Introduction
We encountered a case of extraskeletal osteosarcoma
of the lung following chemoradiotherapy for small-cell lung
carcinoma (SCLC). Primary pulmonary osteosarcoma is a rare entity,
with only a few cases reported in the literature to date (1–5). Miller
et al (6) reported the
incidence of primary pulmonary osteosarcoma as 0.01%. Niimi et
al (7) reviewed the 20 cases of
primary pulmonary osteosarcoma, and the age on onset was 33–81
years old, male/female ratio was 1:1 and the most common site was
left lung. Most of patient died within a year on onset symptom.
Moreover, secondary osteoskeletal osteosarcoma of the lung
following chemoradiotherapy is extremely rare and, to the best of
our knowledge, this is the first case reported to date.
Case report
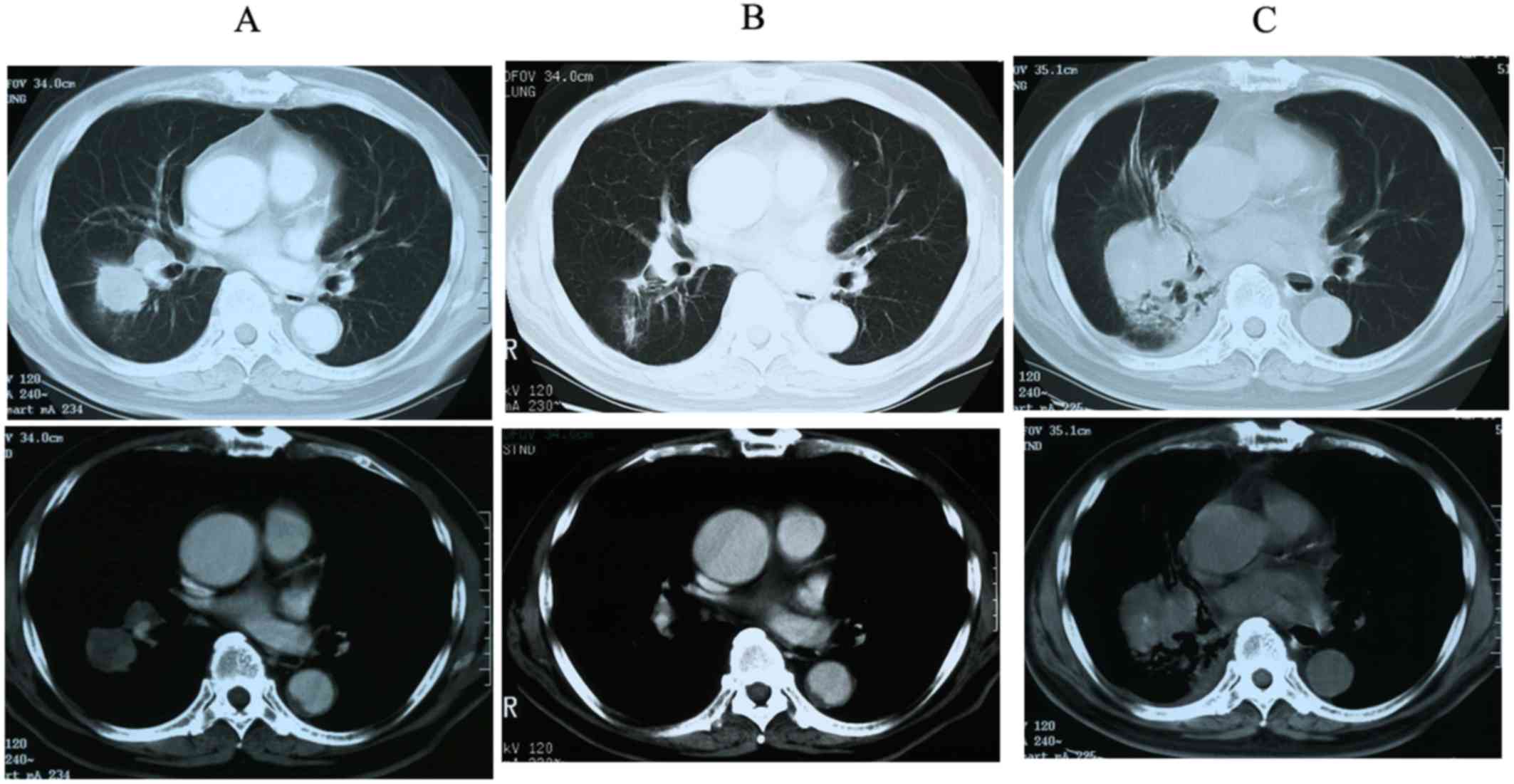
An 80-year-old male patient had been diagnosed with
SCLC of middle lower lobe of the right lung (Fig. 1A) via brushing cytology at the
Obihiro Kosei General Hospital (Obihiro, Japan) in December 2001
and treated with chemoradiotherapy (cisplatin, 80 mg/m2,
130 mg, Day 1; etoposide, 100 mg/m2, 170 mg, Day 1–3)
and accelerated hyperfractionation (AHF) at a dose of 45 Gy/30 fr.
After 4 cycles of chemotherapy, a partial response to the treatment
was observed (Fig. 1B). However, the
disease recurred locally 3 years later, and the patient was again
admitted to our hospital for second-line chemotherapy. The
patient's chest computed tomography (CT) scan revealed an
oval-shaped tumor in the same region of the lung that had been
previously affected (Fig. 1C). The
lesion was not evaluated by pathological examination, as its
location was the same as that at the initial diagnosis of SCLC,
thus, it was considered to be a recurrence of the primary tumor and
it was treated with carboplatin (AUC=4, 330 mg, Day 1) and
irinotecan (CPT-11; 60 mg/m2, 100 mg, Day 1, 8 and 15)
as second-line chemotherapy. As the cancer did not respond
sufficiently to this treatment, third-line amrubicin hydrochloride
(AMR; 30 mg/m2, 50 mg, Day 1–3) was administered.
Unfortunately, the patient's performance status (PS) decreased,
despite treatment. Chemotherapy was discontinued after the first
cycle and followed by best supportive care (BSC). During the second
hospitalization for second- and third-line chemotherapy, the
patient developed a cerebral infarction, causing permanent
paralysis in the lower half of his body.
The patient was again admitted to our hospital after
sustaining a second cerebral infarction. At that point, his PS was
4, and retention of the pleural effusion in the right thoracic
cavity was detected. A chest tube was inserted to drain the fluid
from the lungs; however, the cytology of the pleural effusion was
not examined and the patient was clinically diagnosed with
pleuritis carcinomatosa. Treatment for a pleural adhesion using
OK-432 was administered, which exacerbated his general condition.
The patient ultimately succumbed to cancer progression in January
2005. The patient diagnosed as SCLC in December 2001, treated with
chemoradiotherapy for 4 months. Local recurrence was observed in
January 2004, second and third line chemotherapy was enforced in
February to April 2004 but the effect was no change. The patient's
PS decreased and had a first cerebral infarction in May 2004. BSC
then followed, but second cerebral infarction occurred in June
2004. The patient was also diagnosed clinically as pleuritis
carcinomatosa, and pleural adhesion was treated with OK-432. The
patient died of cancer progression in January 2005.
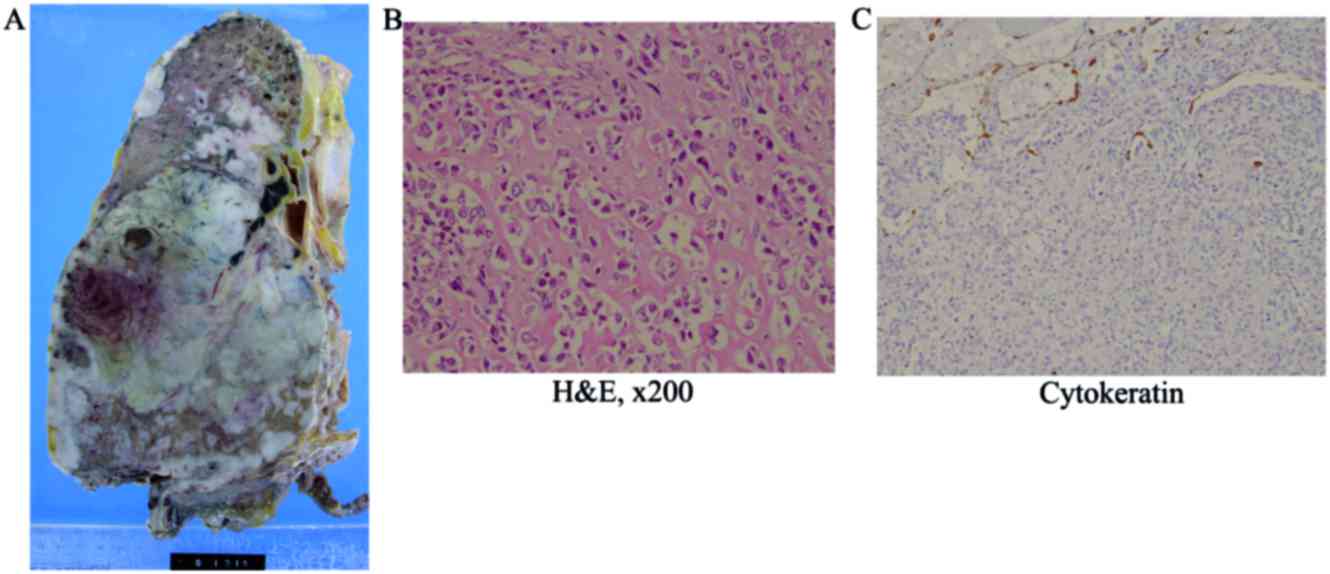
A postmortem examination was performed, and a large
tumor measuring 14 cm was identified in the middle lower lobe of
the right lung (Fig. 2A). On the cut
surface, the tumor was grayish-white and focally necrotic.
Histologically, the lung parenchyma was diffusely infiltrated by
atypical spindle to round cells, with lacy osteoid matrix, bone
trabeculae, focal chondroid differentiation, and osteoclastic giant
cells (Fig. 2B). Although the right
pleura, diaphragm, right bronchus and primary hilum were
macroscopically affected by the tumor, the ribs and vertebral bones
appeared to be intact. Extrathoracic metastasis was not detected.
Immunohistochemically, the tumor cells were positive for vimentin,
but negative for pan-cytokeratin (Fig.
2C). These findings were compatible with osteoblastic-type
extraskeletal osteosarcoma. Despite thorough histological
examination, SCLC was not detected in the autopsy material.
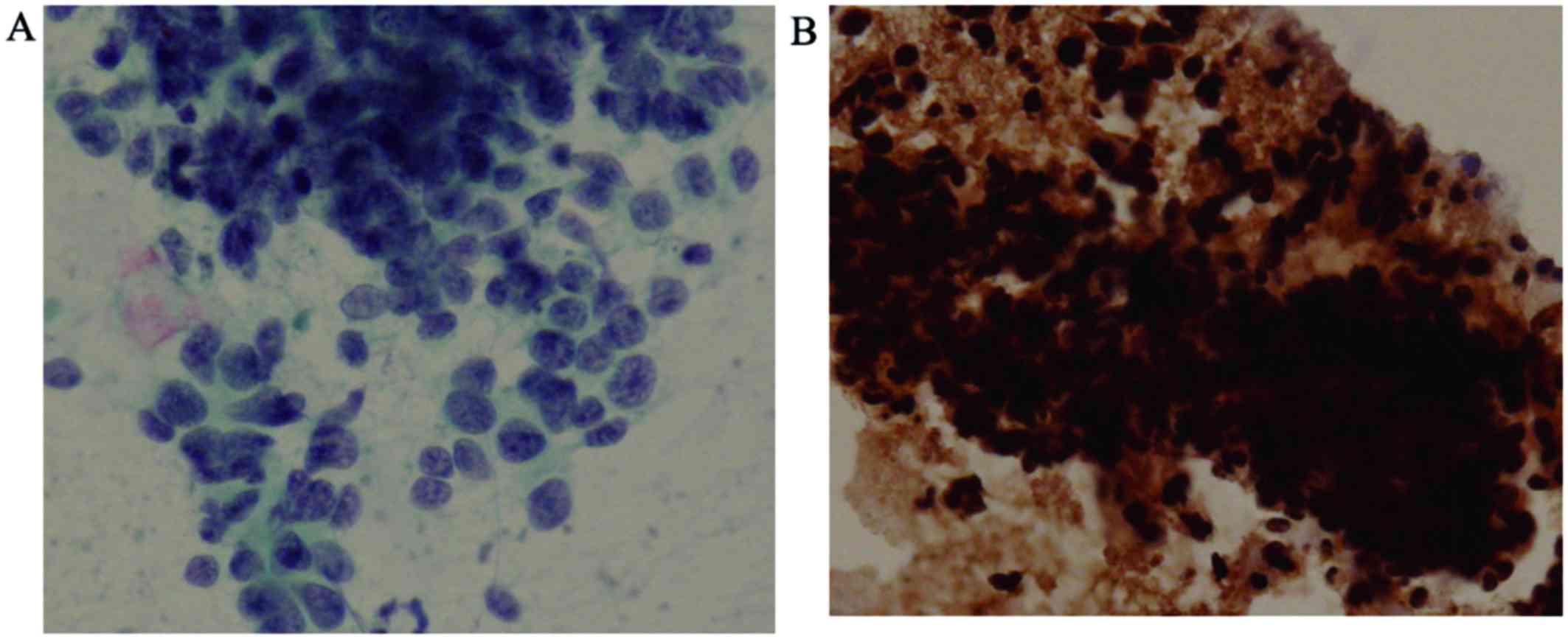
The initial brushing cytology revealed clusters of
undifferentiated small cells with a high nuclear-cytoplasmic ratio
and dense hyperchromatic nuclei, which are findings typical of SCLC
(Fig. 3A). No sarcomatous components
were found on retrospective examination; additionally, these cells
were positive for pan-cytokeratin (Fig.
3B), but immunohistochemically negative for vimentin, which is
the opposite of what was observed in the autopsy material.
Discussion
In the case presented herein, the patient was
diagnosed with SCLC and was treated with chemoradiotherapy.
Clinically, the patient responded partially to the treatment.
However, the tumor relapsed and additional chemotherapy was
administered. The tumor did not respond to second-line
chemotherapy, and the PS of the patient deteriorated. BSC was
selected as the next mode of treatment; however, the patient
succumbed to disease progression. A CT scan revealed that the new
lesion was in the same location as the primary tumor, and it was
initially diagnosed as SCLC recurrence. However, SCLC tissue was
not identified on postmortem examination, and the tumor was instead
diagnosed as osteosarcoma. Therefore, this is an extremely rare
case of extraskeletal osteosarcoma of the lung following treatment
for SCLC with chemoradiotherapy.
The main question is why osteosarcoma occurred in
the thoracic cavity following chemoradiotherapy for the primary
lung carcinoma. To explain this, three possibilities were
considered as follows: The first possibility is that the tumor was
a mixed carcinoma and sarcoma. Primary pulmonary osteosarcomas are
generally extremely rare, with only a few cases reported in the
literature to date (1–5). The origin of the carcinoma in most
cases of primary pulmonary carcinosarcoma is non-SCLC (8). Cases involving the combination of SCLC
and sarcoma have been reported, but the primary sites for these
tumors were the urinary tract or gallbladder (9,10),
rather than the lungs. In the present case, the first diagnosis was
based on the cytology of bronchoscopically obtained material, so it
is possible that the tumor sample was insufficient to detect the
sarcomatous components. However, the cytology findings revealed
proliferation of tumor cells with small nuclei and epithelial
intercellular connections, whereas no sarcomatous component was
detected. Immunohistochemical examination was positive for
cytokeratin, a marker of epithelial cells. The patient's tumor was
reduced in size following chemoradiotherapy for SCLC. In addition,
CPT-11 and AMR were administered as second- and third-line
chemotherapy, respectively, which were unable to suppress tumor
progression. This patient initially responded to anticancer therapy
for SCLC, suggesting that he had primary SCLC or carcinosarcoma of
the lung, in which the SCLC component was dominant at the initial
diagnosis.
The second possibility is histological
transformation of the carcinoma to sarcoma. Another case in which
SCLC transformed into another type of carcinoma after chemotherapy
has been reported (11). In a number
of cases, however, transformation to other histological types, such
as adenocarcinoma, squamous cell carcinoma, and large-cell
carcinoma has been reported. Transformation from an epithelial
tumor, such as SCLC, to a mesenchymal tumor is extremely rare and,
to the best of our knowledge, such a case has not been reported to
date. There is a possibility that the chemoradiotherapy promoted a
gene mutation, with subsequent transformation of carcinoma to
sarcoma.
The last possibility involves the effects of
radiotherapy. Cahn et al studied post-irradiation
osteosarcoma occurring within the irradiation area after a latency
period of several years. The histology of the tumors examined later
in this period was found to be different from those of the primary
lesion (12). In the present case,
the post-irradiation osteosarcoma fulfilled two of these criteria.
However, in the majority of the cases, osteosarcoma occurs in bone
and soft tissue, rather than in the vital organs. Kondo et
al reported a case of pleuropulmonary blastoma with accelerated
cartilaginous differentiation following chemotherapy and radiation
(13). In that study, the authors
suggested the possibility that this treatment was the cause of the
cartilaginous differentiation.
It is hypothesized that the tumor described herein
was a mixed carcinoma and sarcoma, or was due to a gene mutation
promoting the transformation of SCLC to osteosarcoma precipitated
by chemoradiotherapy. In conclusion, it is necessary to take into
consideration the possibility of osteosarcoma when recurrence of
primary lung carcinoma occurs following chemoradiotherapy
treatment. Further examination of this pathological entity is
required to fully elucidate the mechanism underlying the occurrence
of this phenomenon.
Written informed consent was obtained from the
patient for publication of this case report and accompanying
images, and no conflict of interest was declared.
References
|
1
|
Chapman AD, Pritchard SC, Yap WW, Rooney
PH, Cockburn JS, Hutcheon AW, Nicolson MC, Kerr KM and McLeod HL:
Primary pulmonary osteosarcoma: Case report and molecular analysis.
Cancer. 91:779–784. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tatsuaki W, Takashi I, Jotaro S, et al:
Primary osteosarcoma of the lung. Nihon Kokyuki Geka Gakkai Zasshi
Jpn. 49:823–827. 2010.(In Japanese).
|
|
3
|
Kadowaki T, Hamada H, Yokoyama A, Katayama
H, Abe M, Nishimura K, Tomiyama N, Kito K, Miyazaki T and Higaki J:
Two cases of primary pulmonary osteosarcoma. Intern Med.
44:632–637. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Nakata Y, Kubota A, Ueno Y, et al: An
autopsy case of Primary pulmonary ostegenic sarcoma. Byori Rinsho
Jpn. 5:87–90. 1987.(In Japanese).
|
|
5
|
Niimi R, Matsumine A, Kusuzaki K, et al:
Primary osteosarcoma of the lung: A case report. Seikeigeka Jpn.
55:313–316. 2005.(In Japanese).
|
|
6
|
Miller DL and Allen MS: Rare pulmonary
neoplasms. Mayo Clin Proc. 68:pp. 492–498. 1993; View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Niimi R, Matsumine A, Kusuzaki K, Inada Y,
Kato Y, Maeda M and Uchida A: Primary osteosarcoma of the lung: A
case report and review of the literature. Med Oncol. 25:251–255.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Koss MN, Hochholzer L and Frommelt RA:
Carcinosarcomas of the lung: A clinicopathologic study of 66
patients. Am J Surg Pathol. 23:1514–1526. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Takahashi Y, Fukushima J, Fukusato T and
Shiga J: Sarcomatoid carcinoma with components of small cell
carcinoma and undifferentiated carcinoma of the gallbladder. Pathol
Int. 54:866–871. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ishida M, Iwai M, Yoshida K, Kagotani A
and Okabe H: Sarcomatoid carcinoma with small cell carcinoma
component of the urinary bladder: A case report with review of the
literature. Int J Clin Exp Pathol. 6:1671–1676. 2013.PubMed/NCBI
|
|
11
|
Le Vu B, de Vathaire F, Shamsaldin A,
Hawkins MM, Grimaud E, Hardiman C, Diallo I, Vassal G, Bessa E,
Campbell S, et al: Radiation dose, chemotherapy and risk of
osteosarcoma after solid tumours during childhood. Int J Cancer.
77:370–377. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Cahan WG, Woodard HQ, Higinbotham NL,
Stewart FW and Coley BL: Sarcoma arising in irradiated bone: Report
of eleven cases 1948. Cancer. 82:8–34. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kondo Y, Anami Y, Iijima T, Noguchi M,
Watanabe M and Kaneko M: A case of pleuropulmonary blastoma with
accelerated cartilage differentiation after chemotherapy and
radiational therapy. Jap J Lung Cancer. 46:167–169. 2006.(In
Japanese). View Article : Google Scholar
|