Introduction
Primary chondrosarcoma of the thyroid cartilage is a
rare malignancy. Chondrosarcoma of the larynx is also uncommon,
comprising only 1% of laryngeal malignancies (1), of which approximately 20% arise from the
thyroid cartilage, the second most common site after the posterior
lamina of the cricoid cartilage (2).
The pathogenesis of chondrosarcoma of the thyroid cartilage is
unknown, although a recent review suggested that several
precipitating factors, such as multiple hereditary exostoses,
Ollier's disease, chondromyxoid fibroma, and previous irradiation
may contribute to its tumorigenesis (3). However, almost all reported cases
originate from Europe or America.
An epidemiological study by Zhang et al
indicated that in 2010, 20,272 new cases of laryngeal cancer were
diagnosed in China, with a crude incidence rate of 1.54/100,000 in
2010, and 0.66% of all new cancer cases (4). The age-standardized rate in China was
shown to be 1.18/100,000, and 1.20/100,000 worldwide (4). Thus, the incidence of and mortality
associated with laryngeal cancer is still relatively low in China.
New cases of laryngeal chondrosarcoma, and clinical experience with
its management, are extremely rare in China. Fudan University
Shanghai Cancer Center is one of the largest specialized cancer
hospitals in China, and its Department of Head and Neck Surgery is
required to add any new information on the treatment and management
of this tumor into the national literature database, in order to
facilitate a more in depth discussion of these experiences at home
and abroad. In this study, we present an example of a case of
chondrosarcoma arising in the thyroid cartilage, and review the
literature on this rare neoplasm in this location in order to
provide surgeons with any new insight into its optimal
management.
Case report
A 52-year-old male was admitted to the hospital
(Fudan University Shanghai Cancer Center, Shanghai, China) in April
2015 for the evaluation of a firm non-tender left-sided neck mass
that had reportedly become enlarged over a 2-year period. He had no
history of neck pain, hoarseness, dysphagia, or dyspnea. An
examination revealed a painless, fixed, rounded cervical lesion
located in the left anterior triangle measuring 6.0×5.0 cm in
diameter, which moved on swallowing and adhered to the deep planes
but showed no evidence of adenopathy. Ultrasonography revealed a
large mass that extended to the left thyroid lobe; it was
homogeneous, hypervascularized and solid. Both biological thyroid
function tests and serum tumor markers were normal. Upon
fibrolaryngoscopy, the mucosa of the right piriform sinus remained
intact, but underwent slight medial displacement. No evidence of
endolaryngeal involvement or neoplasm from other structural
elements of the larynx (e.g., cricoid cartilage, arytenoid
cartilage) or the fixation of the vocal cords was observed.
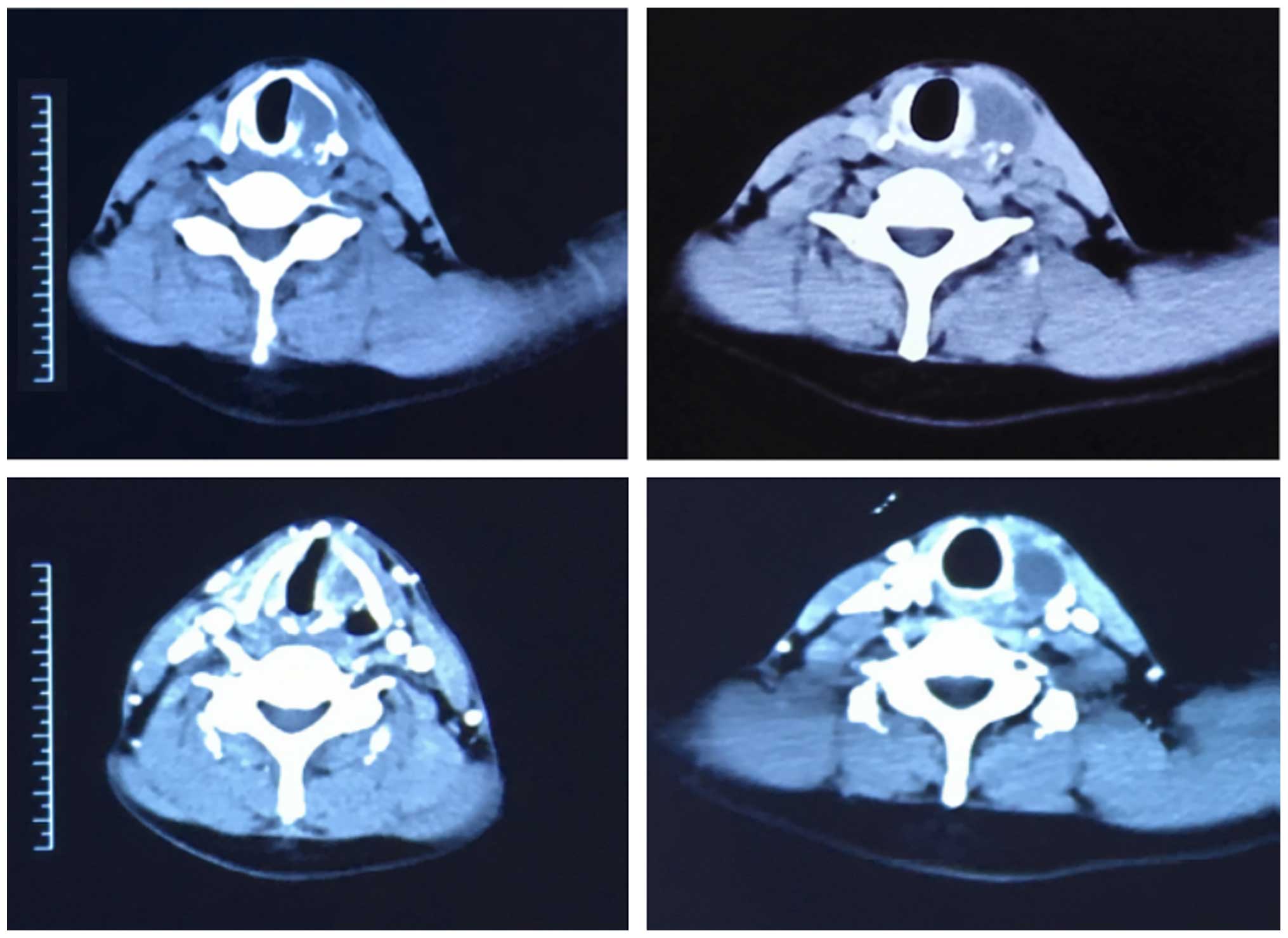
Computed tomography (CT) is reported to be superior
to plain films in showing the exact location and extent of the
tumor. Moreover, CT scans document even minimal deposits of
calcifications, which cannot be detected on conventional
radiographs (5,3). This patient's pre-operative CT scan
revealed an expansive mass of 6.0×5.0 cm in the posterior area of
the left thyroid cartilage lamina without gross inflation or
cortical breakage (Fig. 1). The mass
extended adjacently to the left thyroid lobe, without involving the
true vocal cord homo-laterally, the posterior commissure and
arytenoid cartilage. Calcific foci with a popcorn-like appearance
suggested a chondral origin.
Our diagnostic impression from the CT images and
other evaluations was probable chondroma or chondrosarcoma
(5). Pathological findings from a
fine-needle aspirate also suggested chondroma or
well-differentiated chondrosarcoma. The [F-18]fluorodeoxyglucose
positron emission tomography is helpful in grading tumors,
detecting metastasis and assessing local recurrence (6). The uptake value of 3.3 suggested a
malignancy, but with good differentiation; 1.3 is generally
considered the limit between benign and malignant lesions. It also
showed no evidence of metastasis to the lung or bone.
As the primary tumor had spread out of the
endolarynx by invading the thyroid cartilage, and as radiation or
chemoradiation therapy were inadequate at initial treatment, the
patient was recommended to undergo a total laryngectomy, left
lobectomy of thyroid and a tracheotomy. An apron incision was
outlined to incorporate the tracheostomy incision. The surgery
itself was uneventful (7).
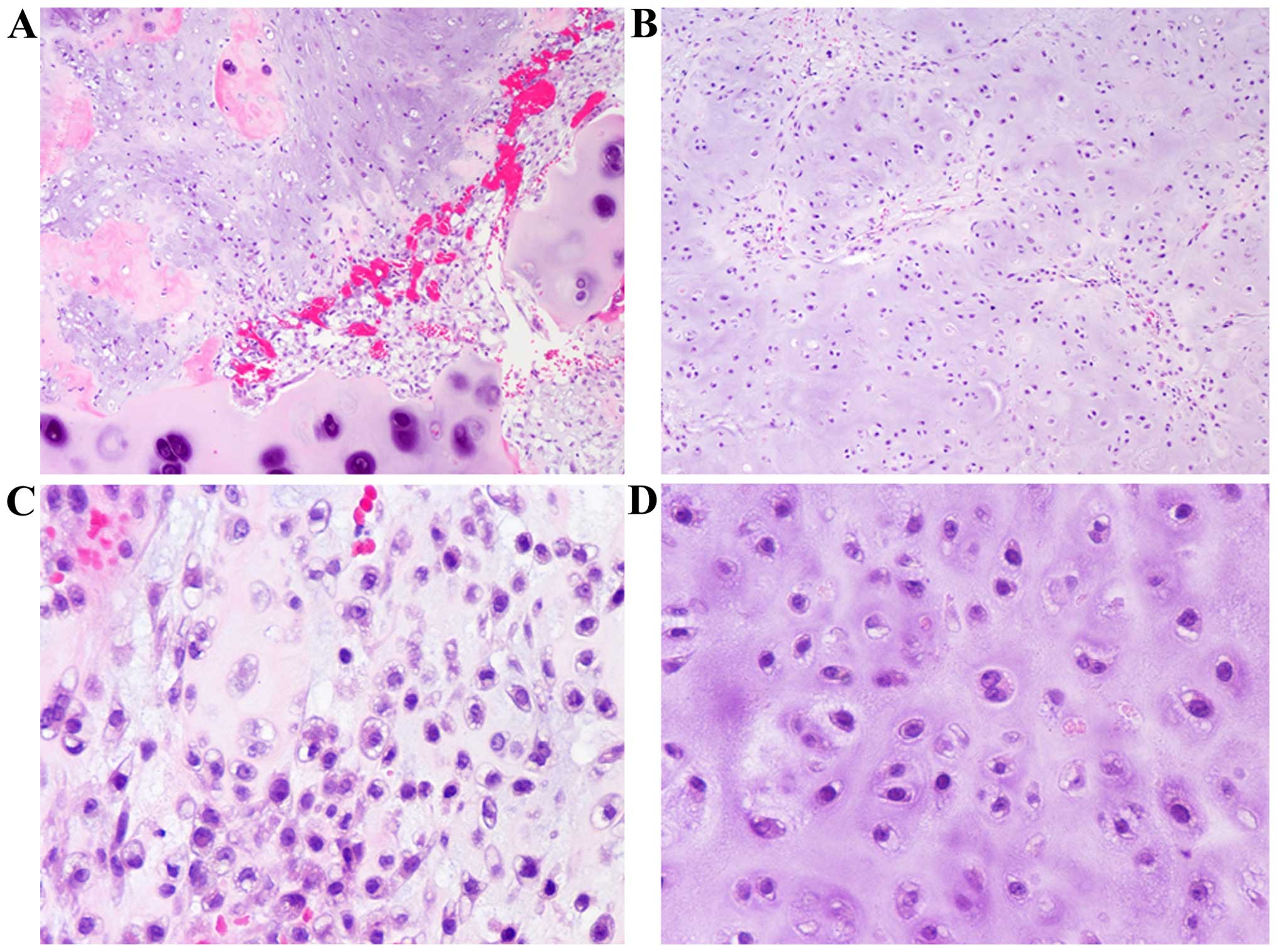
Histopathological examination of the resected
specimen revealed areas of increased cellularity and a greater
degree of cytological abnormality. Neoplastic cells formed clusters
of irregular size and distribution (grade I, chondrosarcoma with
myxoid components), with focal areas of grade II chondrosarcoma
(Fig. 2).
Chondrosarcoma is considered to be insensitive to
both radiation therapy (8) and
chemotherapy. Thus, the patient was regularly followed-up without
any adjuvant therapy, at a projected schedule of 1, 3, 6 and 12
months post-surgery, and every 6 months thereafter (Fig. 3). He is presently symptom-free without
any sign of recurrence.
Discussion
Primary chondrosarcoma arising from the larynx is a
rare disorder of unknown etiology, with a gradual development and a
long clinical course (9). A
chondrosarcoma that develops from the thyroid cartilage typically
protrudes laterally and presents as a firm mass in the neck, but
does not tend to grow into the airways or cause airway obstruction.
Owing to this asymptomatic progression, these tumors are frequently
in a locally advanced state at diagnosis. The pre-operative
evaluation protocol includes a series of imaging examinations and
cytology by needle biopsy (1,10). Imaging modality is important for
locating and delineating the primary tumor and regional metastases,
but is unsatisfactory in distinguishing chondromas from
chondrosarcomas (5,11).
Some authors have suggested that CT is the imaging
method of choice; it discloses a hypodense, well-defined image with
calcifications inside, cartilage destruction and structure
distortion. Others prefer magnetic resonance imaging (MRI) owing to
its greater accuracy in distinguishing between tumor and other
para-laryngeal tissues, with signal strength is low on T1 and high
on T2, with a characteristic mosaic pattern (6,12).
Unlike carcinomas in the neck area, pre-operative
cytological biopsy may not distinguish neoplasms originating from
the elastic cartilage from low-grade cervical sarcoma (11,13), or
between chondroma and low-grade malignancy.
The criteria for pathological diagnosis of
chondrosarcoma include the presence of a number of cells with
large, irregular and/or multiple nuclei, giant cartilage cells with
large single or multiple nuclei and nuclei containing clumped
chromatin upon histology (14), and
are the basis for 3 grades of chondrosarcoma. Grade I is similar to
a chondroma, >2 nuclei, no mitoses and some areas of
calcification and actual bone tissue, and accounts for 70–80% of
cases; grade II involves an increased cell number, a low
nuclear/cytoplasmic ratio and few mitoses; and grade III involves
multinucleated cells, an increased nuclear/cytoplasmic ratio and a
high number of mitoses (1). Notably,
however, grade I (as in the present case) is histologically
difficult to differentiate from chondroma, and requires combined
clinical, radiological and histological signs to diagnose. In
uncertain cases, lesions exceeding 2 cm are usually considered to
be chondrosarcomas (10,15).
Surgery is the treatment of choice, in order to
excise all tumor extensions to negative margins, using either an
external approach or endoscopy. However, cancer-specific recurrence
is common, with a reported rate of 18–40% (1,6,8,16). The
completeness of initial surgery is crucial to local disease
control. In the present case, we performed a total laryngectomy in
order to reduce the risk of local recurrence, having observed the
wide extent of the primary tumor and partial high-grade (grade II)
elements. Neither radiation therapy nor chemotherapy seems to be
effective in eliminating subclinical metastasis post-operatively,
particularly for low-grade, slow-growing tumors with few
proliferating cells (17,18). However, the long-term prognosis for
this rare tumor improves with radical surgery, possibly due to its
indolent nature.
A recent review of ‘Survival in Chondrosarcoma,’
based on the Surveillance, Epidemiology, and End Results (SEER)
database, suggested that head and neck bone sarcomas commonly have
a more favorable prognosis than axial tumors, which is partially
explained by earlier detection, expeditious treatment and fewer
metastases at presentation (19).
Owing to the rarity of this tumor, our presentation is considered
to be a literature-based clinical case. It also provides validation
and experience on its management from Eastern China and this may
promote communication and cooperation on clinical decision-making,
etiology, risk factors and therapeutic choices in the future.
Acknowledgements
The present study was supported by funds from the
National Science Foundation of China (grant nos. 81572622 and
81272934 awarded to Dr Qing-Hai Ji) and the Natural Science
Foundation of Shanghai (grant no. 12JC1402802 awarded to Dr
Qing-Hai Ji).
References
|
1
|
Polaczkiewicz D, Kochanowski B and
Jakubiszyn J: Laryngeal chondrosarcoma. Otolaryngol Pol. 51:(Suppl
25). 50–52. 1997.(In Polish). PubMed/NCBI
|
|
2
|
Oudidi A, Hachimi H and El Alami MN:
Laryngeal chondrosarcoma. Cancer Radiother. 9:343–346. 2005.(In
French). View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Potochny EM and Huber AR: Laryngeal
chondrosarcoma. Head Neck Pathol. 8:114–116. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhang SS, Xia QM, Zheng RS and Chen WQ:
Laryngeal cancer incidence and mortality in China, 2010. J Cancer
Res Ther. 11:(Suppl 2). C143–C148. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Obenauer S, Kunze E, Fischer U,
Schmidberger H and Grabbe E: Unusual chondrosarcoma of the larynx:
CT findings. Eur Radiol. 9:1625–1628. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rinaldo A, Howard DJ and Ferlito A:
Laryngeal chondrosarcoma: a 24-year experience at the Royal
National Throat, Nose and Ear Hospital. Acta Otolaryngol.
120:680–688. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Jabbour N and Tsue T: National operative
case log growth charts in otolaryngology-head and neck surgery
training. Otolaryngol Head Neck Surg. 152:73–79. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Domenech Campos E, Navarro-Conde P, Campos
Dana JJ, Fontal Alvarez M, Zaragosí Castelló JM and Terradez Raro
JJ: Advanced stage laryngeal chondrosarcoma. An Otorrinolaringol
Ibero Am. 29:473–481. 2002.(In Spanish). PubMed/NCBI
|
|
9
|
Eraso A, Lorusso GD and Palacios E:
Laryngeal chondrosarcoma. Ear Nose Throat J. 84:402–403.
2005.PubMed/NCBI
|
|
10
|
Hoffer ME, Pribitkin E, Keane WM and
Atkins JP: Laryngeal chondrosarcoma: diagnosis and management. Ear
Nose Throat J. 71:659–662. 1992.PubMed/NCBI
|
|
11
|
Ibarrola C, Vargas J and de Agustín P:
Laryngeal chondrosarcoma: fine needle aspiration (FNA) of an
unusual tumour. Cytopathology. 9:130–134. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chaturvedi A and Kane SV: Laryngeal
chondrometaplasia: a great mimic of chondrosarcoma. Indian J Pathol
Microbiol. 50:391–394. 2007.PubMed/NCBI
|
|
13
|
Brown DH, Turnbull DI and Heeneman H:
Laryngeal chondrosarcoma: gross pathological, histologic and
electron microscopic characteristics. Can J Surg. 28:534–536.
1985.PubMed/NCBI
|
|
14
|
Milanesi I: Histopathogenetic
considerations on a case of laryngeal chondrosarcoma. Ann Laringol
Otol Rinol Faringol. 67:767–776. 1968.(In Italian). PubMed/NCBI
|
|
15
|
Pareja Martínez A, Alberola Toriol V,
Severa Ferrándiz G and Infante Matarredona E: Chondrosarcoma of the
thyroid cartilage. Presentation of a case and review of the
literature. Acta Otorrinolaringol Esp. 40:373–376. 1989.(In
Spanish). PubMed/NCBI
|
|
16
|
Gierek T, Namysłowski G, Bielawska K and
Myrcik H: Laryngeal chondrosarcoma. Otolaryngol Pol. 35:173–176.
1981.(In Polish). PubMed/NCBI
|
|
17
|
Nicolai P, Ferlito A, Sasaki CT and
Kirchner JA: Laryngeal chondrosarcoma: incidence, pathology,
biological behavior, and treatment. Ann Otol Rhinol Laryngol.
99:515–523. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ghalib SH, Warner ED and DeGowin EL:
Laryngeal chondrosarcoma after thyroid irradiation. JAMA.
210:1762–1763. 1969. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Miller BJ: CORR Insights®:
survival in mesenchymal chondrosarcoma varies based on age and
tumor location: a survival analysis of the SEER Database. Clin
Orthop Relat Res. Apr 5–2016.(Epub ahead of print). View Article : Google Scholar
|