Introduction
Gastric cancer (GC), a highly heterogeneous disease,
is one of the most frequent malignancies and the second leading
cause of cancer-related death worldwide (1). Currently, GC still presents high rates
of morbidity and mortality in China as before (2). Despite many advances in new therapeutic
strategies, such as surgery combined molecular targeted therapy,
has been successfully used for GC, the five-year survival rate of
advanced GC still remains unsatisfactory. The poor survival is
mainly ascribed to late detection. Commonly, patients with locally
advanced GC when diagnosed may experience a high risk of recurrence
(3). Thus, it is widely shared that
early detection is an efficient way to improve the prognosis of GC
(4). Traditional markers such as CEA,
CA199, CA724 and CA125 are frequently used for GC diagnosis,
predicting prognosis, and monitoring postoperative recurrence.
Unfortunately, these markers could not take both sensitivity and
specificity into consideration at the same time in GC detection,
particularly in early stage GC diagnosis. Therefore, exploration of
novel tumor markers for GC is extremely urgent.
Mannose receptor (MR) is commonly expressed in
selected populations of macrophages and dendritic cells (DCs) and
mediates the phagocytosis of pathogens and further anti-pathogenic
microorganism immunity by recognition the pathogen associated
molecular patterns (PAMPs) (5). MR
expressed on lymphatic endothelium takes part in the adhesion of
several cancer cells to lymphatic endothelium and facilitates
lymphatic metastasis (6). Currently,
the presence of serum soluble mannose receptor (sMR) has been
successfully identified (7). Serum
levels of sMR are remarkably elevated in infectious diseases,
sepsis and critical illness (8,9). For
malignancy, serum sMR increased in patients with multiple myeloma
and is demonstrated as an independent marker for overall survival
(10). These inspiring results
support that serum sMR may be a novel serum tumor marker. CD163, a
monocyte-macrophage scavenger receptor, together with MR, are
regarded as macrophage-activation markers. CD163 is described to
remove the redundant free hemoglobin by recognition
hemoglobin-haptoglobin complex in human body (11). Then, functions of anti-inflammatory
and anti-pathogenic microorganism of CD163 have been identified
(12). Soluble CD163 (sCD163) is
generated by proteolytic cleavage of membrane protein and then shed
into serum or tissue fluid as a soluble form (13). Some papers have been reported that
serum sCD163 is increased in the inflammatory and critical diseases
(9,14). Strikingly, serum sCD163 is highly
expressed in several malignancies, including liver cancer, ovarian
cancer, leukemia and multiple myeloma, and sCD163 is identified as
negative prognostic factors for these cancers (15–18). As
promising biomarkers, serum sCD163 and sMR in detection as well as
evaluating prognosis of GC patients are unfortunately absent. In
this study, we will investigate the potential of preoperative serum
levels of sCD163 and sMR in diagnosis and prognosis of GC patients
and expect the results will benefit GC patients in clinic.
Materials and methods
Clinical samples
We recruited 143 patients with gastric cancer (GC),
66 subjects with benign gastric disease (BGD), and 59 healthy
controls (HCs) from the Jingmen First People's Hospital between
March 2012 and June 2013. All subjects were recruited
consecutively. Serum samples were stored at −80°C until they were
analyzed. The median age of the GC patients was 64 (range 35–89)
years. Among them, 24 patients suffered early GC and 119 patients
suffered advanced GC. The median age of the BGD patients was 59
(range 24–87) years. Among them, 17 patients had non-atrophic
gastritis, 9 patients had atrophic gastritis, 23 patients had
benign gastric ulcer, 14 patients had polyp and 3 patients had
gastric adenoma. The median age of the healthy controls was 63
(range 31–84) years. Circulating CEA, CA199, CA125 and CA724 levels
were determined by electro-chemiluminescence immunoassay (ECLIA).
The normal reference values in this study were as follows: CEA≤4.7
ng/ml, CA199≤39.0 U/ml, CA125≤35 U/ml, CA724≤6.9 U/ml. Clinical
parameters for GC patients were acquired from hospitalization
records. The clinical stage for GC patients was diagnosed according
to the criteria established by American Joint Committee on Cancer
in 2010 (12). All of the subjects
with GC and BGD were determined by endoscopy and confirmed by
biopsy. Each healthy control was submitted to a routine physical
examination, and all of the results were in the normal range.
Additionally, all cases of subjects with EBV-positive test results,
severe infections, known allergic disease, other malignancies, and
poor performance status were excluded from the present study. Data
collection and subsequent analyses were conducted by two
independent researchers. The study was approved by the Research
Ethics Committee of Jingmen First People's Hospital, and informed
consent was obtained from all participants, in agreement with the
institutional guidelines.
Enzyme-linked immunosorbent assay
(ELISA)
Soluble MR (sMR) and soluble CD163 (sCD163) in human
serum were detected using standard sandwich ELISA. Briefly, 96-well
microplates were coated with 100 µl of anti-MR goat polyclonal
antibody (pAb, Santa Cruz Biotechnology, Inc., CA, USA) or
anti-CD163 rabbit polyclonal antibody (pAb, Santa Cruz
Biotechnology, Inc., CA, USA) at a final concentration of 0.2 and
1.0 µg/ml, respectively, and incubated overnight at 4°C. The plates
were washed three times with phosphate-buffered saline (PBS)
containing 0.05% Tween-20 (PBST, PH 7.4), and the wells were
blocked with blocking buffer at 37°C for 90 min. Subsequently, 100
µl of undiluted serum from patients and healthy individuals was
added to the wells in duplicate. As a negative control, 100 µl of
PBS without antibody was used. Each plate was incubated at 37°C for
90 min. Subsequently, the plates were washed three times using
PBST, and 100 µl of anti-MR mouse monoclonal antibody (mAb, Abcam,
Inc., UK) diluted to a concentration of 0.5 µg/ml or anti-CD163
mouse monoclonal antibody (mAb, Abcam, Inc., UK) diluted to a
concentration of 1.0 µg/ml was added. The plates were incubated at
37°C for 90 min. After washing, 100 µl of peroxidase-conjugated
anti-mouse antibody (ZSGB-BIO) diluted to a concentration of 0.5
µg/ml was added for 60 min at 37°C. Subsequently, the plates were
washed three times and incubated with
3,3′,5,5′-tetramethy-lbenzidine (TMB, TIANGEN BIOTECH CO, LTD.) at
37°C for 30 min. Finally, the reaction was stopped by adding 2.0
mol/l H2SO4. The optical density (OD) was
measured on a microplate reader at a wavelength of 450 nm. For
standardization, the standard curve was constructed by plotting the
optical density (X) of the standards at 450 nm against the
concentration (Y) of the standards. A second-order polynomial
equation was used to fit the standards, and the quantitative sMR
and sCD163 concentrations were determined by comparing the optical
density values with the standard curve.
Statistical analysis
Differences between count data were confirmed by χ2
test or corresponding continuity correction. The non-parametric
Mann-Whitney U test was used to determine the statistical
significance between the two groups. The statistical significance
among more than two groups was determined with the Kruskal-Wallis
nonparametric test. Receiver operating characteristic (ROC)
analysis was performed to evaluate the diagnostic value of serum
markers in GC. Area under curve (AUC) is a parameter which
represents the diagnostic potential of tumor markers in ROC
analysis. The optimal serum cut-off values were calculated using
the maximum sum of the sensitivity and specificity. The logistic
regression model was used to combine the results from serum levels
of sMR and sCD163 to enhance the accuracy. Correlations of two
parameters were evaluated by using the non-parametric Spearman rank
correlation coefficient test. Overall survival (OS) was defined as
the time from surgery to the last follow-up or death of any cause.
Survival curves were plotted using the Kaplan-Meier method, and
group differences in survival times were assessed by log-rank test.
Cox proportional hazards models were used to assess the
correlations of clinical variables with survival. Cox regression
analysis was performed at both the univariate and multivariate
levels. P<0.05 was considered to indicate a statistically
significant difference. All statistical analyses were performed
using GraphPad Prism5 (GraphPad Software, Inc., San Diego, CA) and
SPSS statistics software (version 17.0, Chicago, IL, USA).
Results
Preoperative serum sMR and sCD163
concentrations on ELISA were significantly higher in GC patients
than in all controls
To evaluate the diagnostic potential of sMR and
sCD163 for GC, we detected preoperative serum concentrations of sMR
and sCD163 in patiens with GC, BGD, and HCs. Additionally, we also
reviewed serum levels of CEA, CA199, CA724 and CA125 as controls.
In this study, preoperative serum levels of sMR ranged from 0.165
to 0.885 µg/ml (median=0.374 µg/ml) in GC patients, from 0.145 to
0.512 µg/ml (median=0.282 µg/ml) in BGD patients, and from 0.125 to
0.501 µg/ml (median=0.250 µg/ml) in HCs. The preoperative serum
levels of sCD163 ranged from 0.291 to 1.760 µg/ml (median=0.628
µg/ml) in GC patients, from 0.244 to 0.908 µg/ml (median=0.430
µg/ml) in BGD patients, and from 0.208 to 0.726 µg/ml (median=0.430
µg/ml) in HCs. Serum sMR and sCD163 levels in GC patients were
significantly elevated compared with BGD patients and HCs
(P<0.0001; Fig. 1A, B).
Strikingly, there was no statistical significance in serum sMR and
sCD163 levels between HCs and BGD patients (P=0.2865; Fig. 1A, P=0.1164; Fig. 1B, respectively). Further, serum levels
of CEA, CA199, CA724 and CA125 in GC were significantly higher
compared with that in HCs and BGC group (P<0.05), but the serum
levels of CA125 between GC and BGD patients is a exception in
present study (P=0.1839) (Fig.
1C-F).
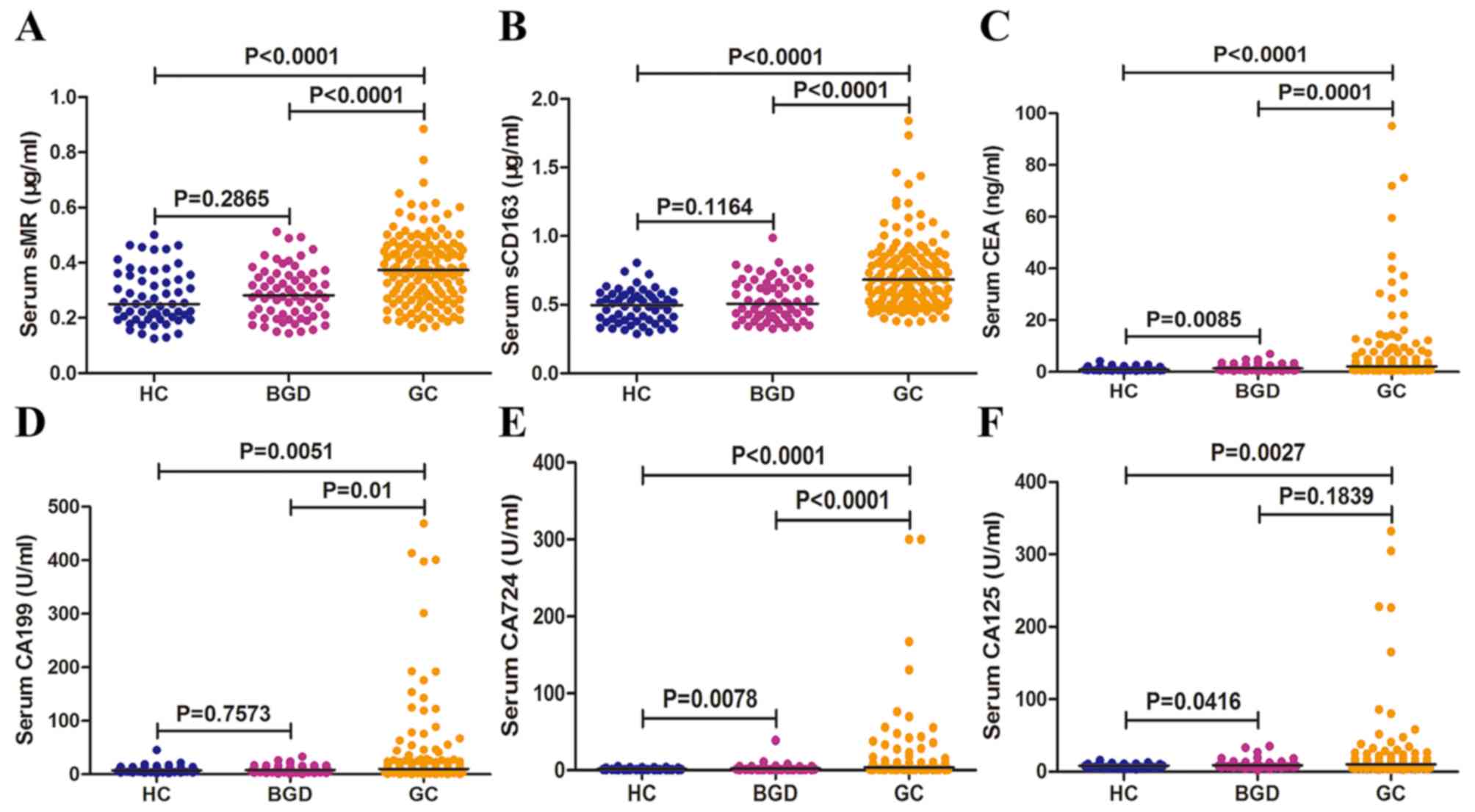 | Figure 1.Preoperative serum sMR, sCD163, CEA,
CA199, CA125 and CA724 concentrations in three groups. Preoperative
serum levels of sMR (A), sCD163 (B), CEA (C), CA199 (D), CA724 (E),
and CA125 (F) in three groups. Each point represents the serum sMR,
sCD163, CEA, CA199, CA125 or CA724 level of one sample. The
horizontal line indicates the median level. HC, healthy control;
BGD, benign gastric disease; GC, gastric cancer. |
Preoperative serum sMR and sCD163
displayed higher diagnostic potential than CEA, CA199, CA125 and
CA724 for GC
ROC analysis is an important methods using to
compare the predictive ability as well as acquire optimal
discriminated value for cancer diagnosis. Since preoperative serum
sMR and sCD163 levels in GC patients were significant elevated than
those of BGD patients and HCs and may be novel markers for GC
diagnosis, we reasonably conducted a ROC analysis to evaluate the
diagnostic capacity of serum sMR and sCD163. In current study, ROC
curves for GC patients suggested that the optimum diagnostic
cut-off for serum sMR was 0.3405 µg/ml (AUC 0.7284, sensitivity
61.54%, and specificity 73.60%) relative to all controls (Fig. 2A). For sCD163, the optimum diagnostic
cut-off was 0.6645 µg/ml (AUC 0.7766, sensitivity 53.85%, and
specificity 86.40%) (Fig. 2A).
Strikingly, measurement of serum sMR and sCD163 together obviously
enhanced the diagnostic accuracy for GC vs. all controls (AUC
0.8490, sensitivity 70.63%, and specificity 84.00%) (Fig. 2A). According to current cut-off
values, the positive rates of serum sMR, sCD163, and together of
them for GC diagnosis were 61.54, 53.85, and 65.73%, respectively
(Fig. 2B). In order to compare the
predictive power of serum sMR and sCD163 with traditional markers,
we performed ROC analyses for serum CEA, CA199, CA125 and CA724.
For single diagnosis, CA724 was apparently superior to CEA, CA199
and CA125 with AUC of 0.7403, but was inferior to sCD163 (Fig. 2C). Then, the combined prediction of
CEA and CA724 showed the highest diagnostic potential with AUC of
0.7979 in any kinds of two markers combination, which was similarly
lower than sMR and sCD163 combination (Fig. 2D). Further, any kinds of combined
detection of three or four tumor markers obviously increased
diagnostic ability, however, that were inferior to sMR and sCD163
combination (Fig. 2E, F). As
displayed in Table I, the combination
of sMR and sCD163 for GC diagnosis is also associated with better
diagnostic parameters (accuracy, PPV and NPV) than traditional GC
markers.
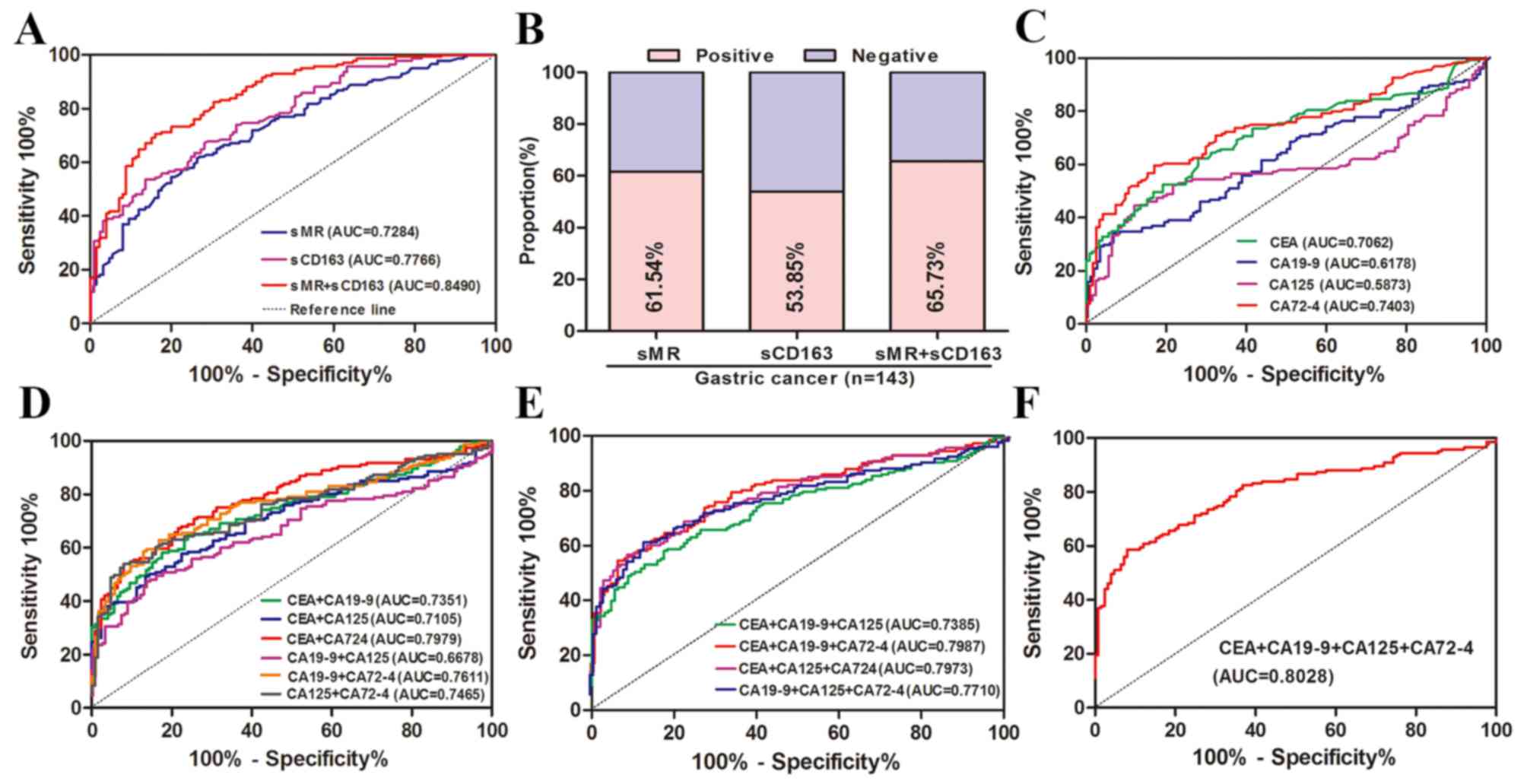 | Figure 2.Diagnostic potential of preoperative
serum levels of sMR, sCD163, CEA, CA199, CA125 and CA724 in GC
detection. (A) ROC curves for sMR, sCD163 and the combination of
them for GC patients vs. all controls. (B) Positive rates of sMR,
sCD163 and the combination of them for GC patients vs. all
controls. (C) ROC curves for single of CEA, CA199, CA125 and CA724
for GC patients vs. all controls. (D) ROC curves of combined
determination for two of CEA, CA199, CA125 and CA724 for GC
patients vs. all controls. (E) ROC curves of combined determination
for three of CEA, CA199, CA125 and CA724 for GC patients vs. all
controls. (F) ROC curves for combined determination of CEA, CA199,
CA125 and CA724 for patients with GC vs. all controls. ROC,
receiver operating characteristics; AUC, area under curve. |
 | Table I.Diagnostic parameters of serum sMR,
sCD163, CEA, CA199, CA125, and CA724 in detection of GC. |
Table I.
Diagnostic parameters of serum sMR,
sCD163, CEA, CA199, CA125, and CA724 in detection of GC.
| Variable | AUC | Sen (%) | Spe (%) | Acc (%) | PPV (%) | NPV (%) | Pos LR | Neg LR |
|---|
| sMR | 0.7284 | 61.54 | 73.60 | 67.16 | 72.73 | 62.59 | 2.33 | 0.62 |
| sCD163 | 0.7766 | 53.85 | 86.40 | 69.03 | 81.91 | 62.07 | 3.96 | 0.53 |
| sMR+sCD163 | 0.8490 | 70.63 | 84.00 | 76.87 | 83.47 | 71.43 | 4.41 | 0.35 |
| CEA(A) | 0.7062 | 62.24 | 72.00 | 66.79 | 71.77 | 62.50 | 2.22 | 0.52 |
| CA199(B) | 0.6178 | 33.57 | 93.60 | 61.57 | 85.71 | 55.19 | 5.25 | 0.71 |
| CA125(C) | 0.5873 | 44.76 | 88.00 | 64.92 | 81.01 | 58.20 | 3.73 | 0.63 |
| CA724(D) | 0.7403 | 59.44 | 83.20 | 70.52 | 80.19 | 64.20 | 3.54 | 0.49 |
| A+B | 0.7351 | 65.03 | 76.00 | 70.15 | 75.61 | 65.52 | 2.71 | 0.46 |
| A+C | 0.7105 | 49.65 | 86.40 | 66.79 | 80.68 | 60.00 | 3.65 | 0.58 |
| A+D | 0.7979 | 55.24 | 92.00 | 72.39 | 88.76 | 64.25 | 6.91 | 0.49 |
| B+C | 0.6678 | 83.22 | 16.00 | 51.87 | 53.13 | 45.45 | 0.99 | 1.05 |
| B+D | 0.7611 | 62.94 | 83.20 | 72.39 | 81.09 | 66.24 | 3.75 | 0.45 |
| C+D | 0.7465 | 53.85 | 92.00 | 71.64 | 88.50 | 63.54 | 6.73 | 0.50 |
| A+B+C | 0.7385 | 58.04 | 82.40 | 69.40 | 79.05 | 63.19 | 3.30 | 0.51 |
| A+B+D | 0.7987 | 55.24 | 93.60 | 73.13 | 90.8 | 64.64 | 8.60 | 0.48 |
| A+C+D | 0.7973 | 58.04 | 91.20 | 73.50 | 88.30 | 65.52 | 6.60 | 0.46 |
| B+C+D | 0.7710 | 61.54 | 87.20 | 73.51 | 84.62 | 66.46 | 4.81 | 0.44 |
| A+B+C+D | 0.8028 | 58.74 | 92.00 | 74.25 | 89.36 | 66.91 | 7.34 | 0.45 |
Preoperative serum levels of sMR and
sCD163 correlated significantly with serum CEA, CA199, CA724 and
CA125 concentrations in GC patients
Then, we evaluated the relationships of preoperative
serum sMR and sCD163 expression with traditional GC markers. As
shown in Table II, the serum levels
of sMR in GC patients correlated significantly with the CEA levels
with a Spearman correlation coefficient of 0.202 (P=0.016).
Similarly, serum levels of sMR were associated remarkably with
CA199 and CA125 (r=0.216, P=0.010; r=0.187, P=0.025, respectively).
Contrary to the above results, serum levels of sMR displayed no
association with the concentrations of CA724, with a Spearman
correlation coefficient of 0.032 (P=0.704). Further, significant
correlations were identified between the serum levels of sCD163 and
CEA, CA199, CA125, and CA724 (r=0.307, 0.204, 0.356, and 0.165;
P=0.002, P=0.015, P<0.0001 and P=0.049, respectively).
| Table II.Correlations of preoperative serum
sMR and sCD163 levels with CEA, CA199, CA125, and CA724
concentrations, respectively. |
Table II.
Correlations of preoperative serum
sMR and sCD163 levels with CEA, CA199, CA125, and CA724
concentrations, respectively.
|
| sMR | sCD163 |
|---|
|
|
|
|
|---|
| Variable | r | P-value | r | P-value |
|---|
| CEA | 0.202 | 0.016 | 0.307 |
0.0002 |
| CA199 | 0.216 | 0.010 | 0.204 | 0.015 |
| CA125 | 0.187 | 0.025 | 0.356 | <0.0001 |
| CA724 | 0.032 | 0.704 | 0.165 | 0.049 |
Preoperative serum sMR and sCD163
concentrations exhibited significant associations with major
clinical variables, such as TNM stage, survival status
We next investigated the relationships of
preoperative serum levels of sMR and sCD163 with age, sex, tumor
size, differentiation, T stage, N stage, M stage, clinical stage,
CEA, CA199, CA125, CA724 and dead status by using χ2 test. As shown
in Table III, serum sMR expression
in GC patients exhibited significant associations with T stage
(P=0.004), N stage (P=0.022), M stage (P=0.034), Clinical stage
(P=0.003), CEA (P=0.001), CA199 (P=0.016) and vital status
(P=0.010). However, no differences in serum sMR levels were
identified on the basis of age, sex, tumor size and
differentiation. Further, serum sCD163 expression in GC patients
displayed remarkably associations with differentiation (P=0.011), T
stage (P<0.001), N stage (P<0.001), M stage (P=0.003),
Clinical stage (P<0.001), CEA (P=0.020), CA199 (P=0.023) and
vital status (P=0.001). Unfortunately, no significant correlations
were indentified for serum sCD163 expression according to age, sex,
tumor size, CA125 and CA724.
| Table III.Correlations between preoperative
serum sMR and sCD163 levels with major clinical variables. |
Table III.
Correlations between preoperative
serum sMR and sCD163 levels with major clinical variables.
|
| Serum sMR
(µg/ml) |
| Serum sCD163
(µg/ml) |
|
|---|
|
|
|
|
|
|
|---|
| Variables | Low (n=55) | High (n=88) | P | Low (n=66) | High (n=77) | P-value |
|---|
| Age, years |
|
| 0.628 |
|
| 0.243 |
|
<60 | 16 | 29 |
| 24 | 21 |
|
|
≥60 | 39 | 59 |
| 42 | 56 |
|
| Sex |
|
| 0.221 |
|
| 0.523 |
|
Male | 41 | 57 |
| 47 | 51 |
|
|
Female | 14 | 31 |
| 19 | 26 |
|
| Tumor size, cm |
|
| 0.628 |
|
| 0.085 |
| ≤5 | 39 | 59 |
| 50 | 48 |
|
|
>5 | 16 | 29 |
| 16 | 29 |
|
|
Differentiation |
|
| 0.714 |
|
| 0.011 |
|
Well/Moderate | 29 | 37 |
| 38 | 28 |
|
|
Poor | 26 | 51 |
| 28 | 49 |
|
| T stage |
|
| 0.004 |
|
| <0.001 |
|
T1+T2 | 23 | 17 |
| 31 | 9 |
|
|
T3+T4 | 32 | 71 |
| 35 | 68 |
|
| N stage |
|
| 0.022 |
|
| <0.001 |
| N0 | 26 | 25 |
| 42 | 9 |
|
|
N1-N3 | 29 | 63 |
| 24 | 68 |
|
| M stage |
|
| 0.034 |
|
| 0.003 |
| M0 | 53 | 75 |
| 65 | 63 |
|
| M1 | 2 | 13 |
| 1 | 14 |
|
| Clinical stage |
|
| 0.003 |
|
| <0.001 |
|
I+II | 34 | 32 |
| 51 | 15 |
|
|
III+IV | 21 | 56 |
| 15 | 62 |
|
| CEA |
|
| 0.001 |
|
| 0.020 |
|
Negative | 48 | 55 |
| 55 | 58 |
|
|
Positive | 7 | 33 |
| 11 | 29 |
|
| CA199 |
|
| 0.016 |
|
| 0.023 |
|
Negative | 51 | 68 |
| 60 | 59 |
|
|
Positive | 4 | 20 |
| 6 | 18 |
|
| CA125 |
|
| 0.078 |
|
| 0.191 |
|
Negative | 54 | 78 |
| 63 | 69 |
|
|
Positive | 1 | 10 |
| 3 | 8 |
|
| CA724 |
|
| 0.663 |
|
| 0.363 |
|
Negative | 40 | 61 |
| 51 | 50 |
|
|
Positive | 15 | 27 |
| 15 | 27 |
|
| Vital status |
|
| 0.010 |
|
| 0.001 |
| No | 46 | 56 |
| 56 | 46 |
|
|
Yes | 9 | 32 |
| 10 | 31 |
|
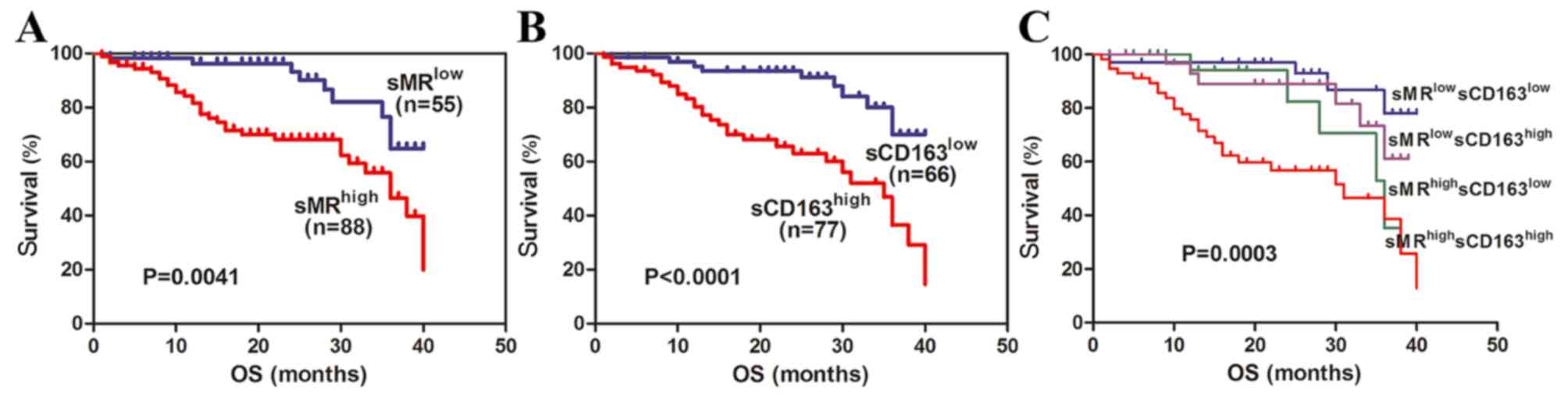
High expression of preoperative serum
levels of sMR and sCD163 correlated significantly with shorter
overall survival
In current study, all GC patients were followed up
with longest follow-up period of 40 months. According to currently
established cut-off values for sMR and sCD163, high expression of
preoperative serum sMR and sCD163 exhibited shorter OS in GC
patients (P=0.0041; Fig. 3A,
P<0.0001; Fig. 3B, respectively).
Consequently, we stratified GC patients into four subgroups based
on sMR and sCD163 simultaneously. High expression of serum sMR as
well as sCD163 simultaneously revealed obviously shorter OS and
significant difference was identified between four subgroups
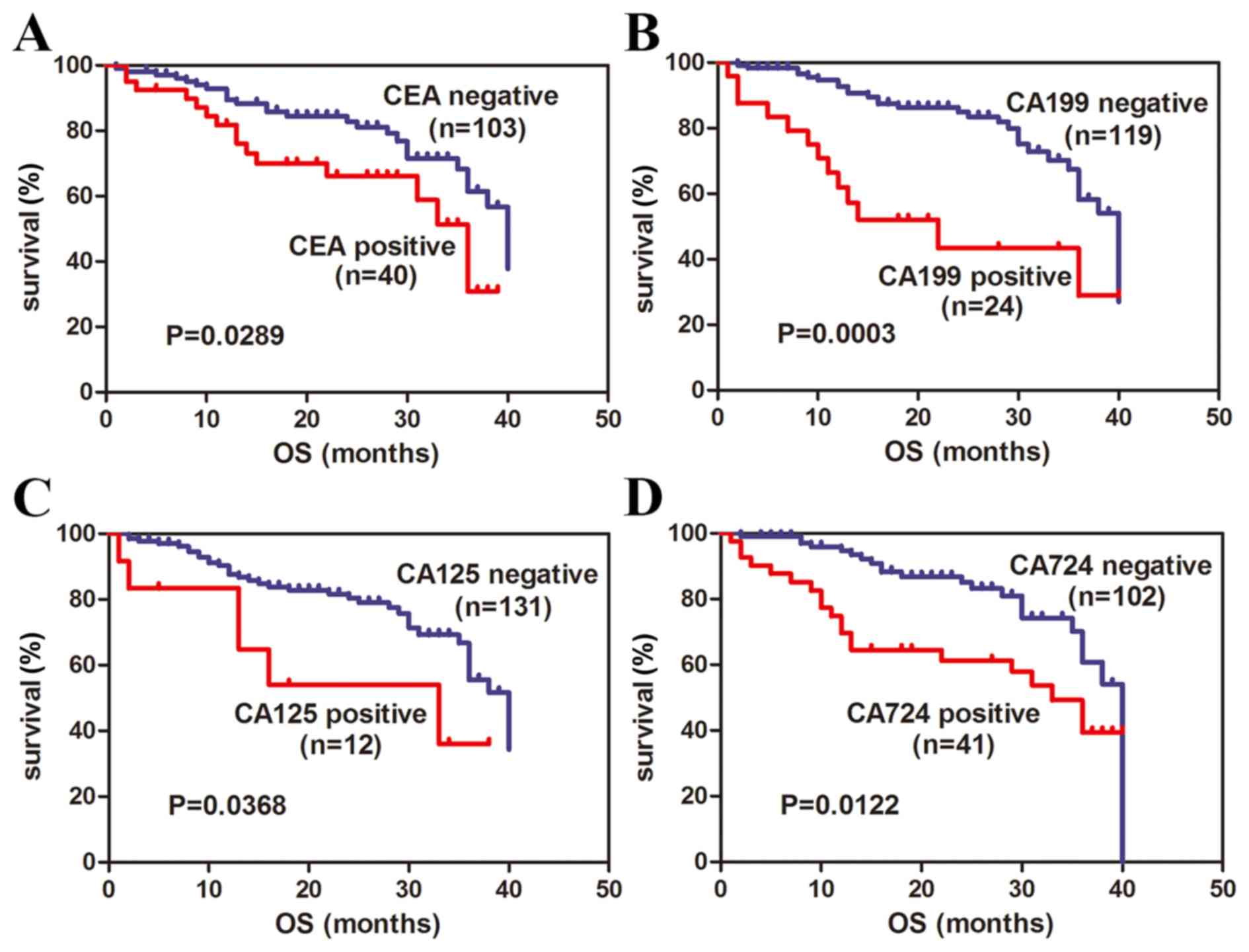
(P=0.0003; Fig. 3C). Then, we
reviewed the correlations of serum levels of CEA, CA199, CA125 and
CA724 with OS. Positive expression of CEA, CA199, CA125, CA 724
also showed significantly shorter OS in GC patients (P=0.0289;
Fig. 4A, P=0.0003; Fig. 4B, P=0.0122; Fig. 4C, P=0.0368; Fig. 4D, respectively). Taken as a whole,
these findings suggest that preoperative serum sMR and sCD163 may
be useful prognostic factors for GC.
Preoperative serum sMR and sCD163 were
adverse prognostic markers for GC patients
To further assess the impact of several clinical
variables on the OS of GC patients, we conducted univariate and
multivariate Cox regressions (Table
IV). Univariate analysis revealed that pathological grade
(P=0.013), clinical stage (P<0.001), CEA (P=0.034), CA199
(P<0.001), CA724 (P=0.027), sMR expression (P=0.006), and sCD163
expression (P<0.001) were all significantly associated with OS.
However, age, sex, tumor size and CA125 were not significant with
OS (P>0.05). Further multivariate analysis based on Cox
proportional hazards models demonstrated that only clinical stage
[hazard ratio (HR)=0.173, 95% confidence interval (95%
CI)=0.071–0.417, P<0.001] and CA199 (HR=0.412, 95%
CI=0.209–0.811, P=0.010) persisted as independent prognostic
factors. Our findings indicate that preoperative serum sMR and
sCD163 were adverse prognostic markers for GC patients.
| Table IV.Univariate and multivariate analyses
of various clinical variables in gastric cancer patients based on
OS |
Table IV.
Univariate and multivariate analyses
of various clinical variables in gastric cancer patients based on
OS
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Clinical
variables | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age (<60 vs. ≥60
years) | 1.100
(0.561–2.157) |
0.782 | 1.259
(0.604–2.625) |
0.540 |
| Sex (male vs.
female) | 1.611
(0.854–3.040) |
0.141 | 0.681
(0.337–1.377) |
0.258 |
| Tumor size (≤5 vs.
>5 cm) | 0.621
(0.333–1.158) |
0.134 | 0.690
(0.336–1.300) |
0.251 |
| Grade (G1+G2 vs.
G3) | 2.420
(1.205–4.857) |
0.013 | 0.651
(0.299–1.267) |
0.243 |
| Clinical stage
(I+II vs. III+IV) | 6.771
(2.833–16.18) | <0.001 | 0.173
(0.071–0.417) | <0.001 |
| CEA (N vs. P) | 0.503
(0.266–0.948) |
0.034 | 1.144
(0.544–2.405) |
0.723 |
| CA199 (N vs.
P) | 3.297
(1.694–6.419) | <0.001 | 0.412
(0.209–0.811) |
0.010 |
| CA125 (N vs.
P) | 1.976
(0.772–5.060) |
0.156 | 0.853
(0.308–2.364) |
0.760 |
| CA724 (N vs.
P) | 2.013
(1.081–3.748) |
0.027 | 0.601
(0.321–1.125) |
0.112 |
| sMR (low vs.
high) | 2.803
(1.335–5.886) |
0.006 | 0.604
(0.273–1.336) |
0.213 |
| sCD163 (low vs.
high) | 3.759
(1.827–7.734) | <0.001 | 0.667
(0.280–1.584) |
0.359 |
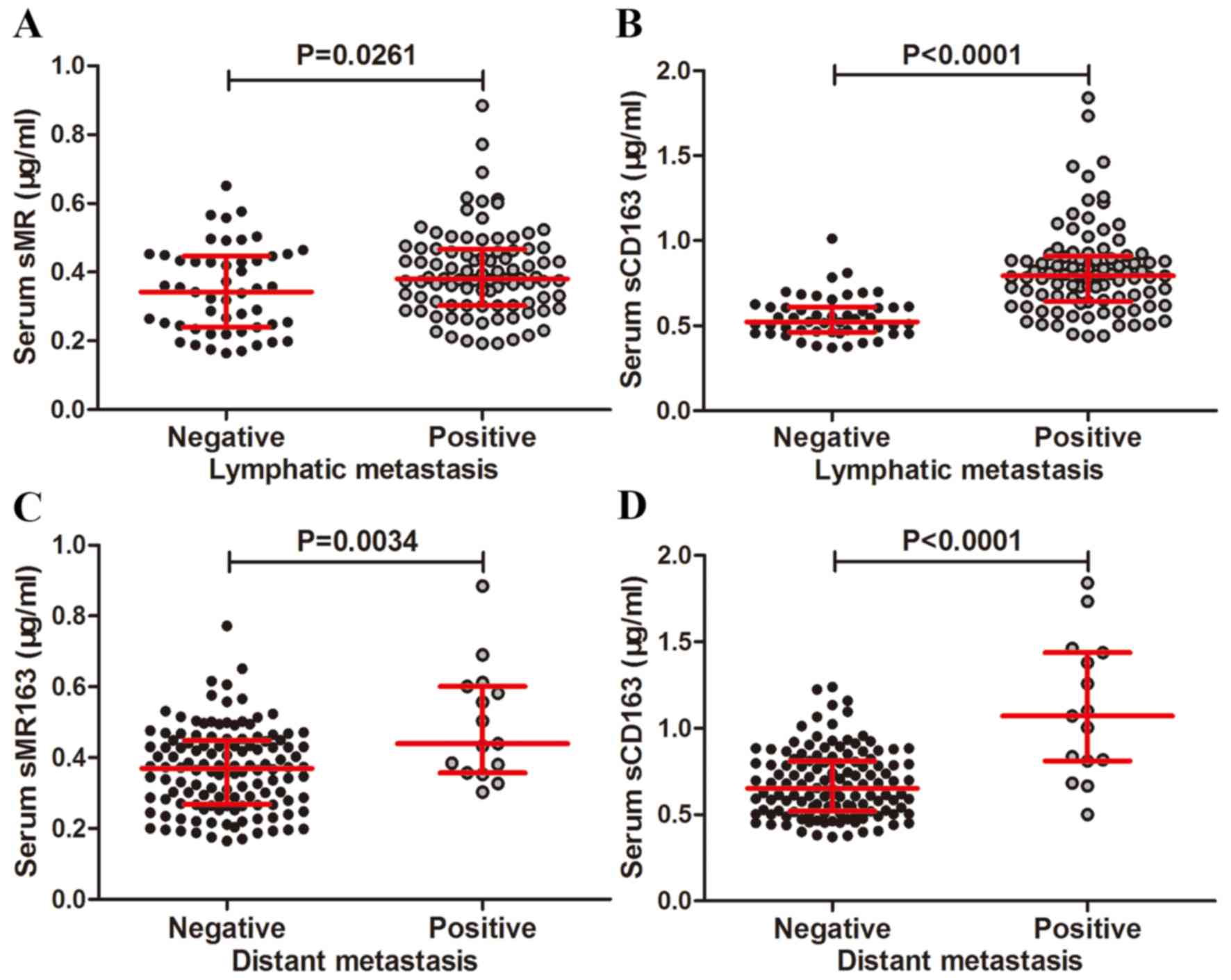
Preoperative serum sMR and sCD163 may
be important factors facilitated lymphatic and distant metastasis
of GC
In order to evaluate the associations of
preoperative serum sMR and sCD163 levels with lymphatic or distant
metastasis in GC, we compared preoperative serum sMR and sCD163
expression in lymphatic or distant metastasis cohort with
non-lymphatic or distant metastasis cohort. The sMR expression in
the lymphatic metastasis cohort was increased relative to the
non-lymphatic metastasis cohort (P=0.0261, Fig. 5A). Similar results was obtained for
sCD163 expression (P<0.0001, Fig.
5B). Serum sMR level in the distant metastasis cohort was
increased compared to the non-distant metastasis cohort (P=0.0034,
Fig. 5C) and the similar results was
obtained for sCD163 expression in the distant metastasis cohort
than in non-distant metastasis cohort (P<0.0001, Fig. 5D).
Discussion
The current study investigated the potential utility
of preoperative serum sMR and sCD163 in the diagnosis and prognosis
of GC. Preoperative serum sMR and sCD163 levels were significantly
increased and appeared to be highly prognostic of survival in GC
patients. Both sMR and sCD163 correlated remarkably with major
clinical variables, especially with CEA, CA199, CA125, and CA724.
High expression of preoperative serum sMR and sCD163 were
associated with high risks of lymphatic and distant metastasis as
well as unfavorable prognosis. These interesting results indicate
that serum sMR and sCD163 may be novel biomarkers for GC.
In the present study, in agreement with the results
of accepted GC markers, such as CEA, CA199, CA125, and CA724,
increased serum sMR and sCD163 levels were demonstrated.
Unfortunately, the mechanisms that affect the serum levels of sMR
and sCD163 in patients with GC remain elusive. Macrophages are
widely recognized as mediator for several physiological processes,
such as chronic inflammatory reaction and immune response, as well
as facilitator for cancer invasion, migration and metastasis. The
hemoglobin scavenger receptor CD163, a membranin acting as specific
macrophage activation marker, is commonly upregulated by the
stimulation of interleukin-6 (IL-6), interleukin-10 (IL-10),
glucocorticoid, and macrophage colony-stimulating factor (13). Inflammatory stimulation, cooperation
with the participation of lipopolysaccharide (LPS), metalloprotease
and inflammatory medium, and activation of Toll-like receptors,
could collectively attribute to the shedding of CD163 from surface
membrane and subsequently appear in serum as a soluble form
(19). The expression of serum sCD163
is justifiably considered as a reflection of the degree of
inflammatory response. There has a certain similarity between the
biological behavior of anti-inflammation and anticancer immunity.
Thus, increased serum sCD163 in GC patients may be partially
ascribed to the response of anti cancer immunity. MR, co-expression
on macrophages with CD163, may experience similar mechanism of
shedding in the process of anticancer immunity and subsequently
regulates the serum levels of soluble pattern. Additionally, MR and
CD163 expression on cancer focus may also affect their
corresponding soluble form which needs further study to verify in
detail.
Then, we investigated the potential of preoperative
serum sMR and sCD163 to discriminate GC patients from non-GC
controls and compared the diagnostic ability of them with
traditional GC markers. For single detection, serum sMR and sCD163
all exhibited medium diagnostic accuracy. Notably, the diagnostic
ability was remarkably enhanced when they combined. Preoperative
serum CEA, with similar sensitivity to CA724, is generally greater
than serum CA199 in GC prediction (20). The positive rate of serum CA125 in GC
patients is relatively low. However, as a predictor of peritoneal
dissemination of GC, serum CA125 is more ideal than CEA or CA199
(21,22). In present study, diagnostic power was
decreased from CA724, CEA, CA199 to CA125 in order which was
consistent with paper recently reported (23). Then, the predictive potential of
sCD163 is greater than CA724, whereas sMR is less than CA724.
Combined detection of several tumor markers which are complementary
with each other is regard as an efficient way to improve diagnostic
value (24). Strikingly, the
predictive power of serum sMR and sCD163 in combination is
apparently better than any kinds of combination of CEA, CA199,
CA125 and CA724 in this study. Therefore, it might be assumed that
preoperative serum serum sMR and sCD163 are novel GC detective
markers which are superior to traditional markers.
Traditionally, serum levels of CEA, CA199, CA125,
together with CA724 are common worse prognostic factors for GC
(24,25). In our study, similar results were
obtained. Recently, serum sMR and sCD163 were determined as adverse
prognostic factors in several malignancies (15,16). In
agreement with these interesting finding, the increased expression
of serum sMR and sCD163 in GC correlated significantly with shorter
OS and were identified as adverse prognostic markers in univariate
analyses based on Cox proportional hazards models. Meanwhile,
clinical stage, CEA, CA199, and CA724 were simultaneously verified
as prognostic factors for GC as previously mentioned (26). As adverse prognostic markers, the
molecular pathways of MR and CD163 to promote occurrence and
development of cancers are absent. Therefore, further studies are
needed to make some exploration.
In present study, the increased expression of
preoperative serum sMR and sCD163 were displayed dramatically
positive correlations with lymphatic and distant metastasis in GC
patients. Early lymphatic metastasis of GC to regional lymph nodes
is a highly critical event linked with further distant metastasis
as well as inferior prognosis (27).
Therefore, we speculate that elevated serum levels of sMR and
sCD163 correlated with shorter survival may be attributed to
participation in GC metastasis. MR expressed on lymphatic
endothelial cells mediates the adhesion of tumor cells to lymphatic
endothelium which contribute to the pivotal step for lymphatic
metastasis. Certainly, MR is identified as a facilitator for
lymphatic spread of many cancers in vitro and in vivo
(6,28). Regardless of lacking of relationship
between CD163 and GC lymphatic metastasis, the interesting results
of this study inspire us to explore the important role of MR and
CD163 in GC metastasis in further study.
In conclusion, this is the first study to report sMR
and sCD163 as valuable biomarkers for diagnosis and prognosis of
GC. Further studies are needed to explore the molecular mechanisms
of sMR and sCD163 in the development and progression of GC in
vivo and in vitro.
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2015. CA Cancer J Clin. 65:5–29. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Zhou M, Wang H, Zhu J, Chen W, Wang L, Liu
S, Li Y, Wang L, Liu Y, Yin P, et al: Cause-specific mortality for
240 causes in China during 1990–2013: A systematic subnational
analysis for the global burden of disease study 2013. Lancet.
387:251–272. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Cohen DJ and Leichman L: Controversies in
the treatment of local and locally advanced gastric and esophageal
cancers. J Clin Oncol. 33:1754–1759. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hu Y, Fang JY and Xiao SD: Can the
incidence of gastric cancer be reduced in the new century? J Dig
Dis. 14:11–15. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Martinez-Pomares L: The mannose receptor.
J Leukoc Biol. 92:1177–1186. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Irjala H, Alanen K, Grénman R, Heikkilä P,
Joensuu H and Jalkanen S: Mannose receptor (MR) and common
lymphatic endothelial and vascular endothelial receptor (CLEVER)-1
direct the binding of cancer cells to the lymph vessel endothelium.
Cancer Res. 63:4671–4676. 2003.PubMed/NCBI
|
|
7
|
Rødgaard-Hansen S, Rafique A, Christensen
PA, Maniecki MB, Sandahl TD, Nexø E and Møller HJ: A soluble form
of the macrophage-related mannose receptor (MR/CD206) is present in
human serum and elevated in critical illness. Clin Chem Lab Med.
52:453–461. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rødgaard-Hansen S, Rafique A, Weis N,
Wejse C, Nielsen H, Pedersen SS, Møller HJ and Kronborg G:
Increased concentrations of the soluble mannose receptor in serum
from patients with pneumococcal bacteraemia, and prediction of
survival. Infect Dis (Lond). 47:203–208. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kjærgaard AG, Rødgaard-Hansen S, Dige A,
Krog J, Møller HJ and Tønnesen E: Monocyte expression and soluble
levels of the haemoglobin receptor (CD163/sCD163) and the mannose
receptor (MR/sMR) in septic and critically ill non-septic ICU
patients. PLoS One. 9:e923312014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Andersen MN, Andersen NF, Rødgaard-Hansen
S, Hokland M, Abildgaard N and Møller HJ: The novel biomarker of
alternative macrophage activation, soluble mannose receptor
(sMR/sCD206): Implications in multiple myeloma. Leuk Res.
39:971–975. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kristiansen M, Graversen JH, Jacobsen C,
Sonne O, Hoffman HJ, Law SK and Moestrup SK: Identification of the
haemoglobin scavenger receptor. Nature. 409:198–201. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Edge SB and Compton CC: The American joint
committee on cancer: the 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Møller HJ, Peterslund NA, Graversen JH and
Moestrup SK: Identification of the hemoglobin scavenger
receptor/CD163 as a natural soluble protein in plasma. Blood.
99:378–380. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Karrasch T, Brünnler T, Hamer OW, Schmid
K, Voelk M, Herfarth H and Buechler C: Soluble CD163 is increased
in patients with acute pancreatitis independent of disease
severity. Exp Mol Pathol. 99:236–239. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kazankov K, Rode A, Simonsen K, Villadsen
GE, Nicoll A, Møller HJ, Lim L, Angus P, Kronborg I, Arachchi N, et
al: Macrophage activation marker soluble CD163 may predict disease
progression in hepatocellular carcinoma. Scand J Clin Lab Invest.
76:64–73. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
No JH, Moon JM, Kim K and Kim YB:
Prognostic significance of serum soluble CD163 level in patients
with epithelial ovarian cancer. Gynecol Obstet Invest. 75:263–267.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nederby L, Roug AS, Knudsen SS, Skovbo A,
Kjeldsen E, Moller HJ and Hokland M: Soluble CD163 as a prognostic
biomarker in B-cell chronic lymphocytic leukemia. Leuk Lymphoma.
56:3219–3221. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Andersen MN, Abildgaard N, Maniecki MB,
Møller HJ and Andersen NF: Monocyte/macrophage-derived soluble
CD163: A novel biomarker in multiple myeloma. Eur J Haematol.
93:41–47. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Weaver LK, Pioli PA, Wardwell K, Vogel SN
and Guyre PM: Up-regulation of human monocyte CD163 upon activation
of cell-surface Toll-like receptors. J Leukoc Biol. 81:663–671.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yang AP, Liu J, Lei HY, Zhang QW, Zhao L
and Yang GH: CA72-4 combined with CEA, CA125 and CA19-9 improves
the sensitivity for the early diagnosis of gastric cancer. Clin
Chim Acta. 437:183–186. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Nakata B, Hirakawa-YS Chung K, Kato Y,
Yamashita Y, Maeda K, Onoda N, Sawada T and Sowa M: Serum CA125
level as a predictor of peritoneal dissemination in patients with
gastric carcinoma. Cancer. 83:2488–2492. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Emoto S, Ishigami H, Yamashita H,
Yamaguchi H, Kaisaki S and Kitayama J: Clinical significance of
CA125 and CA72-4 in gastric cancer with peritoneal dissemination.
Gastric Cancer. 15:154–161. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Liang Y, Wang W, Fang C, Raj SS, Hu WM, Li
QW and Zhou ZW: Clinical significance and diagnostic value of serum
CEA, CA19-9 and CA72-4 in patients with gastric cancer. Oncotarget.
7:49565–49573. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Liu X, Qiu H, Liu J, Chen S, Xu D, Li W,
Zhan Y, Li Y, Chen Y, Zhou Z and Sun X: Combined preoperative
concentrations of CEA, CA 19-9, and 72-4 for predicting outcomes in
patients with gastric cancer after curative resection. Oncotarget.
7:35446–35453. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sun Z and Zhang N: Clinical evaluation of
CEA, CA19-9, CA72-4 and CA125 in gastric cancer patients with
neoadjuvant chemotherapy. World J Surg Oncol. 12:3972014.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kwon OK, Yu W and Chung H: Prognostic
value of postoperative CA19-9 normalization in patients with
advanced gastric cancer. Hepatogastroenterology. 60:240–243.
2013.PubMed/NCBI
|
|
27
|
Shida A, Mitsumori N, Nimura H, Takano Y,
Iwasaki T, Fujisaki M, Takahashi N and Yanaga K: Prediction of
lymph node metastasis and sentinel node navigation surgery for
patients with early-stage gastric cancer. Word J Gastroenterol.
22:7431–7439. 2016. View Article : Google Scholar
|
|
28
|
Marttila-Ichihara F, Turja R, Miiluniemi
M, Karikoski M, Maksimow M, Niemelä J, Martinez-Pomares L, Salmi M
and Jalkanen S: Macrophage mannose receptor on lymphatics controls
cell trafficking. Blood. 112:64–72. 2008. View Article : Google Scholar : PubMed/NCBI
|