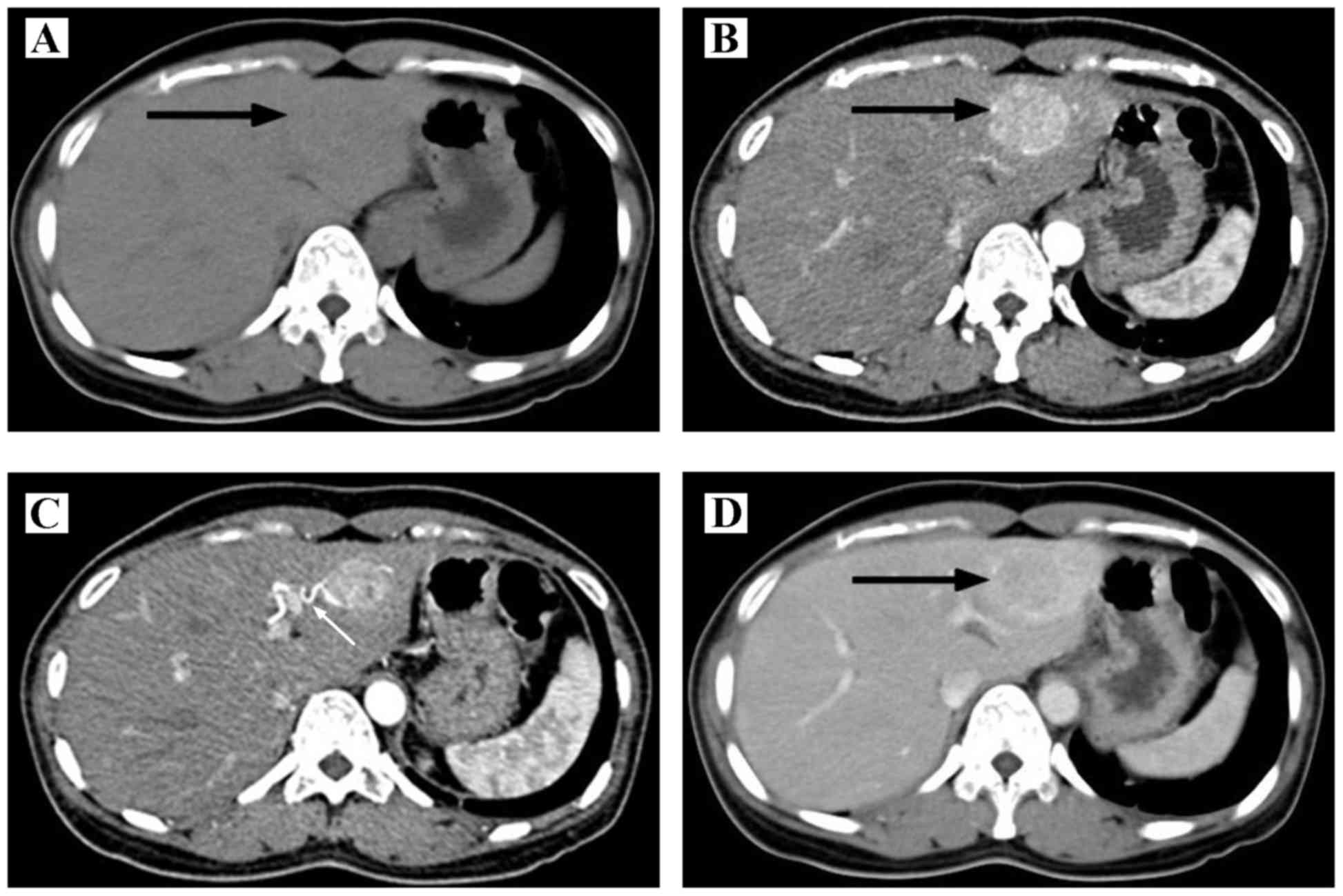
Concerning the 4 patients examined with ultrasound,
3 patients appeared with a hyperechoic mass (75%) and 1 patient
exhibited a hypoechoic mass (25%). In the 4 CT images, during the
scanning period, low dense (75%) or isodense (25%) lesions were
observed. Through the enhanced scanning, it was revealed that the
lesion became intensely enhanced in 3 patients (75%), with no clear
enhancement observed in 1 case (25%; Fig. 1). The images of portal and delay
phase were variable. In the MRI examination, the 3 cases all
exhibited a slightly hypointense signal on the T1 weighted image
(T1WI), and slight hyperintensity on the T2WI signal (100%).
However, the enhanced images were variable (Tables III and IV). Collectively, the correct diagnosis
rate was only 25% within the group of patients who underwent a CT
examination, and the use of ultrasonography or MRI failed to
contribute to the correct diagnosis for any of the patients
examined by these techniques. These cases predominantly had been
mistaken as HCC or hepatic hemangioma.
| Table III.Imaging characteristics of the 7
patients with hepatic PEComa. |
Table III.
Imaging characteristics of the 7
patients with hepatic PEComa.
|
| Ultrasonography | CT | MRI |
|---|
|
|
|
|
|
|---|
| Case no. | Echogeni-city | Preoperative
diagnosis | Density | Arterial phase | Portal phase | Delay phase | Preoperative
diagnosis | T1WI | T2WI | DWI | Enhanced scan | Preoperative
diagnosis |
|---|
| 1 | Hyperechoic | Hemangioma | Low density | No clear
enhancement | No clear
enhancement | No clear
enhancement | AML, hepatic
cyst | Not done | Not done | Not done | Not done | Not done |
| 2 | Hyperechoic | Hemangioma, HCC | Not done | Not done | Not done | Not done | Not done | Not done | Not done | Not done | Not done | Not done |
| 3 | Not done | Not done | Not done | Not done | Not done | Not done | Not done | Slightly
hypointense | Slightly
hyperintense | Restricted
diffusion | Intensely enhanced
in delay phase | HCC, atypical
adenoma |
| 4 | Slightly
hyperechoic | Undetermined | Not done | Not done | Not done | Not done | Not done | Slightly
hypointense | Slightly
hyperintense | Not done | Peri- pherally
enhanced | Metastasis
tumor |
| 5 | Not done | Not done | Isodense | Intensely
enhanced | Slightly lower than
liver parenchyma | Slightly lower than
liver parenchyma | HCC | Hypointense | Slightly
hyperintense | Not done | Lower than the
liver parenchyma | HCC |
| 6 | Hypoechoic | Hemangioma | Low density | Intensely
enhanced | Persistently
enhanced, peripherally enhanced | Slightly low
density | Hemangioma | Not done | Not done | Not done | Not done | Not done |
| 7 | Not done | Not done | Low density | Hetero- geneously,
intensely enhanced | Lower than the
liver parenchyma | Lower than the
liver parenchyma | HCC | Not done | Not done | Not done | Not done | Not done |
| Table IV.Morphology and invasive signs of the
lesions in the 7 patients with hepatic PEComa. |
Table IV.
Morphology and invasive signs of the
lesions in the 7 patients with hepatic PEComa.
|
| Morphology | Blood vessel and
bile duct |
|
|---|
|
|
|
|
|
|---|
| Case no. | Shape | Boundary | Blood vessel
invasion | Blood vessel
displacement | Bile duct
invasion |
Cholangiectasis |
Lymphadenectasis |
|---|
| 1 | Oval | Clear | N | N | N | N | N |
| 2 | Oval | Clear | N | N | N | N | N |
| 3 | Oval | Clear | N | Right
portal vein | N | N | N |
| 4 | Oval | Unclear | N | N | N | N | N |
| 5 | Oval | Clear | N | N | N | N | √ |
| 6 | Oval | Clear | N | N | N | N | N |
| 7 | Oval | Clear | N | Inferior vena
cava | N | N | N |
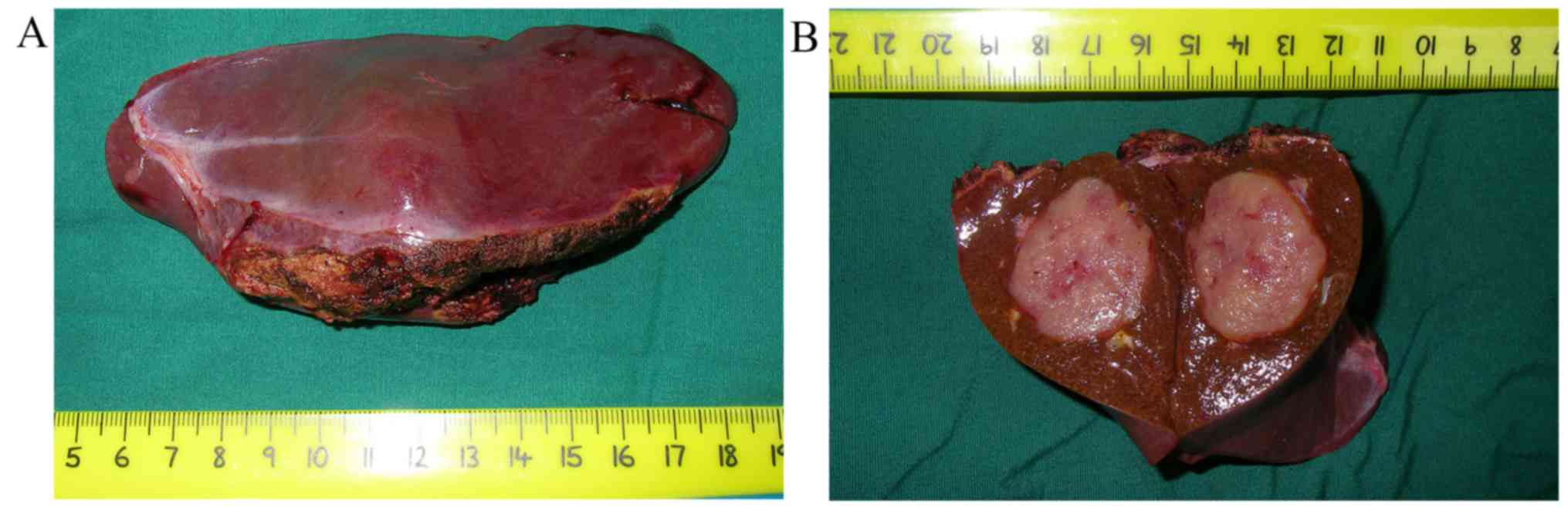
Pathological features
A total of 6 patients underwent partial hepatectomy.
Generally speaking, soft or firm, well-circumscribed nodular masses
with a yellow, yellow-tan, gray-red or tan appearance were observed
(Fig. 2). One of our cases presented
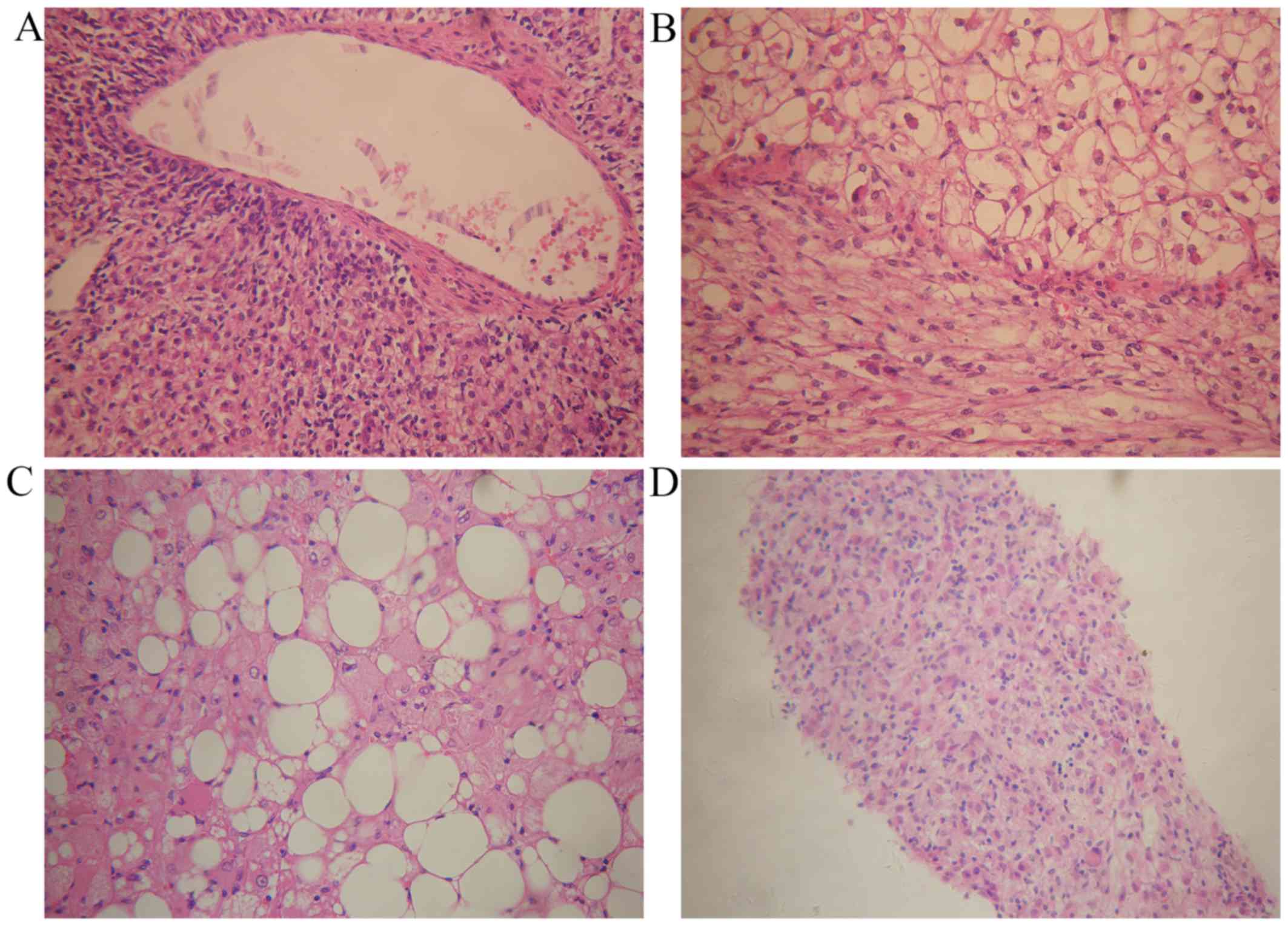
a cyst inside the lesion. Microscopically, epithelioid or
spindle-shaped cells were identified. Adipocytes were identified in
5 specimens (83.3%; Fig. 3A-C). Fine
needle aspiration biopsy (FNAB) was performed for 2 patients.
Microscopy revealed epithelioid cells with pale, clear,
eosinophilic cytoplasm or foamy cytoplasm. The nuclei were round to
oval with small nucleoli, and inclusions were observed in a few of
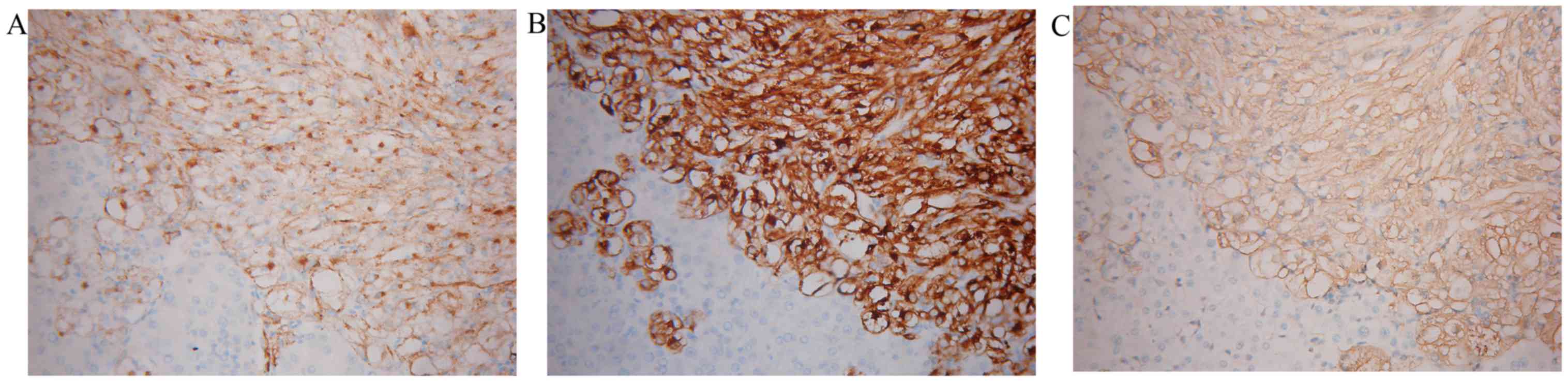
the cells (Fig. 3D). Mitotic figures
were rarely identified. Finally, markedly positive staining for
HMB-45, Melan-A and SMA was observed in all patients (Fig. 4).
Treatment and prognosis
A total of 6 patients received surgical treatments,
including laparotomic and laparoscopic partial hepatectomy. One
patient received tumor arterial embolization (TAE) and percutaneous
microwave coagulation therapy (PMCT). None of the patients had
received chemotherapy or radiation therapy prior to or following
the tumor resection. No patient suffered from postoperative
complications or died during the perioperative period. After a
follow-up period of 12–20 months, no recurrence occurred.
Discussion
PEComas are predominantly diagnosed in the kidney,
and cases of sporadic hepatic PEComa have been reported worldwide.
The majority of cases of hepatic PEComa are found asymptomatically,
and have normal serological test results (6), which makes it difficult to diagnose the
disease. It has been reported that hepatic PEComas predominantly
affect women aged 30–50 years old (5), which is in accordance with our cases.
Certain case studies have reported hepatic PEComa presented as
acute or chronic abdominal pain (7,8), and 2
patients among our case subjects revealed abdominal pain. However,
the majority of them routinely lack specific clinical symptoms and
serological abnormalities. Hepatic PEComa may occur as a solitary
mass or as multiple lesions, and a higher frequency of multiple
masses have been suggested to be associated with tuberous sclerosis
(9).
Clinically, a preoperative diagnosis of a hepatic
lesion is primarily dependent on imaging examinations. Due to the
highly variable histological composition of hepatic PEComa, these
tumors often do not possess typical imaging characteristics. On
ultrasonography, hepatic PEComa presents as any echogenicity. Early
influx into the tumor and rapid drainage of arterial blood to
veins, as determined on performing contrast-enhanced
ultrasonography, may be a feature of PEComa (10). As mentioned above, adipocytes may be
identified intermixing with PECs in varying proportions. Thus, MRI
is preferable compared with CT for detecting fat, which appears
with a high signal intensity (11).
However, it is also difficult to make a diagnosis when the tumors
contain a much lower fatty content.
How to make a correct preoperative diagnosis is a
topic worthy of investigation. FNAB has been considered to be
mandatory for the majority of patients, and histological diagnosis
is based on the identification of the different components.
Microscopically, epithelioid cells, spindled cells and adipocytes
may be identified, which prompt pathologists to take hepatic PEComa
into account. Typically, PECs radially arrange around the vascular
lumen. They exhibit small, centrally placed, normochromatic,
round-to-oval nuclei with small nucleoli, although striking
hyperchromasia and nuclear irregularity may be present (1). As noted above, adipocytes may also be
identified intermixing with PECs in varying proportions. The PECs
are characterized by positivity with melanocytic markers and muscle
markers (12). The most noteworthy
immunological markers include HMB-45, Melan-A and SMA, and
negativity for multiple markers, including cytokeratin, CD117, AFP,
hepatocytes and chromogranin, confirmed the diagnosis (13).
Due to the rarity of the disease, there are clear
difficulties associated with performing a therapeutic trial, and
the management of hepatic PEComa remains controversial. The
overwhelming majority of reported PEComas reveal a benign pattern.
However, there are certain cases that imply invasive growth, with
distant metastasis or recurrences (14–16).
There is not yet a uniform standard for evaluating the malignant
degree of hepatic PEComa. The majority of the reported patients
received surgical resection soon after the identification of the
tumors, since most of the tumors were preoperatively misdiagnosed
as HCC or hepatic metastasis. Postoperative complications or
recurrence are rarely reported. In the present study, 6 patients
received surgical treatments, including laparotomic and
laparoscopic partial hepatectomy. One patient received TAE and
PMCT. None of the patients suffered from postoperative
complications or recurrence in the present study. Due to its benign
tendency, several researchers have suggested that, when hepatic
PEComa is suspected, a fine-needle aspiration combined with HMB-45
staining should be performed in all asymptomatic patients with a
lesion <5 cm and without serological abnormalities (17). If the diagnosis is confirmed by FNAB
and the pathomorphology indicates a benign pattern, careful
observation with serial imaging follow-up is recommended (17,18). For
a lesion >5 cm, in cases of progressive enlargement, if the
patient has clinical symptoms, or if the FNAB indicates a malignant
tendency, a more aggressive approach should be undertaken. Due to
the rarity of reports, the exact effects of these therapies have
yet to be elucidated. As the majority of previous studies and the
present study have shown, patients who undergo surgical resection
may expect a good outcome, and therefore surgical resection remains
the recommended choice for hepatic PEComa therapy.
Acknowledgements
This research was supported by a grant from the
Natural Science Foundation of China (no. 81572348), the Science and
Technology Project of Guangdong Province (no. 2013B021800099) and
the Science and Technology Program of Guangzhou (no.
201510010206).
References
References
|
1
|
Fletcher CDM, Unni KK and Mertens F:
Pathology and Genetics of Tumours of Soft Tissue and Bone. Lyon:
IARC Press; pp. 201–202. 2002
|
|
2
|
Hamilton SR and Aaltonen LA: Pathology and
Genetics of Tumours of the Digestive System. Lyon: IARC Press; pp.
1932000
|
|
3
|
Lu HC, Chau GY and Su CW: Clinical
challenges and images in GI. Diagnosis: Hepatic angiomyolipoma
mimicking hepatocellular carcinoma. Gastroenterology. 136:1169,
14642009.PubMed/NCBI
|
|
4
|
Xie L, Jessurun J, Manivel JC and
Pambuccian SE: Hepatic epithelioid angiomyolipoma with trabecular
growth pattern: A mimic of hepatocellular carcinoma on fine needle
aspiration cytology. Diagn Cytopathol. 40:639–650. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zeng JP, Dong JH, Zhang WZ, Wang J and
Pang XP: Hepatic angiomyolipoma: A clinical experience in diagnosis
and treatment. Dig Dis Sci. 55:3235–3240. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tryggvason G, Blöndal S, Goldin RD,
Albrechtsen J, Bjornsson J and Jonasson JG: Epithelioid
angiomyolipoma of the liver: Case report and review of the
literature. APMIS. 112:612–616. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zimmermann A, von der Brelie C, Berger B,
Kappeler A and Candinas D: Primary perivascular epithelioid cell
tumor of the liver not related to hepatic ligaments: Hepatic PEComa
as an emerging entity. Histol Histopathol. 23:1185–1193.
2008.PubMed/NCBI
|
|
8
|
Priola AM, Priola SM, Cataldi A, Marci V
and Fava C: Acute abdomen as an unusual presentation of hepatic
PEComa. A case report. Tumori. 95:123–128. 2009.PubMed/NCBI
|
|
9
|
Fricke BL, Donnelly LF, Casper KA and
Bissler JJ: Frequency and imaging appearance of hepatic
angiomyolipomas in pediatric and adult patients with tuberous
sclerosis. AJR Am J Roentgenol. 182:1027–1030. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Akitake R, Kimura H, Sekoguchi S, Nakamura
H, Seno H, Chiba T and Fujimoto S: Perivascular epithelioid cell
tumor (PEComa) of the liver diagnosed by contrast-enhanced
ultrasonography. Intern Med. 48:2083–2086. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Prasad SR, Wang H, Rosas H, Menias CO,
Narra VR, Middleton WD and Heiken JP: Fat-containing lesions of the
liver: Radiologic-pathologic correlation. Radiographics.
25:321–331. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Folpe AL and Kwiatkowski DJ: Perivascular
epithelioid cell neoplasms: Pathology and pathogenesis. Hum Pathol.
41:1–15. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Martignoni G, Pea M, Reghellin D, Zamboni
G and Bonetti F: PEComas: The past, the present and the future.
Virchows Arch. 452:119–132. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Dalle I, Sciot R, de Vos R, Aerts R, van
Damme B, Desmet V and Roskams T: Malignant angiomyolipoma of the
liver: A hitherto unreported variant. Histopathology. 36:443–450.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Nguyen TT, Gorman B, Shields D and Goodman
Z: Malignant hepatic angiomyolipoma: Report of a case and review of
literature. Am J Surg Pathol. 32:793–798. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kamimura K, Oosaki A, Sugahara S, Mori S,
Moroda T, Satoh O, Morita T, Kimura K, Kamura T, Nomoto M and
Aoyagi Y: Malignant potential of hepatic angiomyolipoma: Case
report and literature review. Clin J Gastroenterol. 3:104–110.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Yang L, Xu Z, Dong R, Fan J, Du Y, Zhang
Y, Wang X, Cheng X and Guo J: Is surgery necessary for patients
with hepatic angiomyolipoma? Retrospective analysis from eight
Chinese cases. J Gastroenterol Hepatol. 28:1648–1653.
2013.PubMed/NCBI
|
|
18
|
Belghiti J, Cauchy F, Paradis V and
Vilgrain V: Diagnosis and management of solid benign liver lesions.
Nat Rev Gastroenterol Hepatol. 11:737–749. 2014. View Article : Google Scholar : PubMed/NCBI
|