Introduction
Ankylosing spondylitis (AS) is a systemic,
multifactorial, chronic rheumatic disease that affects the joints
of the axial skeleton (1). A thorough
physical examination, in conjunction with family history analysis,
consideration of the patient's individual medical history, X-ray
imaging and serum human leukocyte antigen (HLA)-B27 testing, is
required for an accurate diagnosis (2). Previous research has indicated that the
incidence of spontaneous pneumothorax in patients with AS is 0.29%,
higher than that observed in the general population (1).
Although the underlying etiology of spontaneous
pneumothorax remains unknown, it is an uncommon lung disease that
disrupts respiration in otherwise healthy men who tend to be tall
and thin (3). Spontaneous
pneumothorax results from the rupture of a subpleural emphysematous
bleb typically located at the apex of the lung, leading to the
accumulation of air in the pleural cavity (3). During the course of diagnosis and
treatment, X-ray imaging is often utilized in patients with
spontaneous pneumothorax (4).
Chronic myeloid leukemia (CML) is characterized by
the abnormal growth of mature myeloid cells; it has been associated
with translocation involving chromosomes 9 and 22, resulting in the
formation of the Philadelphia chromosome (5,6). The cause
of this translocation is unknown, although exposure to ionizing
radiation is likely to be a risk factor (7). Previous studies have demonstrated a
dose-dependent risk of CML in patients with cancer who undergo
radiation therapy (8,9) and experience repeated exposure to
diagnostic radiography (7).
Our previous report described the case of a patient
with AS who was diagnosed with CML following repeated chest
radiography and computed tomography (CT) (10); the report focused primarily on a
possible association between low-dose X-ray-derived radiation
exposure and CML. However, a recent follow-up revealed that this
patient experienced mild lower back pain as well as spontaneous
pneumothorax during the course of the disease. No prior reports
described the simultaneous occurrence of spontaneous pneumothorax
and AS followed by CML after diagnostic exposure to low-dose
X-rays. Thus, it was surmised that it was important to reanalyze
this previous case (10), and to
investigate the possible associations between spontaneous
pneumothorax and AS, and CML. The present study reviews the unusual
presence of CML following repeated diagnostic low-dose X-ray
exposure in a patient with recurrent pneumothorax and AS.
Case report
Our previous report (10) described a case of recurrent
spontaneous pneumothorax and the development of CML following
repeated exposure to low-dose diagnostic chest radiography and CT.
The findings indicated the importance of investigating the
potential dangers of low-dose diagnostic radiation. However, that
report only included follow-up information up to January 2015
(10). A more recent follow-up
revealed that the patient was diagnosed with AS one month later. As
the simultaneous occurrence of these two conditions is quite rare,
it was considered vital to reanalyze the case.
The patient was a slender man with no history of
smoking who had been diagnosed at the Department of Respiratory
Medicine, Zhejiang Provincial Hospital of Traditional Chinese
Medicine (Hangzhou, China) with spontaneous pneumothorax on May 6,
2013 at the age of 26. Following the insertion and removal of chest
tubing, the patient was discharged from hospital. However, the
patient then developed recurrent pneumothorax. On May 24, 2013, the
patient underwent thoracoscopic surgery for the resection of
bullae. Over the 9 months following the initial diagnosis of
spontaneous pneumothorax, the patient underwent 10 radiographic
examinations and 4 CT scans of the chest, constituting a total
effective radiation dose of 11.7 mSv. On April 18, 2014 a general
health examination revealed that the patient's white blood cell
(WBC) count had increased to 13.9×109/l (normal range,
4–10×109/l). On June 6, 2014, the patient's WBC count
had increased to 25.4×109/l. Following bone marrow smear
testing on June 13 2014 and a karyotype analysis on June 19, 2014
the patient was diagnosed with CML (10).
On June 28, 2014, the patient began receiving
imatinib mesylate at a dose of 400 mg/day for the treatment of CML.
A WBC count revealed that the abnormally high WBC count had begun
to decrease on September 4, 2014. An additional karyotype analysis
was subsequently performed (Table I)
and a second bone marrow smear test on May 5, 2015 revealed no
abnormal cells.
 | Table I.Karyotype analysis of the patient. |
Table I.
Karyotype analysis of the patient.
| Date | BCR/ABL1a (p210) | BCR/ABL1 (copy) | ABL1 (copy) | BCR-ABL1/ABL1 | IS BCR-ABL1/ABL1 |
|---|
| Jun 19 2014 | + | −(P230) | − | − | − |
| Feb 13 2015 | + | 61.26 |
1.79×104 | 0.003 | 0.003 |
| Jun 25 2015 | − | − |
1.63×104 | 0 | 0 |
| Oct 19 2015 | − | − |
3.26×104 | 0 | 0 |
The patient continued to receive imatinib mesylate
until June 2016. As of January 2015 he had reported no feelings of
discomfort, as previously described (10). However, the patient did report
bilateral sacroiliac joint pain in February 2015. Careful inquiry
revealed that the patient had begun to feel intermittent, mild
bilateral sacroiliac joint pain as early as January 2014, 6 months
prior to the initiation of imatinib treatment. However, the patient
had not noted this information because symptoms were mild.
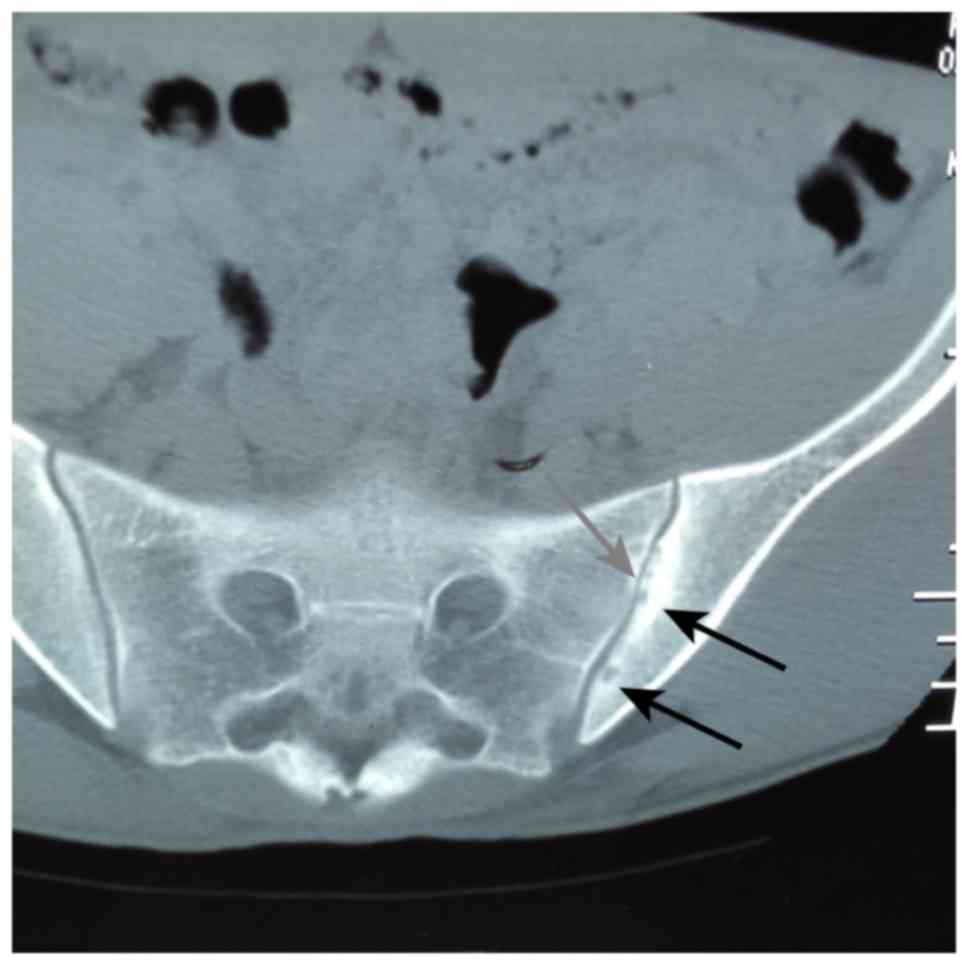
Although the risk of developing CML following
repeated exposure to chest radiography and CT was of concern, a
pelvic CT scan was ultimately performed on February 16, 2015 to
confirm the diagnosis of AS (Fig. 1).
The scan revealed bilateral narrowing of the sacroiliac joints in
addition to bilateral cystic changes, which were more apparent at
the surface of the left sacroiliac joint.
Joint pain, muscle pain and muscle cramps are known
potential side effects of imatinib. In the current case, the
location and nature of the pain had not changed after receiving
imatinib for 6 months. Moreover, a pelvic CT scan was performed 7
months after the initiation of imatinib treatment. To the best of
our knowledge, there have been no prior reports of imatinib
resulting in AS, thus we hypothesize that AS occurred before the
patient was administered imatinib.
The patient tested negative for HLA-B27 and
rheumatoid factor, but a diagnosis of AS was reached in accordance
with the New York criteria (11). The
occurrence of pneumothorax and the subsequent occurrence of CML and
AS were documented within the same 2-year period. The Institutional
Ethics Committee of the Zhejiang Provincial Hospital of Traditional
Chinese Medicine (Hangzhou, China) approved the current study. The
subject of this case report provided written informed consent
agreeing to publication.
Discussion
The present study describes the case of a
29-year-old man who presented with recurrent spontaneous
pneumothorax, then AS, and who subsequently developed CML following
repeated exposure to low-dose diagnostic X-ray radiation. To the
best of our knowledge, these combined medical conditions have not
been previously reported in the clinical literature.
The patient visited the physician due to
pneumothorax; initially, only chest CT scans and chest X-ray data
were available. Pelvic CT scanning was not conducted until February
16th, 2015, when it was performed to confirm the diagnosis of AS
(Fig. 1). That scan revealed the
bilateral narrowing of the sacroiliac joints, in addition to
bilateral cystic changes, which were more apparent at the surface
of the left sacroiliac joint. The possibility that imatinib caused
the occurrence of AS was rejected for the following reasons.
Firstly, neither the location nor the nature of the pain changed;
secondly, following commencement of imatinib treatment there were
no evident changes in the patient's symptoms: Thirdly, the pelvic
CT scan was performed just 7 months after the initiation of
imatinib treatment; lastly, as no reports of imatinib-induced AS
could be located in the literature, we considered this eventuality
to be unlikely.
In the majority of cases of unclear etiology,
spontaneous pneumothorax is reported in healthy young men and stems
from the rupture of apical blebs on the visceral pleura (3). Lee et al (1) reported that the incidence of spontaneous
pneumothorax in patients with AS is 0.29% (n=1,028), higher than
that reported for the general population. Although rare, the
development of apical pulmonary fibrosis and bullous disease has
been recognized as an extra-articular manifestation of AS (12). Studies have also demonstrated that
recurrent pneumothorax may be caused by the inadequate sealing of
air leaks, and that this can be responsible for the persistence of
pneumothorax in patients with connective tissue autoimmune
diseases, including AS (1,13).
In prior reports involving AS and concurrent
pneumothorax, the pneumothorax was diagnosed a number of years
(4–30 years) following the diagnosis of AS (1,14,15). In one previously reported case study,
the pneumothorax was diagnosed 16 months after radiation exposure
(16). However, the current patient
presented with recurrent spontaneous pneumothorax prior to a
diagnosis of AS. Notably, previous studies have indicated that the
incidence of occult pneumothorax may be underestimated in patients
with AS, owing to the vague nature of the symptoms or lack of
diagnosis (1,12). Thus, patients with recurrent
spontaneous pneumothorax should be thoroughly evaluated for AS.
Specific studies have suggested that rheumatic
diseases may develop during the course of CML, although it remains
unclear whether the development of rheumatic disease in patients
with CML is due to the long-term use of drugs or the underlying
disease (17,18). AS is unlikely to be caused by drugs;
however, it is imperative to bear in mind that AS, an autoimmune
and inflammatory disease, may impair immune function and render
patients susceptible to diseases stemming from gene mutations
(19). A previous study described a
case of CML in a patient with AS following multiple CT imaging
sessions (20). Although few reports
have documented an association between AS and the development of
CML following exposure to low-dose radiation, studies indicate that
the risk of hematopoietic cancer is increased in patients with AS
(21). The aforementioned findings,
together with those of the current case report, indicate that
patients with AS may be susceptible to the development of CML
following low doses of radiation compared with healthy
individuals.
Although blood tests for HLA-B27 are positive in
>90% of Chinese patients with AS (22), the present patient tested negative for
HLA-B27. Numerous studies have also failed to detect an association
between HLA-B27 in AS and spontaneous pneumothorax (1,12,14,15). Thus,
whether patients with AS who test negative for HLA-B27 are more
sensitive to X-ray damage remains to be elucidated. In addition,
the potential contributions of sex, age and smoking history to the
development of pneumothorax have been reported (1,12,14,15).
Therefore, the evidence accumulated to date indicates that further
research into the association between spontaneous pneumothorax and
sensitivity to radiation in patients with AS and CML is
required.
Acknowledgements
The authors would like to thank the National Natural
Science Foundation of China, Beijing, China for supporting the
present study (grant no. 81400107).
Glossary
Abbreviations
Abbreviations:
|
AS
|
ankylosing spondylitis
|
|
CML
|
chronic myeloid leukemia
|
|
CT
|
computed tomography
|
|
WBC
|
white blood cell
|
References
|
1
|
Lee CC, Lee SH, Chang IJ, Lu TC, Yuan A,
Chang TA, Tsai KC and Chen WJ: Spontaneous pneumothorax associated
with ankylosing spondylitis. Rheumatology (Oxford). 44:1538–1541.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Boos N and Aebi M: Spinal Disorders:
Fundamentals of Diagnosis and Treatment. Springer Science+Business
Media B.V.; Dorhrecht, The Netherlands: 2008, View Article : Google Scholar
|
|
3
|
Noppen M: Spontaneous pneumothorax:
Epidemiology, pathophysiology and cause. Eur Respir Rev.
19:217–219. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sahn SA and Heffner JE: Spontaneous
pneumothorax. N Engl J Med. 342:868–874. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Konopka JB, Watanabe SM, Singer JW,
Collins SJ and Witte ON: Cell lines and clinical isolates derived
from Ph1-positive chronic myelogenous leukemia patients express
c-abl proteins with a common structural alteration. Proc Natl Acad
Sci USA. 82:pp. 1810–1814. 1985, View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Davis RL, Konopka JB and Witte ON:
Activation of the c-abl oncogene by viral transduction or
chromosomal translocation generates altered c-abl proteins with
similar in vitro kinase properties. Mol Cell Biol. 5:204–213. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Preston-Martin S, Thomas DC, Yu MC and
Henderson BE: Diagnostic radiography as a risk factor for chronic
myeloid and monocytic leukaemia (CML). Br J Cancer. 59:639–644.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Penfold JB and Rhys-Lewis RD: Leukaemia,
amyloidosis, and renal vein thrombosis in irradiated ankylosing
spondylitis. Br Med J. 2:1034–1036. 1957. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Court-Brown WM and Doll R: Leukaemia and
aplastic anaemia in patients irradiated for ankylosing spondylitis.
1957. J Radiol Prot. 27:B15–B154. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ju FH, Gong XB, Jiang LB, Hong HH, Yang
JC, Xu TZ, Chen YU and Wang Z: Chronic myeloid leukaemia following
repeated exposure to chest radiography and computed tomography in a
patient with pneumothorax: A case report and literature review.
Oncol Lett. 11:2398–2402. 2016.PubMed/NCBI
|
|
11
|
van der Linden S, Valkenburg HA and Cats
A: Evaluation of diagnostic criteria for ankylosing spondylitis. A
proposal for modification of the New York criteria. Arthritis
Rheum. 27:361–368. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Rosenow E, Strimlan CV, Muhm JR and
Ferguson RH: Pleuropulmonary manifestations of ankylosing
spondylitis. Mayo Clin Proc. 52:641–649. 1977.PubMed/NCBI
|
|
13
|
Lawrence RC, Hochberg MC, Kelsey JL,
McDuffie FC, Medsger TA Jr, Felts WR and Shulman LE: Estimates of
the prevalence of selected arthritic and musculoskeletal diseases
in the United States. J Rheumatol. 16:427–441. 1989.PubMed/NCBI
|
|
14
|
Ersoy E, Akgol G and Ozgocmen S: Bilateral
spontaneous pneumothorax in a patient with longstanding ankylosing
spondylitis. Acta Reumatol Port. 39:353–354. 2014.PubMed/NCBI
|
|
15
|
Wang CT, Tsen JC, Lin HJ and Cheng HH:
Bilateral spontaneous pneumothorax in a patient with ankylosing
spondylitis. Eur J Emerg Med. 14:123–124. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bhardwaj H, Bhardwaj B and Youness HA: A
case of spontaneous pneumothorax following radiation therapy for
non-small cell lung cancer. Lung India. 30:360–362. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Senel S, Kaya E, Aydogdu I, Erkurt MA and
Kuku I: Rheumatic diseases and chronic myelogenous leukemia,
presentation of four cases and review of the literature. Rheumatol
Int. 26:857–861. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sacchi S, Kantarjian H, O'Brien S, Cohen
PR, Pierce S and Talpaz M: Immune-mediated and unusual
complications during interferon alfa therapy in chronic myelogenous
leukemia. J Clin Oncol. 13:2401–2407. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Linet MS, Slovis TL, Miller DL, Kleinerman
R, Lee C, Rajaraman P and de Gonzalez Berrington A: Cancer risks
associated with external radiation from diagnostic imaging
procedures. CA Cancer J Clin. 62:75–100. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ben Abdelghani K, El Menaa M, Ben
Abdelghani K, Souabni L, Belhadj S, Chekili S, Laatar A and
Zakraoui L: Chronic myeloid leukemia and ankylosing spondylitis.
Tunis Med. 90:9012012.PubMed/NCBI
|
|
21
|
Thomas E, Brewster DH, Black RJ and
Macfarlane GJ: Risk of malignancy among patients with rheumatic
conditions. Int J Cancer. 88:497–502. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ho HH and Chen JY: Ankylosing spondylitis:
Chinese perspective, clinical phenotypes, and associated
extra-articular systemic features. Curr Rheumatol Rep. 15:3442013.
View Article : Google Scholar : PubMed/NCBI
|