Introduction
Lung cancer is the primary cause of
cancer-associated mortality (1,2) and may be
classified as non-small cell lung cancer (NSCLC) or small cell lung
cancer. NSCLC accounts for ~85% of all lung cancer cases, of which
two-thirds are diagnosed as advanced disease that is not
susceptible to therapy and confers a poor prognosis (1). Chemotherapy based on platinum-containing
doublets appears to have reached a therapeutic plateau in lung
cancer, with median survival times on those receiving this therapy
approaching 12 months (2). The
development of more effective first-line therapies remains a
challenge (2–4).
The results of previous randomized studies suggest
that patients with advanced NSCLC with EGFR mutations have a
significantly improved progression-free survival (PFS) when treated
with EGFR tyrosine kinase inhibitors (TKIs) alone, compared with
standard chemotherapy. Conversely, in wild-type EGFR patients, EGFR
TKIs treatment was less effective when administered alone compared
with chemotherapy (5–11). In patients with lung cancer with
metastatic disease of the pleura, pleurodesis with talc has been
utilized as an integrated treatment option to inhibit the drainage
of pleural fluid and preserve lung function, improving the
patient's quality of life (12–15).
Radiotherapy is approved for the treatment of stage
IIIA and B lung cancer [as described by the American Joint
Committee on Cancer staging system, eighth edition (16)], and for stage IV lung cancer in
certain cases (1). Radical
radiotherapy for patients with NSCLC can be curative for the
minority of patients with early stage disease (17). In addition, when treatment is not
curative palliative radiotherapy can be used to aid in pain relief
(17,18).
The present study reports two cases of stage IV
NCLC, which highlight that a timely and integrated
multidisciplinary treatment strategy, including stereotactic
radiotherapy and talc pleurodesis, may lead to improved patient
survival and quality of life.
Case report
Patient 1
A male 69-year-old non-smoker was admitted to the
Department of Cardiovascular and Thoracic Disease in the Division
of Pulmonology at St. Andrew's Hospital (Rome, Italy) complaining
of exertional dyspnea, a cough and chest pain, in September 2012.
The patient had a family history of cancer and the primary
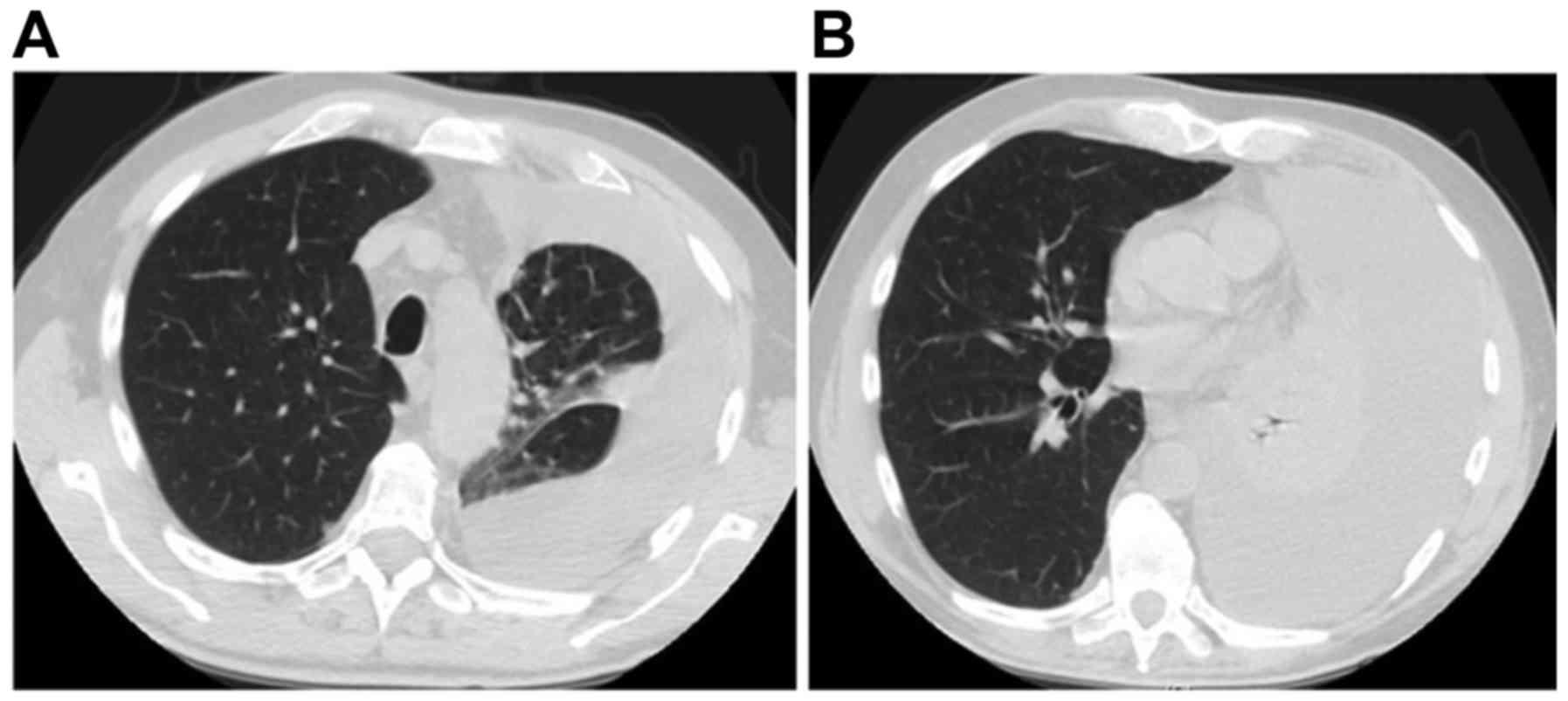
comorbidity was arterial hypertension. Following a chest X-ray,
high resolution computed tomography (CT) of the thorax was
performed (Fig. 1). This revealed a
large pleural effusion with pulmonary atelectasis and multiple
lymphadenopathies of the mediastinum. The patient subsequently
underwent three thoracentesis procedures, with a cytological
assessment of adenocarcinoma cells positive for transcription
termination factor 1 (TTF1), carcinoembryonic antigen and
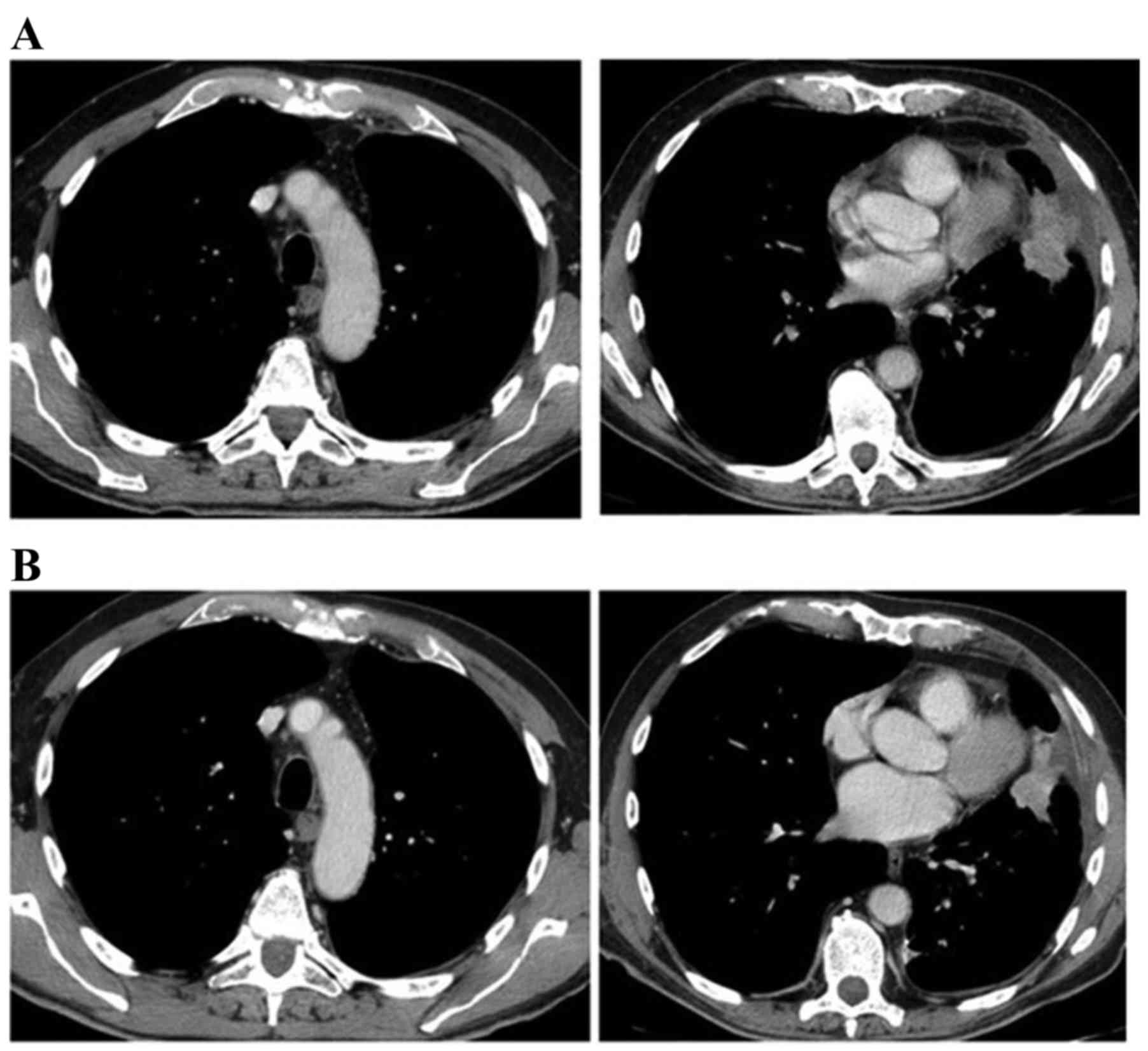
cytokeratin-7 (CK7), and negative for tumor protein p63. CT scans
demonstrated a re-expansion of the lung and a lesion in the left
lower lobe following enhancement with contrast medium injection
(Fig. 2A). Bronchoscopy with
transbronchial biopsies confirmed the diagnosis of lung
adenocarcinoma. Spirometry investigations of lung function
identified no significant flow limitation, with forced expiratory
volume in 1 sec and forced vital capacity measurements at >80%
of the predicted level. Hemogasanalysis reported a pH of 7.38,
partial pressure (Pa) of CO2 of 40 mmHg and PaO2 of 80
mmHg. A bone scan with radiolabeled technetium highlighted an
increased uptake of the compound in the seventh left rib as a
metastasis. The patient underwent thoracoscopy and talc pleurodesis
(using talc poudrage) in order to maintain integrity of lung
function and prevent further thoracentesis. CT confirmed the
success of the surgery and the pleural biopsies taken confirmed the
metastatic spread of the tumor to the pleura. Chemotherapy was
initiated; each cycle was 21 days. Chemotherapy included a
cisplatin dose of 70 mg/m2 on days 1 and 21 for 1 cycle,
gemcitabine 1,000 mg/m2 on days 1, 8 and 21 for 8 cycles, and
bevacizumab 7.5 mg/kg on days 1 and 21 for 4 cycles, resulting in a
partial tumor response (Fig. 2B).
Additionally, polymerase chain reaction screening of the pleural
biopsies identified a deletion of exon 19 of the EGFR gene.
Consequently, therapy with gefitinib (250 mg/day) was initiated,
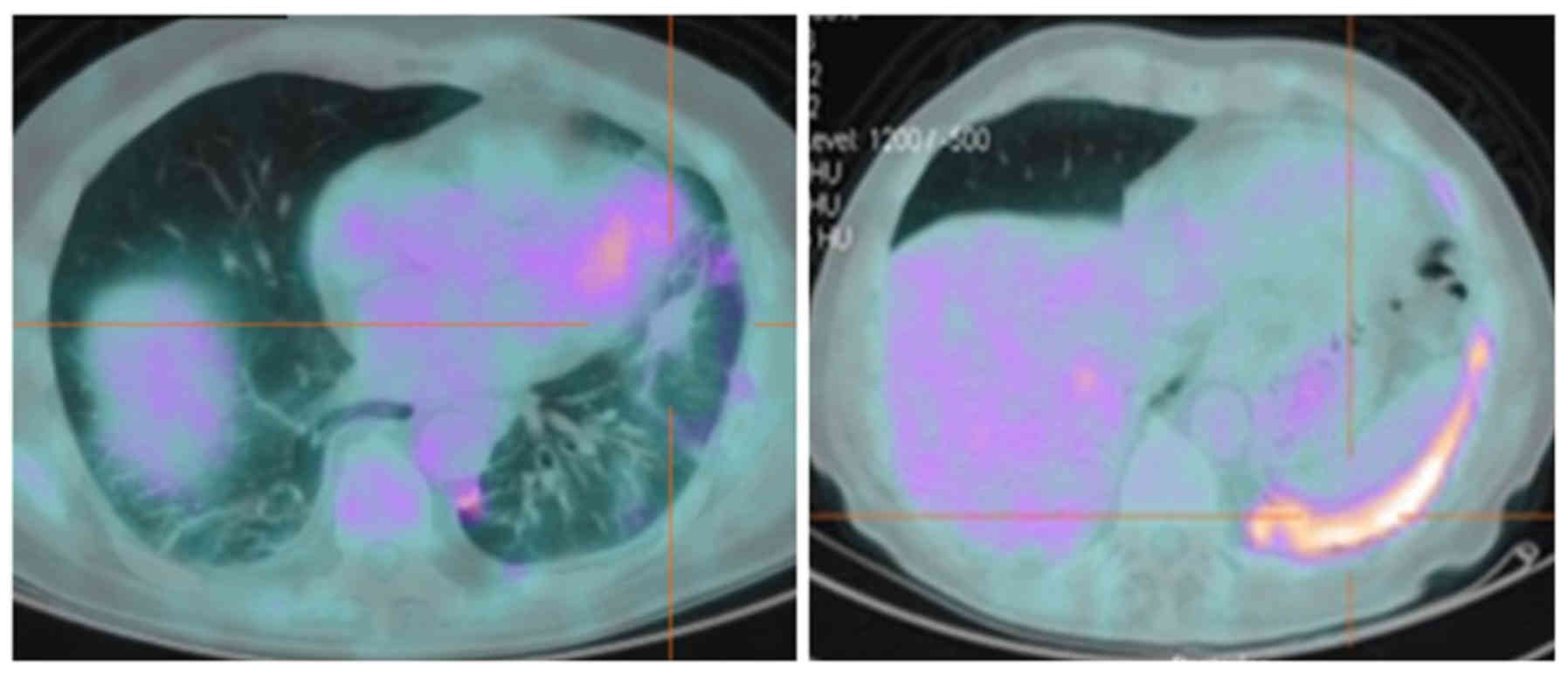
with a good response for 10 months; however, a further positron
emission tomography (PET)/CT scan identified a residual lesion
through fluorodeoxyglucose (18F-FDG) uptake. Stereotactic
radiotherapy with a total dose of 45 Gy divided into 3 fractions
was performed on the residual lesion over 3 days. A subsequent
PET/CT scan revealed residual inflammation and reduced metabolic
activity, with a standardized uptake value <3 (Fig. 3). The patient was alive 4 years
following diagnosis, exhibited good health and continued gefitinib
maintenance with a dose of 250 mg a day, now on the 40th cycle of
treatment.
Patient 2
A 52-year-old male ex-smoker with a history of 20
packs/year was admitted to St. Andrew's Hospital in October 2013,
complaining of persistent chest pain. The patient's clinical
history was negative for comorbidities. The patient received
paracetamol without great benefit, while blood counts indicated
only mild anemia (hemoglobin, 11.5 g/dl; normal range, 12–15 g/dl).
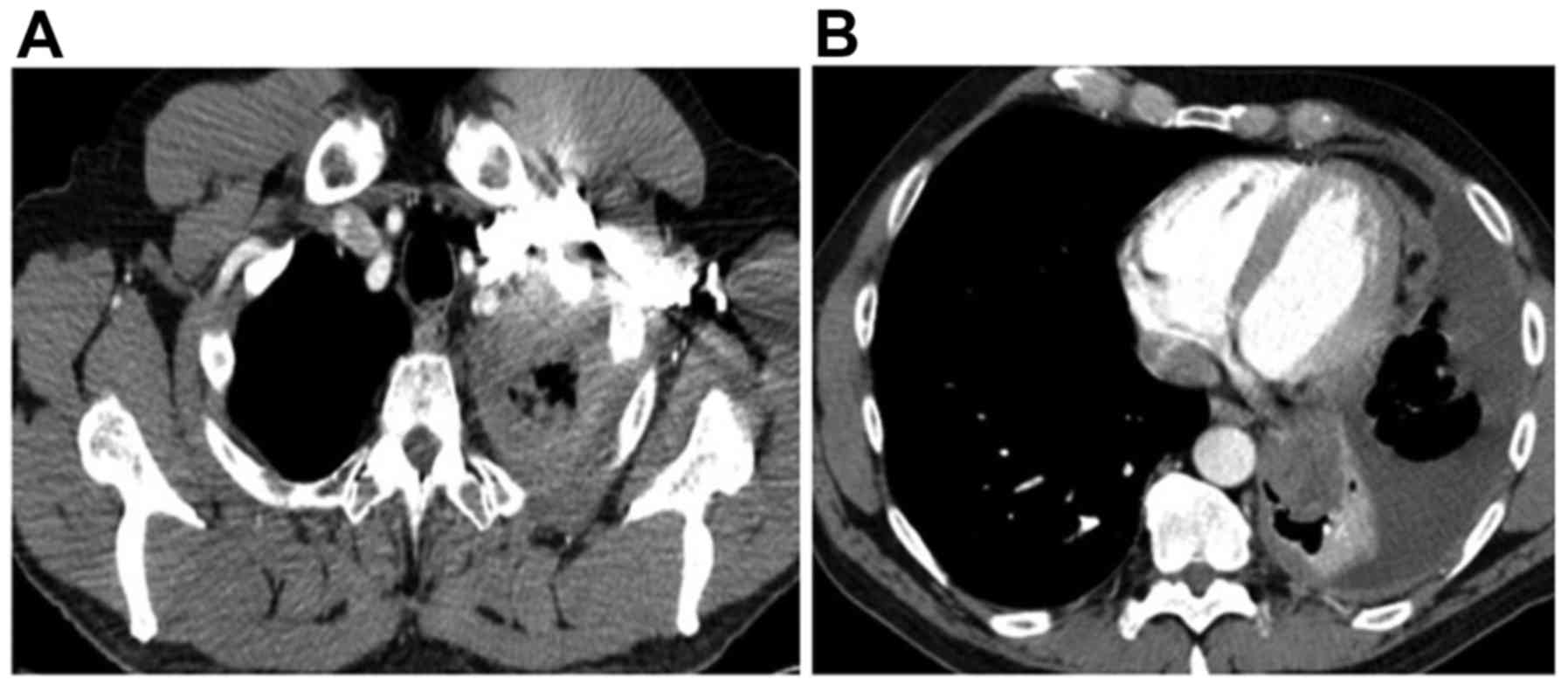
Following a chest X-ray that revealed a large mass on the left
lung, a total body CT scan revealed a mass of 48 mm in diameter
located in the left lower lobe of the lung with mediastinal
adenopathies and pleural effusions (Fig.
4A and B). Four thoracentesis procedures, video-assisted
thoracoscopy, several biopsies of pleural lesions and talc
pleurodesis were performed. A diagnosis of lung adenocarcinoma
(CK7+, TTF1+ and p63 negative) with a
deletion of exon 19 of the EGFR gene was made, based on the biopsy
specimen. Therapy with gefitinib (250 mg/day) was initiated,
continuing for ten months until further disease progression. A
total body CT scan 1 year from diagnosis revealed a partial
response to therapy, with a reduction in tumor mass of 50%
(Fig. 5A) according to the Response
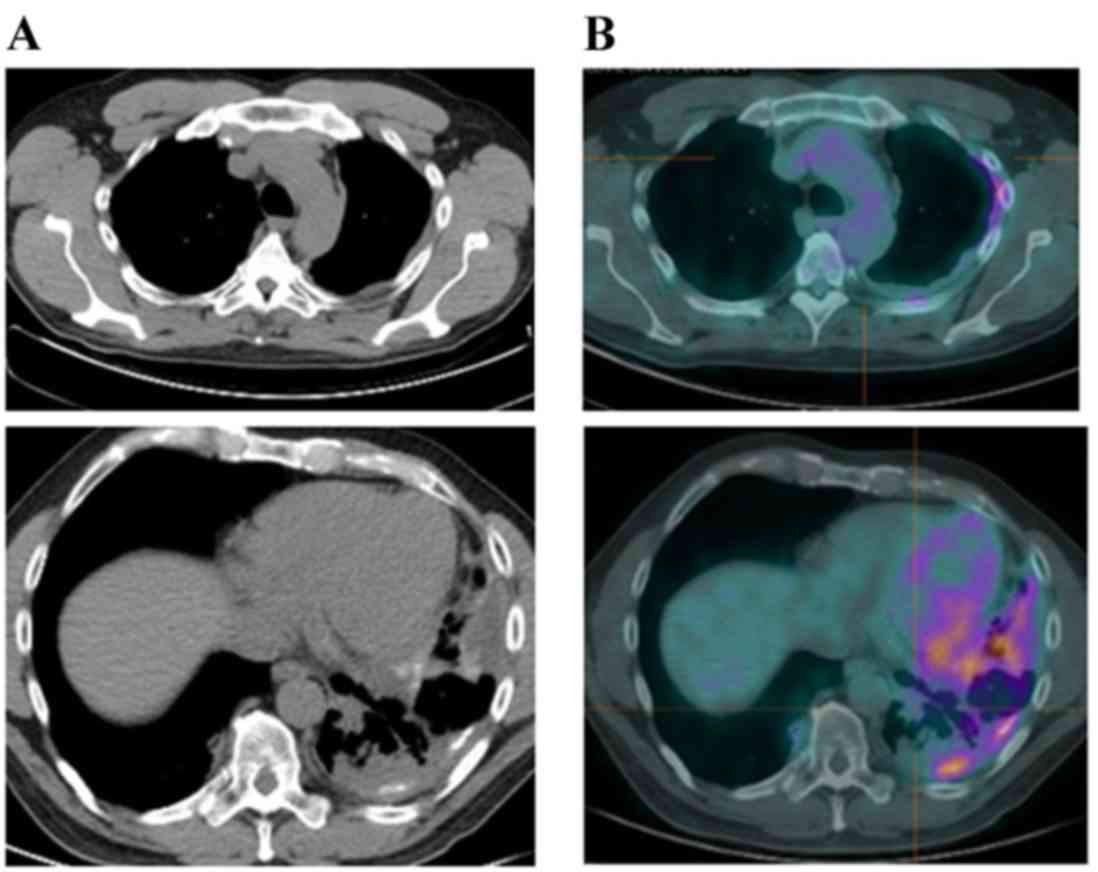
Evaluation Criteria In Solid Tumours version 1.1 (19). However, a 18F-FDG-PET scan 3 months
later (15 months following diagnosis) identified local progression
of the disease (Fig. 5B).
Radiotherapy in 20 fractions of 3 Gy each for a total of 60 Gy was
performed on the residual lesion over 3 weeks. The patient
tolerated the treatment well and continued gefitinib; however,
further progression of the disease was observed at 20 months after
diagnosis. At this point, cisplatin (60 mg/m2, d1) combined with
pemetrexed (500 mg/m2, d1) treatment was initiated for 4 cycles of
21 days. Premetrexed was continued as a maintenance treatment at a
dose of 500 mg/m2 (to date, 23 cycles). The patient was alive 3
years after diagnosis and did not complain of respiratory symptoms.
The patient's response to therapy was good and thoracic imaging
revealed only residual actinic fibrosis, without any sign of
disease.
Discussion
Lung cancer is the second most common cancer in
males and the third most common in females; however, it is the
primary cause of cancer-associated mortality. In the first three
stages of the disease, the various treatment options available
(surgery, chemotherapy, radiotherapy and biological therapy) are
frequently ineffective depending on the initial stage (1). Stage IV lung cancer confers a poor
prognosis, particularly when it co-occurs with pleural effusion
(14). In recent years, there have
been advancements in techniques that can preserve lung function,
such as talc pleurodesis (12). The
identification of genetic mutations associated with lung cancer
(EGFR, anaplastic lymphoma receptor tyrosine kinase and ROS
proto-oncogene 1 receptor tyrosine kinase) and the availability of
biological drugs that are less toxic, better tolerated and more
effective is improving the prognosis of patients with lung cancer,
at least in the short term (5–7). It is a
necessity that the therapeutic options available are known by the
patients, are the subject of interdisciplinary discussion and are
used appropriately.
The cases described in the present report were
characterized by a variability in response to different therapeutic
options and a relatively good survival time due to the use of all
possible treatments. Patient 1 and patient 2 received similar
treatment (standard chemotherapy and a biological EGFR-targeted
therapy) but exhibited different responses. EGFR-targeted therapy
has resulted in a better PFS of patients with NSCLC harboring an
activating mutation of EGFR compared with patients with wild-type
EGFR (3). The deletion of exon 19 and
the L858R mutation of exon 21 are the EGFR alterations that exhibit
the best sensitivity to EGFR-TKI treatment (9,10).
Patients with NSCLC in the East have been demonstrated to respond
better to this treatment compared with those in the West (5). A previous randomized phase III clinical
trial investigated the use of the EGFR-TKI gefitinib as a
first-line treatment for NSCLC compared with standard
platinum-based chemotherapy (6),
examining PFS and the overall response rate, achieving a median
survival time of 16 months. Gefitinib has been demonstrated to be
effective in the treatment of lung adenocarcinoma and
well-tolerated compared with standard chemotherapy (7). NSCLC cases with the deletion of exon 19
or L858R mutation of exon 21 of EGFR are highly responsive to
gefitinib (7,10). Erlotinib is another first generation
TKI and it has been demonstrated to be effective in phase III
studies as a first-line treatment in patients with EGFR
mutation-positive NSCLC (9). In
patients with NSCLC with wild-type EGFR, therapy with pemetrexed
combined with platinum-base compounds has been identified to
improve patient outcomes, such as PFS and overall survival (OS)
particularly as a maintenance treatment (3,4). In
addition, gefitinib maintenance therapy has been demonstrated to
further improve patient survival in a phase III clinical trial
(7,8,10).
Clinical guidelines indicate that the use of
pemetrexed and bevacizumab should be limited to patients with
non-squamous NSCLC histology (20).
Bevacizumab can also be used to control brain metastases. The use
of maintenance therapy should be considered after 4 cycles of
chemotherapy in patients with NSCLC who are responders or do not
exhibit disease progression (21).
The effect of therapy beyond the third line has not yet been
demonstrated. In regards to radiotherapy, guidelines suggest that
radiotherapy only be used in stage IV NSCLC for palliative
purposes. However, it is a feasible and effective treatment for
stage III NSCLC (1,17).
A previous study investigated the use of sequential
or concurrent radio-chemotherapy in unresectable lung cancer, which
was successful in improving progression free survival (16). In the cases discussed in the present
report, high-dose radiotherapy proved useful in boosting the
effects of the EGFR-TKI and to treat residual disease. Radiotherapy
could be either palliative or curative, depending on the stage at
the time of treatment (18).
Radiotherapy in elderly people has been demonstrated to provide
some benefit to patients with stage I as a curative treatment and
in patients with metastatic stage as palliative treatments to
improve the quality of life (17).
The presence of pleural effusion, a common
manifestation of NSCLC, worsens the prognosis of patients (12,13). The
management of pleural effusions is crucial for improving the
patient's quality of life and prognosis (12). Talc pleurodesis is a relatively new
method for treating recurrent pleural effusions and is less
invasive than other methods (12,14).
Pleurodesis can limit the spread of NSCLC and the development of
respiratory failure (15).
Pleurodesis by thoracoscopy can be performed in certain conditions,
including recurrent benign pleural effusion, recurrent pneumothorax
and malignant pleural effusion. In the majority of lung cancer
cases pleurodesis can slow the progression of the disease (12). The presence of a low glucose level and
of low pH fluid in NSCLC is associated with a poor prognosis
(13,15). Zimmer et al (12) compared talc slurry with other chemical
substances in a prospective randomized trial, demonstrating that
talc was the best agent for the treatment of malignant pleural
effusion.
In conclusion, a multidisciplinary approach
involving pneumologists, radiotherapists, oncologists and thoracic
surgeons, in addition to a variety of treatments, are required for
the management of lung cancer. The two patients described in the
present report were successfully treated using a range of agents.
This suggests that sequential therapies with different agents
provide clinical benefit while being well tolerated, improving PFS
and OS.
References
|
1
|
Ettinger DS, Wood DE, Akerley W, Bazhenova
LA, Borghaei H, Camidge DR, Cheney RT, Chirieac LR, D'Amico TA,
Demmy TL, et al: NCCN guidelines insights: Non-Small cell lung
cancer, version 4.2016. J Natl Compr Canc Netw. 14:255–264. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Molina JR, Yang P, Cassivi SD, Schild SE
and Adjei AA: Non-small cell lung cancer: Epidemiology, risk
factors, treatment, and survivorship. Mayo Clin Proc. 83:pp.
584–594. 2008; View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Xiao HQ, Tian RH, Zhang ZH, Du KQ and Ni
YM: Efficacy of pemetrexed plus platinum doublet chemotherapy as
first-line treatment for advanced nonsquamous non-small-cell-lung
cancer: A systematic review and meta-analysis. Onco Targets Ther.
9:1471–1476. 2016.PubMed/NCBI
|
|
4
|
Paz-Ares LG, de Marinis F, Dediu M, Thomas
M, Pujol JL, Bidoli P, Molinier O, Sahoo TP, Laack E, Reck M, et
al: PARAMOUNT: Final overall survival results of the phase III
study of maintenance pemetrexed versus placebo immediately after
induction treatment with pemetrexed plus cisplatin for advanced
nonsquamous non-small-cell lung cancer. J Clin Oncol. 31:2895–2902.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Li G, Gao S, Sheng Z and Li B: The
efficacy of single-agent epidermal growth factor receptor tyrosine
kinase inhibitor therapy in biologically selected patients with
non-small-cell lung cancer: A meta-analysis of 19 randomized
controlled trials. Chemotherapy. 61:179–189. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mitsudomi T, Morita S, Yatabe Y, Negoro S,
Okamoto I, Tsurutani J, Seto T, Satouchi M, Tada H, Hirashima T, et
al: Gefitinib versus cisplatin plus docetaxel in patients with
non-small-cell lung cancer harbouring mutations of the epidermal
growth factor receptor (WJTOG3405): An open label, randomised phase
3 trial. Lancet Oncol. 11:121–128. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Maemondo M, Inoue A, Kobayashi K, Sugawara
S, Oizumi S, Isobe H, Gemma A, Harada M, Yoshizawa H, Kinoshita I,
et al: Gefitinib or chemotherapy for non-small-cell lung cancer
with mutated EGFR. N Engl J Med. 362:2380–2388. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Paez JG, Jänne PA, Lee JC, Tracy S,
Greulich H, Gabriel S, Herman P, Kaye FJ, Lindeman N, Boggon TJ, et
al: EGFR mutations in lung cancer: Correlation with clinical
response to gefitinib therapy. Science. 304:1497–1500. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zhou C, Wu YL, Chen G, Feng J, Liu XQ,
Wang C, Zhang S, Wang J, Zhou S, Ren S, et al: Erlotinib versus
chemotherapy as first-line treatment for patients with advanced
EGFR mutation-positive non-small-cell lung cancer (OPTIMAL,
CTONG-0802): A multicentre, open-label, randomised, phase 3 study.
Lancet Oncol. 12:735–742. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mok TS, Wu YL, Thongprasert S, Yang CH,
Chu DT, Saijo N, Sunpaweravong P, Han B, Margono B, Ichinose Y, et
al: Gefitinib or carboplatin-paclitaxel in pulmonary
adenocarcinoma. N Engl J Med. 361:947–957. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yang JC, Sequist LV, Zhou C, Schuler M,
Geater SL, Mok T, Hu CP, Yamamoto N, Feng J, O'Byrne K, et al:
Effect of dose adjustment on the safety and efficacy of afatinib
for EGFR mutation-positive lung adenocarcinoma: Post hoc analyses
of the randomized LUX-Lung 3 and 6 trials. Ann Oncol. 27:2103–2110.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zimmer PW, Hill M, Casey K, Harvey E and
Low DE: Prospective randomized trial of talc slurry vs bleomycin in
pleurodesis for syntomatic malignant pleural effusions. Chest.
112:430–434. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Cox SE and Katlic MR: Non-intubated
video-assisted thoracic surgery as the modality of choice for
treatment of recurrent pleural effusions. Ann Transl Med.
3:1032015.PubMed/NCBI
|
|
14
|
Rodriguez-Panadero F, Janssen JP and
Astoul P: Thoracoscopy: General overview and place in the diagnosis
and management of pleural effusion. Eur Resp J. 28:409–422. 2006.
View Article : Google Scholar
|
|
15
|
Xia H, Wang XJ, Zhou Q, Shi HZ and Tong
ZH: Efficacy and safety of talc pleurodesis for malignant pleural
effusion: A meta-analysis. PLoS One. 9:e870602014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Rami-Porta R, Asamura H, Travis WD and
Rusch VW: Lung cancer-major changes in the American Joint Committee
on cancer eighth edition cancer staging manual. CA Cancer J Clin.
67:138–155. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Baker S, Dahele M, Lagerwaard F and Senan
S: A critical review of recent developments in radiotherapy for
non-small cell lung cancer. Radiat Oncol. 11:1152016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Dupic G and Bellière-Calandry A: Non-small
cell lung cancer irradiation in elderly. Cancer Radiother.
20:322–329. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zappa C and Mousa SA: Non-small cell lung
cancer: Current treatment and future advances. Transl Lung Cancer
Res. 5:288–300. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bearz A, Passalacqua R, Alabiso O, Cinieri
S, Gridelli C, Cravesana C and Crinò L: First-line
bevacizumab-based therapy in advanced non-squamous non-small-cell
lung cancer: Analysis of the Italian patients enrolled in the SAiL
study. Clin Drug Investig. 32:755–760. 2012. View Article : Google Scholar : PubMed/NCBI
|