Introduction
Prostate cancer (PCa) is the second most frequently
diagnosed type of cancer in men (1).
Although a number of methods for cancer therapy have been
developed, PCa remains the second leading cause of
cancer-associated mortality among males in economically developed
countries (2). In China, the
incidence of PCa has increased over the past few years, and has
become the sixth most common type of cancer and the ninth leading
cause of cancer-associated mortality. Although multiple molecular
and signaling pathways have characterized PCa proliferation,
migration, and invasion, the mechanisms remain elusive (3). Therefore, an improved understanding of
the biological mechanisms underlying PCa progression may contribute
to improve the clinical management and therapy. Furthermore, it is
essential to improve accuracy rate for tumor detection in males, as
the low specificity of prostate-specific antigen (PSA) induces
unnecessary biopsies and overtreatment (4). This could be achieved by identifying
other more specific biomarkers that can be useful in the diagnosis
of PCa.
microRNAs (miRNAs) are a type of endogenous, small
noncoding RNA. Growing evidence has demonstrated that miRNAs may
serve as potential tumor suppressors and oncogenes in PCa,
regulating the expression of its specific target genes involved in
cell development, and metastasis (5,6). The
miR-17-92 cluster, also termed oncomiR-I, is composed of six
members, including miR-17, miR-18a, miR-19a, miR-19b, miR-20a and
miR-92a (7). The miR-17-92 cluster
has been validated to be upregulated in several types of malignant
cancer (8). Hayashita et al
(9) suggested that overexpression of
the miR-17-92 cluster may perform an important role in the
development of lung cancer, particularly in small-cell lung cancer.
In Em-myc transgenic mice, B-cell lymphomas were
accelerated when the miR-17-92 cluster was transduced into
hematopoietic stem cells (10).
Higher expression levels of various miR-17-92 cluster miRNAs were
significantly associated with a lower overall survival rate in
patients with osteosarcoma (11). In
addition, a previous study indicated that the miR-17-92 cluster was
downregulated following exposure to radiation in prostate cancer
LNCaP cells (12). These findings
demonstrate the oncogenic role of the miR-17-92 cluster. Therefore,
the present study aimed to detect the differential expression of
the miR-17-92 cluster between PCa and benign prostatic hyperplasia
(BPH) tissue samples from patients, as well as between PCa, and BPH
cell lines. In addition, the association between miR-17-92 cluster
and PCa development was investigated.
Materials and methods
Patient samples
A total of 29 PCa tissues and 16 BPH tissues were
obtained from male patients who underwent surgery at Beijing
Chao-Yang Hospital, Capital Medical University (Beijing, China)
from January 2014 to January 2015. The mean age of patients was
68.14 years (range, 55–76 years). The experiment was conducted in
accordance with the Declaration of Helsinki (World Medical
Association), and the study was approved by the Ethics Committee of
Beijing Chao-Yang Hospital, Capital Medical University. Written
informed consent was obtained from each patient.
Cell cultures
The benign prostatic hyperplasia BPH1 cell line, and
the LNCaP and PC3 PCa cell lines were obtained from the American
Type Culture Collection (Manassas, VA, USA). Cells were cultured
routinely in RPMI-1640 supplemented with 5% fetal bovine serum, 100
U/ml penicillin and 50 µg/ml streptomycin (all Gibco; Thermo Fisher
Scientific, Inc., Waltham, MA, USA). All cell lines were grown in a
humidified incubator at 37°C with CO2.
RNA extraction and reverse
transcription-quantitative polymerase chain reaction (RT-qPCR)
Small RNA was extracted from tissues and cell lines
grown to 80% confluence using TRIzol® reagent
(Invitrogen; Thermo Fisher Scientific, Inc.). The primers for the
miR-17-92 cluster (including miR-17-3p, cat. no., CD201-0017;
miR-17-5p, cat. no., CD201-0016; miR-18a, cat. no., CD201-0018;
miR-19a, cat. no., CD201-0021; miR-19b, cat. no., CD201-0278; and
miR-92a, cat. no., CD201-0040), miRcute miRNA first-strand cDNA
synthesis kit and the miRcute miRNA qPCR detection kit (SYBR-Green;
both Tiangen Biotech Co., Ltd., Beijing, China) were used to detect
the miR-17-92 cluster expression according to the manufacturer's
protocol. The forward primer sequence for U6 was
5′-GCAAGGATGACACGCAAATTC-3′. A universal reverse primer was
provided in the miRcute miRNA qPCR Detection kit. The PCR
conditions included an initiation period at 94°C for 2 min,
followed by a two-step PCR program consisting of 94°C for 20 sec
and 60°C for 34 sec for 40 cycles. All samples were normalized
against the internal control (U6 small nuclear RNA) and analyzed
using the 2−ΔΔCq method (13).
Statistical analysis
All experiments were repeated three times, and all
data were analyzed using SPSS software (version 19.0; IBM SPSS,
Armonk, NY, USA). Quantified data are presented as the mean ±
standard deviation. Comparisons between groups were performed using
one-way analysis of variance followed by all pairwise multiple
comparison procedures using Bonferroni correction and Student's
t-tests or nonparametric tests. In addition, Spearman's correlation
was used for comparison and estimation of correlations between
miRNA expression levels, and clinicopathological characteristics,
including the Gleason score (14) and
PSA. Receiver operating curve (ROC) analysis was performed for
evaluation of specificity and sensitivity of miR-17-92 cluster
expression levels for distinguishing between patients with PC, and
patients with BPH. All miRNAs significantly different between the
PCa and BPH group were incorporated by logistic regression, and
then multiplied by the relative quantities levels for each miRNA in
each patient. Biochemical recurrence-free survival times of the
patients with PCa were evaluated using the Kaplan-Meier method and
log-rank tests according to the cutoff value of combined miRNA
score: (−4.668+0.069) × (miR-17-3p+0.023) × (miR-17-5p+0.107) ×
(miR-18a+0.171) × (miR-19a+0.479) × (miR-19b-0.057) × (miR-92a).
P<0.05 was considered to indicate a statistically significant
difference.
Results
Differential expression of miR-17-92
cluster in PCa specimens compared with BPH
Total RNA was isolated from prostate tissues of 29
males with PCa and 16 with BPH. The clinicopathological
characteristics of patients are presented in Table I. The RT-qPCR results revealed
significantly increased expression levels of miR-17-3p, miR-17-5p,
miR-18a, miR-19a, miR-19b and miR-92a in the cancer tissues of
patients with PCa compared with patients with BPH, but no
significant differences in the level of miR-20a were identified
between the two groups (Fig. 1A).
Notably, miR-19a and miR-92a were only significantly increased in
the high-grade PCa group (Gleason >6; n=23), but similar levels
were maintained in patients with low-grade PCa (Gleason ≤6; n=6)
and BPH (n=16) (Fig. 1A).
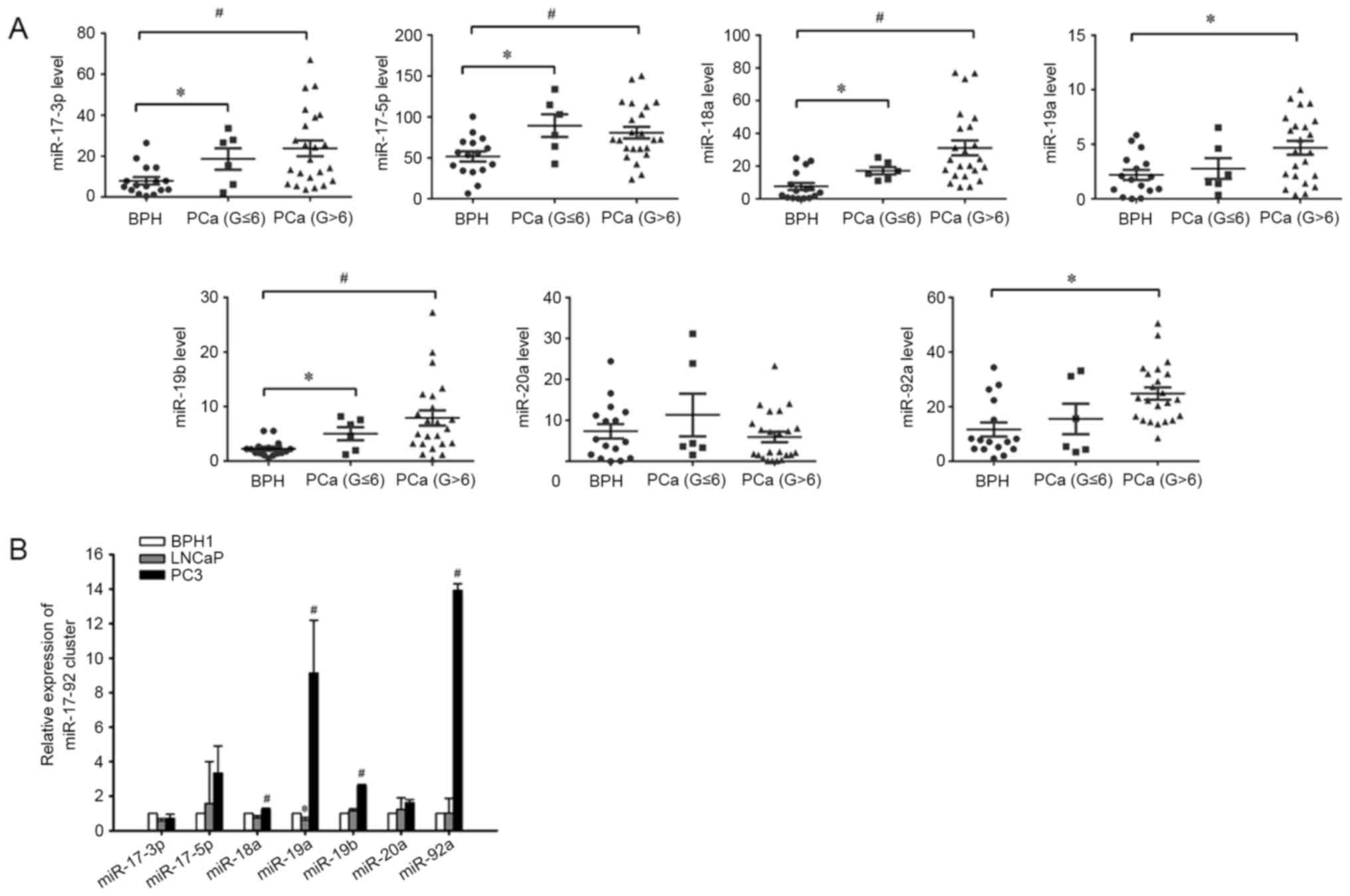 | Figure 1.miR-17-92 cluster expression levels in
patients with BPH, low-grade PCa, or high-grade PCa, and in BPH and
PCa cell lines. (A) Expression of the miR-17-92 cluster was higher
in PCa tissues compared with in BPH tissues. The expression of the
miR-17-92 cluster in tissues was measured using reverse
transcription-quantitative polymerase chain reaction. U6 served as
an internal loading control. Each sample was detected in
triplicate. *P<0.05 vs. BPH, #P<0.05 vs. BPH. (B)
Expression of miR-18a, miR-19a, miR-19b and miR-92a was
significantly higher in PC3 cells compared with in BPH1 and LNCaP
cell lines, but the expression of miR-19a was significantly lower
in LNCaP cells compared with BPH1 cells. *P<0.05 vs. BPH1,
#P<0.05 vs. BPH1 and LNCaP. PCa, prostate cancer;
miR, microRNA; BPH, benign prostatic hyperplasia; G, Gleason
score. |
 | Table I.Clinicopathological data of patients
with PCa and BPH. |
Table I.
Clinicopathological data of patients
with PCa and BPH.
|
| Value |
|---|
|
|
|
|---|
| Characteristic | PCa | BPH |
|---|
| Total, n | 29 | 16 |
| Mean age, years
(range) | 68.14 (55–76) | 68.25 (49–77) |
| Mean PSA (range) | 56.004
(0.002–1000) | 5.080
(0.343–12.035) |
| Clinical stage,
n |
|
|
| T1c | 2 | N/A |
| T2c | 11 | N/A |
| T3a | 6 | N/A |
| T3b | 8 | N/A |
| T4b | 2 | N/A |
| Gleason score, n |
|
|
| 3 +
3 | 6 | N/A |
| 3 +
4 | 6 | N/A |
| 4 +
3 | 8 | N/A |
| 4 +
4 | 6 | N/A |
| 4 +
5 | 2 | N/A |
| 5 +
4 | 1 | N/A |
miR-17-92 cluster expression in
prostate cell lines
The miR-17-92 cluster expression pattern was
determined in cultured prostate cell lines. Three different benign
and PCa cell lines were used. All of the six miRNAs in miR-17-92
cluster were detectable in the human BPH1 cell line and PCa cell
lines, LNCaP and PC3. Similarly, it was revealed that the
expression level of miR-18a, miR-19a, miR-19b and miR-92a were
significantly increased in the human PC3 cell line compared with
that in the BPH1 and LNCaP cell lines (Fig. 1B).
Correlations between miR-17-92 cluster
expression and clinicopathological features in PCa specimens
Among the 29 patients with PCa, the correlations of
Gleason grade and PSA level with the progression risk of PCa were
evaluated using bivariate correlation analysis. High expression of
miR-17-3p, miR-18a, miR-19a, miR-19b and miR-92a was identified to
be positively correlated with Gleason grade, but no correlation
with PSA was observed (Table
II).
| Table II.Correlation coefficients between
miR-17-92 cluster expression and clinicopathological features in
prostate cancer specimens. |
Table II.
Correlation coefficients between
miR-17-92 cluster expression and clinicopathological features in
prostate cancer specimens.
|
| PSA | Gleason |
|---|
|
|
|
|
|---|
| Variable | R | P-value | R | P-value |
|---|
| miR-17a-3p | 0.018 | 0.928 | 0.602 | 0.001 |
| miR-17a-5p | 0.240 | 0.210 | −0.352 | 0.061 |
| miR-18a | −0.029 | 0.880 | 0.764 | <0.001 |
| miR-19a | 0.121 | 0.532 | 0.468 | 0.011 |
| miR-19b | −0.046 | 0.812 | 0.710 | <0.001 |
| miR-20a | −0.175 | 0.364 | 0.080 | 0.682 |
| miR-92a | −0.111 | 0.566 | 0.592 | 0.001 |
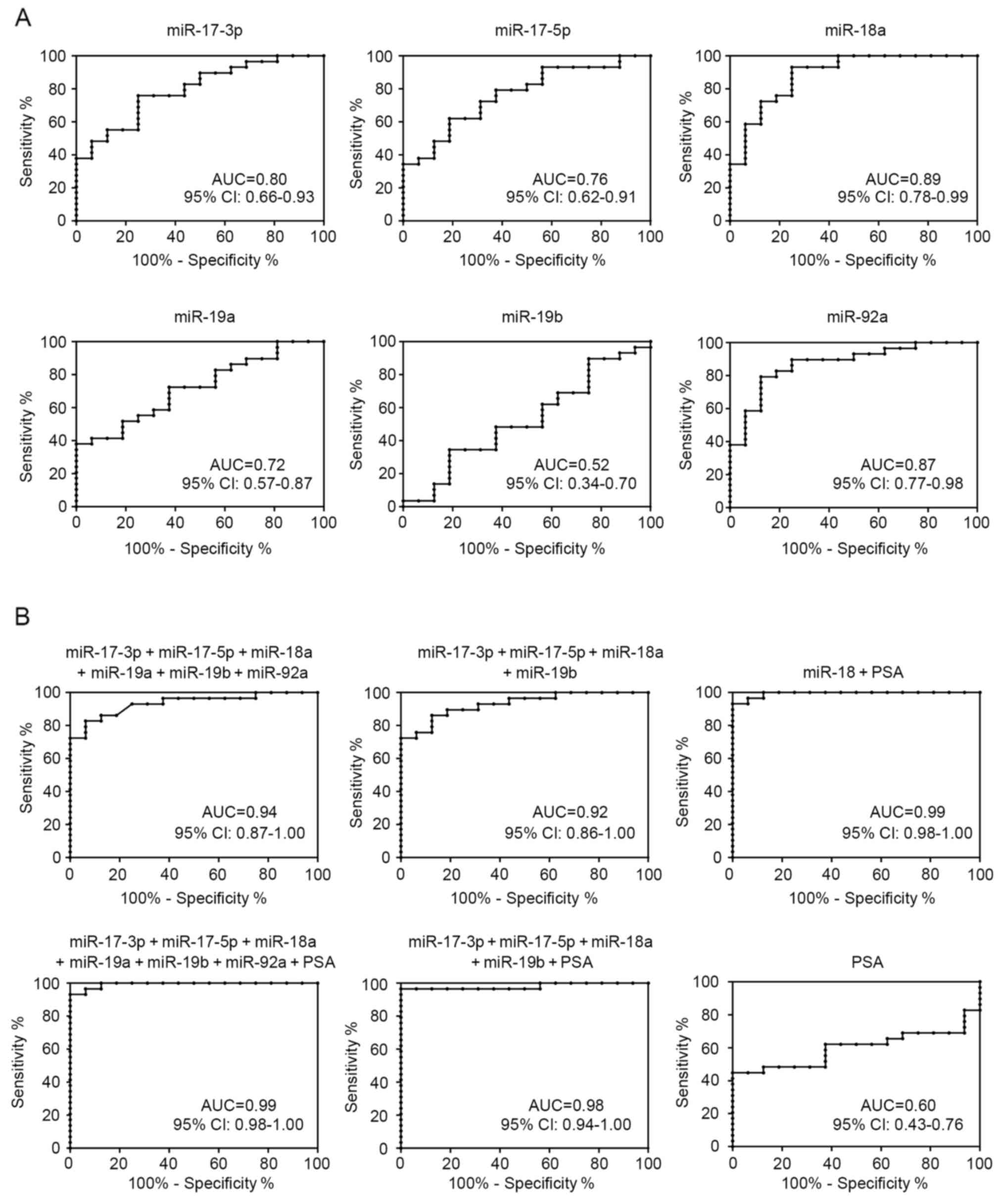
ROC analysis of the miR-17-92 cluster
expression in PCa specimens
ROCs were constructed to explore the potential value
of analyzed miR-17-92 cluster expression as diagnostic biomarkers
for PCa (Fig. 2A). Notably, miR-18a
demonstrated the most accurate discrimination [area under the ROC
curve (AUC), 0.89; 95% confidence interval, 0.78–0.99; P<0.0001]
between PCa and BPH. At the optimal cut-off value (9.54) of
relative quantification, the sensitivity was 93.1% and specificity
was 75.0%.
Combinations of miR-17-92 cluster and
PSA improve diagnostic accuracy in ROC analysis
As presented in Fig.
2B, to evaluate the use of the miR-17-92 cluster as biomarkers
of PCa diagnosis and progression, all the upregulated miRNAs were
combined to distinguish between patients with PCa and BPH. In
addition, four significantly increased miRNAs in the low-grade and
high-grade PCa groups, including miR-17-3p, miR-17-5p, miR-18a, and
miR-19b, were also grouped together to identify the presence of
PCa. These multimarker ROC analyses demonstrated higher AUC,
sensitivity and specificity compared with the use of each miRNA
alone (Fig. 2A). Furthermore, certain
combinations of these miRNAs and PSA improved the diagnostic
accuracy in ROC analysis. Considering that the miR-18a alone
demonstrated the most accurate discrimination between PCa and BPH,
miR-18a was combined with PSA, and the combination significantly
outperformed miR-18a use alone with an AUC of 0.99.
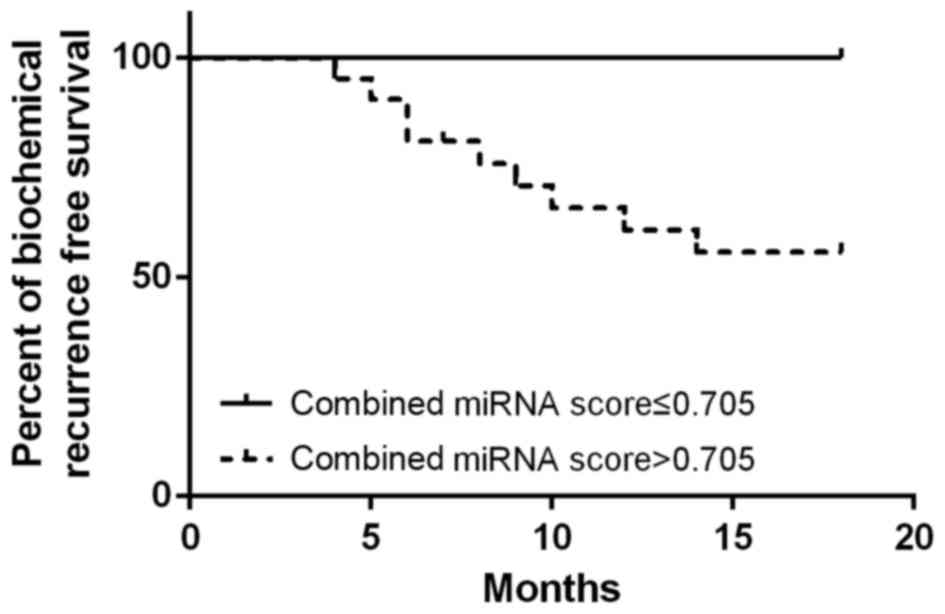
miR-17-92 cluster is a predictor of
aggressive PCa
The median follow-up time was 15.6 months. A total
of 9 patients exhibited biochemical PSA recurrence. For patients
with a combined miRNA score above vs. below the cutoff value (high,
>0.705; n=21 vs. low, ≤0.705; n=8), a high combined miRNA score
of miR-17-92 cluster was identified to be associated with shorter
biochemical recurrence interval (Fig.
3).
Discussion
Accumulating studies have demonstrated that aberrant
expression levels of miRNAs are involved in the development of
cancer. Aberrant expression of miRNA has been identified in various
tumor types, and effect essential cellular processes involved in
prostate tumorigenesis, including apoptosis-avoidance, cell
proliferation and migration, and the androgen signaling pathway
(15). Porkka et al (16) identified 51 differentially-expressed
miRNAs between benign and carcinoma tumors with 37 downregulated,
and 14 upregulated in carcinoma samples. Lichner et al
(17) identified 25
differentially-expressed miRNAs between the high and low
biochemical failure risk groups, and revealed that specific miRNAs
could aid in predicting biochemical failure risk at the time of
prostatectomy.
The polycistronic miR-17-92 cluster, located in the
third intron of the chromosome 13 open reading frame 25 gene, was
identified by Ota et al (18)
in 2004. Expression of these miRNAs promoted the proliferation and
suppressed apoptosis of cancer cells, and was identified to be
dysregulated in several types of malignant tumor (19,20). In
MYC transgenic mice, lymphoma development was accelerated following
the transduction of the miR-17-92 cluster into hematopoietic cells
(10). The miR-17-92 cluster was
highly expressed in human hepatocellular carcinoma compared with
the non-tumorous liver tissues (21).
High miR-17-92 cluster expression exhibited poor prognostic
implications in patients with diffuse large B-cell lymphoma
(22). In addition, the miR-17-92
cluster was highly expressed in T precursor cells, and regulated
lymphoproliferation in miR-17-92-transgenic models by targeting the
phosphatase and tensin homolog (23).
In addition, the miR-17-92 cluster was frequently and markedly
overexpressed in lung cancer, particularly in those with small-cell
lung cancer (9,24). The upregulation of the miR-17-92
cluster serves an important role in breast tumorigenesis and cell
invasion, which contributes to the response of triple-negative
breast to caloric restriction used in combination with radiation
(25). A previous study reported that
the miR-17-92 cluster was implicated in cervical cancer progression
(26). Altogether, these findings
demonstrated the potential of miR-17-92 cluster to disrupt the
homeostasis of multiple organs and induce malignancy.
miRNAs in the miR-17-92 cluster have been
demonstrated to function as oncogenes in PCa cells. Sylvestre et
al (27) suggested that miRNAs
from the miR-17-92 cluster serves as oncogenic miRNAs when
overexpressed, by acting on essential regulators of the cell cycle
and apoptosis. In addition, the miR-17-92 cluster can harbor
androgen receptor binding sites, and their expression is sensitive
to androgen stimulation in DUCaP and LNCaP cells (28). Members of the miRNA-17-92 cluster were
also identified in PCa progression. Yang et al (29) confirmed that miR-17-5p and miR-17-3p
could enhance PCa growth, and invasion by repressing the same
target tissue inhibitor of metalloproteinase 3. Furthermore, serum
levels of miR-19a and miR-19b were upregulated in patients with PCa
(30). In contrast to the present
results, the expression level of miR-20a was significantly higher
in patients with a Gleason score of 7–10 compared with the patients
with a Gleason score of 0–6, supporting the oncogenic role of
miR-20a in PCa (31). This
discrepancy may have been caused by differences in the source of
miRNA obtained and the detection methods used.
Of note, miR-18a is a highly expressed miRNA in
several types of cancer. The concentrations of miR-18a in
plasma/serum of patients with cancer, including esophageal,
pancreatic, hepatocellular and colorectal cancers, were all higher
compared with that of healthy volunteers (32). Shen et al (33) revealed that the expression levels of
miR-18a increased in lung cancer tissues, and Su et al
(34) demonstrated that miR-18a could
be a promising biomarker for the detection of gastric cancer, and
its upregulation may be associated with prognosis of bladder
cancer. Similar to these results, the present study also identified
miR-18a to be upregulated in patients with PCa, and ROC analysis
demonstrated that the increase of miR-18a in PCa tissues was the
most accurate diagnostic biomarker and could distinguish patients
with PCa from controls with high sensitivity and specificity.
Several studies have reported that numerous miRNAs
may be independent biochemical recurrence prediction markers
(35–38). The present study aimed to investigate
the potential of miR-17-92 cluster derived from surgery at the
initial visit in predicting the possibility of PCa progression or
metastasis, and the results obtained demonstrated that the
expression status of the miR-17-92 cluster was a good prognostic
marker for time to progression to biochemical recurrence.
To the best of our knowledge, the present study was
the first to demonstrate that the miR-17-92 cluster was upregulated
in PCa tissue samples as compared with BPH control tissue, which
suggests that these miRNAs are contributors to PCa oncogenesis.
Furthermore, the high expression of the miR-17-92 cluster
demonstrated increased sensitivity and specificity compared with
PSA on diagnosis of PCa. Finally, the present findings suggested
the high expression of the miR-17-92 cluster could be an
independent prognostic marker for PCa progression. Therefore,
miR-17-92 cluster is a potential diagnostic and prognostic
biomarker for PCa, and possesses clinical utility to identify
between patients with PCa and BPH. A combination of the miR-17-92
cluster and serum PSA can enhance the accuracy for diagnosis of
PCa. However, the cellular mechanisms for the changes in miRNA
levels in the prostate tissues with pathological progression are
yet to be elucidated.
Acknowledgements
The present study was supported by the Beijing
Municipal Administration of Hospitals Clinical Medicine Development
of Special Funding Support (grant no. ZYLX201408), National Natural
Science Foundation of China (grant no. 81200543), Beijing Natural
Science Foundation (grant no. 7142057) and Beijing Municipal Health
Bureau High-level Medical Professionals Promotion Project (grant
no. 2013-3-016).
References
|
1
|
Torre LA, Siegel RL, Ward EM and Jemal A:
Global cancer incidence and mortality rates and trends-an update.
Cancer Epidemiol Biomarkers Prev. 25:16–27. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Saad F and Fizazi K: Androgen deprivation
therapy and secondary hormone therapy in the management of
hormone-sensitive and castration resistant prostate cancer.
Urology. 86:852–861. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ren SC, Chen R and Sun YH: Prostate cancer
research in China. Asian J Androl. 15:350–353. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Schröder FH, Hugosson J, Roobol MJ,
Tammela TL, Ciatto S, Nelen V, Kwiatkowski M, Lujan M, Lilja H,
Zappa M, et al: Screening and prostate-cancer mortality in a
randomized European study. N Engl J Med. 360:1320–1328. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Carthew RW and Sontheimer EJ: Origins and
Mechanisms of miRNAs and siRNAs. Cell. 136:642–655. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Vanacore D, Boccellino M, Rossetti S,
Cavaliere C, D'Aniello C, Di Franco R, Romano FJ, Montanari M, La
Mantia E, Piscitelli R, et al: Micrornas in prostate cancer: An
overview. Oncotarget. 2017.[Epub ahead of print]. View Article : Google Scholar
|
|
7
|
Fuziwara CS and Kimura ET: Insights into
regulation of the miR-17-92 cluster of miRNAs in cancer. Front Med
(Lausanne). 2:642015.PubMed/NCBI
|
|
8
|
Olive V, Li Q and He L: mir-17-92: A
polycistronic oncomir with pleiotropic functions. Immunol Rev.
253:158–166. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hayashita Y, Osada H, Tatematsu Y, Yamada
H, Yanagisawa K, Tomida S, Yatabe Y, Kawahara K, Sekido Y and
Takahashi T: A polycistronic microRNA cluster, miR-17-92, is
overexpressed in human lung cancers and enhances cell
proliferation. Cancer Res. 65:9628–9632. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
He L, Thomson JM, Hemann MT,
Hernando-Monge E, Mu D, Goodson S, Powers S, Cordon-Cardo C, Lowe
SW, Hannon GJ and Hammond SM: A microRNA polycistron as a potential
human oncogene. Nature. 435:828–833. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Arabi L, Gsponer JR, Smida J, Nathrath M,
Perrina V, Jundt G, Ruiz C, Quagliata L and Baumhoer D:
Upregulation of the miR-17-92 cluster and its two paraloga in
osteosarcoma-reasons and consequences. Genes Cancer. 5:56–63.
2014.PubMed/NCBI
|
|
12
|
John-Aryankalayil M, Palayoor ST, Makinde
AY, Cerna D, Simone CB II, Falduto MT, Magnuson SR and Coleman CN:
Fractionated radiation alters oncomir and tumor suppressor miRNAs
in human prostate cancer cells. Radiat Res. 178:105–117. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) Method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rees MA, Resnick MI and Oesterling JE: Use
of prostate-specific antigen, Gleason score and digital rectal
examination in staging patients with newly diagnosed prostate
cancer. Urol Clin North Am. 24:379–388. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Catto JW, Alcaraz A, Bjartell AS, De Vere
White R, Evans CP, Fussel S, Hamdy FC, Kallioniemi O, Mengual L,
Schlomm T and Visakorpi T: MicroRNA in prostate, bladder and kidney
cancer: A systematic review. Eur Urol. 59:671–681. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Porkka KP, Pfeiffer MJ, Waltering KK,
Vessella RL, Tammela TL and Visakorpi T: MicroRNA expression
profiling in prostate cancer. Cancer Res. 67:6130–6135. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lichner Z, Fendler A, Saleh C, Nasser AN,
Boles D, Al-Haddad S, Kupchak P, Dharsee M, Nuin PS, Evans KR, et
al: MicroRNA signature helps distinguish early from late
biochemical failure in prostate cancer. Clin Chem. 59:1595–1603.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ota A, Tagawa H, Karnan S, Tsuzuki S,
Karpas A, Kira S, Yoshida Y and Seto M: Identification and
characterization of a novel gene, C13orf25, as a target for
13q31-q32 amplification in malignant lymphoma. Cancer Res.
64:3087–3095. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mendell JT: miRiad roles for the miR-17-92
cluster in development and disease. Cell. 133:217–222. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mogilyansky E and Rigoutsos I: The
miR-17/92 cluster: A comprehensive update on its genomics,
genetics, functions and increasingly important and numerous roles
in health and disease. Cell Death Differ. 20:1603–1614. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zhu H, Han C and Wu T: MiR-17-92 cluster
promotes hepatocarcinogenesis. Carcinogenesis. 36:1213–1222. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Go H, Jang JY, Kim PJ, Kim YG, Nam SJ,
Paik JH, Kim TM, Heo DS, Kim CW and Jeon YK: MicroRNA-21 plays an
oncogenic role by targeting FOXO1 and activating the PI3K/AKT
pathway in diffuse large B-cell lymphoma. Oncotarget.
6:15035–15049. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Saki N, Abroun S, Soleimani M, Hajizamani
S, Shahjahani M, Kast RE and Mortazavi Y: Involvement of microRNA
in T-cell differentiation and malignancy. Int J Hematol Oncol Stem
Cell Res. 9:33–49. 2015.PubMed/NCBI
|
|
24
|
Osada H and Takahashi T: let-7 and
miR-17-92: Small-sized major players in lung cancer development.
Cancer Sci. 102:9–17. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Jin L, Lim M, Zhao S, Sano Y, Simone BA,
Savage JE, Wickstrom E, Camphausen K, Pestell RG and Simone NL: The
metastatic potential of triple-negative breast cancer is decreased
via caloric restriction-mediated reduction of the miR-17~92
cluster. Breast Cancer Res Treat. 146:41–50. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Servín-González LS, Granados-López AJ and
López JA: Families of microRNAs expressed in clusters regulate cell
signaling in cervical cancer. Int J Mol Sci. 16:12773–12790. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sylvestre Y, De Guire V, Querido E,
Mukhopadhyay UK, Bourdeau V, Major F, Ferbeyre G and Chartrand P:
An E2F/miR-20a autoregulatory feedback loop. J Biol Chem.
282:2135–2143. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Pasqualini L, Bu H, Puhr M, Narisu N,
Rainer J, Schlick B, Schäfer G, Angelova M, Trajanoski Z, Börno ST,
et al: miR-22 and miR-29a are members of the androgen receptor
cistrome modulating LAMC1 and Mcl-1 in prostate cancer. Mol
Endocrinol. 29:1037–1054. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Yang X, Du WW, Li H, Liu F, Khorshidi A,
Rutnam ZJ and Yang BB: Both mature miR-17-5p and passenger strand
miR-17-3p target TIMP3 and induce prostate tumor growth and
invasion. Nucleic Acids Res. 41:9688–9704. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wang SY, Shiboski S, Belair CD, Cooperberg
MR, Simko JP, Stoppler H, Cowan J, Carroll PR and Blelloch R:
miR-19, miR-345, miR-519c-5p serum levels predict adverse pathology
in prostate cancer patients eligible for active surveillance. PLoS
One. 9:e985972014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Pesta M, Klecka J, Kulda V, Topolcan O,
Hora M, Eret V, Ludvikova M, Babjuk M, Novak K, Stolz J and Holubec
L: Importance of miR-20a expression in prostate cancer tissue.
Anticancer Res. 30:3579–3583. 2010.PubMed/NCBI
|
|
32
|
Komatsu S, Ichikawa D, Takeshita H,
Morimura R, Hirajima S, Tsujiura M, Kawaguchi T, Miyamae M, Nagata
H, Konishi H, et al: Circulating miR-18a: A sensitive cancer
screening biomarker in human cancer. In Vivo. 28:293–297.
2014.PubMed/NCBI
|
|
33
|
Shen Z, Wu X, Wang Z, Li B and Zhu X:
Effect of miR-18a overexpression on the radiosensitivity of
non-small cell lung cancer. Int J Clin Exp Pathol. 8:643–648.
2015.PubMed/NCBI
|
|
34
|
Su ZX, Zhao J, Rong ZH, Wu YG, Geng WM and
Qin CK: Diagnostic and prognostic value of circulating miR-18a in
the plasma of patients with gastric cancer. Tumour Biol.
35:12119–12125. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Li T, Li RS, Li YH, Zhong S, Chen YY,
Zhang CM, Hu MM and Shen ZJ: miR-21 as an independent biochemical
recurrence predictor and potential therapeutic target for prostate
cancer. J Urol. 187:1466–1472. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Kobayashi N, Uemura H, Nagahama K, Okudela
K, Furuya M, Ino Y, Ito Y, Hirano H, Inayama Y, Aoki I, et al:
Identification of miR-30d as a novel prognostic maker of prostate
cancer. Oncotarget. 3:1455–1471. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Barron N, Keenan J, Gammell P, Martinez
VG, Freeman A, Masters JR and Clynes M: Biochemical relapse
following radical prostatectomy and miR-200a levels in prostate
cancer. Prostate. 72:1193–1199. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Goto Y, Kojima S, Nishikawa R, Enokida H,
Chiyomaru T, Kinoshita T, Nakagawa M, Naya Y, Ichikawa T and Seki
N: The microRNA-23b/27b/24-1 cluster is a disease progression
marker and tumor suppressor in prostate cancer. Oncotarget.
5:7748–7759. 2014. View Article : Google Scholar : PubMed/NCBI
|