Introduction
Gastric cancer is the fourth most common malignant
tumor worldwide (1) and the second
most common malignant tumor in China (2). Although the overall incidence of
gastric cancer has been decreasing over the last two decades
(3), the 5-year mortality rate for
advanced gastric cancer remains 30–50% (4).
A proportion of advanced gastric cancer patients are
diagnosed with Krukenberg tumors. Krukenberg tumors are metastatic
ovarian tumors arising from a specific type of gastric cancer
(signet-ring cell carcinoma). The median overall survival of
advanced gastric cancer has been reported to be 13–19.2 months
(5–9). These patients may not be considered
eligible for surgical resection, and are instead treated with
chemotherapy or local radiotherapy. After every 2–4 cycles of
chemotherapy, tumor re-evaluation is performed. At baseline at the
time of diagnosis and during follow-up, tumor lesions (such as
liver and lung metastatic nodules) and positive lymph nodes (≥15 mm
in the short axis) may be selected as target lesions. Under certain
conditions, if only metastatic cystic lesions are present in the
patient, these measurable cystic masses may be considered as target
lesions (10).
We herein report a case of gastric cancer
complicated by a Krukenberg tumor. The question of whether the
Krukenberg tumor could be considered as the target lesion in the
therapeutic assessment of gastric cancer was addressed. Although
the measurable cystic lesion decreased by >30% in greatest
diameter after a course of chemotherapy, the increasing levels of
tumor markers and a new lesion detected on positron emission
tomography-computed tomography (PET/CT) indicated progressive
disease.
Case report
A 30-year-old woman without a relevant medical or
significant family history visited a local hospital in May 2017 due
to abdominal distention, nausea and melena; the symptoms reportedly
increased after eating. The patient underwent gastroscopy, which
revealed a thickened gastric wall (linitis plastica), with several
hard and bleeding ulcers. The patient was histologically diagnosed
with adenocarcinoma of the gastric fundus. Human epidermal growth
factor receptor 2 immunostaining was performed and scored as 3+.
Abdominal CT and ultrasonography were performed and revealed
massive ascites and thickening of the peritoneum. The patient
underwent diagnostic abdominocentesis, and routine ascites cytology
analysis indicated malignancy. During June 2018, the patient was
transferred to the Cancer Center, Union Hospital, Tongji Medical
College, Huazhong University of Science and Technology (Wuhan,
China) for more thorough examination. The pathological consultation
reported a poorly differentiated adenocarcinoma of the gastric
fundus, which was proven to be signet-ring cell carcinoma.
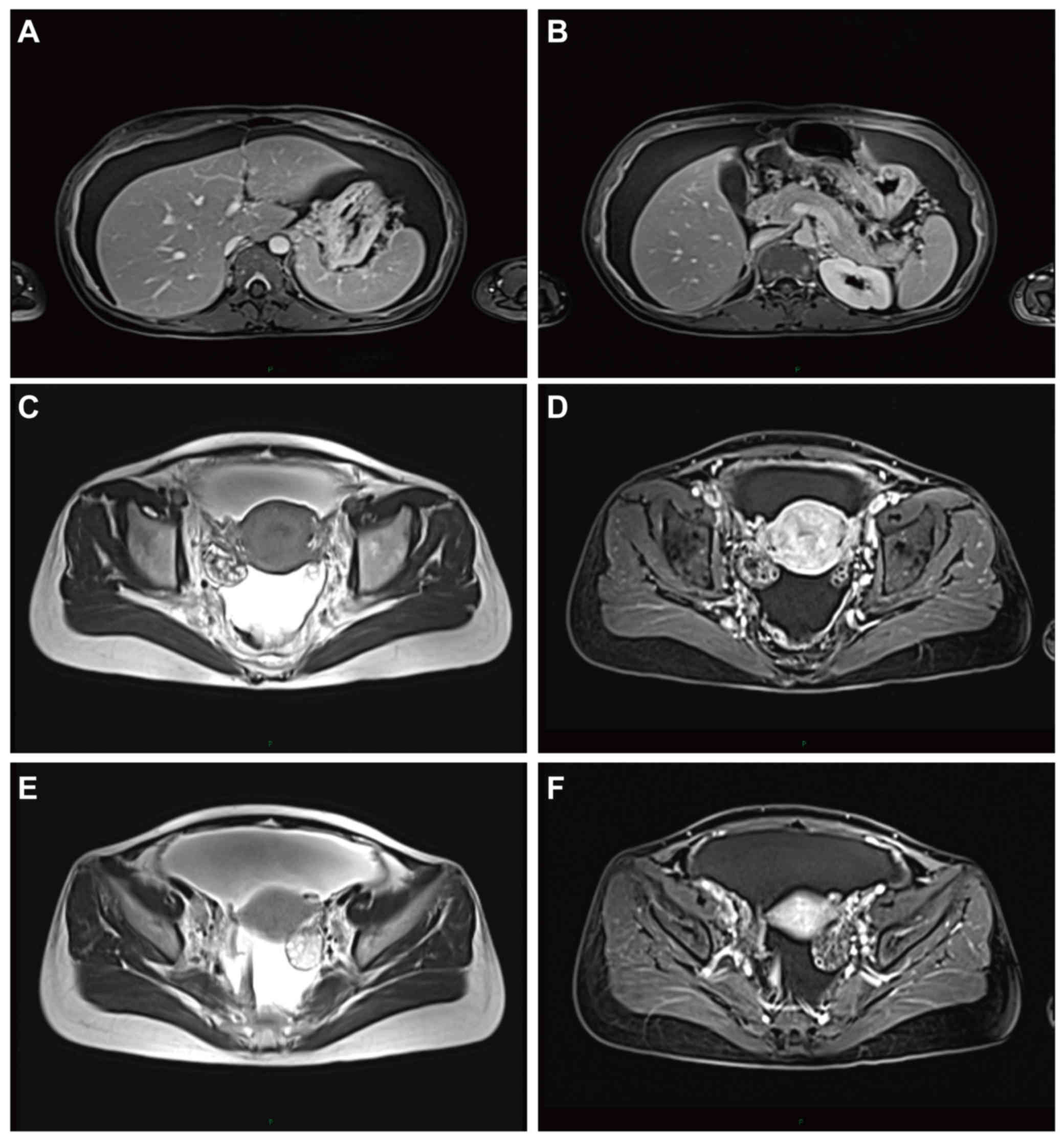
Abdominal and pelvic contrast-enhanced magnetic resonance imaging
(MRI) revealed gastric adenocarcinoma with mesenteric, greater
omental, peritoneal and pelvic metastases, and a cystic mass
(3.2×2.2 cm) to the right of the uterus, which was considered to be
a Krukenberg tumor (Fig. 1). A bone
scan revealed enhancement in the ribs, thoracic vertebrae, lumbar
vertebrae and left and right iliac crests. As regards tumor
markers, the carcinoembryonic antigen (CEA; 67.27 µg/ml; normal
value: <5 µg/ml), cancer antigen (CA)19-9 (3,073.9 U/ml; normal
value: <37 U/ml) and CA125 (301.6 U/ml; normal value: <35
U/ml) levels were raised, while the α-fetoprotein (AFP; 3.8 µg/l;
normal value: 0.89–8.78 µg/l) and CA15-3 (16.8 U/ml; normal value:
<31.3 U/ml) levels were normal. According the TNM Classification
of Malignant Tumors classification (11), the final diagnosis was poorly
differentiated gastric adenocarcinoma, stage IV.
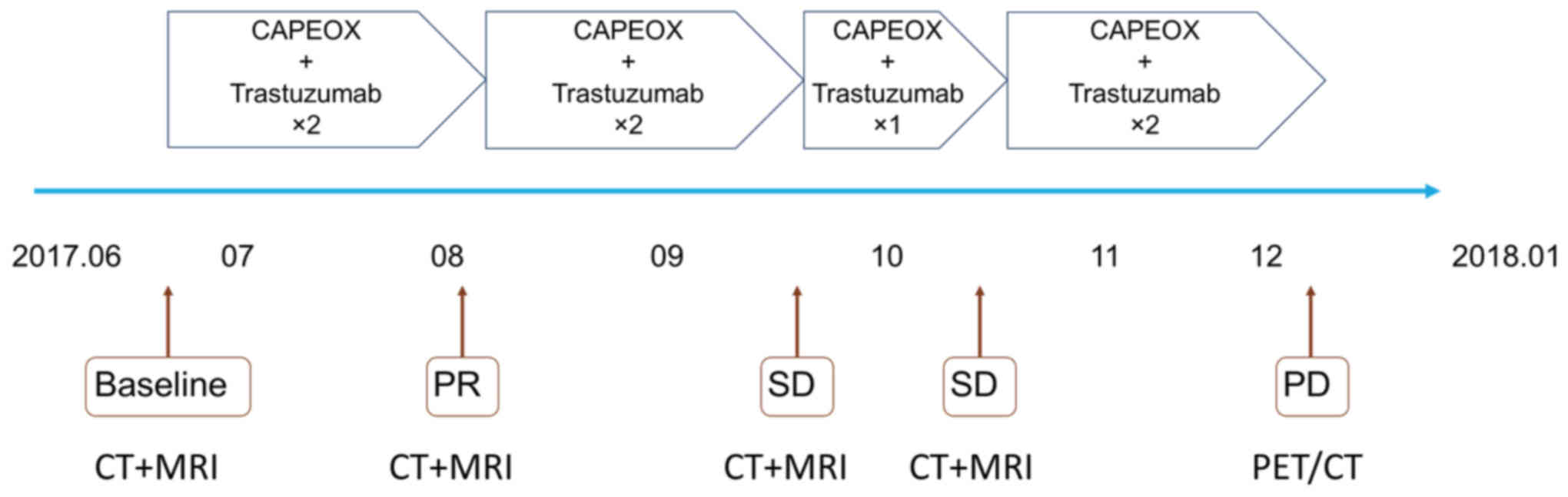
Due to the multiple metastases, the patient was not
considered to be an eligible candidate for surgery. In total, she
received seven courses of oxaliplatin/capecitabine [oxaliplatin,
130 mg/m2 (day 1); capecitabine, 1,000 mg/m2
(days 1–14)] plus trastuzumab (OCT) chemotherapy [oxaliplatin 130
mg/m2 (day 1); capecitabine 1,000 mg/m2 (days
1–14); and trastuzumab 8 mg/m2 (day 0 prior to treatment
initiation, first course of 21 days) and 6 mg/m2 (day 0, 2–7
courses, 21 days/course)]. After two courses, the therapeutic
assessment was stable disease (Fig.
2). The patient's serum CEA, CA19-9 and CA125 levels had
decreased to 3.00 µg/ml, 61.1 U/ml and 17.9 U/ml, respectively,
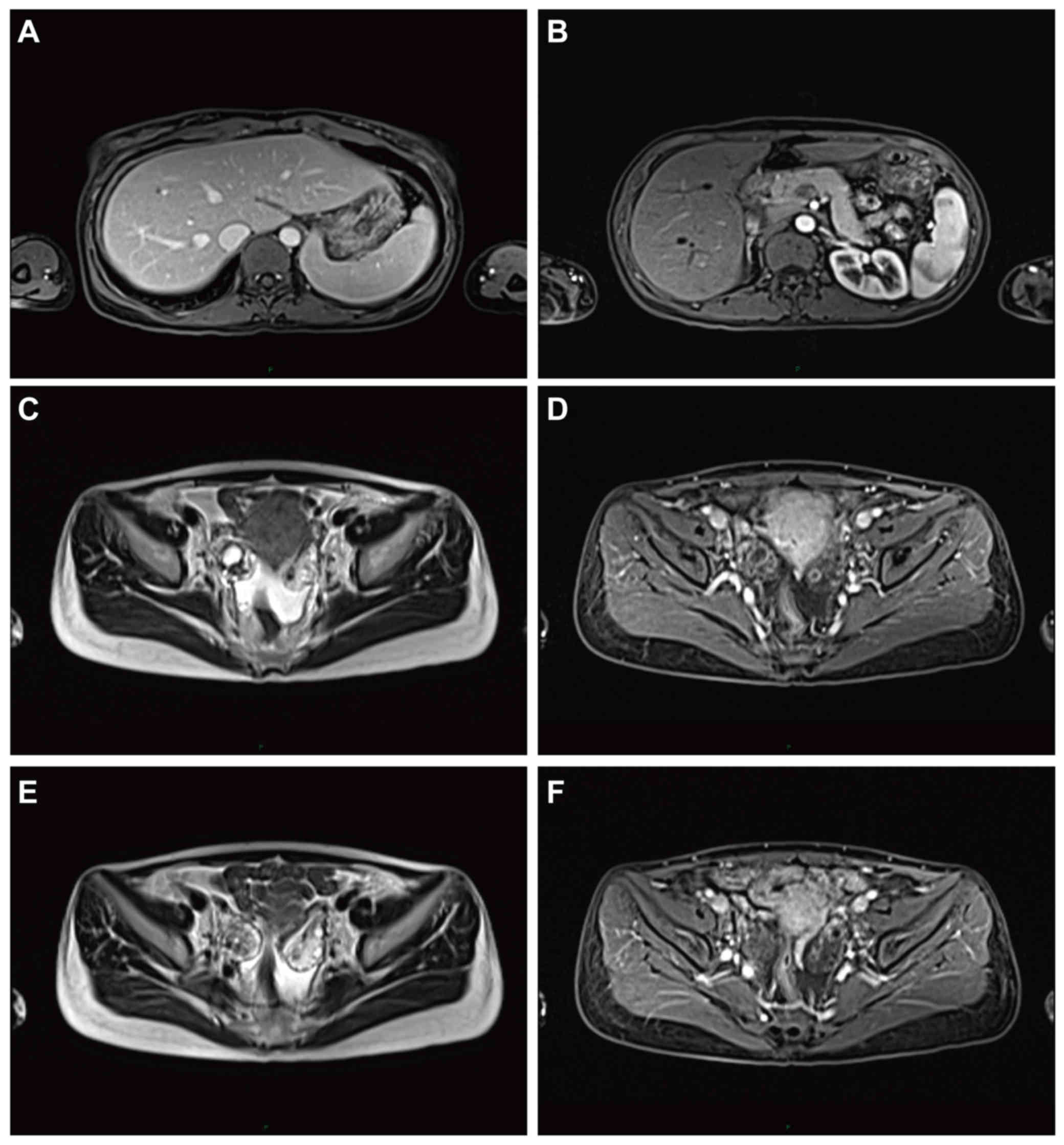
after three courses of chemotherapy. However, after four courses of
OCT, the CEA, CA19-9 and CA125 levels mildly increased. Abdominal
and pelvic contrast-enhanced MRI revealed that the size of the
right adnexal cystic mass had increased to 4.6×3.9 cm, a 43.13%
increase compared with the baseline at diagnosis (Fig. 3A and B). Considering that the patient
experienced monthly menstrual cycles, although the diameter of the
Krukenberg tumor was increased, the treatment efficacy was
difficult to assess. Therefore, OCT treatment was continued.
Abdominal and pelvic contrast-enhanced MRI examination revealed
that the cystic mass (1.4cx2.9 cm) had decreased in size by 36.96%
compared with after the last course (Fig. 3C and D). However, the serum CEA,
CA19-9 and CA125 levels had markedly increased to 14.80 µg/ml,
1,179.4 U/ml and 38.7 U/ml, respectively. At this point, the
patient's Eastern Cooperative Oncology Group performance status
score was 0, and there was no evidence supporting a change in the
treatment regimen. As the cystic mass had decreased in size, the
patient was administered two more courses of OCT chemotherapy.
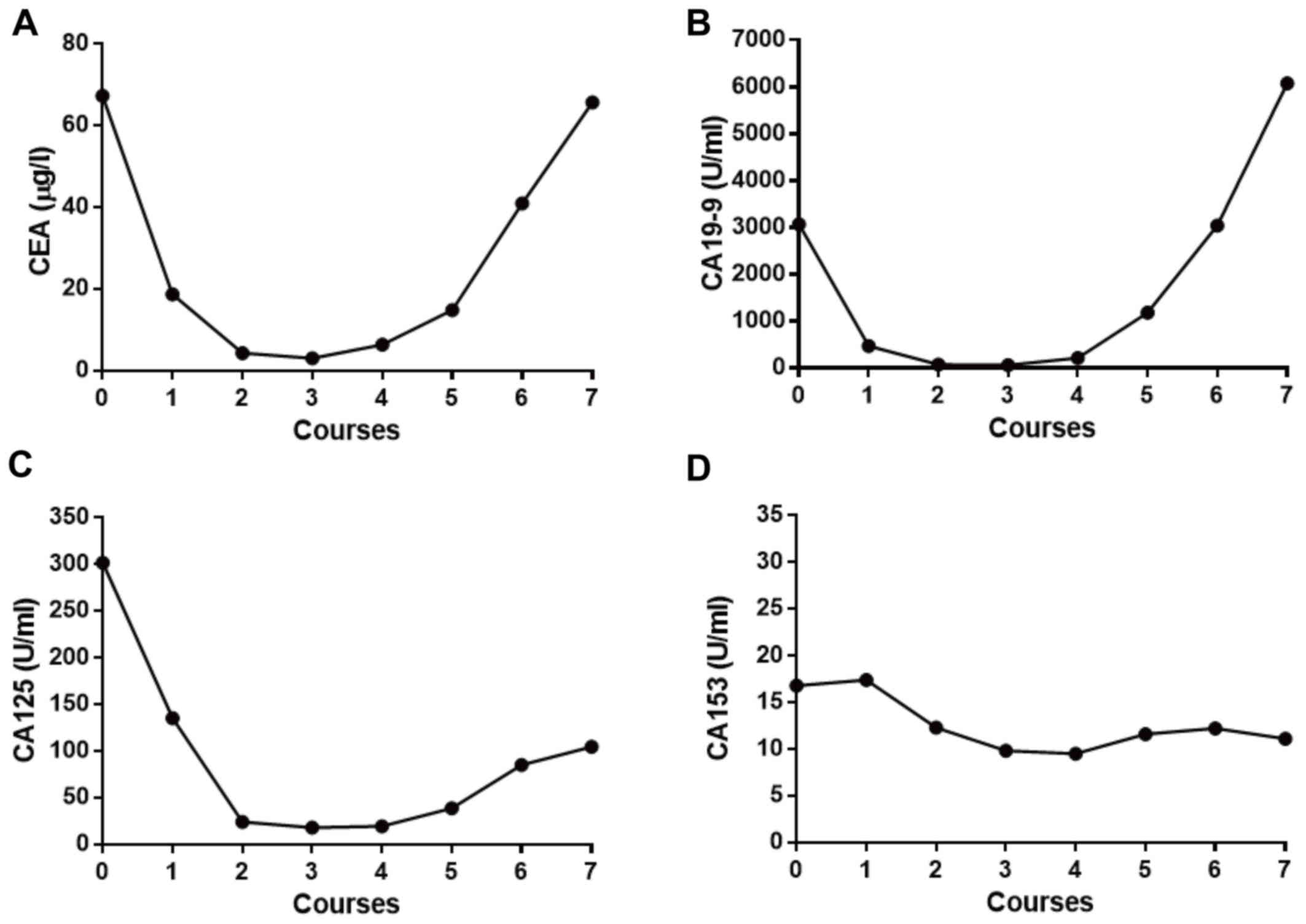
Unexpectedly, the serum CEA, CA19-9 and CA125 levels increased
rapidly to 65.7 µg/ml, 6,081.4 U/ml and 104.7 U/ml, respectively,
after the seventh cycle (Fig. 4). At
this point, the patient remained in good condition, without
abdominal or pelvic pain, bloating or abdominal distension, but
reported changes in the menstrual cycle and vaginal bleeding.
Moreover, the β-human chorionic gonadotropin level was 7.3 mIU/ml
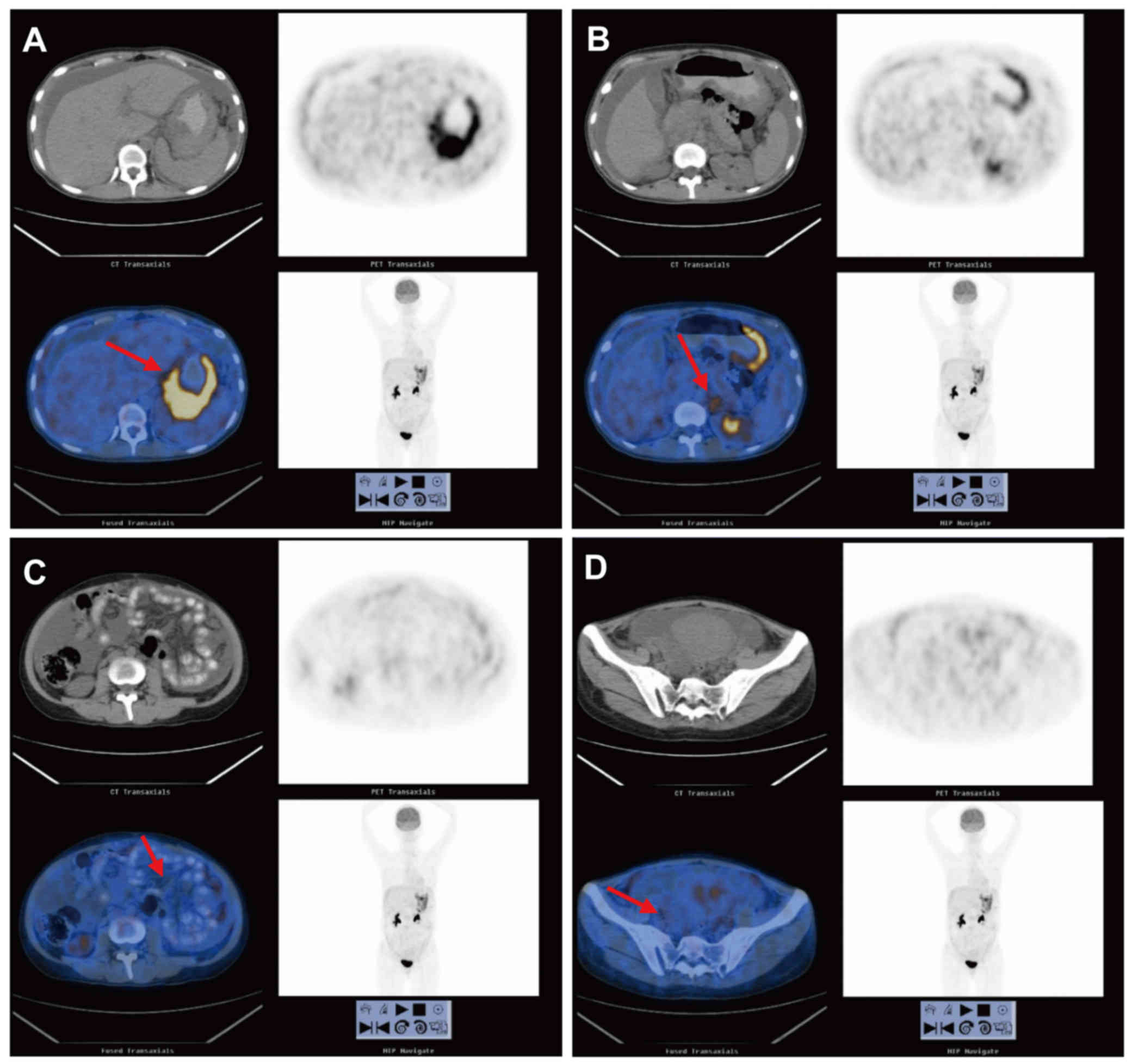
(normal value: <5 mIU/ml). Whole-body PET/CT was then performed,
revealing increased 18F-fluorodeoxyglucose (FDG) uptake
in the gastric fundus and body, left adrenal gland, mesentery and
right pelvic cystic mass, with maximum standardized uptake values
of 4.3–13.0, 4.5, 2.1–2.6 and 1.6–2.7, respectively (Fig. 5). As a new lesion was found in the
left adrenal gland, the final response evaluation of the patient
was progressive disease and docetaxel monotherapy (60
mg/m2 on day 1 every three weeks) was initiated as
second-line treatment (Fig. 6).
Discussion
Krukenberg tumors are defined as ovarian metastatic
tumors, two-thirds of which originate from the stomach (12). On imaging, these tumors may appear as
well-demarcated intramural cysts (12,13). MRI
shows a hypointense signal density of the solid components on
T2-weighted images (14–16). According to RECIST 1.0 (17), cystic lesions are considered to be
non-target lesions. In the present study, based on the persistence
of the non-target lesions (including Krukenberg tumors) and the
levels of the tumor markers being persistently raised over the
normal limits, the therapeutic assessment of the patient after four
and five cycles of treatment was incomplete response/stable
disease. However, according to RECIST 1.1 (10), if only cystic measurable lesions are
present in the same patient, they may be considered as target
lesions. Therefore, after four courses of OCT, the patient should
have been considered to have progressive disease, whereas the
therapeutic assessment was partial response after five courses of
OCT treatment, although the levels of the tumor markers had
markedly increased. These assessments were contradictory. If
treatment had failed, partial response would not have been achieved
after another cycle of OCT treatment. After seven courses of OCT,
PET/CT revealed progression. It was then hypothesized that the
patient may have already been progressive after four cycles of
OCT.
In the present case report, it appears more
appropriate to adopt RECIST 1.0 rather than the 1.1 version. Cystic
lesions, such as Krukenberg tumors, are preferably considered as
non-target lesions. In 2004, Husband et al (18) suggested that characterizing all
cystic lesions as targets, which may still be included in the
assessment and documentation of the changes in tumor composition,
should be avoided. Over the last two decades, there have only been
few studies on the evaluation of cystic lesions. In the present
study, we demonstrated that cystic lesions should be considered as
non-target lesions, although they may be measurable.
In patients with non-measurable as well as
non-target disease only, tumor marker levels should be considered
in the therapeutic assessment. In both versions of RECIST, tumor
markers alone cannot be used to evaluate objective tumor response.
However, specific guidelines for tumor markers, including CA-125
and prostate-specific antigen, are being validated, and CA-125 is
recommended for integration with objective assessment in ovarian
cancer (19–22). Moreover, PET/CT may be introduced for
the assessment of progression (particularly possible new lesions)
(10). In this case, PET/CT was used
to detect new lesions, as the tumor markers had increased
multifold.
In conclusion, the present case report demonstrated
that, considering measurable Krukenberg tumors or cystic lesions as
target lesions in the response assessment of advanced gastric
cancer, must be avoided. In addition, tumor markers and PET/CT may
provide complementary results to the therapeutic assessment of
advanced gastric cancer with only non-target lesions.
Acknowledgements
The authors would like to thank the members of the
Xin Li team for their critical comments and technical support.
Funding
No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
BW, CF, TZ, GW and QL contributed to the conception
and design of the study. BW, CF, JL, YL and JX contributed to data
acquisition and analysis, and drafting of the article. TZ, GW and
QL revised the manuscript. All authors have read and approved the
final version for publication.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient and her husband for publication of this case report and any
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
RECIST
|
Response Evaluation Criteria in Solid
Tumors
|
|
SD
|
stable disease
|
|
PD
|
progressive disease
|
|
CAPEOX
|
oxaliplatin/capecitabine
|
|
OCT
|
oxaliplatin/capecitabine plus
trastuzumab
|
|
CEA
|
carcinoembryonic antigen
|
|
CA19-9
|
cancer antigen 19-9
|
|
CA125
|
cancer antigen 125
|
|
CA153
|
cancer antigen 153
|
|
AFP
|
α-fetoprotein
|
|
PSA
|
prostate-specific antigen
|
|
CT
|
computed tomography
|
|
MRI
|
magnetic resonance imaging
|
|
PET/CT
|
positron emission tomography-computed
tomography
|
References
|
1
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2013. CA Cancer J Clin. 63:11–30. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ferlay J, Shin HR, Bray F, Forman D,
Mathers C and Parkin DM: Estimates of worldwide burden of cancer in
2008: GLOBOCAN 2008. Int J Cancer. 127:2893–2917. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hamashima C, Shabana M, Okada K, Okamoto M
and Osaki Y: Mortality reduction from gastric cancer by endoscopic
and radiographic screening. Cancer Sci. 106:1744–1749. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jeung YJ, Ok HJ, Kim WG, Kim SH and Lee
TH: Krukenberg tumors of gastric origin versus colorectal origin.
Obstet Gynecol Sci. 58:32–39. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jiang R, Tang J, Cheng X and Zang RY:
Surgical treatment for patients with different origins of
Krukenberg tumors: Outcomes and prognostic factors. Eur J Surg
Oncol. 35:92–97. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kim HK, Heo DS, Bang YJ and Kim NK:
Prognostic factors of Krukenberg's tumor. Gynecol Oncol.
82:105–109. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ayhan A, Guvenal T, Salman MC, Ozyuncu O,
Sakinci M and Basaran M: The role of cytoreductive surgery in
nongenital cancers metastatic to the ovaries. Gynecol Oncol.
98:235–241. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gagnon Y and Têtu B: Ovarian metastases of
breast carcinoma. A clinicopathologic study of 59 cases. Cancer.
64:892–898. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ajani JA, D'Amico TA, Almhanna K, Bentrem
DJ, Chao J, Das P, Denlinger CS, Fanta P, Farjah F, Fuchs CS, et
al: Gastric Cancer, Version 3.2016, NCCN Clinical Practice
Guidelines in Oncology. J Natl Compr Canc Netw. 14:1286–1312. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kiyokawa T, Young RH and Scully RE:
Krukenberg tumors of the ovary: A clinicopathologic analysis of 120
cases with emphasis on their variable pathologic manifestations. Am
J Surg Pathol. 30:277–299. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Agnes A, Biondi A, Ricci R, Gallotta V,
D'Ugo D and Persiani R: Krukenberg tumors: Seed, route and soil.
Surg Oncol. 26:438–445. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ha HK, Baek SY, Kim SH, Kim HH, Chung EC
and Yeon KM: Krukenberg's tumor of the ovary: MR imaging features.
AJR Am J Roentgenol. 164:1435–1439. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Cho JY, Seong CK and Kim SH: Krukenberg
tumor findings at color and power Doppler US; correlation with
findings at CT, MR imaging, and pathology. Case reports. Acta
Radiol. 39:327–329. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Koyama T, Mikami Y, Saga T, Tamai K and
Togashi K: Secondary ovarian tumors: Spectrum of CT and MR features
with pathologic correlation. Abdom Imaging. 32:784–795. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Therasse P, Arbuck SG, Eisenhauer EA,
Wanders J, Kaplan RS, Rubinstein L, Verweij J, Van Glabbeke M, van
Oosterom AT, Christian MC, et al: New guidelines to evaluate the
response to treatment in solid tumors. European Organization for
Research and Treatment of Cancer, National Cancer Institute of the
United States, National Cancer Institute of Canada. J Natl Cancer
Inst. 92:205–216. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Husband JE, Schwartz LH, Spencer J,
Ollivier L, King DM, Johnson R and Reznek R; International Cancer
Imaging Society, . Evaluation of the response to treatment of solid
tumours - a consensus statement of the International Cancer Imaging
Society. Br J Cancer. 90:2256–2260. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Vergote I, Rustin GJ, Eisenhauer EA,
Kristensen GB, Pujade-Lauraine E, Parmar MK, Friedlander M,
Jakobsen A and Vermorken JB: Re: New guidelines to evaluate the
response to treatment in solid tumors [ovarian cancer]. Gynecologic
Cancer Intergroup. J Natl Cancer Inst. 92:1534–1535. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Rustin GJ, Quinn M, Thigpen T, du Bois A,
Pujade-Lauraine E, Jakobsen A, Eisenhauer E, Sagae S, Greven K,
Vergote I, et al: Re: New guidelines to evaluate the response to
treatment in solid tumors (ovarian cancer). J Natl Cancer Inst.
96:487–488. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bubley GJ, Carducci M, Dahut W, Dawson N,
Daliani D, Eisenberger M, Figg WD, Freidlin B, Halabi S, Hudes G,
et al: Eligibility and response guidelines for phase II clinical
trials in androgen-independent prostate cancer: Recommendations
from the Prostate-Specific Antigen Working Group. J Clin Oncol.
17:3461–3467. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Scher HI, Halabi S, Tannock I, Morris M,
Sternberg CN, Carducci MA, Eisenberger MA, Higano C, Bubley GJ,
Dreicer R, et al; Prostate Cancer Clinical Trials Working Group, .
Design and end points of clinical trials for patients with
progressive prostate cancer and castrate levels of testosterone:
Recommendations of the Prostate Cancer Clinical Trials Working
Group. J Clin Oncol. 26:1148–1159. 2008. View Article : Google Scholar : PubMed/NCBI
|