Introduction
Periosteal osteosarcoma (PO) is a rare tumor, which
usually originates from the diaphysis of long bones (1). On radiological examination, PO presents
as fusiform masses located in the periosteum that are accompanied
by periosteal reactions and a soft tissue mass (1). PO represents <2% of all osteosarcomas
(1) and this low incidence is
mirrored by the lack of large case series. The diagnosis of PO
should preclude high-grade surface sarcoma and parosteal sarcoma
(2,3).
Compared with other osteosarcoma subtypes, PO has a low propensity
to metastasize, and it is histologically an intermediate-grade
tumor. The therapeutic regimen for PO is controversial (4–6), although
there is a widely accepted consensus that a wide surgical excision
is the mainstay of treatment for PO (3–6). However,
post-operative limb function is usually compromised by a wide
excision as the procedure results in a considerable wound, which
leads to difficulties regarding reconstruction and rehabilitation
(5,6).
In the present study, a marginal resection was manipulated in the
setting of pre-operative chemotherapy for two patients with
intermediate PO; post-operative limb function was well preserved
and the patients were satisfied with the therapeutic outcome. The
current study presents the detailed therapeutic strategies used for
these two patients and conducts a review of the literature. Written
informed consent was obtained from the patients' families in both
cases.
Case report
Case 1
A 14-year-old boy presented to the General Hospital
of Jinan Military Commanding Region (Jinan, Shandong, China) in
July 2010 with a 4-week history of a progressively enlarging mass
and pain in the right knee. On examination, a tender, firm lump was
apparent in the right medial knee. The patient experienced
difficulty in walking, with fixed right knee flexion of 40°.
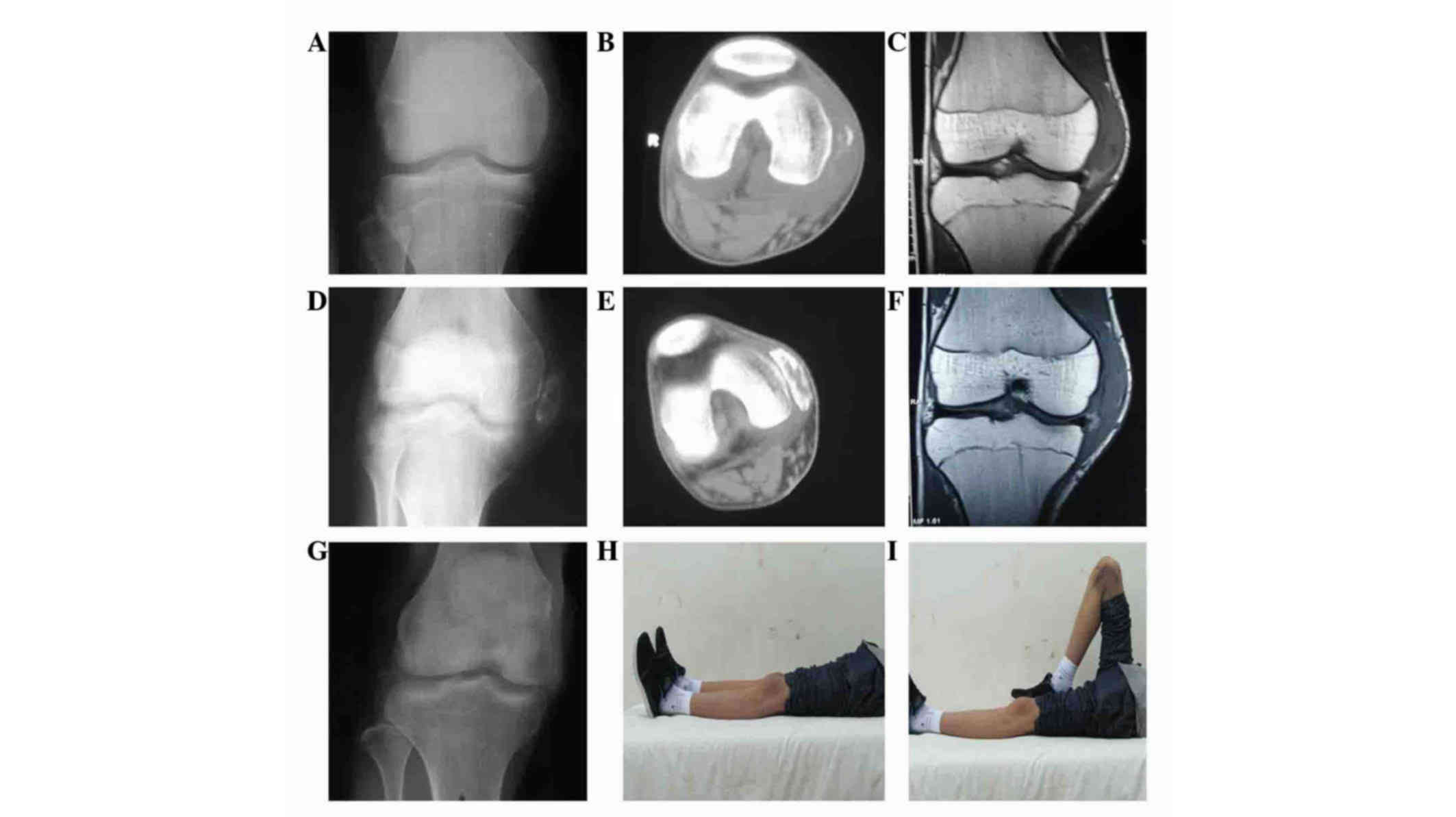
Imaging examinations, including X-ray, computed tomography (CT) and
magnetic resonance imaging (MRI) showed an osseous fusiform mass
encircling the right distal femur, whilst the periosteum was intact
(Fig. 1A-C). Tissue samples were
paraffin-embedded, fixed and cut into 5-µm sections. The tissue
sections were fixed with formalin. A biopsy of the lesion confirmed
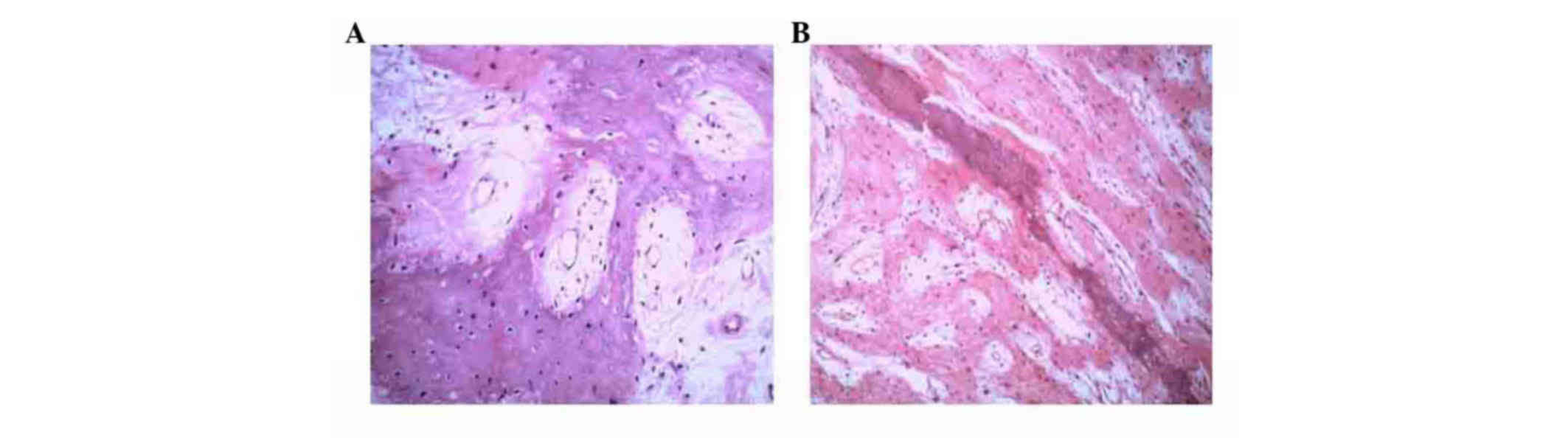
a diagnosis of PO; the hematoxylin and eosin-stained slides showed
spindle cells with osteoid matrix, indicating an intermediate-grade
tumor (Fig. 2A), according to the
grading system described by Unni and Dahlin (7). Bone scans and CT of the thorax ruled out
metastasis. The patient was started on two 2-week cycles of
chemotherapy (8–12 g/m2 high-dose methotrexate, 30
mg/m2 doxorubicin and 2.0 g/m2 ifosfamide)
with an interval of 2 weeks, and experienced pain relief, shrinkage
of the mass and an improvement in right knee motion (0–75°).
Furthermore, imaging findings showed that the mass had become
well-defined, with peripheral calcification (Fig. 1D-F). Surgery was performed 2 weeks
after the chemotherapy in the form of an excision of the tumor,
preserving the main structures, including the neurovascular
bundles, tendons, muscles and epiphyses. A limited excision of the
peripheral soft tissue (<2 cm from the tumor) and bone (<3 cm
from the tumor) was performed, and biological reconstruction of the
right medial collateral ligament was performed by forward locating
the right semitendinosus muscle tendon. The post-operative
histological findings indicated a good response to the
pre-operative chemotherapy (necrosis percentage, ≥90%) and a
negative excision margin. A single 2-week cycle of chemotherapy
(8–12 g/m2 high-dose methotrexate, 30 mg/m2
doxorubicin and 2.0 g/m2 ifosfamide), was performed at 2
weeks post-surgery, with an interval of 2 weeks. After being
discharged, the patient received five 2-week cycles of chemotherapy
(8–12 g/m2 high-dose methotrexate, 30 mg/m2
doxorubicin and 2.0 g/m2 ifosfamide), with an interval
of 2 weeks between chemotherapy cycles. At the end of the follow-up
period, the range of motion in the right knee was normal (0–130°).
Radiological findings demonstrated no metastases or recurrence
(Fig. 1G). Normal life activities
were recorded until the end of the follow-up time of 37 months
(Fig. 1H and I). According to the
Musculo-Skeletal Tumor Society (MSTS) functional scoring system,
the patient's score was 100% (8).
Case 2
A 14-year-old boy was referred to the General
Hospital of Jinan Military Commanding Region in August 2004 due to
a suspicious lesion in the right proximal medial tibia. Clinical
examination revealed a tender, bony-hard lump on the proximal
tibia. The patient's ambulatory ability was constrained, with fixed
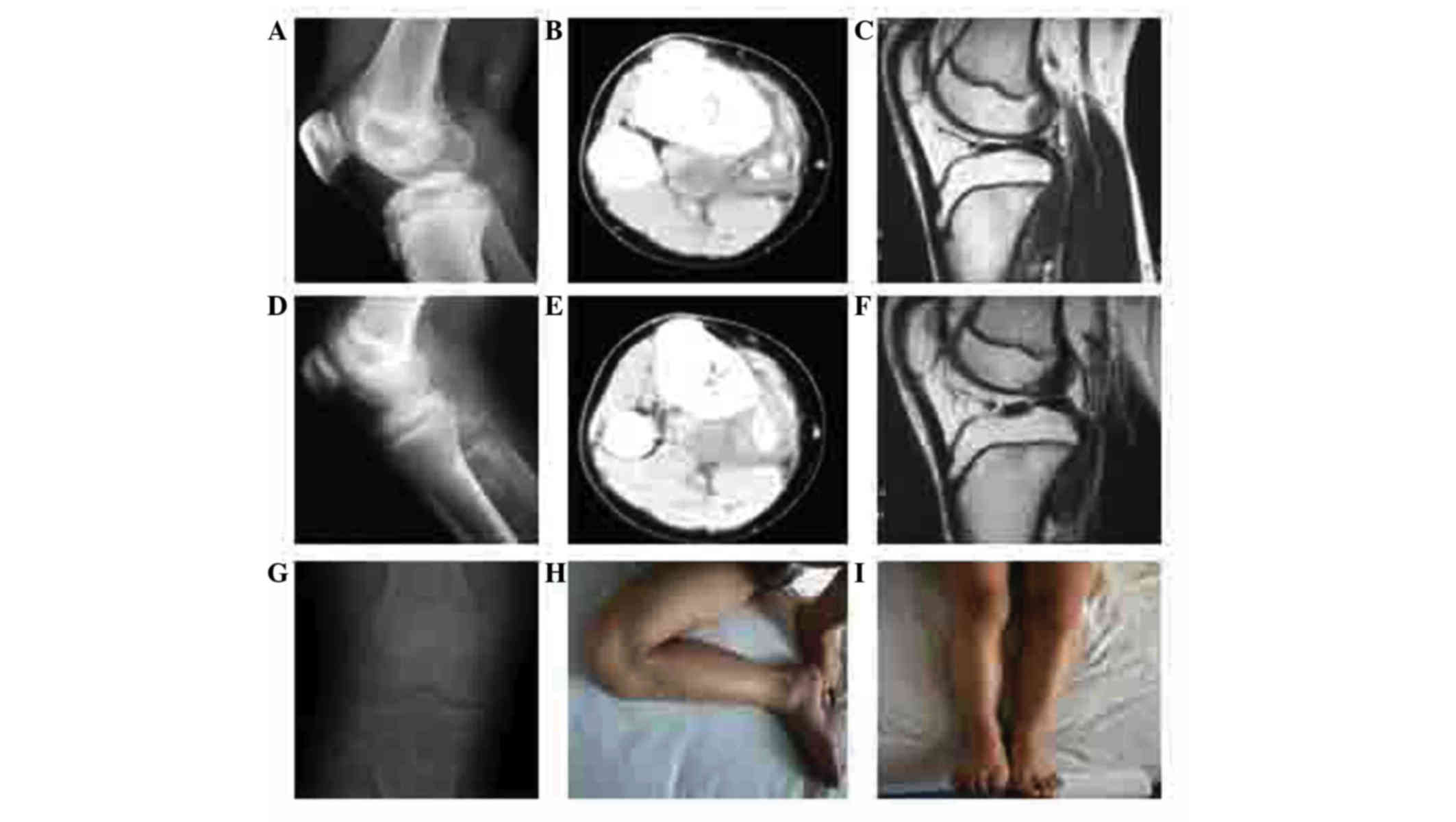
right knee flexion of 30°. Imaging findings indicated a
space-occupying mass adjacent to the cortex of the right proximal
tibia (Fig. 3A-C). Tissue samples
were paraffin-embedded, fixed and cut into 5-µm sections for
staining. The tissue sections were fixed with formalin. A diagnosis
of PO was determined by histopathological results; hematoxylin and
eosin-stained slides showed spindle cells with an osteoid matrix,
indicating that the tumor was of intermediate grade (Fig. 2B), according to the grading system
described by Meister et al (9). As a routine process, metastases was
ruled out. Next, two 2-week cycles of chemotherapy (120
mg/m2 cisplatin, 30 mg/m2 doxorubicin and 2.0
g/m2 ifosfamide) with an interval of 2 weeks were
started. The patient's symptoms were relieved along with improving
imaging findings, including a well-defined tumor border and
progressive calcification (Fig.
3D-F). A portion of the local tibial cortex and peripheral soft
tissue were removed along with the tumor in accordance with the
criteria for a marginal excision. The main functional structures
were preserved. The excised bone was soaked in 99% alcohol for
inactivation, followed by replantation. No other biological
reconstruction was performed. The post-operative histological
findings determined a good response and a negative margin. Routine
chemotherapy (2-week cycle of 120 mg/m2 cisplatin, 30
mg/m2 doxorubicin and 2.0 g/m2 ifosfamide
with an interval of 2 weeks) was commenced at 2 weeks post-surgery.
After being discharged, the patient underwent another six 2-week
cycles of chemotherapy (120 mg/m2 cisplatin, 30
mg/m2 doxorubicin and 2.0 g/m2 ifosfamide)
with an interval of 2 weeks. The patient experienced disease-free
survival in 108 months of follow-up (Fig.
3G). The range of motion in the right knee was normal (0–130°;
Fig. 3H and I), and the patient's
MSTS score was 100%. The patient had recommenced normal life
activities during the follow-up period.
Discussion
Previous studies have demonstrated that PO has less
aggressive behavior compared with other osteosarcoma subtypes
(10). According to one of these
studies, a PO diagnosis should preclude intramedullary involvement,
which may suggest tumor progression (3). By contrast, opposing studies have
concluded that medullary extension is frequent among PO cases
(11). Gulia et al (12) suggested that intramedullary
involvement may suggest the aggressive nature of PO. The present
study did not include medullary extension, however, we hypothesize
that if patients with intramedullary involvement were included, the
tumor grades could be elevated, resulting in adverse impact on the
results.
Since being introduced, multiple-agent chemotherapy
has greatly improved the long-term survival rate among osteosarcoma
patients, which is now 49–76% (13).
The frontline chemotherapeutic agents for osteosarcoma include
methotrexate, cisplatin, doxorubicin and ifosfamide (14). However, the role of chemotherapy as a
treatment for PO has been doubted. Since PO has less aggressive
behavior than other sarcoma subtypes, chemotherapy may be absent in
intermediate-grade PO (1,3–6). Clinical
studies have demonstrated that local recurrence rather than
chemotherapy is an important prognostic factor for survival in PO
(6,15). A single center study indicated that
wide resection is the only predictor for survival (1). However, a review of 17 cases with a mean
follow-up time of 52 months showed the encouraging effects of
chemotherapy, with results indicating 100% metastasis-free survival
among PO cases (3). Furthermore, the
outcome indicated that it may be too prudent for the decision to
use chemotherapy to be only shared with patients with high-grade
PO, suggesting that chemotherapy may be routinely utilized in PO of
intermediate grade (1,3,16). In the
present study, chemotherapy was administered in two
intermediate-grade PO patients who proved to be good responders to
the treatment, and who experienced disease-free survival times of
37 and 108 months, respectively, at last follow-up. Based on these
findings, chemotherapy may be beneficial to patients with PO of
intermediate grade.
There is wide consensus regarding aggressive
resection being used for PO (1,17,18). Tumors have been reported to spread
further than could be imaged using CT or MRI, and in addition, an
incomplete tumor resection is considered as the most important risk
factor for an adverse outcome. Therefore, a wide excision is
considered mandatory to achieve the complete removal of a tumor
(1,19,20).
However, a wide excision often necessitates removal of functional
structures, resulting in prolonged surgery time and compromised
limb function (3,8,20–22). Furthermore, recurrences and metastases
are not rare in patients undergoing a wide excision of a tumor
(1,19). Therefore, in the present study,
marginal excision of tumor preserving functional structures was
sought in the setting of effective neoadjuvant chemotherapy; two
cases without intramedullary involvement were enrolled to ensure
the intermediate tumor grade of the patients. The survival outcome
was encouraging, but more importantly, the patients returned to
normal daily activities and were satisfied with the outcome of the
treatment (22–24).
It is noteworthy that the discrimination of good
responders to chemotherapy is crucial for marginal excision
manipulation. Sumiya et al (25) argued that when a good response was
documented by at least two out of four radiological modalities,
including X ray, MRI, angiography and thallium-201 scintigraphy,
>90% tumor necrosis could be expected. In the present study, a
good response originated from symptomatic relief, improved imaging
findings and a good histopathological response to chemotherapy. It
should also be highlighted that only PO cases of intermediate grade
were included, and that further studies are warranted to verify the
effectiveness of marginal excision along with chemotherapy for
patients with higher grade PO.
In conclusion, marginal surgical removal of the
tumor in conjunction with effective neoadjuvant chemotherapy may
improve survival in patients with intermediate PO. Furthermore,
limb function could be restored to a good standard. The
discrimination of good responses to chemotherapy could be important
for marginal excision manipulation.
References
|
1
|
Cesari M, Alberghini M, Vanel D, Palmerini
E, Staals EL, Longhi A, Abate M, Ferrari C, Balladelli A and
Ferrari S: Periosteal osteosarcoma: A single-institution
experience. Cancer. 117:1731–1735. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Schajowicz F, McGuire MH, Araujo E
Santini, Muscolo DL and Gitelis S: Osteosarcomas arising on the
surfaces of long bones. J Bone Joint Surg Am. 70:555–564. 1988.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Revell MP, Deshmukh N, Grimer RJ, Carter
SR and Tillman RM: Periosteal osteosarcoma: A review of 17 cases
with mean follow-up of 52 months. Sarcoma. 6:123–130. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Okada K, Unni KK, Swee RG and Sim FH: High
grade surface osteosarcoma: A clinicopathologic study of 46 cases.
Cancer. 85:1044–1054. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Murphey MD, Jelinek JS, Temple HT,
Flemming DJ and Gannon FH: Imaging of periosteal osteosarcoma:
Radiologic-pathologic comparison. Radiology. 233:129–138. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Grimer RJ, Bielack S, Flege S, Cannon SR,
Foleras G, Andreeff I, Sokolov T, Taminiau A, Dominkus M,
San-Julian M, et al: Periosteal osteosarcoma-a European review of
outcome. Eur J Cancer. 41:2806–2811. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Unni KK and Dahlin DC: Grading of bone
tumours. Semin Diag Pathol. 1:165–172. 1984.
|
|
8
|
Kanazawa Y, Tsuchiya H, Nonomura A,
Takazawa K, Yamamoto N and Tomita K: Intentional marginal excision
of osteosarcoma of the proximal fibula to preserve limb function. J
Orthop Sci. 8:757–761. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Meister P, Konrad E, Lob G, Janka G, Keyl
W and Stürz H: Osteosarcoma: Histological evaluation and grading.
Arch Orthop Trauma Surg. 94:91–98. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ma Q, Zhou Y, Ma B, Chen X, Wen Y, Liu Y,
Fan Q and Qiu X: The clinical value of CXCR4, HER2 and CD44 in
human osteosarcoma: A pilot study. Oncol Lett. 3:797–801.
2012.PubMed/NCBI
|
|
11
|
Hall RB, Robinson LH, Malawar MM and
Dunham WK: Periosteal osteosarcoma. Cancer. 55:165–171. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gulia A, Puri A, Pruthi M and Desai S:
Oncological and functional outcome of periosteal osteosarcoma.
Indian J Orthop. 48:279–284. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Saeter G, Alvegård TA, Elomaa I, Stenwig
AE, Holmström T and Solheim OP: Treatment of osteosarcoma of the
extremities with the T-10 protocol, with emphasis on the effects of
preoperative chemotherapy with single-agent high-dose methotrexate:
A Scandinavian sarcoma group study. J Clin Oncol. 9:1766–1775.
1991.PubMed/NCBI
|
|
14
|
Arpaci F, Ataergin S, Ozet A, Erler K,
Basbozkurt M, Ozcan A, Komurcu S, Ozturk B, Celasun B, Kilic S and
Kuzhan O: The feasibility of neoadjuvant high-dose chemotherapy and
autologous peripheral blood stem cell transplantation in patients
with nonmetastatic high grade localized osteosarcoma: Results of a
phase II study. Cancer. 104:1058–1065. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Rose PS, Dickey ID, Wenger DE, Unni KK and
Sim FH: Periosteal osteosarcoma: Long-term outcome and risk of late
recurrence. Clin Orthop Relat Res. 453:314–317. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Papagelopoulos PJ, Galanis E, Sim FH and
Unni KK: Periosteal osteosarcoma. Orthopedics. 22:971–974.
1999.PubMed/NCBI
|
|
17
|
Singh D, Sen R, Chaudhary S and Tripathy
SK: Periosteal osteosarcoma of the calcaneum: A case report. Foot
Ankle Spec. 5:121–123. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Maheshwari AV, Jelinek JS, Seibel NL,
Meloni-Ehrig AM, Kumar D and Henshaw RM: Bilateral synchronous
tibial periosteal osteosarcoma with familial incidence. Skeletal
Radiol. 41:1005–1009. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Masterson EL, Ferracini R, Davis AM,
Wunder JS and Bell RS: The geometric osteotomy: Joint preservation
in juxta-articular surface bone neoplasms. Sarcoma. 1:167–174.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tsuchiya H, Tomita K, Mori Y, Asada N and
Yamamoto N: Marginal excision for osteosarcoma with caffeine
assisted chemotherapy. Clin Orthop Relat Res. 27–35.
1999.PubMed/NCBI
|
|
21
|
Kabukcuoglu Y, Grimer RJ, Tillman RM and
Carter SR: Endoprosthetic replacement for primary malignant tumors
of the proximal femur. Clin Orthop Relat Res. 8–14. 1999.PubMed/NCBI
|
|
22
|
Tsuchiya H, Tomita K, Mori Y, Asada N,
Morinaga T, Kitano S and Yamamoto N: Caffeine-assisted chemotherapy
and minimized tumor excision for nonmetastatic osteosarcoma.
Anticancer Res. 18:657–666. 1998.PubMed/NCBI
|
|
23
|
Enneking WF, Dunham W, Gebhardt MC,
Malawar M and Pritchard DJ: A system for the functional evaluation
of reconstructive procedures after surgical treatment of tumors of
the musculoskeletal system. Clin Orthop Relat Res. 241–246.
1993.PubMed/NCBI
|
|
24
|
Winkler K, Beron G, Delling G, Heise U,
Kabisch H, Purfürst C, Berger J, Ritter J, Jürgens H, Gerein V, et
al: Neoadjuvant chemotherapy of osteosarcoma: Results of a
randomized cooperative trial (COSS-82) with salvage chemotherapy
based on histological tumor response. J Clin Oncol. 6:329–337.
1988.PubMed/NCBI
|
|
25
|
Sumiya H, Taki J, Tsuchiya H, Nonomura A,
Miyauchi T and Tonami N: Midcourse thallium-201 scintigraphy to
predict tumor response in bone and soft-tissue tumors. J Nucl Med.
39:1600–1604. 1998.PubMed/NCBI
|