Introduction
Pancreaticoduodenectomy (PD) is the standard
treatment method for malignant hepatobiliary pancreatic tumors.
However, the perioperative mortality rate of PD has remained at 5%
over the last few decades, despite improved techniques and advances
in surgical assist devices (1,2). In
addition, perioperative morbidity rates have been reported to range
from 30 to 60% (3,4). Among the potential complications of PD,
the most common are surgical site infections (SSIs), delayed
gastric emptying and postoperative pancreatic fistula (POPF).
Especially, POPF is an independent risk factor for SSIs such as
intra-abdominal abscesses (5). SSIs
are well-known factors, which lead to increased medical costs and
prolonged hospital stays. Therfore, in order to reduce those
medical costs and hospital stays, necessitating prompt
identification and prevention of SSIs are clinically very
important. More recently, the geriatric nutritional risk index
(GNRI) has gained favor in assessing a patient's nutritional status
and in predicting the clinical outcomes of elderly patients,
particularly those with chronic kidney disease and heart failure
(6–8). More importantly, GNRI is easily and
inexpensively attainable, as it only requires body weight, height
and serum albumin levels. Due to the intimate relationship between
preoperative nutritional status and SSI, the authors hypothesized
that GNRI could be utilized as a novel tool to predict the SSI in
patients who would undergo PD. Thus, a retrospective study was
performed to assess this association between GNRI and SSI. The aim
of the present study was to evaluate the GNRI and SSI in patents
who underwent PD. The identification of predictive markers for SSI
may help identify patients who are at a high risk of developing
them in the future.
Patients and methods
Patients
A total of 106 patients who underwent PD for
malignant hepatobiliary pancreatic tumors between January 2008 and
December 2017 were retrospectively analyzed at Kawaguchi Municipal
Medical Center for SSI. This protocol was reviewed and approved at
the Kawaguchi Municipal Medical Center in 2016. All participants
including retrospectively registered patients or their guardians
verbally consented to the use of their medical information for
scientific research (no. KMMC2017-27).
Clinicopathological data
Medical records were analyzed to determine SSI rates
and evaluate the role of other potential risk factors for SSI.
Demographic variables (sex and age), anthropometric parameters
[height, weight, and body mass index (BMI)], comorbidities, history
of smoking and alcohol use, American society of anesthesiologist
(ASA)'s physical status classification, estimated blood loss,
operation time, and laboratory data (albumin) were collected from
individual medical records.
Nutritional assessment using GNRI
Nutritional status was determined according to GNRI
[GNRI=(14.89×serum albumin (g/l)) + (41.7×present/ideal body weight
(kg))]. Ideal body weight was defined using patient height and a
BMI of 22. When present body weight was higher than the ideal body
weight, present/ideal body weight ratio was set to 1.
Analytic method
All statistical analyses were performed using
Graphpad Prism v5.0 (Graphpad Software Inc., La Jolla, CA, USA) and
StatView (Abacus Concepts, Inc., Berkeley, CA, USA). Differences
between the SSI and non-SSI groups were compared using the Fisher's
exact test or Chi-squared test. The optimal cut-off value of GNRI
was determined using a receiver operating characteristic (ROC)
curve. Potential risk factors for SSI were evaluated using
univariate and multivariate analyses. The Chi-squared test or
Fisher's exact test as univariate analyses was performed for the
SSI group. Independent risk factors for SSI were identified by
univariate analysis using a logistic regression. The probability of
P<0.05 was considered statistically significant.
Results
Patient characteristics
The male-to-female ratio was 1:1 (53/53). The mean
age was 70.2±8.7 years. Among them, 15 patients had wound infection
complications (15.4%) and 17 (16.0%) developed POPFs.
Univariate analysis for SSI risk
following PD
Patients were divided into two groups according to
the presence or absence of SSI. Clinical and demographic data from
each group are summarized in Table
I. No statistically significant difference in sex, age, smoking
habit, ASA classification, BMI, alcohol abuse, preoperative biliary
drainage, estimated blood loss, operation time, blood transfusions,
and postoperative hospital stays were observed between SSI and
non-SSI groups. However, BMI was higher in the SSI group than in
the non-SSI group (24± 4.4 vs. 21.8 ±3.0, P=0.05). Statistically
significant differences were observed for preoperative albumin (P
< 0.001), GNRI values (P < 0.001), postoperative hospital
stays (P < 0.001), and pancreatic fistulization (P < 0.001).
POPF occurred in 17 patients (16.0%), 6 of whom (40.0%) developed
SSIs. Moreover, majority of SSIs were caused at the surface (n=12)
in Table II.
 | Table I.Background of patients with or without
SSI. |
Table I.
Background of patients with or without
SSI.
| Characteristics | SSI group (n=15) | Non-SSI group
(n=91) | P-value |
|---|
| Sex |
|
|
|
|
Male/female | 6/9 | 47/44 | 0.58 |
| Age
(years) | 70.9±8.5 | 70.1±8.7 | 0.72 |
| Smoking |
|
|
|
| Yes
(%) | 2 (13.3) | 15 (16.5) | 0.76 |
| ASA
classification |
|
|
|
| 1 | 0 (0.0) | 3 (3.3) | 0.48 |
| 2 or
3 | 15 (100.0) | 88 (96.7) |
|
| Body mass
index | 24.0±4.4 | 21.8±3.0 | 0.05 |
| Alcohol abuse |
|
|
|
| Yes
(%) | 3 (20.0) | 36 (39.6) | 0.25 |
| Diabetes
mellitus |
|
|
|
| Yes
(%) | 4 (26.7) | 35 (38.5) | 0.56 |
| Preoperative biliary
drainage |
|
|
|
| Yes
(%) | 13 (86.7) | 66 (72.5) | 0.34 |
| Preoperative albumin
(g/l) | 3.2±0.5 | 4.0±0.4 | <0.001 |
| Geriatric nutritional
risk index | 87.9±7.5 | 100.0±7.6 | <0.001 |
|
<94 | 12 (80.0) | 15 (16.5) | <0.001 |
| ≥94 | 3 (20.0) | 76 (83.5) |
|
| Time of operation
(min) | 458.0±83.8 | 476.2±104.5 | 0.52 |
| Estimated blood loss
(ml) | 1,461.5±1,002.1 | 1,447.4±1,432.1 | 0.97 |
| Blood
transfusion |
|
|
|
| Yes
(%) | 11 (73.3) | 64 (70.3) | 0.81 |
| Postoperative
pancreatic fistula |
|
|
|
| Yes
(%) | 8 (53.3) | 9 (9.9) | <0.001 |
| Postoperative
hospital stays (day) | 58.5±15.0 | 27.2±2.0 | <0.001 |
| Table II.Type of SSI and disease. |
Table II.
Type of SSI and disease.
| Type of SSI
(n=15) | Type of disease
(n=15) |
|---|
| Surface: 12
(overlapped data) | Pancreatic head
cancer 20.0% (n=3) |
| Deep: 5 (overlapped
data) | Bile duct cancer
40.0% (n=6) |
| Organ/space: 5
(overlapped data) | Cancer of the ampulla
of vater 40.0% (n=6) |
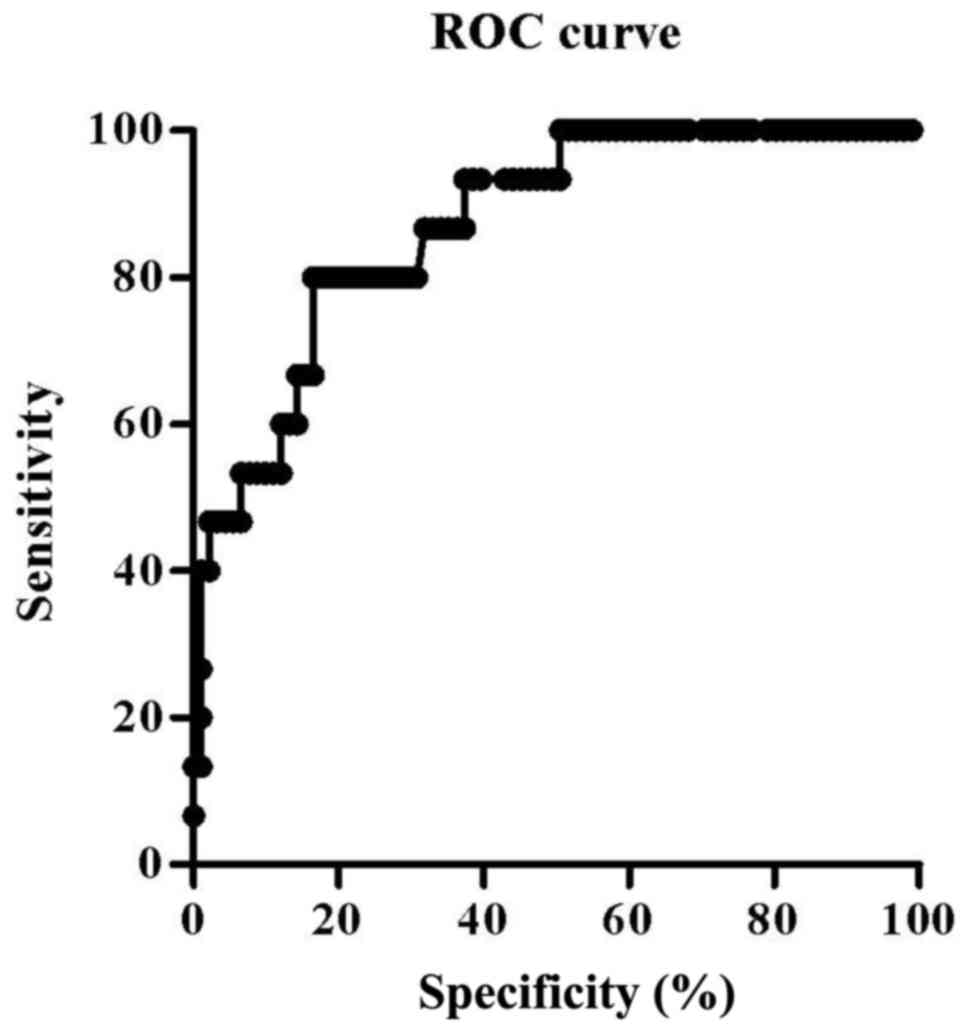
Determination of the optimal GNRI
cut-off value
The cut-off value was identified using ROC curve
analysis (Fig. 1). Area under the
curve was 0.87. A GNRI value of 94 was determined as the most
appropriate cut-off value, rendering a sensitivity of 80.0% and a
specificity of 83.5%. Patients were then divided into two groups:
Group A (GNRI ≥94, n=79) and group B (GNRI <94, n=27) using the
established GNRI cut-off value of 94. The observed SSI rate was
3.8% in group A and 44.4% in group B.
Univariate analysis of a GNRI <94
for SSI risk following PD
Univariate analysis was performed to identify
factors predicting SSI risk after PD. The incidence of SSI was
significantly higher in group B than in group A (P<0.001).
Multivariable with logistic regression
analyses
Logistic regression analysis revealed that a GNRI
value <94 (P<0.001) and POPF occurrence (P<0.006) were
independent predictors for SSI as outlined in Table III.
| Table III.Multivariate analysis by logistical
regression. |
Table III.
Multivariate analysis by logistical
regression.
| Characteristics | Odds ratio | 95% confidence
interval | P-value |
|---|
| Body mass index | 0.85 | 0.72-1.00 | 0.05 |
| Preoperative albumin
(g/l) | 0.36 | 0.12-1.10 | 0.07 |
| Geriatric nutritional
risk index <94 | 0.05 | 0.01-0.20 | <0.001 |
| Postoperative
pancreatic fistula | 9.39 | 1.91-46.12 | <0.006 |
Discussion
SSIs remain one of the most common postoperative
complications (9), with an estimated
incidence of 10-33% of patients after PD (10–12). In
general, risk factors for postsurgical wound complications
following abdominal procedures include the ASA score, obesity,
diabetes, age, operation time, estimated blood loss, and poor
nutrition (13,14). Among them, malnutrition is by far the
most common risk factor for developing SSIs (15,16), and
Bozzetti et al found that hypoalbuminemia was an independent
predictor (17). As SSIs are
associated with prolonged hospital stay, ultimately leading to
higher medical costs, surgeons should promptly identify at-risk
patients prior to elective procedures. In this regard, several
nutritional assessment tools have been developed and validated: The
nutrition risk index (NRI), malnutrition inflammation score,
malnutrition universal screening tool, prognostic nutritional index
(PNI), and GNRI (18–21). Among them, recent reports revealed
that GNRI has been identified as a prognostic indicator in patients
with heart failure and chronic renal disease (6–8). GNRI
was originally developed to evaluate malnutrition and related
morbidity and mortality in elderly patients (22). Therefore, we aimed to determine
whether GNRI can predict the incidence of SSI following PD. Several
studies have reported the use of nutritional assessment tools in
predicting the incidence of postoperative complications, such as
SSI. Hu et al reported that preoperative PNI is a useful
predictor of SSI in gastrointestinal surgery (23). Additionally, Yamana et al
showed that GNRI is useful in predicting the development of
respiratory complications in patients with esophageal malignancies
(24). In contrast, Shinkawa et
al found that NRI is an independent predictive factor for the
risk of SSI after PD (12).
Likewise, Kitagawa et al reported that GNRI could be used to
evaluate postoperative nutritional status after PD (25).
In the present study, 15.4% of the patients
developed SSI following PD in our center. Among them, a low GNRI
value (<94) was strongly associated with a higher risk of SSI,
supporting the use of nutritional assessment prior to an elective
procedure. In addition, the development of POPFs is also a
potential predictor of SSI, although they are intimately related to
SSI, particularly space/organ infections. Parikh et al
reported that 55% of POPFs contributed to the occurrence of
intra-abdominal abscess (26). In
our data, SSIs were observed in 40% of patients with POPFs.
Therefore, low GNRI might be a possible marker of POPF and SSI.
Although our data are consistent with previously
published NRI data (12), we are the
first to demonstrate the relationship between GNRI and SSI.
However, our study has several limitations. The most important
limitation is the lack of statistical power due to small sample
size. The second is that our data were collected at a single
center. Therefore, a more comprehensive prospective study should be
conducted in the future to validate the present findings.
In conclusion, the results of the present study
suggest that a GNRI score of <94 is a probable candidate for
predicting SSI in patients who undergo PD.
Acknowledgements
The authors would like to thank Dr Curtis Lacy
(Department of Internal Medicine, Mayo Clinic, USA) for his advice
and assistance.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
NF performed the experimental studies and wrote the
manuscript. NF and YN participated in the design of the study. NF,
YN, TI and KK performed the surgeries. YN and TI collected the
patient data. NF conceived the study and performed the statistical
analysis. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Fernández-del Castillo C, Morales-Oyarvide
V, McGrath D, Wargo JA, Ferrone CR, Thayer SP, Lillemoe KD and
Warshaw AL: Evolution of the whipple procedure at the Massachusetts
general hospital. Surgery. 152 3 Suppl 1:S56–S63. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kimura W, Miyata H, Gotoh M, Hirai I,
Kenjo A, Kitagawa Y, Shimada M, Baba H, Tomita N, Nakagoe T, et al:
A pancreaticoduodenectomy risk model derived from 8575 cases from a
national single-race population (Japanese) using a web-based data
entry system: The 30-day and in-hospital mortality rates for
pancreaticoduodenectomy. Ann Surg. 259:773–780. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ahmad SA, Edwards MJ, Sutton JM, Grewal
SS, Hanseman DJ, Maithel SK, Patel SH, Bentram DJ, Weber SM, Cho
CS, et al: Factors influencing readmission after
pancreaticoduodenectomy: A multi-institutional study of 1302
patients. Ann Surg. 256:529–537. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hill JS, Zhou Z, Simons JP, Ng SC, McDade
TP, Whalen GF and Tseng JF: A simple risk score to predict
in-hospital mortality after pancreatic resection for cancer. Ann
Surg Oncol. 17:1802–1807. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
DeOliveira ML, Winter JM, Schafer M,
Cunningham SC, Cameron JL, Yeo CJ and Clavien PA: Assessment of
complications after pancreatic surgery: A novel grading system
applied to 633 patients undergoing pancreaticoduodenectomy. Ann
Surg. 244:931–939. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Matsumura T, Mitani Y, Oki Y, Fujimoto Y,
Ohira M, Kaneko H, Kawashima T, Nishio M and Ishikawa A: Comparison
of geriatric nutritional risk index scores on physical performance
among elderly patients with chronic obstructive pulmonary disease.
Heart Lung. 44:534–538. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Komatsu M, Okazaki M, Tsuchiya K,
Kawaguchi H and Nitta K: Geriatric nutritional risk index is a
simple predictor of mortality in chronic hemodialysis patients.
Blood Purif. 39:281–287. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kaneko H, Suzuki S, Goto M, Yuzawa Y,
Arita T, Yagi N, Murata N, Kato Y, Kano H, Matsuno S, et al:
Geriatric nutritional risk index in hospitalized heart failure
patients. Int J Cardiol. 181:213–215. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Walz JM, Paterson CA, Seligowski JM and
Heard SO: Surgical site infection following bowel surgery: A
retrospective analysis of 1446 patients. Arch Surg. 141:1014–1018.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pisters PW, Hudec WA, Hess KR, Lee JE,
Vauthey JN, Lahoti S, Raijman I and Evans DB: Effect of
preoperative biliary decompression on
pancreaticoduodenectomy-associated morbidity in 300 consecutive
patients. Ann Surg. 234:47–55. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Poruk KE, Lin JA, Cooper MA, He J, Makary
MA, Hirose K, Cameron JL, Pawlik TM, Wolfgang CL, Eckhauser F and
Weiss MJ: A novel, validated risk score to predict surgical site
infection after pancreaticoduodenectomy. HPB (Oxford). 18:893–899.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Shinkawa H, Takemura S, Uenishi T, Sakae
M, Ohata K, Urata Y, Kaneda K, Nozawa A and Kubo S: Nutritional
risk index as an independent predictive factor for the development
of surgical site infection after pancreaticoduodenectomy. Surg
Today. 43:276–283. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Watanabe M, Miyata H, Gotoh M, Baba H,
Kimura W, Tomita N, Nakagoe T, Shimada M, Kitagawa Y, Sugihara K
and Mori M: Total gastrectomy risk model: Data from 20,011 Japanese
patients in a nationwide internet-based database. Ann Surg.
260:1034–1039. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Takagi K, Yoshida R, Yagi T, Umeda Y,
Nobuoka D, Kuise T and Fujiwara T: Radiographic sarcopenia predicts
postoperative infectious complications in patients undergoing
pancreaticoduodenectomy. BMC Surg. 17:642017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kuzu MA, Terzioğlu H, Genç V, Erkek AB,
Ozban M, Sonyürek P, Elhan AH and Torun N: Preoperative nutritional
risk assessment in predicting postoperative outcome in patients
undergoing major surgery. World J Surg. 30:378–390. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Norman K, Pichard C, Lochs H and Pirlich
M: Prognostic impact of disease-related malnutrition. Clin Nutr.
27:5–15. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bozzetti F, Gianotti L, Braga M, Di Carlo
V and Mariani L: Postoperative complications in gastrointestinal
cancer patients: The joint role of the nutritional status and the
nutritional support. Clin Nutr. 26:698–709. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Putwatana P, Reodecha P, Sirapo-ngam Y,
Lertsithichai P and Sumboonnanonda K: Nutrition screening tools and
the prediction of postoperative infectious and wound complications:
Comparison of methods in presence of risk adjustment. Nutrition.
21:691–697. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sharma Y, Thompson C, Kaambwa B, Shahi R
and Miller M: Validity of the malnutrition universal screening tool
(MUST) in Australian hospitalized acutely unwell elderly patients.
Asia Pac J Clin Nutr. 26:994–1000. 2017.PubMed/NCBI
|
|
20
|
Kalantar-Zadeh K, Kopple JD, Block G and
Humphreys MH: A malnutrition-inflammation score is correlated with
morbidity and mortality in maintenance hemodialysis patients. Am J
Kidney Dis. 38:1251–1263. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Maeda K, Nagahara H, Shibutani M, Otani H,
Sakurai K, Toyokawa T, Tanaka H, Kubo N, Muguruma K, Kamata N, et
al: A preoperative low nutritional prognostic index correlates with
the incidence of incisional surgical site infections after bowel
resection in patients with Crohn's disease. Surg Today.
45:1366–1372. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Bouillanne O, Morineau G, Dupont C,
Coulombel I, Vincent JP, Nicolis I, Benazeth S, Cynober L and
Aussel C: Geriatric nutritional risk index: A new index for
evaluating at-risk elderly medical patients. Am J Clin Nutr.
82:777–783. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hu Q, Wang G, Ren J, Ren H, Li G, Wu X, Gu
G, Li R, Guo K, Deng Y, et al: Preoperative prognostic nutritional
index predicts postoperative surgical site infections in
gastrointestinal fistula patients undergoing bowel resections.
Medicine (Baltimore). 95:e40842016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yamana I, Takeno S, Shibata R, Shiwaku H,
Maki K, Hashimoto T, Shiraishi T, Iwasaki A and Yamashita Y: Is the
geriatric nutritional risk index a significant predictor of
postoperative complications in patients with esophageal cancer
undergoing esophagectomy? Eur Surg Res. 55:35–42. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kitagawa Y, Kawabata Y, Fujishiro K and
Fukata S: Postoperative nutritional evaluation using geriatric
nutritional risk index (GNRI) for aged patients with
pancreatocoduodenectomy. J Geriatr Oncol. 5 Suppl 1:S12–S13. 2014.
View Article : Google Scholar
|
|
26
|
Parikh JA, Beane JD, Kilbane EM, Milgrom
DP and Pitt HA: Is American college of surgeons NSQIP organ space
infection a surrogate for pancreatic fistula? J Am Coll Surg.
219:1111–1116. 2014. View Article : Google Scholar : PubMed/NCBI
|