Introduction
Hepatitis B virus (HBV) reactivation and hepatitis
flares are well-recognized complications that occur in cancer
patients who have undergone cytotoxic chemotherapy. HBV
reactivation (HBV-R) is most often reported in patients with
haematologic malignancies, particularly patients with lymphoma who
have been treated with rituximab. The incidence of HBV-R has been
reported to range from 4.1 to 23.8%, even in lymphoma patients with
resolved HBV infection, who, from a clinical standpoint, are
considered to have recovered from HBV infection (1–5). The
clinical spectrum of HBV-R in this population varies from
self-limited or asymptomatic hepatitis to fulminant hepatitis.
HBV-R occasionally leads to hepatitis-related death (4). In particular, the combination regimen of
rituximab and cytotoxic chemotherapy, which is the standard regimen
for patients with diffuse large B-cell lymphoma and follicular
lymphoma, has been found to increase the risk of HBV-R and
hepatitis flares in patients with resolved HBV infection (3,6).
In addition to rituximab use, other potential
factors, including advanced age and male sex, have been reported to
be associated with HBV-R (3,7,8). Recently,
a relationship between antibodies to hepatitis B surface antigen
(anti-HBs) and HBV-R was reported. However, to our knowledge, no
important pre-therapy predictive markers of HBV-R timing and
development have been reported. Thus, it remains unclear how HBV-R
may be identified prior to chemotherapy in lymphoma patients with
resolved HBV infection. Additionally, there are limited clinical
data on patients with resolved HBV infection, and there is no
established standard surveillance method for monitoring patients
with resolved HBV to prevent HBV-R.
Several reports have demonstrated the importance of
monitoring of HBV DNA to detect HBV-R occurrence in patients with
resolved HBV infection. These reports have indicated that such
patients should be closely monitored with HBV DNA and serum
biochemistry studies for at least 6 months after completion of
therapy and that antivirals should be administered promptly upon
detection of reactivation (9,10). However, no previous studies of cancer
patients with resolved HBV infection were able to devise unified
methods of diagnosing HBV-R, nor were these studies able to
determine appropriate follow-up intervals for monitoring patients
with different tumour types who were receiving chemotherapy
regimens of different intensities during and after chemotherapy.
Generally, the incidence of HBV-R in outpatients is low (11), and HBV monitoring is expensive.
Additionally, clinical evidence alone is insufficient for
determining the optimal frequency and duration of HBV DNA
monitoring during and after chemotherapy.
Therefore, this retrospective study sought to
clarify the predictive factors for chemotherapy-induced HBV-R in
lymphoma patients with resolved HBV infection who were undergoing
standard chemotherapy.
Materials and methods
Patients
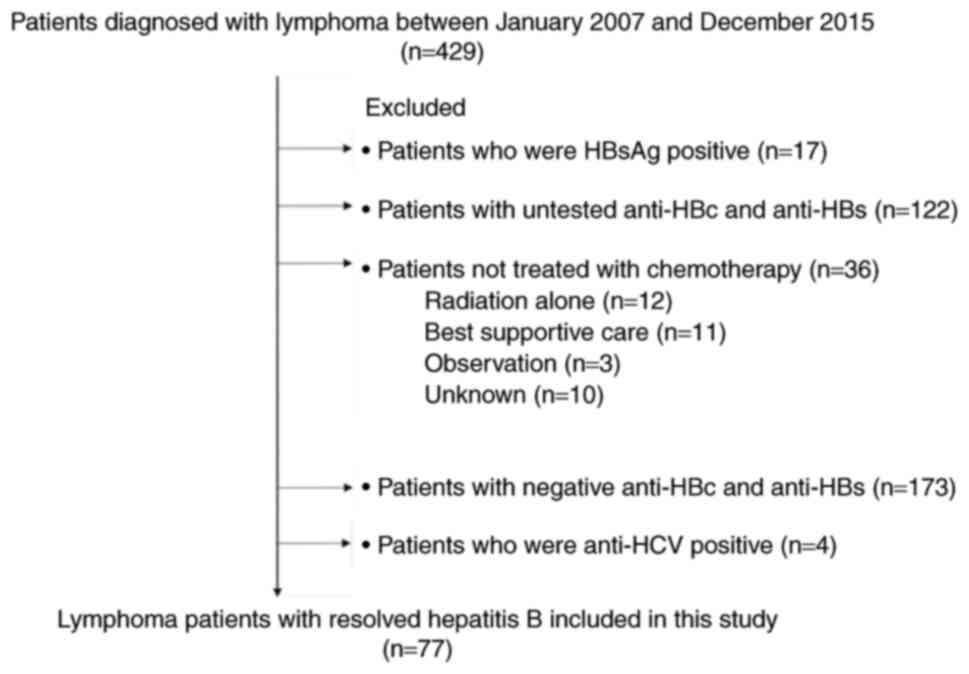
This was a single-centre retrospective study. A
total of four hundred twenty-nine consecutive patients with newly
diagnosed, histologically proven lymphoma who were treated at
Toyonaka Municipal Hospital from January 2007 to December 2015 were
enrolled in the study. Of these 429 patients, 393 patients
underwent chemotherapy. The remaining 36 patients did not undergo
chemotherapy due to poor performance status or because they
received another form of treatment for their disease. Regarding HBV
serological markers, 17 patients were positive for hepatitis B
surface antigen (HBsAg) (4.0%), and 412 patients were negative for
HBsAg (96.0%). Of the HBsAg-negative patients, 173 were negative
for both antibodies to hepatitis B core antigen (anti-HBc) and
anti-HBs, and 122 (28%) were untested for anti-HBc and/or anti-HBs
because we did not always check for these markers prior to the
publication and introduction into practice of the Hepatitis B
Treatment Guidelines of the Japan Society of Hepatology in 2011
(12). Four patients were positive
for antibodies against hepatitis C virus. Resolved hepatitis B was
defined as HBsAg seronegativity and anti-HBs seropositivity and/or
having anti-HBc, but 6 patients with anti-HBs seropositivity and
anti-HBc seronegativity had not been previously vaccinated against
HBV. Fifty-five patients (71%) enrolled in this study were tested
for HBV DNA prior to chemotherapy, and they were negative; however,
the other patients were not tested. We excluded 352 patients;
therefore, a total of 77 patients (17.9%) with resolved hepatitis B
who received chemotherapy were ultimately analysed in the study
(Fig. 1). This study conformed to the
Declaration of Helsinki and local legislation and was approved by
the Ethics Committee of Toyonaka Municipal Hospital in 2015.
HBV-related marker measurements
Serum HBV viral loads were quantified using reverse
transcription- quantitative polymerase chain reaction
(TaqMan® HBV Test; Roche Diagnostics Japan, Tokyo,
Japan), with a minimal sensitivity of 2.1 log copies/ml, and all
serum HBsAg, anti-HBc and anti-HBs levels were evaluated using the
same commercially available enzyme immunoassays with minimum
sensitivities of 0.05 IU/ml, 1 S/CO and 10 mIU/ml, respectively,
via CLIA (ArchitectR; Abbott Japan, Chiba, Japan). The
intra-assay and total (inter- and intra-assay) variation (%
coefficient of variation) of anti-HBc levels in this study were
evaluated and reported as 2.5 to 6.5% and 2.8 to 7.5%, respectively
(Architect®; Abbott Japan; www.ilexmedical.com/files/PDF/AntiHBc_ARC.pdf).
Additionally, anti-HBc and anti-HBs levels were measured only prior
to treatment according to the guidelines (12).
Definitions of hepatitis flare and HBV
reactivation
HBV reactivation (HBV-R) was defined according to
the Hepatitis B Treatment Guidelines of the Japan Society of
Hepatology (12), and HBV-R was
defined as a detectable elevated HBV viral load or as HBsAg
reverse-seroconversion in patients with resolved hepatitis B during
or after chemotherapy. Hepatitis flare was defined as a 3-fold or
greater increase in alanine aminotransferase (ALT) to a level
exceeding the upper limit of normal (ULN) (40 U/l) in patients with
HBV-R. As previously reported, delayed HBV-R was defined as HBV-R
more than 3 months after completing chemotherapy (1,7).
Chemotherapy for lymphoma and
treatment for HBV-R
Lymphoma treatment was based on the guidelines of
the Japan Society of Hematology. The details of the chemotherapy
regimens are presented in Table I.
Patients with resolved HBV infection who experienced HBV-R were
orally administered 0.5–1 mg of entecavir daily.
 | Table I.Baseline characteristics of lymphoma
patients with resolved HBV infection who were treated with
chemotherapy. |
Table I.
Baseline characteristics of lymphoma
patients with resolved HBV infection who were treated with
chemotherapy.
|
Characteristics | Number of patients
(n=77) |
|---|
| Age, years | 75
(47–89) |
| Sex, male | 46 (59.7) |
| Haematologic
diagnosis |
|
| Diffuse
large B cell lymphoma | 53 (68.8) |
|
Follicular lymphoma | 9
(11.7) |
|
Mantle-cell lymphoma | 4 (5.2) |
|
Angioimmunoblastic T-cell
lymphoma | 3 (3.9) |
| MALT
lymphoma | 2 (2.6) |
| Burkitt
lymphoma | 1 (1.3) |
|
Lymphoplasmacytic
lymphoma | 1 (1.3) |
|
Other | 4 (5.2) |
| Viral serology |
|
|
Anti-HBc seropositive | 71 (92.2) |
|
Anti-HBs seropositive | 58 (75.3) |
| Blood biochemical
findings |
|
|
Baseline ALT, U/l | 17.5±8.5 |
|
Baseline albumin, g/l | 3.3±0.8 |
|
Baseline total bilirubin,
mg/dl | 0.8±0.5 |
| Treatment
regimens |
|
|
Rituximab-containing
chemotherapya | 68 (88.3) |
|
CHOP-based
chemotherapyb | 6 (7.8) |
|
Otherc | 3 (3.9) |
| Duration of
follow-up, days | 987
(7–2769) |
Outcomes and follow-up
The primary endpoint was the incidence of HBV-R
during or after chemotherapy in lymphoma patients with resolved
HBV. Time to HBV-R was calculated as the elapsed time from the day
of chemotherapy initiation to the day of HBV-R detection. Delayed
HBV-R was defined as HBV-R more than 3 months after completing
chemotherapy. All enrolled patients were evaluated at least once
every chemotherapy cycle and underwent liver function and HBV viral
load testing every one to three months. After the patients
completed chemotherapy, their HBV viral loads were followed for at
least for 12 months. The follow-up observation period was measured
from the day of chemotherapy initiation to the date of the last
visit or the date of death during the study period.
Statistical analysis
Correlations between two groups were assessed via
Pearson's analysis, and multiple comparisons among more than two
groups were assessed via the Kruskal-Wallis non-parametric test.
HBV reactivation-free survival rates in patients with lymphoma who
underwent chemotherapy were estimated by the Kaplan-Meier method,
and the log-rank test was used for comparisons. Receiver operating
characteristic (ROC) curve analysis was used to determine the
anti-HBc and anti-HBs cut-off titres for predicting HBV-R. The
other predicting factors, namely, serum ALT levels, albumin levels,
prothrombin times (%), total bilirubin levels and age, were each
divided into two categories based on their median values.
Univariate and multivariate analyses of the factors associated with
HBV-R were performed using logistic regression analysis, and
factors with P-values <0.05 in the univariate analysis were
considered in the multivariate model. All statistical analyses were
performed using the JMP Pro 11 statistical software package
(version 11.2.1, SAS, Cary, NC, USA). All the tests were
two-tailed, and P<0.05 was considered to indicate a
statistically significant difference.
Results
Patients (baseline
characteristics)
Baseline patient clinical characteristics are
presented in Table I. The median age
of the study population was 75 years (range, 47–89), and diffuse
large B-cell lymphoma (DLBCL) was the most common type of lymphoma
(n=53, 68.8%) in the study population. Regarding chemotherapy
regimen, 68 patients (88.3%) received rituximab-containing
chemotherapy. The median length of the follow-up observation period
during the study period was 987 days (range, 7–2769) after
chemotherapy initiation for lymphoma. Fourteen patients died of
lymphoma, and 3 patients died of other diseases.
Of the 77 patients with resolved hepatitis B, 10
(13%) experienced HBV-R during and after chemotherapy and were
subsequently started on oral antiviral agents. Two of these 10
patients developed HBV-related hepatitis flares, but both recovered
with treatment, and no patients died of HBV-R. Three of the 10
patients became positive for anti-HBsAg, including 2 patients who
developed hepatitis flares.
Impact of the combination of anti-HBc
and HBs titres on predicting HBV-R
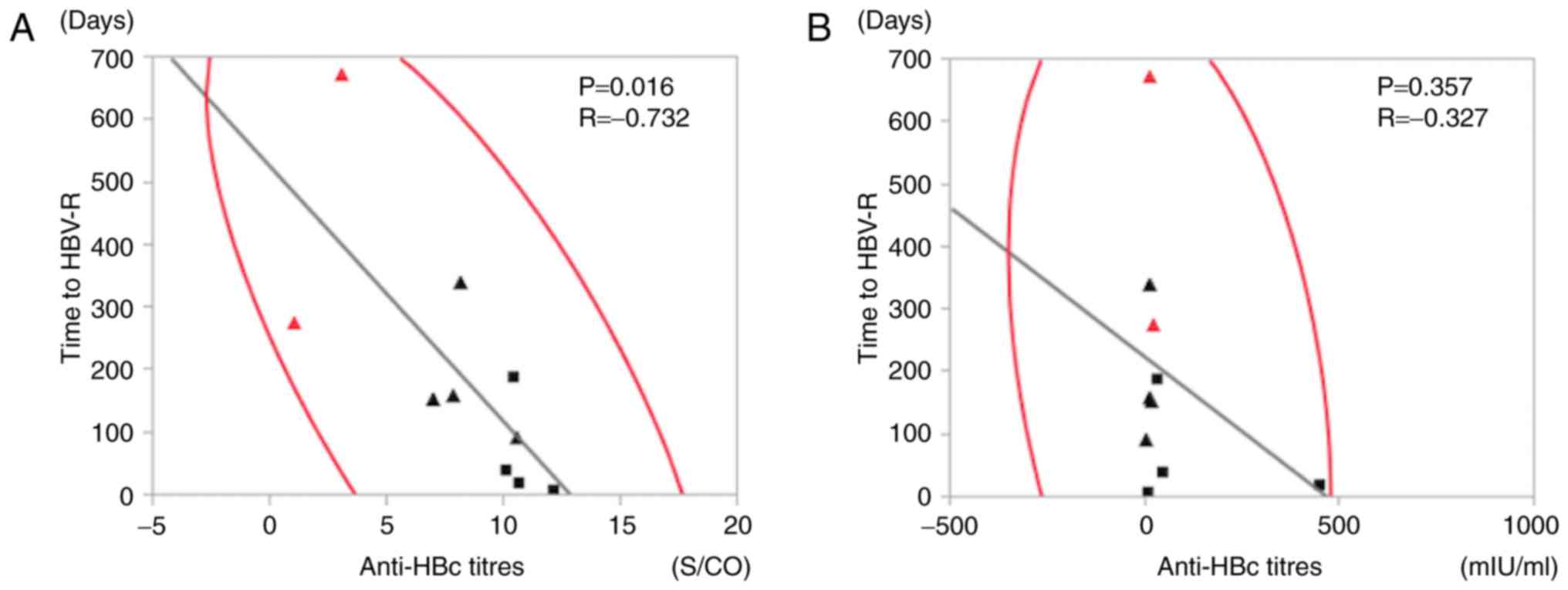
We performed correlation analyses using HBV-related
markers and time to HBV-R (Fig. 2).
There was no correlation between anti-HBs titres prior to
chemotherapy and time to HBV-R (R=−0.327, P=0.357) (Fig. 2B), but anti-HBc titres were
significantly negatively correlated with time to HBV-R
(R=−0.732, P=0.016) (Fig. 2A).
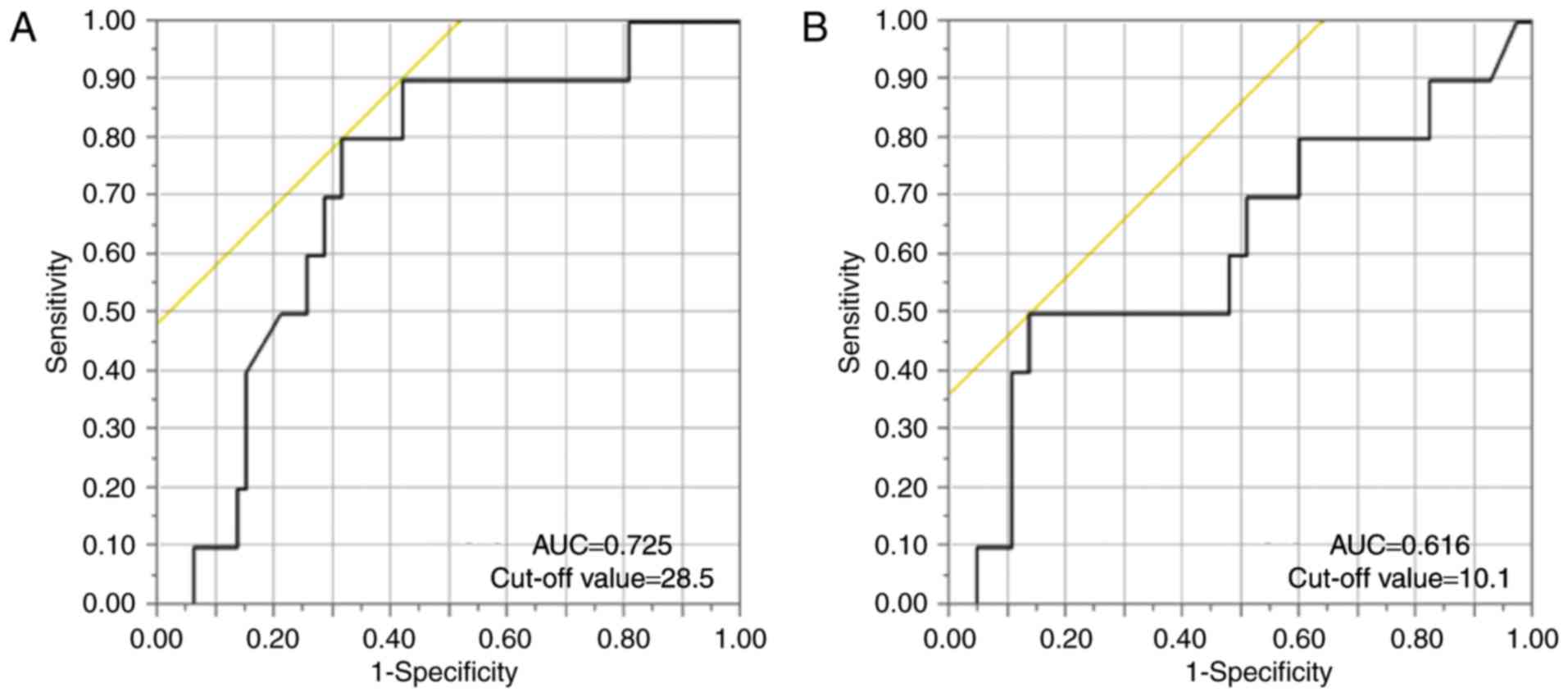
We then established anti-HBs and anti-HBc titre cut-off values for
predicting HBV-R via ROC curve analysis of the patients with
resolved hepatitis B. Our analysis demonstrated that the anti-HBs
and anti-HBc titre cut-off values were 28.5 mIU/ml (AUC: 0.725) and
10.1 S/CO (AUC: 0.616), respectively (Fig. 3A and B). We therefore established
anti-HBs and anti-HBc titre cut-off values of 28 mIU/ml and 10 S/CO
for predicting HBV-R.
Univariate and multivariate logistic regression
analyses were performed to identify the predictive factors
associated with HBV-R. In both types of analyses, both anti-HBc and
anti-HBs titres at baseline were significant predictive factors for
HBV-R. However, rituximab-containing chemotherapy was not a
significant predictive factor for HBV-R (Table II). Additionally, treatment efficacy
and HBV-R were not correlated (data not shown).
| Table II.Analysis of the factors associated
with HBV reactivation. |
Table II.
Analysis of the factors associated
with HBV reactivation.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variable | Odds ratio (95%
CI) | P-value | Odds ratio (95%
CI) | P-value |
|---|
| Age |
|
|
|
|
|
>75 | 1 |
| 1 |
|
|
<75 | 0.914
(0.234–3.569) | 0.895 | 1.577
(0.265–10.693) | 0.616 |
| Sex |
|
|
|
|
| M | 1 |
| 1 |
|
| F | 0.597
(0.121–2.354) | 0.471 | 0.425
(0.035–4.095) | 0.464 |
| ALT |
|
|
|
|
|
>16 | 1 |
| 1 |
|
|
<16 | 1.456
(0.381–6.134) | 0.583 | 1.986
(0.261–16.023) | 0.501 |
| Albumin |
|
|
|
|
|
>3.5 | 1 |
| 1 |
|
|
<3.5 | 1.216
(0.318–5.127) | 0.776 | 1.135
(0.182–7.114) | 0.889 |
| Prothrombin time
(%) |
|
|
|
|
|
>90 | 1 |
| 1 |
|
|
<90 | 0.853
(0.217–3.347) | 0.815 | 0.480
(0.048–4.046) | 0.501 |
| Total
bilirubin |
|
|
|
|
|
>0.6 | 1 |
| 1 |
|
|
<0.6 | 2.8
(0.711–13.869) | 0.144 | 1.733
(0.266–12.171) | 0.560 |
| Anti-HBc titres
(S/CO) |
|
|
|
|
|
>10 | 1 |
| 1 |
|
|
<10 | 0.115
(0.036–0.655) | 0.012 | 0.110
(0.013–0.665) | 0.016 |
| Anti-HBs titres
(mIU/ml) |
|
|
|
|
|
>28 | 1 |
| 1 |
|
|
<28 | 5.111
(1.286–25.565) | 0.020 | 10.505
(1.749–105.993) | 0.009 |
| Treatment
regimen |
|
|
|
|
|
RTX(+) | 1 |
| 1 |
|
|
RTX(−) | 1.579
(0.253–30.717) | 0.665 | 1.331
(0.120–34.000) | 0.828 |
Comparison of HBV-R rates among groups
based on anti-HBc and anti-HBs titres
Using the cut-off anti-HBc value alone does not have
good predictive value. Therefore, we concluded that the combination
of anti-HBc and anti-HBs titres at baseline in patients with
lymphoma could serve as a surrogate marker of HBV-R under the
influence of chemotherapy. We initially divided the patients with
resolved hepatitis B prior to chemotherapy, for whom the
combination of anti-HBs and anti-HBc cut-off titres was used to
predict HBV-R, into 4 groups. We divided the anti-HBc group into a
high-titre group (Chigh) and a low-titre group
(Clow) based on the predetermined cut-off levels
(Fig. 4A). In the same manner, we
divided the anti-HBs group into a high-titre group
(Shigh) and a low-titre group (Slow)
(Fig. 4B). However, the
ChighShigh (n=9) and
ChighSlow (n=5) groups were analysed
collectively as Chigh because the number of patients in
each group was small and because the incidence of HBV-R (3/9, 33%;
2/5, 40%, respectively) was high among these patients, resulting in
the following 3 HBV-R risk groups: Chigh (n=14),
ClowSlow (n=23) and
ClowShigh (n=40) (Fig. 4C). Comparison analysis was performed
to determine the HBV-R rates in the Chigh,
ClowSlow and ClowShigh
groups, which were 35.7% (5/14), 21.7% (5/23) and 0% (0/40),
respectively (Fig. 4C). Consequently,
compared with the patients in the ClowShigh
group, who did not experience complete reactivation, those in the
Chigh and ClowSlow groups
experienced significantly higher rates of HBV-R (P<0.0001 and
P=0.002, respectively). Additionally, the patients in the
Chigh group experienced a significantly higher rate of
HBV-R than those in the Clow group (P=0.015; Fig. 4A). Similarly, the patients in the
Slow group experienced a significantly higher rate of
HBV-R than those in the Shigh group (P=0.031; Fig. 4B). Additionally, a comparison of the
HBV-R rate between those with anti-HBs high and anti-HBs low in the
anti-HBc high group (ChighShigh vs.
ChighSlow) would be useful for estimating the
importance of anti-HBc in HBV-R. Patients in the
ChighSlow group seemed more likely to
experience HBV-R than those in the ChighShigh
group, although the difference was not statistically significant
due to the limited number of subjects. An overview of the 4 groups
categorized by antibody titres is provided in Table III.
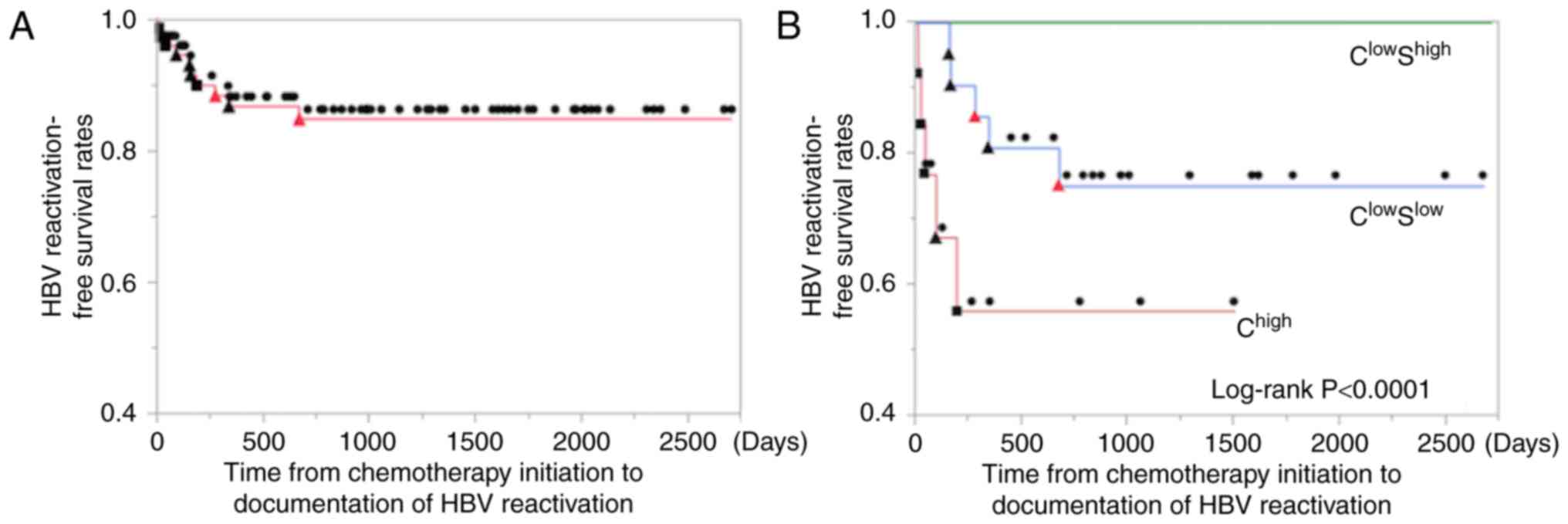
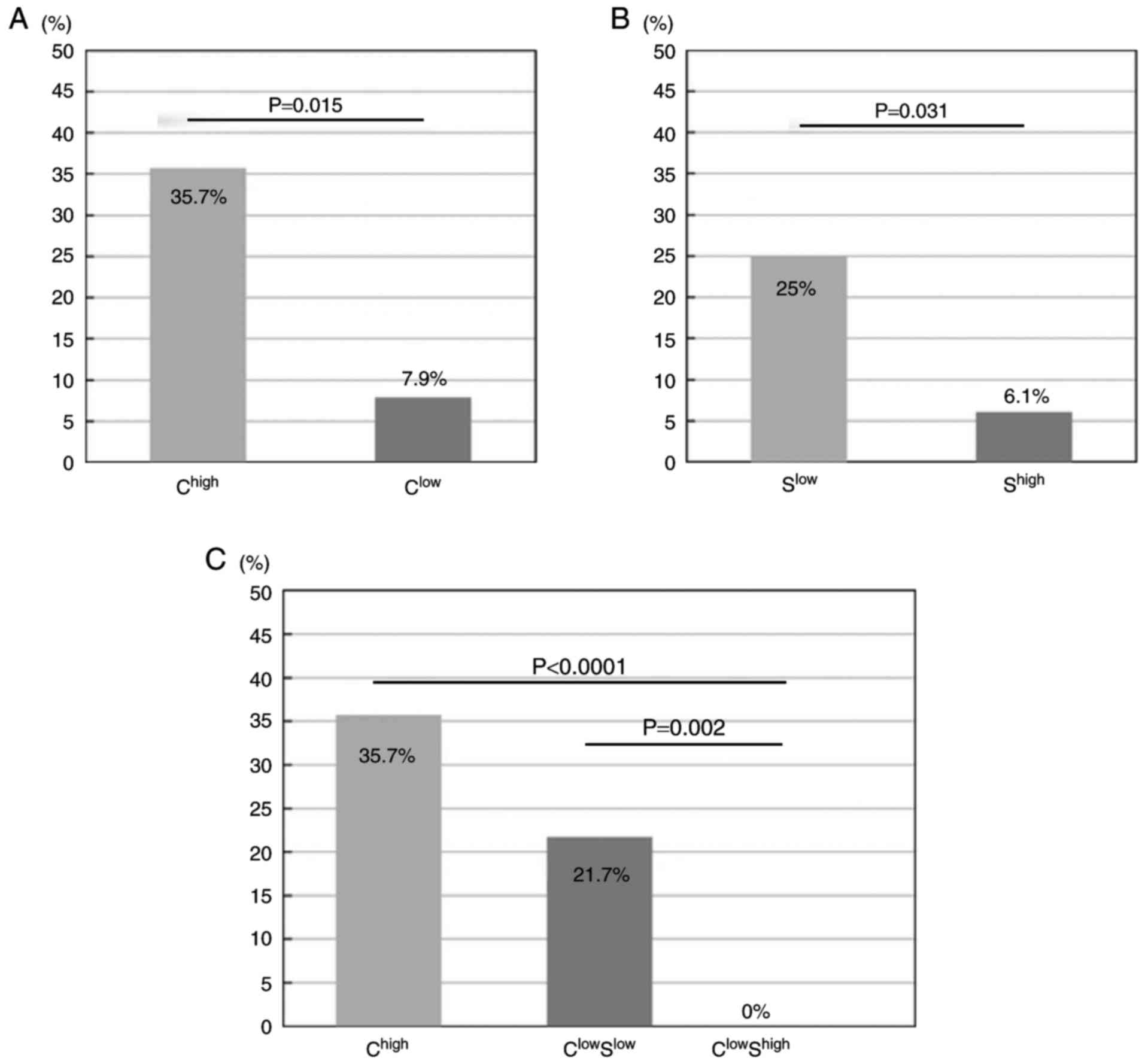 | Figure 4.Incidence of hepatitis B virus
reactivation (HBV-R). (A) Lymphoma patients were divided into the
following two groups according to cut-off values predetermined via
ROC analysis: A high anti-hepatitis B core (HBc) (HBc) titre group
(Chigh) and a low anti-HBc (Clow) group. The
left and right bars represent the data for the Chigh and
Clow groups, respectively. The incidences of HBV-R in
the two groups are shown (Chigh=35.7% (5/14) and
Clow=7.9% (5/63), respectively). The Chigh
group experienced a significantly higher rate of HBV-R than the
Clow group (P=0.015). The incidences of HBV-R were
compared using Chi-square tests. (B) Lymphoma patients were divided
into the following two groups according to cut-off values
predetermined via ROC curve analysis of anti-hepatitis B
surfac(HBs) titres: A high anti-HBs titre group (Shigh)
and a low anti-HBs group (Slow). The left and right bars
show the data for Slow and Shigh,
respectively. The incidences of HBV-R in the two groups are shown
(Slow=25% (7/28) and Shigh=6.1% (3/49),
respectively). The Slow group experienced a
significantly higher rate of HBV-R than the Shigh group
(P=0.031). The incidences of HBV-R were compared using chi-square
tests. (C) Lymphoma patients were divided into the following three
groups according to cut-off values predetermined via ROC analysis:
A high anti-HBc titre group (Chigh), a low anti-HBc/low
anti-HBs (ClowSlow) group, and a
Clow/high anti-HBs titre group
(ClowShigh). The left, middle and right bars
represent the data for the Chigh,
ClowSlow and ClowShigh
groups, respectively. The incidences of HBV-R in the three groups
are shown (Chigh=35.7% (5/14),
ClowSlow=21.7% (5/23), and
ClowShigh=0% (0/40), respectively).
Chigh and ClowSlow experienced a
significantly higher rate of HBV-R than did
ClowShigh, P<0.0001 and P=0.002,
respectively. The incidences of HBV-R were compared using the
Kruskal-Wallis non-parametric test. |
| Table III.Details of the 4 groups categorized
by antibody titres. |
Table III.
Details of the 4 groups categorized
by antibody titres.
| Group | Patients, n | Age, years | Sex (% male) | Anti-HBc titres
(S/CO) | Anti-HBs titres
(mIU/ml) | Occurrence of HBV-R
(%) | Time to HBV-R
(days) | HBV-R/HF |
|---|
|
ChighShigh | 9 | 76 (71–83) | 56 | 10.8
(10.1–12.9) | 254 (28.5–500) | 33.3 | 84 (21–190) | HBV-R |
|
ChighSlow | 5 | 78 (73–81) | 60 | 16.2 (10.6–35) | 3.5 (0–6.7) | 40 | 51 (9–93) | HBV-R |
|
ClowShigh | 40 | 73 (47–89) | 60 | 6.1 (0.07–10) | 358
(28.6–2990) | 0 | none | HBV-R |
|
ClowSlow | 23 | 76 (62–83) | 61 | 6.4
(0.98–9.85) | 10.9
(0.2–27.5) | 21.7 | 322 (156–673) | HBV-R/HF |
Comparison of time to HBV-R after
starting chemotherapy among the three groups
No patients in the ClowShigh
group completely reactivated. Therefore, the median time to HBV-R
after starting chemotherapy was compared between the
Chigh and ClowSlow groups via the
log-rank test. Their cumulative median times were 41 and 277 days
(range, 9–190, 156–673), respectively. In the Chigh
group, all cases of HBV-R occurred within 1 year after starting
chemotherapy (P<0.0001). However, in the
ClowSlow group, one patient (1/5) developed
HBV-R beyond 1 year after starting or finishing chemotherapy (673
or 475 days, respectively) (Fig.
5).
Details of the 10 patients who
developed HBV-R
The details of the 10 patients who developed HBV-R
are shown in Table IV, which lists
these patients' HBcAb titres prior to chemotherapy in descending
order. Of these 10 patients, 7 (70%) were male. The patients with
HBV-R ranged from 62–82 years of age. Two patients (20%) developed
HBV-related hepatitis flares, and three patients' (30%) serum HBsAg
turned positive after HBV-R. Both patients with hepatitis flares
experienced a reversion of their HBsAg seropositivity.
| Table IV.Details of the 10 patients with HBV
reactivation. |
Table IV.
Details of the 10 patients with HBV
reactivation.
| Patient No. | Age (years) | Sex | Haematologic
diagnosis | Treatment
regimen | Anti-HBc titres
(S/CO) | Anti-HBs titres
(mIU/ml) | Time to HBV-R
(days) | Time from the final
chemotherapy treatment to HBV-R | HBsAg reverse
seroconversion | Peak HBV-DNA (log
copies/ml) | Peak ALT
(IU/l) | HBV-R or HF |
|---|
| 1 | 73 | M | FL | Rituximab
alone | 12.1 | 6.7 |
9a |
| (−) | 2.6 |
11 | HBV-R |
| 2 | 71 | F | DLBCL | R-CHOP | 10.6 | 446.4 |
21a |
| (−) | <2.1 |
15 | HBV-R |
| 3 | 79 | M | DLBCL | R-CHOP | 10.6 | 1.1 | 93 | 25 | (+) | 7.0 |
38 | HBV-R |
| 4 | 73 | M | LPL | Fludarabine | 10.4 | 28.5 | 190a |
| (−) | 2.8 |
40 | HBV-R |
| 5 | 78 | F | BL | DA-EPOCH-R | 10.1 | 45.7 |
41a |
| (−) | <2.1 |
26 | HBV-R |
| 6 | 82 | M | DLBCL | R-THP-COP | 8.1 | 9 | 341 | 299 | (−) | <2.1 |
11 | HBV-R |
| 7 | 77 | M | DLBCL | R-THP-COP | 7.8 | 9.3 | 161 | 48 | (−) | <2.1 |
32 | HBV-R |
| 8 | 78 | M | DLBCL | R-THP-COP | 6.9 | 17.2 | 156 | 1 | (−) | <2.1 |
10 | HBV-R |
| 9 | 62 | F | DLBCL | R-CHOP | 3.0 | 10 | 673 | 475 | (+) | 6.3 | 1768 | HF |
| 10 | 74 | M | DLBCL | Rituximab
alone | 1.0 | 20 | 277 | 134 | (+) | 8.4 |
143 | HF |
Regarding the clinical courses of the patients with
HBV-R, the median anti-HBc titres and anti-HBs titres prior to
chemotherapy were 9.1 S/CO and 13.6 mIU/ml, respectively. The
median time from the start of chemotherapy to HBV-R in the four
patients who experienced reactivation during chemotherapy was 31
days (range, 9–190), and all these patients were in the
Chigh group. In contrast, the median time to HBV-R in
the six patients who experienced reactivation during follow-up was
91 days (range, 1–475) from the final chemotherapy treatment to
HBV-R. Three of the 10 patients had delayed HBV-R (30%), and all
three were in the ClowSlow group. No cases of
HBV-related fulminant hepatitis or hepatitis-related deaths
occurred during the study period. All 5 patients with HBV-R and
lower titres of HBcAb showed lower titres of HBsAb (Table IV). Thus, patients in the
ClowShigh group did not experience complete
reactivation, but those in the ClowSlow group
had a relatively higher risk of HBV-R.
Discussion
Fatal HBV-R is a well-described serious complication
of chemotherapy in cancer patients with resolved HBV infection and
is reported to have a higher incidence than liver-related mortality
in patients with acute hepatitis (13). Meticulous monitoring of HBV DNA is a
unique predictive method of detecting the occurrence of
life-threatening HBV-R (9,10). Thus far, the patterns that are
predictive of the occurrence of HBV-R remain unclear, and methods
for identifying these patterns are in high demand clinically and
economically.
The relationship between HBV-R and HBV-related
markers in lymphoma patients with resolved HBV infection has
recently been reported. In previous reports related to anti-HBs,
lymphoma patients with high anti-HBs titres (>100 mIU/ml) prior
to chemotherapy experienced significantly lower HBV-R rates than
did other patients (7). However,
patients with undetectable anti-HBs titres (<10 mIU/ml) faced a
significantly higher risk of HBV-R than did other patients and had
a poor prognosis (9,14). Regarding anti-HBc, anti-HBc-positive
patients were reported to experience reactivation rates that were
significantly higher than those of anti-HBc-negative patients
(15). The results of these previous
reports indicate that the incidence of HBV-R may be associated with
the HBV immune status of the host prior to therapy. Hence, we
retrospectively examined the risk factors for developing HBV-R
using data pertaining to HBV-related markers in patients with
resolved HBV infection. In the present study, we found that the
combination of anti-HBc and anti-HBs levels may be useful for
predicting the development and timing of chemotherapy-induced
hepatitis B reactivation in lymphoma patients with resolved HBV
infection. Our results demonstrated that patients with high
anti-HBc titres (>10 S/CO) prior to chemotherapy experienced a
significantly higher rate of HBV-R than did patients with both low
anti-HBc (<10 S/CO) and high anti-HBs levels (>28 mIU/ml),
who did not completely reactivate. We conclude that anti-HBc and
anti-HBs titres prior to chemotherapy can be used to identify HBV-R
in lymphoma patients with resolved HBV infection. We did not track
serial changes in these parameters because regular monitoring of
only HBV-DNA, not of HBsAg, HBcAb or HBsAb, is recommended
according to the guidelines (12).
However, we agree that monitoring serial changes in HBsAg, HBcAb
and HBsAb during the follow-up period is important, and this will
be done in future studies.
Generally, anti-HBc antibodies are considered an
indicator of past and persistent HBV infection. However, it is
well-recognized that the utility of quantitative anti-HBc
(qAnti-HBc) measurements is hampered by detection technology
limitations and a lack of international standardization compared
with measurements of anti-HBs. Additionally, to date, little is
known about the clinical significance of qAnti-HBc levels; however,
several recent reports revealed that baseline qAnti-HBc levels were
a useful predictor of treatment response in both interferon-alpha
and nucleoside analogue therapy. Additionally, qAnti-HBc levels
were closely correlated with signs of hepatic inflammation, such as
ALT levels, during therapy and follow-up. The reported mechanism
behind this correlation involves the release of HBcAg particles
from damaged hepatocytes and the production of antibodies against
HBcAg by B-cells, resulting in increased serum anti-HBc levels
(16,17). These results indicate that higher
qAnti-HBc levels at baseline may reflect higher host immune
activity for HBV. The reason for the discrepancy between anti-HBc
and anti-HBs levels in the host immune response against HBV remains
unclear, but Zhang et al (16)
reported a difference in the intrahepatic localization of HBcAg and
HBAg, which may provide insight into the observed discrepancy in
levels. In the present study, the same method of measuring
qAnti-HBc levels was used throughout the study period. Regarding
the incidence of HBV-R, we speculate that patients with high
anti-HBc titres can regularly activate their immunity for HBV;
therefore, they may be much more likely to experience HBV-R when
host immunity is supressed by chemotherapy or immunosuppressive
treatment. However, clinical evidence regarding the ability of
qAnti-HBc to predict HBV-R is lacking, and the collection of
additional data is awaited.
In patients with resolved HBV infection, HBV
replication has been shown to persist in the liver and in
peripheral blood mononuclear cells for decades (17,18).
Interestingly, in healthy liver transplantation donors with
anti-HBc-positivity, HBsAg-negativity and undetectable HBV DNA, HBV
was shown to be present in the liver, resulting in HBV-R in
recipients due to transmission after transplantation (19). These reports show that even patients
previously infected with HBV who were considered to be cured of
clinical infection retain HBV in their bodies, resulting in a risk
of HBV-R during and after chemotherapy and immunosuppressive
treatment.
To date, several studies of host immune status after
acute hepatitis have been performed. These studies have reported
that insufficient decreases in anti-HBc titres after acute
hepatitis B infection may influence the disappearance of HBV DNA
(20,21). Therefore, the existence of a
relationship between HBV-R and declining immunocompetence in
patients with resolved HBV infection cannot be denied. Thus,
circulating HBV antigen-antibody marker measurements are very
important for understanding the immune condition of the host after
HBV infection. Furthermore, these reports indicate that the levels
of HBV-related antibodies, including anti-HBc and anti-HBs, may
serve as surrogate markers for host anti-HBV immune status after
acute hepatitis B infection. Based on these reports, we examined
whether anti-HBc and anti-HBs titres at baseline prior to
chemotherapy were related to the development and timing of HBV-R in
lymphoma patients with resolved HBV infection. In a previous study
of HBV-R and timing in HBsAg-negative patients who underwent
cytotoxic chemotherapy, Hui et al (4) reported that the time to HBV-R, defined
as a 100-fold increase in serum HBV-DNA levels compared with
pre-therapy levels, was 18.5 weeks after starting chemotherapy
(range, 12 to 28 weeks). Additionally, a multicentre cooperative
study in Japan reported that 36% of patients who experienced HBV-R
developed reactivation more than 12 months after completion of
chemotherapy (22). However, it has
been difficult to predict the incidence and timing of HBV-R prior
to therapy. In this study, we investigated whether HBV-related
markers can predict the development of HBV-R.
Our study has several limitations because of its
retrospective design. Although the criteria and monitoring of HBV-R
have been introduced according to the Hepatitis B Treatment
Guidelines of the Japan Society of Hepatology since 2011 in Japan,
they are not based on conclusive evidence. Consequently, in the
present study, the follow-up strategy, including the administration
of HBV DNA tests or the evaluation of anti-HBc or anti-HBs status
prior to chemotherapy, was determined by the attending physicians.
This suggests that HBV DNA monitoring may be necessary every one to
three months and that we might have underestimated the incidence of
self-limited HBV-R. However, no deaths due to HBV-R occurred during
the approximately 2.7-year follow-up period. Therefore, it is
economically important to identify those patients at high risk for
HBV-R and the factors associated with its timing. This study was
conducted in only lymphoma patients. Accordingly, it is possible
that the results could be applied to patients with other
malignancies, but there are no data at this time on the diagnostic
value of our findings in other patient populations.
In summary, the combination of anti-HBc and anti-HBs
titres may represent a predictive marker for the development of
HBV-R and can reflect the elapsed time between chemotherapy
initiation and HBV-R. Because this retrospective cohort study was
performed at a single centre, validation analyses with a
prospective cohort in a clinical study group or at a high-volume
centre should be performed to confirm these findings.
Acknowledgements
The authors would like to thank Dr Hironori Take for
assistance with data collection and Dr Tatsuya Kanto for their
advice and comments during the preparation of the manuscript.
Glossary
Abbreviations
Abbreviations:
|
HBV
|
hepatitis B virus
|
|
HBV-R
|
HBV reactivation
|
References
|
1
|
Huang YH, Hsiao LT, Hong YC, Chiou TJ, Yu
YB, Gau JP, Liu CY, Yang MH, Tzeng CH, Lee PC, et al: Randomized
controlled trial of entecavir prophylaxis for rituximab-associated
hepatitis B virus reactivation in patients with lymphoma and
resolved hepatitis B. J Clin Oncol. 31:2765–2772. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Matsue K, Kimura S, Takanashi Y, Iwama K,
Fujiwara H, Yamakura M and Takeuchi M: Reactivation of hepatitis B
virus after rituximab-containing treatment in patients with
CD20-positive B-cell lymphoma. Cancer. 116:4769–4776. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yeo W, Chan TC, Leung NW, Lam WY, Mo FK,
Chu MT, Chan HL, Hui EP, Lei KI, Mok TS and Chan PK: Hepatitis B
virus reactivation in lymphoma patients with prior resolved
hepatitis B undergoing anticancer therapy with or without
rituximab. J Clin Oncol. 27:605–611. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hui CK, Cheung WW, Zhang HY, Au WY, Yueng
YH, Leung AY, Leung N, Luk JM, Lie AK, Kwong YL, et al: Kinetics
and risk of de novo hepatitis B infection in HBsAg-negative
patients undergoing cytotoxic chemotherapy. Gastroenterology.
131:59–68. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Fukushima N, Mizuta T, Tanaka M, Yokoo M,
Ide M, Hisatomi T, Kuwahara N, Tomimasu R, Tsuneyoshi N, Funai N
and Sueoka E: Retrospective and prospective studies of hepatitis B
virus reactivation in malignant lymphoma with occult HBV carrier.
Ann Oncol. 20:2013–2017. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Dong HJ, Ni LN, Sheng GF, Song HL, Xu JZ
and Ling Y: Risk of hepatitis B virus (HBV) reactivation in
non-Hodgkin lymphoma patients receiving rituximab-chemotherapy: A
meta-analysis. J Clin Virol. 57:209–214. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cho Y, Yu SJ, Cho EJ, Lee JH, Kim TM, Heo
DS, Kim YJ and Yoon JH: High titers of anti-HBs prevent
rituximab-related viral reactivation in resolved hepatitis B
patient with non-Hodgkin's lymphoma. J Med Virol. 88:1010–1017.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hayashi K, Ishigami M, Ishizu Y, Kuzuya T,
Honda T, Tachi Y, Ishikawa T, Katano Y, Yoshioka K, Toyoda H, et
al: Clinical characteristics and molecular analysis of hepatitis B
virus reactivation in hepatitis B surface antigen-negative patients
during or after immunosuppressive or cytotoxic chemotherapy. J
Gastroenterol. 51:1081–1089. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Seto WK, Chan TS, Hwang YY, Wong DK, Fung
J, Liu KS, Gill H, Lam YF, Lie AK, Lai CL, et al: Hepatitis B
reactivation in patients with previous hepatitis B virus exposure
undergoing rituximab-containing chemotherapy for lymphoma: A
prospective study. J Clin Oncol. 32:3736–3743. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kusumoto S, Tanaka Y, Suzuki R, Watanabe
T, Nakata M, Takasaki H, Fukushima N, Fukushima T, Moriuchi Y, Itoh
K, et al: Monitoring of hepatitis B virus (HBV) DNA and risk of HBV
reactivation in B-cell lymphoma: A prospective observational study.
Clin Infect Dis. 61:719–729. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Nishida T, Hiramatsu N, Mizuki M, Nagatomo
I, Kida H, Tazumi K, Shinzaki S, Miyazaki M, Yakushijin T, Tatsumi
T, et al: Managing hepatitis B virus carriers with systemic
chemotherapy or biologic therapy in the outpatient clinic. Hepatol
Res. 43:339–346. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Drafting Committee for Hepatitis
Management Guidelines and the Japan Society of Hepatology, . JSH
Guidelines for the Management of Hepatitis B Virus infection.
Hepatol Res. 44 Suppl:S1–S58. 2014. View Article : Google Scholar
|
|
13
|
Umemura T, Tanaka E, Kiyosawa K and Kumada
H; Japan de novo Hepatitis B Research Group, : Mortality secondary
to fulminant hepatic failure in patients with prior resolution of
hepatitis B virus infection in Japan. Clin Infect Dis. 47:e52–e56.
2008. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pei SN, Ma MC, Wang MC, Kuo CY, Rau KM, Su
CY and Chen CH: Analysis of hepatitis B surface antibody titers in
B cell lymphoma patients after rituximab therapy. Ann Hematol.
91:1007–1012. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Han JW, Yang H, Lee HL, Bae SH, Choi JY,
Lee JW, Kim HJ, Lee S, Cho SG, Min CK, et al: Risk factors and
outcomes of hepatitis B virus reactivation in hepatitis B surface
antigen negative patients with hematological malignancies. Hepatol
Res. 46:657–668. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhang X, Lu W, Zheng Y, Wang W, Bai L,
Chen L, Feng Y, Zhang Z and Yuan Z: In situ analysis of
intrahepatic virological events in chronic hepatitis B virus
infection. J Clin Invest. 126:1079–1092. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rehermann B, Ferrari C, Pasquinelli C and
Chisari FV: The hepatitis B virus persists for decades after
patients' recovery from acute viral hepatitis despite active
maintenance of a cytotoxic T-lymphocyte response. Nat Med.
2:1104–1108. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yuki N, Nagaoka T, Yamashiro M, Mochizuki
K, Kaneko A, Yamamoto K, Omura M, Hikiji K and Kato M: Long-term
histologic and virologic outcomes of acute self-limited hepatitis
B. Hepatology. 37:1172–1179. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Uemoto S, Sugiyama K, Marusawa H, Inomata
Y, Asonuma K, Egawa H, Kiuchi T, Miyake Y, Tanaka K and Chiba T:
Transmission of hepatitis B virus from hepatitis B core
antibody-positive donors in living related liver transplants.
Transplantation. 65:494–499. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Akahane Y, Okada S, Sakamoto M, Wakamiya
M, Kitamura T, Tawara A, Naitoh S, Tsuda F and Okamoto H:
Persistence of hepatitis B viremia after recovery from acute
hepatitis B: Correlation between anti-HBc titer and HBV DNA in
serum. Hepatol Res. 24:82002. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kobyashi M, Chayama K, Arase Y, Tsubota A,
Saitoh S, Suzuki Y, Kobayashi M, Murashima N, Ikeda K, Hagiwara M,
et al: Progressive and sufficient decrease of hepatitis B core
antibody can predict the disappearance of hepatitis B virus DNA in
Japanese patients with hepatitis B surface antigen clearance. J
Gastroenterol. 35:753–757. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Takahashi H, Ikeda M, Kumada T, Osaki Y,
Kondo S, Kusumoto S, Ohkawa K, Nadano S, Furuse J, Kudo M, et al:
Multicenter cooperative case survey of hepatitis B virus
reactivation by chemotherapeutic agents. Hepatol Res. 45:1220–1227.
2015. View Article : Google Scholar : PubMed/NCBI
|