Introduction
Breast cancer is a heterogeneous disease and divided
into different subtypes according to estrogen receptor (ER),
progesterone receptor (PR), and human epidermal growth factor
receptor 2 (HER2) status (1,2). Triple-negative breast cancer (TNBC),
which is characterized by the lack of ER, PR and HER2 expression,
has attracted substantial attention (3,4). There is
a significant overlap between TNBC and basal-like breast cancer.
Therefore, TNBC and basal-like breast cancer are frequently
regarded as synonymous (5,6). TNBC is assessed by immunohistochemistry,
and basal-like breast cancer is identified using gene expression
profiling (7). TNBCs are fast-growing
tumors and tend to metastasize compared with other types of breast
cancer (8). TNBC has consistently
been associated with poor clinical outcomes in radical mastectomy
due to its invasive characteristics, and poor response to hormone
therapy and HER2-targeted therapy (9–11).
Similar survival rates of women following
breast-conserving treatment (BCT) and radical mastectomy have been
demonstrated (12,13). Consequently, BCT has become a
preferable option for early stage breast cancer patients (14). However, due to the aggressive
characteristics of TNBC, whether patients with TNBC are suitable
for BCT remains controversial. A number of studies have reported
that following BCT women with TNBC had a higher rate of local
failure compared with women with other breast cancer subtypes
(15,16). Investigators reported that TNBC was
associated with an increased risk of distant metastasis, but it was
not associated with increased locoregional recurrence (LRR)
(17). However, Millar et al
(18) reported that there was no
increase in distant metastasis risk following BCT in patients with
TNBC compared with patients with other breast cancer phenotypes.
Additionally, Gangi et al (19) demonstrated that patients with TNBC
were not associated with increased local relapse compared with
patients with non-TNBC subtypes following BCT; however, they found
that the TNBC phenotype was associated with shorter overall
survival (OS).
Taken together, the role of TNBC in BCT remains
unclear. The outcomes of patients with TNBC following BCT have not
been well described. Therefore, an investigation was conducted to
retrospectively compare the 5-year outcomes of women with TNBC to
women with other subtypes breast cancer following BCT and to
evaluate the prognostic value of TNBC in patients with BCT.
Patients and methods
Patients
Between January 2002 and March 2010, a total of 757
patients with early-stage breast cancer treated with BCT at Tianjin
Medical University Cancer Institute and Hospital were identified to
meet the inclusion criteria. The inclusion criteria were as
follows: i) Full details of ER, PR and HER2 status and ii) patients
had with stage I/II/III breast cancer and treated by lumpectomy.
Exclusion criteria included: i) males with breast cancer; ii) T4
disease; iii) stage IV disease; iv) previously underwent mastectomy
and v) unknown ER, PR or HER2 status. Data collected included
standard prognostic factors, such as age, menopausal status, tumor
size, lymph node, ER, PR, and HER2 status, histological grade, date
of surgery, adjuvant treatment received, time of LRR and metastatic
progression, date of last follow-up (March 2015) and mortality. In
the present study, the age of breast cancer patients ranged between
19 and 83 years, and the median age was 45 years. The pathological
samples were taken as part of routine examination and biopsy, and
the specimens were obtained on the day of operation performed, the
number of specimens obtained varied between 6 and 20, according to
different circumstances. The patients were staged using the sixth
edition of the American Joint Committee on Cancer (AJCC) staging
manual (20). The Elston-Ellis
modification of Scarff-Bloom-Richardson (SBR) grading system was
used for histological grade of breast cancer (21). Negative pathological margins were
defined as no invasive carcinoma or ductal carcinoma in situ
(DCIS) present at the margins; positive margins were defined as the
presence of invasive carcinoma or DCIS at the margin. Ethical
approval was obtained from the Tianjin Medical University Hospital
(grant no. bc2017008), and written informed consent was obtained
from all patients.
Formalin-fixed paraffin-embedded
tissues
Samples obtained from each patient were
formalin-fixed and paraffin-embedded as part of routine
examination. In the study, a 4-mm-thick tissue specimen was cut
from breast tumor for formalin fixation processes. Each sample was
placed into standard tissue cassettes and completely submerged in a
container filled with 4% neutral buffered formaldehyde for 24 h at
room temperature. The formaldehyde-fixed samples were embedded in
paraffin after stepwise dehydration in 70, 80, 90 and 99% ethanol,
followed by isopropanol and xylene.
Immunohistochemistry (IHC) and
fluorescent in situ hybridization (FISH)
IHC and FISH analysis were conducted on tissue
sections (3–4 µm) and tissue microarray slides. IHC (Benchmark XT;
Ventana Medical Systems, Inc., Tucson, AZ, USA) was performed on
formalin-fixed and paraffin-embedded tissues of 757 patients using
the avidin-biotin-immunoperoxidase technique (22). Tissue sections were deparaffinized in
xylene and rehydrated in a graded series of ethanol.
Antigen-retrieval was performed in citrate buffer (pH 6.0) at 120°C
for 2.5 min. Subsequently, the slides were exposed to 3% hydrogen
peroxide for 20 min and washed with PBS for 5 min 3 times. The
further blocking of tissues was performed with normal goat serum
(Abcam Inc., Cambridge, UK) for 30 min at room temperature. The
sections were then incubated overnight at 4°C with the following
primary antibodies: ER (cat no. NCL-L-PGR-312; dilution, 1:100), PR
(cat no. NCL-L-ER-6F11; dilution, 1:80) (both Novocastra; Leica
Biosystems GmbH, Wetzlar, Germany), HER2 (cat no. 800-2996;
dilution 1:300; Ventana Medical Systems, Inc.). Following 5 washes
with PBS, the slides were incubated with biotin-conjugated
secondary antibody (cat no. ZB-2010; dilution, 1:200; OriGene
Technologies, Inc., Beijing, China) for 30 min at room temperature.
The sections with positive expression level was used as the
positive control, the negative control was established with the
primary antibody replaced by PBS. Detection was done by utilizing
iView DAB Detection kit (Ventana Medical Systems, Inc.).
FISH analysis was conducted in line with the
protocol of Abbott/Vysis PathVysion HER2 DNA Probe kit (cat no.
30161060/02J01-030; Abbott Molecular, Inc., Des Plaines, IL, USA),
the Spectrum Orange fluorophore-labeled DNA probe and Spectrum
Green fluorophore-labeled α-satellite DNA probes from this kit were
used to assess the HER2 gene locus and chromosome 17, respectively.
In total, 2 separate fields of ≥20 cells were counted and the
average of the results of the selected tumor areas were used to
calculate mean gene and chromosome 17 counts, which were used to
calculate the ratio of HER2:CEP17 signal. Tumor cells from matching
sites of IHC were scored for the number of red (HER2) and green
(chromosome 17) signals. The slides were evaluated using an Olympus
BX51 microscope (Olympus Corporation, Tokyo, Japan) with an
oil-immersion objective lens and an appropriate filter set at a
magnification of ×100. Immunoreactivity was assessed independently
by ≥2 pathologists.
Subtype definitions
The patients were divided into three subtypes
according to receptor expression: i) Luminal: ER or PR-positive,
ii) HER2-enriched: ER and PR-negative but HER2 receptor-positive
and iii) TNBC:ER, PR and HER2-negative. ER, PR and HER2 data were
obtained through routine clinical testing. The samples were defined
as ER or PR-positive if >1% of the cells were positive for
immunohistostaining. HER2 immunoreactivity was assessed using a
standardized score from 0–3, based on the intensity of staining of
the cell membrane and the proportion of tumor cells stained. The no
staining or <10% of tumor cells was estimated as negative
(score, 0), the weak and incomplete staining of the membrane in
>10% of tumor cells was considered negative (score, 1+), the
weak to moderate complete staining of the membrane in >10% tumor
cells was evaluated as 2+, and strong complete staining of the
membrane in >10% of tumor cells was determined to be positive
(score, 3+). Samples with 2+ were needed to be detected by FISH
test, and the HER2 gene was considered to be amplified when the
ratio of HER2:CEP17 in tumor cells was >2.0. Patients with
negative ER and PR status and HER2 immunohistostaining score of 2+
but no fluorescence in situ hybridization results were
excluded in the present analysis.
Treatment delivery
All patients in the present study were treated
surgically with breast-conserving surgery. A total of 675 patients
had completed breast radiation therapy. Breast plus supraclavicular
fossa radiation therapy was performed on 61 patients. A total of 21
patients did not undergo radiation treatment. Adjuvant systemic
chemotherapy and hormone therapy were performed according to
standard practices during that time interval. The majority of
patients in the present study received anthracycline/taxane-based
or cyclophosphamide, methotrexate and 5-fluorouracil chemotherapy
regimens, and a minority of patients chose other chemotherapy
regimens. It was recommended that patients with ER- and/or
PR-positive disease who were premenopausal received tamoxifen
treatment; postmenopausal patients chose aromatase inhibitors. Of
the 757 patients with breast cancer, 717 received adjuvant systemic
chemotherapy and 493 received hormone therapy. In total, 3 patients
in the present study received trastuzumab therapy (data not
shown).
Follow-up and outcomes
Follow-up has been maintained by reviewing clinical
charts and by contacting patients by telephone or mail. Factors
analyzed included clinical (age, menopause status,
tumor-node-metastasis stage, tumor size), pathological (lymph node
status, histological grade, pathological subtype and final margin
status) and treatment (systemic therapy). The end-point of the
present study was 5-year LRR, distant metastasis or mortality, and
the study was ended when breast cancer mortality occurred. Total
recurrence referred to LRR or distant metastasis. LRR-free survival
(LRFS) was defined as the time from diagnosis to development of LRR
(recurrence within the breast and regional relapse, including
ipsilateral supraclavicular fossa, axilla or internal mammary lymph
nodes). Distant metastasis-free survival (DMFS) was defined as the
time from pathological diagnosis to the time from first evidence of
distant metastasis. Disease-free survival (DFS) defined as the time
of diagnosis to development of first evidence of metastasis or LRR.
OS was defined as from the time of diagnosis to last follow-up or
time of mortality from breast cancer (patients who succumbed to
other causes were considered censored from the time of
mortality).
Statistical analysis
All statistical analyses were carried out using SPSS
17.0 (SPSS, Inc., Chicago, IL, USA). The Kaplan-Meier method was
used for univariate analysis and calculating LRFS, DMFS, DFS and
OS, and the significance was assessed using the log-rank test. Cox
proportional hazards regression analysis was used for multivariate
analysis. Factors with a significance of P<0.10 in univariate
analysis were included in the multivariate Cox model. Differences
between categorical variables were calculated using the
χ2 test. P<0.05 was considered to indicate a
statistically significant difference.
Results
Patients
Of the 757 patients diagnosed with early breast
cancer and treated with BCT in whom the status of all three markers
(ER, PR, and HER2) were available, 541 (71.5%) were sorted as
luminal subtype, 66 (8.7%) were defined as HER2-enriched subtype
and 150 (19.8%) were classified as TNBC subtype (Table I). The follow-up time ranged from 13
to 157 months, and the median follow-up time was 83 months. The
5-year LRFS, DMFS, DFS and OS for the whole cohort were 96.2, 94.3,
92.9 and 96.7%, respectively.
 | Table I.Distribution of clinical and
treatment characteristics among different types patients with
breast-conserving treatment. |
Table I.
Distribution of clinical and
treatment characteristics among different types patients with
breast-conserving treatment.
| Parameters | Luminal, n (%) | HER2-enriched, n
(%) | TNBC, n (%) | P-value |
|---|
| Total | 541 (71.5) | 66 (8.7) | 150 (19.8) |
|
| Age at diagnosis,
years |
|
|
| 0.016 |
|
≤35 | 71 (13.1) | 18 (27.3) | 29 (19.3) |
|
|
36–55 | 368 (68.0) | 39 (59.1) | 100 (66.7) |
|
|
>55 | 102 (18.9) | 9 (13.6) | 21 (14.0) |
|
| Menopausal
status |
|
|
| 0.676 |
|
Premenopausal | 369 (68.2) | 48 (72.7) | 100 (66.7) |
|
|
Postmenopausal | 172 (31.8) | 18 (27.3) | 50 (33.3) |
|
| Number of positive
LNs |
|
|
| 0.937 |
| 0 | 421 (77.8) | 54 (81.8) | 119 (79.3) |
|
|
1–3 | 97 (17.9) | 10 (15.2) | 26 (17.3) |
|
| ≥4 | 23 (4.3) | 2 (3.0) | 5 (3.3) |
|
| Tumor size, cm |
|
|
| 0.316 |
| T1
(≤2) | 378 (69.9) | 41 (62.1) | 93 (62.0) |
|
| T2
(>2, ≤5) | 145 (26.8) | 22 (33.3) | 49 (32.7) |
|
| T3
(>5) | 18 (3.3) | 3 (4.6) | 8 (5.3) |
|
| TNM stage |
|
|
| 0.601 |
| I | 321 (59.3) | 35 (53.1) | 81 (54.0) |
|
| II | 196 (36.2) | 29 (43.9) | 61 (40.7) |
|
|
III | 24 (4.5) | 2 (3.0) | 8 (5.3) |
|
| Pathological
subtype |
|
|
| 0.566 |
|
IDC | 396 (73.2) | 50 (75.8) | 116 (77.3) |
|
|
Other | 145 (26.8) | 16 (24.2) | 34 (22.7) |
|
| Histological
grade |
|
|
| <0.001 |
| I | 106 (19.6) | 5 (7.6) | 16 (10.7) |
|
| II | 344 (63.6) | 41 (62.1) | 81 (54.0) |
|
|
III | 45 (8.3) | 11 (16.7) | 41 (27.3) |
|
|
Unknown | 46 (8.5) | 9 (13.6) | 12 (8.0) |
|
| Margin status |
|
|
| 0.230 |
|
Positive | 12 (2.2) | 0 (0.0) | 1 (0.7) |
|
|
Negative | 529 (97.8) | 66 (100.0) | 149 (99.3) |
|
| Chemotherapy |
|
|
| 0.021 |
|
CMF | 89 (16.4) | 21 (31.8) | 23 (15.3) |
|
|
A/T | 404 (74.7) | 39 (59.1) | 119 (79.4) |
|
|
Other | 15 (2.8) | 2 (3.0) | 5 (3.3) |
|
| No | 33 (6.1) | 4 (6.1) | 3 (2.0) |
|
| Radiation |
|
|
| 0.138 |
|
Breast | 477 (88.2) | 58 (87.8) | 140 (93.3) |
|
| Breast
and SCF | 48 (8.9) | 4 (6.1) | 9 (6.0) |
|
| No | 16 (2.9) | 4 (6.1) | 1 (0.7) |
|
| Hormone
therapy |
|
|
| <0.001 |
|
Yes | 484 (89.5) | 3 (4.5) | 6 (4.0) |
|
| No | 18 (3.3) | 63 (95.5) | 144 (96.0) |
|
|
Unknown | 39 (7.2) | 0 (0.0) | 0 (0.0) |
Clinicopathological characteristics
according to different subtypes
Patient characteristics and results of statistical
comparisons according to different breast cancer subtypes were
summarized in Table I. The
distribution of young patients (≤35 years) was significantly
different between luminal (13.1%), HER2-enriched (27.3%) and TNBC
(19.3%) subtypes, (P=0.016; Table I).
Patients with TNBC were more likely to have histological grade III
tumors (27.3%) compared with the luminal (8.3%) and HER2 (16.7%)
subtypes (P<0.001; Table I).
Selection of chemotherapy treatment was also different among the 3
groups (P=0.021; Table I).
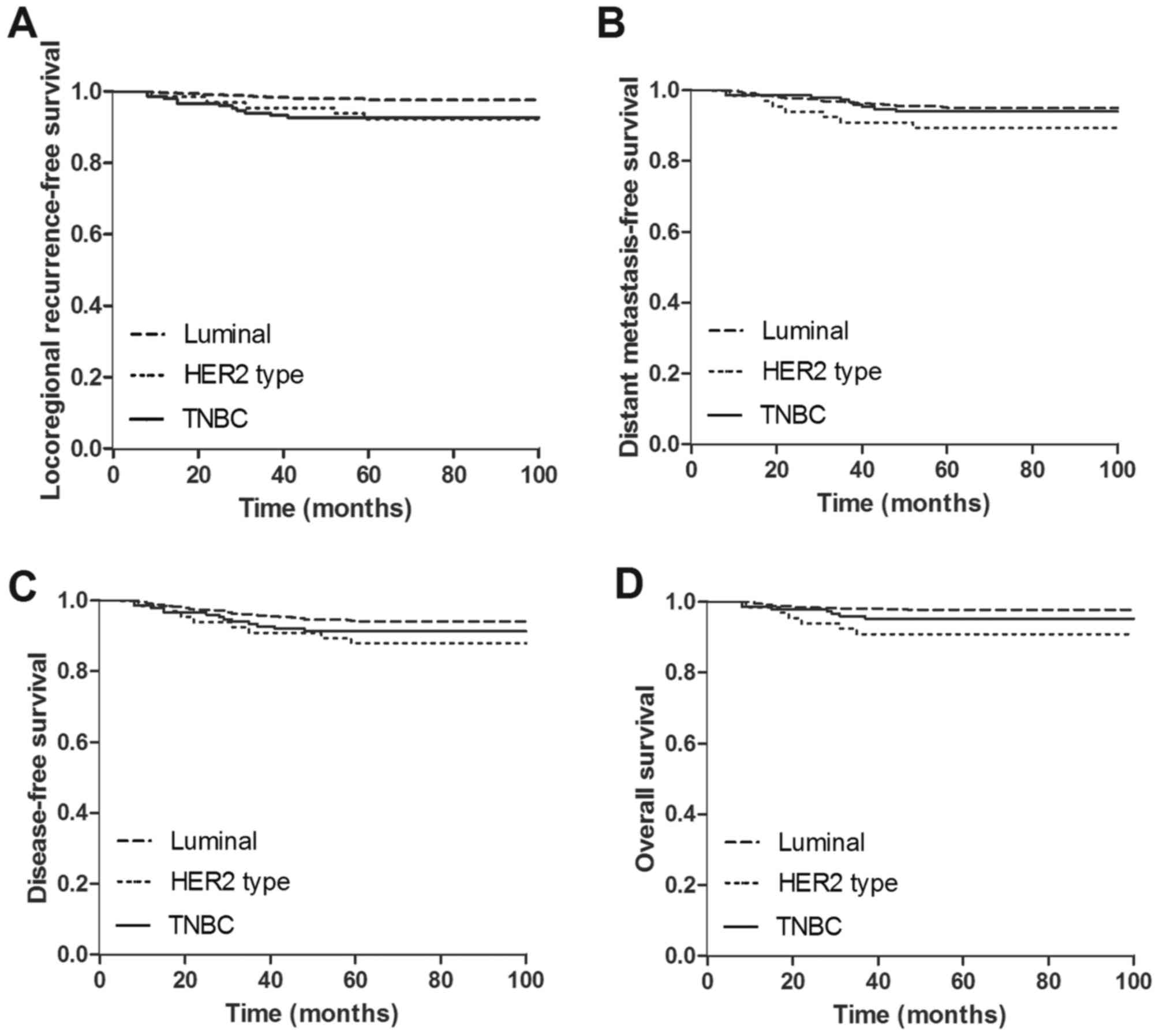
5-year outcomes of breast cancer
patients following BCT according to different subtypes
The 5-year outcomes of the three different breast
cancer subtypes following BCT were different. The rate of 5-year
LRR was significantly different between luminal (2.4%),
HER2-enriched (7.6%) and TNBC (7.3%) groups (P=0.005; Table II). The rate of 5-year mortality was
2.2, 9.1 and 4.7% for luminal, HER2-enriched and TNBC, respectively
(P=0.007; Table II). There was no
significant difference in the rates of distant metastases (P=0.164)
and total relapse (P=0.138; Table
II). The 5-year LRFS was 97.6, 92.4 and 92.7% for luminal,
HER2-enriched and TNBC groups, respectively (P=0.005; Fig. 1A). The 5-year DMFS was 95.0, 89.4 and
94.0% for luminal, HER2-enriched and TNBC groups, respectively
(P=0.164; Fig. 1B). The 5-year DFS
was 93.9, 87.9 and 91.3% for luminal, HER2-enriched and TNBC
groups, respectively (P=0.138; Fig.
1C). The 5-year OS was 97.8, 90.9 and 95.3% for luminal,
HER2-enriched and TNBC groups, respectively (P=0.007; Fig. 1D).
| Table II.5-year outcomes of different subtype
breast cancer patients with breast-conserving treatment. |
Table II.
5-year outcomes of different subtype
breast cancer patients with breast-conserving treatment.
| Parameters | Luminal, n (%) | HER2 type, n
(%) | TNBC, n (%) | P-value |
|---|
| Total | 541 (71.5) | 66 (8.7) | 150 (19.8) |
|
| LRR |
|
|
| 0.005 |
|
Yes | 13 (2.4) | 5 (7.6) | 11 (7.3) |
|
| No | 528 (97.6) | 61 (92.4) | 139 (92.7) |
|
| Distant
metastases |
|
|
| 0.164 |
|
Yes | 27 (5.0) | 7 (10.6) | 9 (6.0) |
|
| No | 514 (95.0) | 59 (89.4) | 141 (94.0) |
|
| Total relapse |
|
|
| 0.138 |
|
Yes | 33 (6.1) | 8 (12.1) | 13 (8.7) |
|
| No | 508 (93.9) | 58 (87.9) | 137 (91.3) |
|
| Mortality |
|
|
| 0.007 |
|
Yes | 12 (2.2) | 6 (9.1) | 7 (4.7) |
|
| No | 529 (97.8) | 60 (90.9) | 143 (95.3) |
|
Univariate analysis of the prognostic
factors associated with 5-year outcomes of patients following
BCT
The prognostic factors associated with 5-year LRFS,
DMFS, DFS and OS in the whole cohort of patients following BCT were
evaluated by univariate analysis. The results indicated that margin
status (P=0.021), radiation therapy (P=0.031) and hormone therapy
(P=0.008) may be associated with LRFS (Table III). Menopausal status (P=0.032),
histological grade (P=0.049), margin status (P=0.004), chemotherapy
treatment (P=0.001) and radiotherapy (P<0.001) may be prognostic
factors for DMFS. Age at breast cancer diagnosis (P=0.029),
histological grade (P=0.018), margin status (P<0.001),
chemotherapy treatment (P=0.015), radiation therapy (P<0.001)
and hormone therapy (P=0.046) may be associated with DFS. Factors
associated with OS may be chemotherapy treatment (P=0.011),
radiation therapy (P<0.001) and hormone therapy (P=0.026;
Table III).
| Table III.Univariate analysis of
clinicopathological parameters for 5-year LRFS, DMFS, DFS and OS of
patients with BCT. |
Table III.
Univariate analysis of
clinicopathological parameters for 5-year LRFS, DMFS, DFS and OS of
patients with BCT.
|
|
| LRFS | DMFS | DFS | OS |
|---|
|
|
|
|
|
|
|
|---|
|
Characteristics | n | % | P-value | % | P-value | % | P-value | % | P-value |
|---|
| Age at diagnosis,
years |
|
| 0.054 |
| 0.142 |
| 0.029 |
| 0.256 |
|
≤35 | 118 | 92.4 |
| 92.4 |
| 88.1 |
| 94.9 |
|
|
36–55 | 507 | 97.0 |
| 95.5 |
| 94.5 |
| 97.4 |
|
|
>55 | 132 | 96.2 |
| 91.7 |
| 90.9 |
| 95.5 |
|
| Menopausal
status |
|
| 0.458 |
| 0.032 |
| 0.075 |
| 0.362 |
|
Premenopausal | 517 | 96.5 |
| 95.6 |
| 94.0 |
| 97.1 |
|
|
Postmenopausal | 240 | 95.4 |
| 91.7 |
| 90.4 |
| 95.8 |
|
| Number of positive
LNs |
|
| 0.176 |
| 0.169 |
| 0.071 |
| 0.177 |
| 0 | 594 | 96.5 |
| 95.1 |
| 93.9 |
| 97.3 |
|
|
1–3 | 133 | 96.2 |
| 91.0 |
| 89.5 |
| 94.7 |
|
| ≥4 | 30 | 90.0 |
| 93.3 |
| 86.7 |
| 93.3 |
|
| Tumor size, cm |
|
| 0.120 |
| 0.191 |
| 0.163 |
| 0.225 |
| T1
(≤2) | 512 | 96.1 |
| 93.4 |
| 92.4 |
| 96.3 |
|
| T2
(>2, ≤5) | 216 | 97.2 |
| 96.8 |
| 94.9 |
| 98.1 |
|
| T3
(>5) | 29 | 89.7 |
| 93.1 |
| 86.2 |
| 93.1 |
|
| TNM stage |
|
| 0.246 |
| 0.995 |
| 0.502 |
| 0.667 |
| I | 437 | 96.1 |
| 94.3 |
| 93.4 |
| 96.8 |
|
| II | 286 | 96.9 |
| 94.4 |
| 92.7 |
| 96.9 |
|
|
III | 34 | 91.2 |
| 94.1 |
| 88.2 |
| 94.1 |
|
| Pathological
subtype |
|
| 0.814 |
| 0.282 |
| 0.553 |
| 0.807 |
|
IDC | 562 | 96.3 |
| 93.8 |
| 92.5 |
| 96.8 |
|
|
Other | 195 | 95.9 |
| 95.9 |
| 93.8 |
| 96.4 |
|
| Histological
grade |
|
| 0.061 |
| 0.049 |
| 0.018 |
| 0.193 |
| I | 127 | 98.4 |
| 98.4 |
| 96.9 |
| 99.2 |
|
| II | 466 | 96.4 |
| 93.6 |
| 92.7 |
| 96.1 |
|
|
III | 97 | 91.8 |
| 90.7 |
| 86.6 |
| 94.8 |
|
|
Unknown | 67 | 97.0 |
| 97.0 |
| 95.5 |
| 98.5 |
|
| Margin |
|
| 0.021 |
| 0.004 |
| <0.001 |
| 0.338 |
|
Positive | 13 | 84.6 |
| 76.9 |
| 61.5 |
| 92.3 |
|
|
Negative | 744 | 96.4 |
| 94.6 |
| 93.4 |
| 96.8 |
|
| Chemotherapy |
|
| 0.558 |
| 0.001 |
| 0.015 |
| 0.011 |
|
CMF | 133 | 95.5 |
| 92.5 |
| 91.0 |
| 96.2 |
|
|
A/T | 562 | 96.6 |
| 95.9 |
| 94.3 |
| 97.5 |
|
|
Other | 22 | 95.5 |
| 81.8 |
| 85.0 |
| 92.5 |
|
|
None | 40 | 92.5 |
| 85.0 |
| 81.8 |
| 86.4 |
|
| Radiation |
|
| 0.031 |
| <0.001 |
| <0.001 |
| <0.001 |
|
Breast | 675 | 96.4 |
| 95.3 |
| 94.1 |
| 97.2 |
|
| Breast
and SCF | 61 | 96.7 |
| 91.8 |
| 88.5 |
| 96.7 |
|
| No | 21 | 85.7 |
| 71.4 |
| 66.7 |
| 81.0 |
|
| Hormone
therapy |
|
| 0.008 |
| 0.200 |
| 0.046 |
| 0.026 |
|
Yes | 493 | 97.6 |
| 95.3 |
| 94.3 |
| 98.0 |
|
| No | 225 | 92.9 |
| 92.0 |
| 89.3 |
| 94.2 |
|
|
Unknown | 39 | 97.4 |
| 94.9 |
| 94.9 |
| 94.9 |
|
Multivariate analysis of prognosis of
TNBC for patients following BCT within 5 years
Multivariate Cox regression analysis included
molecular subtype, age at diagnosis, menopausal status, lymph node
status, histological grade, margin status, chemotherapy treatment,
radiation and hormone therapy. Compared with patients with TNBC,
the luminal subtype was not associated with a significant lower
risks in LRR [hazard ratio (HR), 0.316; 95% confidence interval
(CI), 0.043–2.317; P=0.257; Table
IV)], distant metastasis (HR, 0.767; 95% CI, 0.344–1.712;
P=0.517; Table IV), total relapse
(HR, 1.623; 95% CI, 0.475–5.539; P=0.440; Table V) or breast cancer mortality (HR,
0.478; 95% CI, 0.080–2.869; P=0.419; Table V). HER2-enriched subtype was also not
associated with reduced risks in LRR (HR, 0.937; 95% CI,
0.318–2.757; P=0.906; Table IV),
distant metastasis (HR, 1.492; 95% CI, 0.540–4.126; P=0.441;
Table IV), total relapse (HR, 1.277;
95% CI, 0.512–3.186; P=0.600; Table
V) or breast cancer mortality (HR, 1.602; 95% CI, 0.511–5.023;
P=0.419; Table V) when contrasted to
that of TNBC group. As a result, TNBC was not an independent
prognostic predictor for patients with BCT in the present
study.
| Table IV.Multivariate analysis of 5-year risks
of LRR and distant metastases of patients with breast-conserving
treatment. |
Table IV.
Multivariate analysis of 5-year risks
of LRR and distant metastases of patients with breast-conserving
treatment.
|
| LRR | Distant
metastases |
|---|
|
|
|
|
|---|
|
Characteristics | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Molecular
subtypes |
|
|
|
|
|
|
|
TNBC | 1.000 |
|
| 1.000 |
|
|
|
Luminal | 0.316 | 0.043–2.317 | 0.257 | 0.767 | 0.344–1.712 | 0.517 |
|
HER2-enriched | 0.937 | 0.318–2.757 | 0.906 | 1.492 | 0.540–4.126 | 0.441 |
| Age at diagnosis,
years |
|
|
|
|
|
|
|
≤35 | 1.000 |
|
| NA |
|
|
|
36–55 | 0.407 | 0.174–0.949 | 0.037 |
|
|
|
|
>55 | 0.459 | 0.143–1.470 | 0.190 |
|
|
|
| Menopausal
status |
|
|
|
|
|
|
|
Premenopausal | NA |
|
| 1.000 |
|
|
|
Postmenopausal |
|
|
| 1.536 | 0.770–3.063 | 0.223 |
| Histological
grade |
|
|
|
|
|
|
| I | 1.000 |
|
| 1.000 |
|
|
| II | 2.345 | 0.534–10.291 | 0.259 | 5.064 | 1.198–21.407 | 0.027 |
|
III | 3.595 | 0.731–17.675 | 0.115 | 6.408 | 1.351–30.397 | 0.019 |
|
Unknown | 1.274 | 0.172–9.440 | 0.813 | 1.487 | 0.202–10.939 | 0.697 |
| Margin |
|
|
|
|
|
|
|
Positive | 1.000 |
|
| 1.000 |
|
|
|
Negative | 0.135 | 0.028–0.647 | 0.012 | 0.210 | 0.059–0.746 | 0.016 |
| Chemotherapy |
|
|
|
|
|
|
|
None | NA |
|
| 1.000 |
|
|
|
CMF |
|
|
| 1.007 | 0.295–3.434 | 0.992 |
|
A/T |
|
|
| 0.473 | 0.159–1.403 | 0.177 |
|
Other |
|
|
| 1.826 | 0.479–6.965 | 0.378 |
| Radiation
therapy |
|
|
|
|
|
|
|
None | 1.000 |
|
| 1.000 |
|
|
|
Breast | 0.178 | 0.050–0.638 | 0.008 | 0.206 | 0.077–0.554 | 0.002 |
| Breast
and SCF | 0.123 | 0.019–0.805 | 0.029 | 0.338 | 0.090–1.266 | 0.107 |
| Hormone
therapy |
|
|
|
|
|
|
| No | 1.000 |
|
| NA |
|
|
|
Yes | 1.081 | 0.152–7.697 | 0.938 |
|
|
|
|
Unknown | 1.119 | 0.069–18.065 | 0.937 |
|
|
|
| Table V.Multivariate analysis of 5-year risks
of total relapse and breast cancer mortality of patients with
breast-conserving treatment. |
Table V.
Multivariate analysis of 5-year risks
of total relapse and breast cancer mortality of patients with
breast-conserving treatment.
|
| Total relapse | Breast cancer
mortality |
|---|
|
|
|
|
|---|
|
Characteristics | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Molecular
subtype |
|
|
|
|
|
|
|
TNBC | 1.000 |
|
| 1.000 |
|
|
|
Luminal | 1.623 | 0.475–5.539 | 0.440 | 0.478 | 0.080–2.869 | 0.419 |
|
HER2-enriched | 1.277 | 0.512–3.186 | 0.600 | 1.602 | 0.511–5.023 | 0.419 |
| Age at diagnosis,
years |
|
|
|
|
|
|
|
≤35 | 1.000 |
|
| NA |
|
|
|
36–55 | 0.359 | 0.173–0.747 | 0.006 |
|
|
|
|
>55 | 0.250 | 0.078–0.807 | 0.020 |
|
|
|
| Menopausal
status |
|
|
|
|
|
|
|
Premenopausal | 1.000 |
|
| NA |
|
|
|
Postmenopausal | 2.133 | 0.972–4.682 | 0.059 |
|
|
|
| Number of positive
LNs |
|
|
|
|
|
|
| 0 | 1.000 |
|
| NA |
|
|
|
1–3 | 1.741 | 0.868–3.490 | 0.118 |
|
|
|
| ≥4 | 2.077 | 0.536–8.050 | 0.290 |
|
|
|
| Histological
grade |
|
|
|
|
|
|
| I | 1.000 |
|
| NA |
|
|
| II | 2.532 | 0.885–7.247 | 0.083 |
|
|
|
|
III | 3.584 | 1.121–11.457 | 0.031 |
|
|
|
|
Unknown | 0.836 | 0.175–3.989 | 0.823 |
|
|
|
| Margin status |
|
|
|
|
|
|
|
Positive | 1.000 |
|
| NA |
|
|
|
Negative | 0.117 | 0.041–0.336 | <0.001 |
|
|
|
| Chemotherapy |
|
|
|
|
|
|
|
None | 1.000 |
|
| 1.000 |
|
|
|
CMF | 1.331 | 0.382–4.633 | 0.653 | 0.611 | 0.134–2.784 | 0.525 |
|
A/T | 0.723 | 0.236–2.220 | 0.571 | 0.496 | 0.126–1.960 | 0.318 |
|
Other | 2.218 | 0.564–8.720 | 0.254 | 1.877 | 0.355–9.921 | 0.458 |
| Radiation
therapy |
|
|
|
|
|
|
|
None | 1.000 |
|
| 1.000 |
|
|
|
Breast | 0.179 | 0.068–0.471 | <0.001 | 0.219 | 0.066–0.729 | 0.013 |
| Breast
and SCF | 0.174 | 0.041–0.740 | 0.018 | 0.278 | 0.046–1.672 | 0.162 |
| Hormone
therapy |
|
|
|
|
|
|
| No | 1.000 |
|
| 1.000 |
|
|
|
Yes | 0.455 | 0.147–1.407 | 0.171 | 0.812 | 0.149–4.426 | 0.810 |
|
Unknown | 0.326 | 0.056–1.902 | 0.213 | 1.961 | 0.219–17.577 | 0.547 |
Other prognostic factors associated
with 5-year outcomes for patients with BCT
In multivariate analysis, patients who were aged
36–55 years showed a reduced risk in 5-year LRR compared with
patients ≤35 years (P=0.037; Table
IV), and both patients aged 36–55 years and patients >55
years showed a inferior risk of total relapse compared with
patients ≤35 years (P<0.05; Tables
IV and V). Patients with
histological grade II or III tumors exhibited higher risk of
distant metastasis (P<0.05; Table
IV), and patients with histological grade III tumors also
showed an increased risk of total relapse (P=0.031; Table V) compared with patients with
histological grade I tumors. Negative margin status was associated
with reduced risks of LRR, distant metastasis and total relapse
(P<0.05; Tables IV and V) compared with positive margin status.
Patients performed radiation therapy presented decreased risks in
LRR, distant metastasis, total relapse and breast cancer mortality
compared with patients without radiation therapy (Tables IV and V).
Discussion
The associations between breast cancer types with
different gene expression profiles and the prognosis of patients
have recently been investigated (23). TNBC confers a poor clinical outcome to
patients following BCT (24).
Basal-like subtype has also been reported to be associated with an
increased risk of local relapse and distant metastasis following
BCT (15). Although basal-like
subtype and TNBC are different breast cancer subtypes, it has been
widely accepted that TNBC and basal-like breast tumors are
synonymous (7).
In the current study, it was demonstrated that
patients with TNBC presented different clinicopathological
parameters compared with patients with luminal and HER2-enriched
breast cancer. Patients with TNBC tended to have relatively high
histological grades of tumor compared with luminal and
HER2-enriched breast cancer patients. Consistent with this finding,
previous studies have also reported that TNBC was more frequently
associated with a higher histological grade (8,24).
Selection of chemotherapy treatment also differed between the 3
groups. The proportion of the patients that received chemotherapy
was higher in the TNBC group than in other groups, which was
consistent with the results of a previous study (25). Besides, patients with TNBC tended to
choose anthracycline/taxane based chemotherapy regimens in the
present study, although Kim et al (26) did not find similar results among
luminal, HER2-enriched and TNBC groups.
However, there was no significant difference in
prognosis between patients with TNBC and patients with luminal and
HER2 subtypes following BCT. In the present study, the results of
univariate analysis revealed that patients in the HER2-enriched
subtype group exhibited reduced 5-year LRFS and OS, and rates of
LRR and mortality were relatively high compared with the luminal
and TNBC groups (i.e. the prognosis of patients with TNBC was not
the poorest). Furthermore, results of multivariate analysis in our
study indicated that TNBC was not associated with increased risks
of 5-year LRR, distant metastasis, total relapse and mortality for
patients with BCT. Similar to the present study, Gangi A et
al (19) observed that TNBC was
not associated with an increased rate of 5-year local relapse
compared with non-TNBC subtypes in a retrospective study of 1851
patients with BCT. Additionally, Freedman et al (27) reported that the isolated 5-year LRR
rate for patients with BCT was not different according to different
breast cancer subtypes, and it was observed that there was a
significantly higher rate of mortality in the HER2-enriched group
compared with other subtypes. Findings in the present study
indicated that HER2-enriched tumor was not an independent
prognostic predictor for patients with BCT. The high rates of LRR
and mortality in HER2-enriched subtype may be attributed to a small
proportion of patients with positive HER2 status that had received
trastuzumab therapy. Another reason for these high rates might be
that young patients (≤35 years) who appeared to have a poorer
prognosis (as confirmed in the present study) tended to be assigned
to the HER2-enriched group and not the TNBC group. Noh et al
(25) also demonstrated that despite
the observation that TNBC and HER2-enriched subtypes were
associated with younger age and higher histological grade, the
rates of LRR and distant recurrence were not significantly
different according to different molecular subtypes of breast
cancer in patients following BCT.
To the best of our knowledge, the outcomes of TNBC
patients with BCT remain contradictory. Solin et al
(16) investigated 519 patients
treated with BCT, and reported that patients with TNBC had an
increased risk of local failure but a reduced risk of distant
metastasis compared with other breast cancer subtypes. On the
contrary, another investigation demonstrated that the TNBC subtype
was associated with a higher risk of distant metastasis and
mortality but was not associated with significantly higher rates of
local relapse compared with other subtype (17). Kaplan et al (24) reported that patients with TNBC at a
low risk of LRR had a significantly higher risk of distant
metastasis compared with hormone receptor-positive/HER2-negative
patients. Additionally, Braunstein et al (28) observed that TNBC was associated with
reduced DFS following BCT in a retrospective study, which included
2,233 women who underwent BCT. In general, the issues regarding the
role of TNBC in BCT remain unresolved. Encouragingly, the
investigators have reported that TNBC patients with BCT had
significantly lower LRR rate compared with patients treated with
mastectomy (29). Results from a
prospective randomized controlled multi-center trial indicate that
for patients with TNBC following BCT, radiotherapy and chemotherapy
exhibited significantly improved 5-year DFS and OS compared with
those that received chemotherapy alone (30). Together with the findings from the
previously mentioned reports and results from our study, patients
with TNBC may remain appropriate candidates for BCT.
To date, publications evaluating the prognostic
value of TNBC in BCT, demonstrated mixed results. There may be a
number of reasons to account of these inconsistencies in findings.
The term ‘TNBC’ has been used interchangeably with ‘basal-like
tumor’. The majority of TNBC are basal-like breast cancers, and the
majority of basal-like tumors are also TNBC, which means that there
is a considerable overlap between TNBC and basal-like tumors
(31,32). Additionally, TNBC has been subdivided
into six distinct subtypes based on expression of various genes,
including two basal-like subtypes, one with cell-cycle and
DNA-damage-response gene expression signatures and the other
enriched in growth factor signaling and myoepithelial markers; one
immunomodulatory subtype; two mesenchymal subtypes with high
expression of genes involved in differentiation and growth factor
pathways; and one luminal androgen receptor subtype driven by
androgen signaling (4,33). For certain TNBC subtypes, mastectomy
may lead to improved long-term outcomes compared with BCT (34). However, few studies differentiate
basal-like subtype tumors from TNBC or clearly define the distinct
TNBC subtypes (32,35), which may result in contradictory
outcomes following BCT reported in studies investigating patients
with TNBC.
There are a number of limitations to the present
study. Firstly, similar to other publications, owing to the
limitations of detection techniques, examination instrumentation
and cost, TNBC was not distinguished from basal-like tumors, and
TNBC was used as a surrogate to represent the basal-like category
of breast cancer, which may confound the results of our
investigation to some extent. Secondly, the immunostaining data did
not classify TNBC into detailed subtypes in the present study.
Thirdly, we acknowledge other limitations, including the
retrospective study design, small sample size used and short
follow-up periods. Finally, other unbalanced confounding factors
between groups, including hormone therapy regimen, economic
conditions, smoking, alcohol consumption, obesity and chronic
disease, were also potential limitations. As a result, the
contribution of the present study to the investigation of molecular
subtypes in breast cancer may be limited.
In conclusion, the data in the present study
suggests that the clinicopathological characteristics of TNBC
differ from luminal and HER2-enriched subtypes. TNBC patients
treated with BCT did not have a significantly increased risk of
recurrence or mortality, and patients with TNBC may remain
appropriate candidates for BCT. However, detailed molecular
taxonomy and prospective randomized clinical trials are
required.
Acknowledgements
The present study was partly supported by the Grant
from National Natural Science Foundation of China (grant no.
81472472) and Grant from the Clinical New Technology Development
Project from the Tianjin Medical University Cancer Institute and
Hospital (grant no. 2012017).
Glossary
Abbreviations
Abbreviations:
|
TNBC
|
triple-negative breast cancer
|
|
ER
|
estrogen receptor
|
|
PR
|
progesterone receptor
|
|
HER2
|
human epidermal growth factor receptor
2
|
|
BCT
|
breast-conserving treatment
|
|
LRR
|
locoregional recurrence
|
|
LRFS
|
locoregional recurrence-free
survival
|
|
DMFS
|
distant metastasis-free survival
|
|
DFS
|
disease-free survival
|
|
OS
|
overall survival
|
|
HR
|
hazard ratio
|
|
CI
|
confidence interval
|
References
|
1
|
Wiechmann L, Sampson M, Stempel M, Jacks
LM, Patil SM, King T and Morrow M: Presenting features of breast
cancer differ by molecular subtype. Ann Surg Oncol. 16:2705–2710.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Perou CM: Molecular stratification of
triple-negative breast cancers. Oncologist. 1 16 Suppl:S61–S70.
2011. View Article : Google Scholar
|
|
3
|
Perou CM, Sorlie T, Eisen MB, van de Rijn
M, Jeffrey SS, Rees CA, Pollack JR, Ross DT, Johnsen H, Akslen LA,
et al: Molecular portraits of human breast tumours. Nature.
406:747–752. 2000. View
Article : Google Scholar : PubMed/NCBI
|
|
4
|
Abramson VG, Lehmann BD, Ballinger TJ and
Pietenpol JA: Subtyping of triple-negative breast cancer:
Implications for therapy. Cancer. 121:8–16. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Foulkes WD, Smith IE and Reis-Filho JS:
Triple-negative breast cancer. N Engl JMed. 363:1938–1948. 2010.
View Article : Google Scholar
|
|
6
|
Brenton JD, Carey LA, Ahmed AA and Caldas
C: Molecular classification and molecular forecasting of breast
cancer: Ready for clinical application? J Clin Oncol. 23:7350–7360.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pignol JP, Rakovitch E and Olivotto IA: Is
breast conservation therapy superior to mastectomy for women with
triple-negative breast cancers? J Clin Oncol. 29:2841–2843. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Dent R, Trudeau M, Pritchard KI, Hanna WM,
Kahn HK, Sawka CA, Lickley LA, Rawlinson E, Sun P and Narod SA:
Triple-negative breast cancer: Clinical features and patterns of
recurrence. Clin Cancer Res. 13:4429–4434. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kyndi M, Sørensen FB, Knudsen H, Overgaard
M, Nielsen HM and Overgaard J; Danish Breast Cancer Cooperative
Group, : Estrogen receptor, progesterone receptor, HER-2, and
response to postmastectomy radiotherapy in high-risk breast cancer:
The danish breast cancer cooperative group. J Clin Oncol.
26:1419–1426. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Voduc KD, Cheang MC, Tyldesley S, Gelmon
K, Nielsen TO and Kennecke H: Breast cancer subtypes and the risk
of local and regional relapse. J Clin Oncol. 28:1684–1691. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gabos Z, Thoms J, Ghosh S, Hanson J,
Deschenes J, Sabri S and Abdulkarim B: The association between
biological subtype and locoregional recurrence in newly diagnosed
breast cancer. Breast Cancer Res Treat. 124:187–194. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
van Dongen JA, Voogd AC, Fentiman IS,
Legrand C, Sylvester RJ, Tong D, van der Schueren E, Helle PA, van
Zijl K and Bartelink H: Long-term results of a randomized trial
comparing breast-conserving therapy with mastectomy: European
organization for research and treatment of cancer 10801 trial. J
Natl Cancer Inst. 92:1143–1150. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Veronesi U, Cascinelli N, Mariani L, Greco
M, Saccozzi R, Luini A, Aguilar M and Marubini E: Twenty-year
follow-up of a randomized study comparing breast-conserving surgery
with radical mastectomy for early breast cancer. N Engl J Med.
347:1227–1232. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lazovich D, Solomon CC, Thomas DB, Moe RE
and White E: Breast conservation therapy in the United States
following the 1990 national institutes of health consensus
development conference on the treatment of patients with early
stage invasive breast carcinoma. Cancer. 86:628–637. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Nguyen PL, Taghian AG, Katz MS, Niemierko
A, Abi Raad RF, Boon WL, Bellon JR, Wong JS, Smith BL and Harris
JR: Breast cancer subtype approximated by estrogen receptor,
progesterone receptor and HER-2 is associated with local and
distant recurrence after breast-conserving therapy. J Clin Oncol.
26:2373–2378. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Solin LJ, Hwang WT and Vapiwala N: Outcome
after breast conservation treatment with radiation for women with
triple-negative early-stage invasive breast carcinoma. Clin Breast
Cancer. 9:96–100. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Haffty BG, Yang Q, Reiss M, Kearney T,
Higgins SA, Weidhaas J, Harris L, Hait W and Toppmeyer D:
Locoregional relapse and distant metastasis in conservatively
managed triple negative early-stage breast cancer. J Clin Oncol.
24:5652–5657. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Millar EK, Graham PH, O'Toole SA, McNeil
CM, Browne L, Morey AL, Eggleton S, Beretov J, Theocharous C, Capp
A, et al: Prediction of local recurrence, distant metastases and
death after breast-conserving therapy in early-stage invasive
breast cancer using a five-biomarker panel. J Clin Oncol.
27:4701–4708. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gangi A, Chung A, Mirocha J, Liou DZ,
Leong T and Giuliano AE: Breast-conserving therapy for
triple-negative breast cancer. JAMA Surg. 149:252–258. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Connolly JL: Changes and problematic areas
in interpretation of the AJCC cancer staging manual, 6th edition,
for breast cancer. Arch Pathol Lab Med. 130:287–291.
2006.PubMed/NCBI
|
|
21
|
Elston CW and Ellis IO: Pathological
prognostic factors in breast cancer. I. The value of histological
grade in breast cancer: Experience from a large study with
long-term follow-up. Histopathology. 19:403–410. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tummaruk P, Tienthai P, Manee-In S and
Srisuwatanasagul S: Expression of progesterone receptor in the
utero-tubal junction after intra-uterine and deep intra-uterine
insemination in sows. Reprod Domest Anim. 45:e26–e31.
2010.PubMed/NCBI
|
|
23
|
Cejalvo JM, Martínez de Dueñas E, Galván
P, García-Recio S, Burgués Gasión O, Paré L, Antolín S, Martinello
R, Blancas I, Adamo B, et al: Intrinsic subtypes and gene
expression profiles in primary and metastatic breast cancer. Cancer
Res. 77:2213–2221. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kaplan HG, Malmgren JA and Atwood M: T1N0
triple negative breast cancer: Risk of recurrence and adjuvant
chemotherapy. Breast J. 15:454–460. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Noh JM, Choi DH, Huh SJ, Park W, Yang JH,
Nam SJ, Im YH and Ahn JS: Patterns of recurrence after
breast-conserving treatment for early stage breast cancer by
molecular subtype. J Breast Cancer. 14:46–51. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kim JY, Chang SK, Park H, Lee BM and Shin
HS: Treatment outcome in patients with triple negative early stage
breast cancers compared with other molecular subtypes. Radiat Oncol
J. 30:124–131. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Freedman GM, Anderson PR, Li T and
Nicolaou N: Locoregional recurrence of triple-negative breast
cancer after breast-conserving surgery and radiation. Cancer.
115:946–951. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Braunstein LZ, Niemierko A, Shenouda MN,
Truong L, Sadek BT, Abi Raad R, Wong JS, Punglia RS, Taghian AG and
Bellon JR: Outcome following local-regional recurrence in women
with early-stage breast cancer: Impact of biologic subtype. Breast
J. 21:161–167. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Abdulkarim BS, Cuartero J, Hanson J,
Deschenes J, Lesniak D and Sabri S: Increased risk of locoregional
recurrence for women with T1-2N0 triple-negative breast cancer
treated with modified radical mastectomy without adjuvant radiation
therapy compared with breast-conserving therapy. J Clin Oncol.
29:2852–2858. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wang J, Shi M, Ling R, Xia Y, Luo S, Fu X,
Xiao F, Li J, Long X, Wang J, et al: Adjuvant chemotherapy and
radiotherapy in triple-negative breast carcinoma: A prospective
randomized controlled multi-center trial. Radiother Oncol.
100:200–204. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Guiu S, Michiels S, Andre F, Cortes J,
Denkert C, Di Leo A, Hennessy BT, Sorlie T, Sotiriou C, Turner N,
et al: Molecular subclasses of breast cancer: How do we define
them? The IMPAKT 2012 working group statement. Ann Oncol.
23:2997–3006. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Weigelt B, Mackay A, A'Hern R, Natrajan R,
Tan DS, Dowsett M, Ashworth A and Reis-Filho JS: Breast cancer
molecular profiling with single sample predictors: A retrospective
analysis. Lancet Oncol. 11:339–349. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Lehmann BD, Bauer JA, Chen X, Sanders ME,
Chakravarthy AB, Shyr Y and Pietenpol JA: Identification of human
triple-negative breast cancer subtypes and preclinical models for
selection of targeted therapies. J Clin Invest. 121:2750–2767.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Eiermann W and Vallis KA: Locoregional
treatments for triple-negative breast cancer. Ann Oncol. 23 Suppl
6:vi30–vi34. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Sotiriou C, Neo SY, McShane LM, Korn EL,
Long PM, Jazaeri A, Martiat P, Fox SB, Harris AL and Liu ET: Breast
cancer classification and prognosis based on gene expression
profiles from a population-based study. Proc Natl Acad Sci USA.
100:pp. 10393–10398. 2003; View Article : Google Scholar : PubMed/NCBI
|