Introduction
Extranodal lymphoma occurs in ~40% of all patients
with lymphoma and has been described in virtually all organs and
tissue (1). Extranodal disease is
more common with non-Hodgkin's lymphoma (NHL) (2), and diffuse large B-cell lymphoma (DLBCL)
is the most common histological NHL subtype in adults, accounting
for ~25% of all NHL cases (3). Thus,
it is known that gastrointestinal DLBCL is the most frequent form
of extranodal lymphoma (4). However,
DLBCL primarily arising in the retroperitoneal region has been
rarely reported. The largest series on retroperitoneal DLBCL was
published by Pileri et al in 2001 (5). Moreover, to the best of our knowledge,
primary retroperitoneal lymphoma without renal and ureteral
involvement affecting the genitourinary system has not been
reported until now.
Here, we report the extremely rare case of a young
female suffering with primary DLBCL located in the retroperitoneal
and gastrointestinal region simultaneously. Unusually, the first
symptom of this disease was renal colic. Written informed consent
was obtained from the patient for inclusion in the present
study.
Case report
Case presentation
A 33-year-old female presented with a 2-month
history of renal colic and abdominal pain, which became aggravated
at night. No fever was noted, but there was hematuria when the pain
occurred. The patient's weight remained unchanged. Her family
history was not contributory. Surgical history included two
Caesarean sections 13 and 9 years prior.
Physical examination revealed an ill-defined mass in
the right lower hypogastrium and tenderness in the abdomen, but
without abdominal distention. There were no enlarged or palpable
lymph nodes. The remaining systemic examination was not
significant. The peripheral blood count was unremarkable
(hemoglobin 109 g/l, red blood cell count 3.81×1012/l,
white blood cell count 3.05×109/l, and platelet count
230×109/l). The peripheral blood smear revealed no
immature cells (66.2% neutrophils, 25.6% lymphocytes, 7.2%
monocytes, 1.0% eosinophils and 0.0% basophils). Liver and renal
functional tests, bilirubin and electrolytes were normal. Serum
tumor markers were negative with the exception of CA-125 values of
63.88 U/ml (normal value, <35 U/ml). The remaining laboratory
tests were all within the normal limits.
Imaging
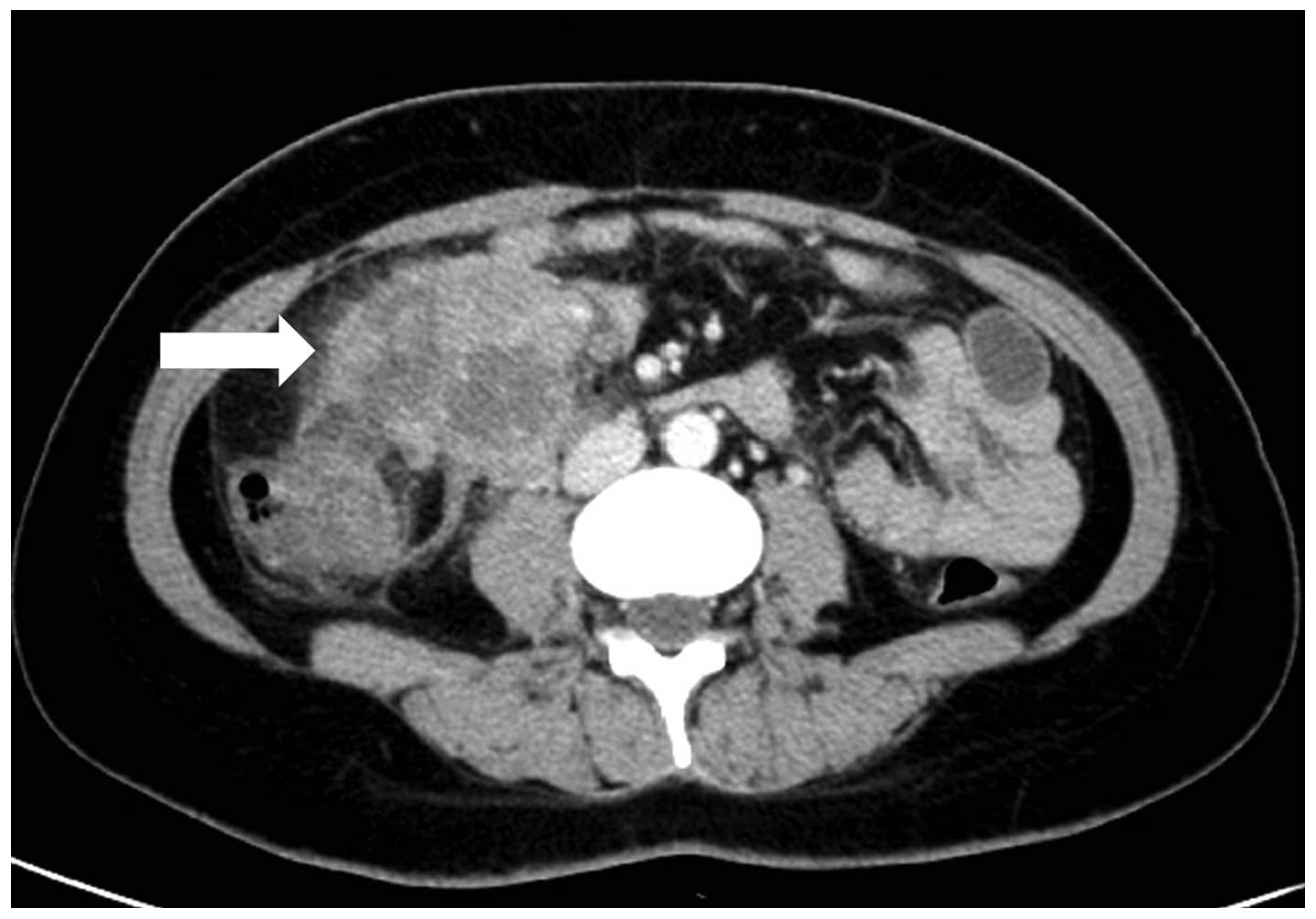
A normal chest X-ray was obtained. An abdominopelvic
contrast-enhanced computed tomography (CT) scan (Fig. 1) revealed: i) A bulky soft-tissue
dense mass in the middle of the ascending colon and superior to the
ileocecum; heterogeneous enhancement following enhanced scan;
thickened anterior of the renal fascia of the right kidney and
local parietal peritoneum. ii) Multiple renal cysts in both
kidneys. The CT scan did not indicate any bowel involvement,
distant metastasis or abdominal lymph node enlargement. The
abdominal ultrasound did not reveal any coexisting lesion in the
hepato-pancreato-biliary system. Single-photon emission computed
tomography (SPECT) renal imaging (99mTc-DTPA) revealed that the
glomerular filtration rate was slightly decreased and the upper
urinary tract had unobstructed drainage in the two kidneys.
Surgical treatment
Since the tumor had no distant involvement and there
was no evidence of worsening symptoms (renal colic and abdominal
pain), the patient underwent surgical resection. Intra-operative
findings were as follows: no ascites were in the abdominal cavity;
no dilation of the small and large bowel; the mass was
predominantly located in the right mesocolon and retroperitoneal
region, and extended to the distal ileum, ascending colon and the
beginning of the transverse colon. Intra-operative biopsy and
frozen section study indicated malignancy but did not confirm the
tumor type. Complete excision was performed, retaining the right
kidney and right ureter due to their lack of involvement.
Side-to-side anastomosis of the transverse colon and ileum was
used. The patient had an uneventful postoperative recovery. She was
discharged from the surgical ward and referred to the hematology
clinic for additional evaluation and adjuvant chemotherapy.
Pathological evaluation
The tumor consisted of two masses. The first mass
(measuring 9×8×7 cm) was located in the retroperitoneal region, and
the second (measuring 2.5×2×2 cm) was located in the mucosa of the
ileum, involving the submucosa and muscularis layers as well as the
serosa. There was no association between the two masses.
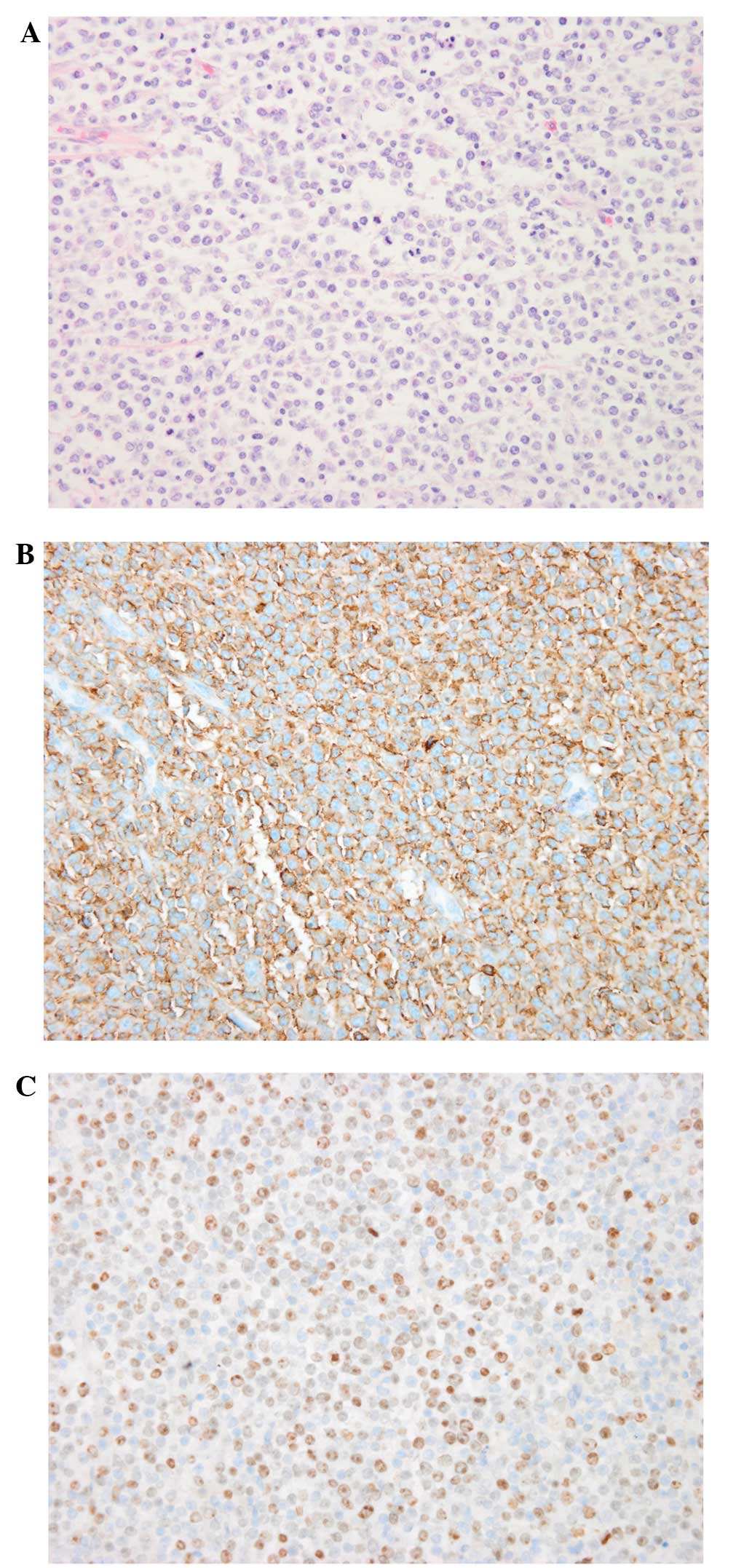
Pathological assessment was performed using
immunohistochemistry staining, which revealed positivity for CD20
and Ki67) (Fig. 2). DLBCL was the
final confirmed diagnosis.
Follow-up
The patient's general condition remained good and
she went on to receive CHOP chemotherapy. After 3 months of
follow-up, no postoperative complications were identified.
Discussion
DLBCL is the most common type of lymphoma worldwide
(6). However, NHL rarely presents
with a retroperitoneal or pelvic mass; during post-mortem studies
of NHL patients an incident of less than 1% incidence was noted
(7). Due to the uncommon anatomical
location, the diagnosis and subsequent management of these patients
tend to be difficult. The initial presentation of NHL varies
depending on the subtype and involved area, with symptoms including
enlarged palpable lymphadenopathy, B-symptoms (fever, weight loss,
night sweats), and symptoms secondary to compression of adjacent
structures. This is a unique case of retroperitoneal DLBLC, in
which the first manifestation was renal colic.
Renal colic mainly occurs in patients with renal or
ureteral calculus. Based on the findings of the abdominal CT,
abdominal X-ray and SPECT renal imaging, our patient did not suffer
with renal or ureteral calculus. Certain studies have reported that
the genitourinary system may be affected by retroperitoneal NHL.
Domazetovski et al (8)
presented a case of acute renal failure in a patient with DLBLC,
and Jaeger et al (9) reported
DLBLC in a male presenting with ureteral stricture. However, the
majority of cases have primary renal lymphoma or renal involvement.
Renal colic alone without genitourinary involvement, as observed in
our patient, is extremely rare, and could only be confirmed by
surgery in our case. When the patient initially presented at our
hospital, we considered that malignant retroperitoneal tumors
account for ~0.1% of all malignancies (10) and are more common than benign tumors
in the retroperitoneal space (11).
As the symptom of renal colic was increasing, it was speculated
that there was a high possibility of renal involvement. It is known
that the most effective treatment is surgical removal of the
tumors, with the exception of chemosensitive tumors, and that a
definitive diagnosis can usually be made from the surgical
specimens (12). Thus, considering
the patient's wishes, surgery was performed.
Unexpectedly, the tumors were located not only in
the retroperitoneal region, but also in the ileum. The latter was
relatively small, therefore no signs or symptoms had been noted.
According to our pathological evaluation, there was no association
between the two masses. Literature regarding this condition is
lacking, thus a reasonable explanation may be the variety of
extranodal lymphoma. Moreover, surgery indicated that the tumor did
not infiltrate the renal or ureteral areas. Thus, renal colic was
determined to have been the result of compression.
Although CT is the diagnostic modality of choice
(13), magnetic resonance imaging
(MRI) offers superior soft-tissue contrast in comparison with CT.
Indeed, a variety of contrast mechanisms have previously been
explored for the characterization of lymphoma in the
retroperitoneum, including T2-weighted imaging, diffusion-weighted
imaging and dynamic contrast-enhanced imaging (14). The absence of MRI is a limitation in
our diagnostic process. In the study of Tambo et al
(12), a clinicopathological review
of 46 primary retroperitoneal tumors identified that MRI imaging
diagnosis prior to surgery was compatible with the histological
diagnosis in only 26 patients (57%), and all six malignant lymphoma
patients underwent biopsy or surgical resection. Therefore, if
clinical diagnosis cannot be determined by MRI, definitive
histological diagnosis by biopsy or tumor resection is required in
order to determine the appropriate treatment.
Currently, CHOP therapy is the treatment of choice
for DLBLC patients. Since rituximab is a chimeric anti-CD20 IgG1
monoclonal antibody which is a cell surface protein that occurs
almost exclusively in mature B-cells, the combination of rituximab
and CHOP is likely become the standard for treating patients with
DLBLC (15). The prognosis has
improved in recent years owing to the development of various
aggressive chemotherapeutic regimens depending on the histological
type, stage and age of each patient. Therefore, a definitive
histological diagnosis is essential for patients with DLBLC. Our
patient did not present with any specific indications for the
diagnosis of this rare tumor as the initial manifestation was renal
colic. Surgery has a key role in establishing a definitive
diagnosis.
Primary retroperitoneal DLBLC has a variable and
non-specific presentation and may resemble other neoplastic or
inflammatory conditions. Manifestations, laboratory data and
imaging alone may initially lead to an incorrect diagnosis.
Obtaining a definitive histological diagnosis by surgery and using
appropriate chemotherapy played an essential role in the recovery
of our patient. This case study indicates the significance of
including a differential diagnosis of primary retroperitoneal NHL
in patients presenting with a retroperitoneal mass where the first
sign of this disease is renal colic.
References
|
1
|
Metser U, Goor O, Lerman H, Naparstek E
and Even-Sapir E: PET-CT of extranodal lymphoma. AJR Am J
Roentgenol. 182:1579–1586. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Vinnicombe SJ and Reznek RH: Extranodal
manifestations of lymphoma. Imaging. 11:240–268. 1999. View Article : Google Scholar
|
|
3
|
Morton LM, Wang SS, Devesa SS, Hartge P,
Weisenburger DD and Linet MS: Lymphoma incidence patterns by WHO
subtype in the United States, 1992–2001. Blood. 107:265–276. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
d'Amore F, Christensen BE, Brincker H,
Pedersen NT, Thorling K, Hastrup J, Pedersen M, Jensen MK, Johansen
P, Andersen E, et al: Danish LYFO Study Group: Clinicopathological
features and prognostic factors in extranodal non-Hodgkin
lymphomas. Eur J Cancer. 27:1201–1208. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pileri SA, Zinzani PL, Ascani S, Orcioni
GF, Gamberi B, Piccioli M, Sabattini E, Poggi S, Piccaluga PP and
Falini B: Diffuse large B-cell lymphoma with primary
retroperitoneal presentation: Clinico-pathologic study of nine
cases. Ann Oncol. 12:1445–1453. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hunt KE and Reichard KK: Diffuse large
B-cell lymphoma. Arch Pathol Lab Med. 132:118–124. 2008.PubMed/NCBI
|
|
7
|
Fulignati C, Pantaleo P, Cipriani G,
Turrini M, Nicastro R, Mazzanti R and Neri B: An uncommon clinical
presentation of retroperitoneal non-Hodgkin lymphoma successfully
treated with chemotherapy: a case report. World J Gastroenterol.
11:3151–3155. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Domazetovski I, Jovanovic R,
Kostadinova-Kunovska S, Duganovska S, Labachevski B, Nikolov I,
Ivanovski N, Sikole A and Petrushevska G: Acute renal failure in a
patient with diffuse large B-cell lymphoma: case report. Prilozi.
33:231–238. 2012.PubMed/NCBI
|
|
9
|
Jaeger CD, McAlvany KL, Zingula SN, Kramer
SA and Granberg CF: Diffuse large B-cell lymphoma in an adolescent
male presenting as ureteral stricture. Case Rep Radiol.
2014:239–345. 2014.
|
|
10
|
Heslin MJ, Lewis JJ, Nadler E, Newman E,
Woodruff JM, Casper ES, Leung D and Brennan MF: Prognostic factors
associated with long-term survival for retroperitoneal sarcoma:
Implications for management. J Clin Oncol. 15:2832–2839.
1997.PubMed/NCBI
|
|
11
|
Arlen M and Marcove RC: Retroperitoneal
sarcomasSurgical Management of Soft Tissue Sarcomas. W.B. Saunders;
Philadelphia, PA: pp. 203–232. 1987
|
|
12
|
Tambo M, Fujimoto K, Miyake M, Hoshiyama
F, Matsushita C and Hirao Y: Clinicopathological review of 46
primary retroperitoneal tumors. Int J Urol. 14:785–788. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Karaosmanoglu D, Karcaaltincaba M, Oguz B,
Akata D, Ozmen M and Akhan O: CT findings of lymphoma with
peritoneal, omental and mesenteric involvement: peritoneal
lymphomatosis. Eur J Radiol. 71:313–317. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nakayama T, Yoshimitsu K, Irie H, Aibe H,
Tajima T, Shinozaki K, Nishie A, Asayama Y, Kakihara D, Matsuura S,
et al: Usefulness of the calculated apparent diffusion coefficient
value in the differential diagnosis of retroperitoneal masses. J
Magn Reson Imaging. 20:735–742. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Feugier P, Van Hoof A, Sebban C,
Solal-Celigny P, Bouabdallah R, Fermé C, Christian B, Lepage E,
Tilly H, Morschhauser F, et al: Long-term results of the R-CHOP
study in the treatment of elderly patients with diffuse large
B-cell lymphoma: A study by the Groupe d'Etude des Lymphomes de
l'Adulte. J Clin Oncol. 23:4117–4126. 2005. View Article : Google Scholar : PubMed/NCBI
|